
Epidemiology of Merkel Cell Polyomavirus Infection and Merkel Cell Carcinoma
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
3. Epidemiology of MCPyV Infection
3.1. MCPyV Infection of the Skin
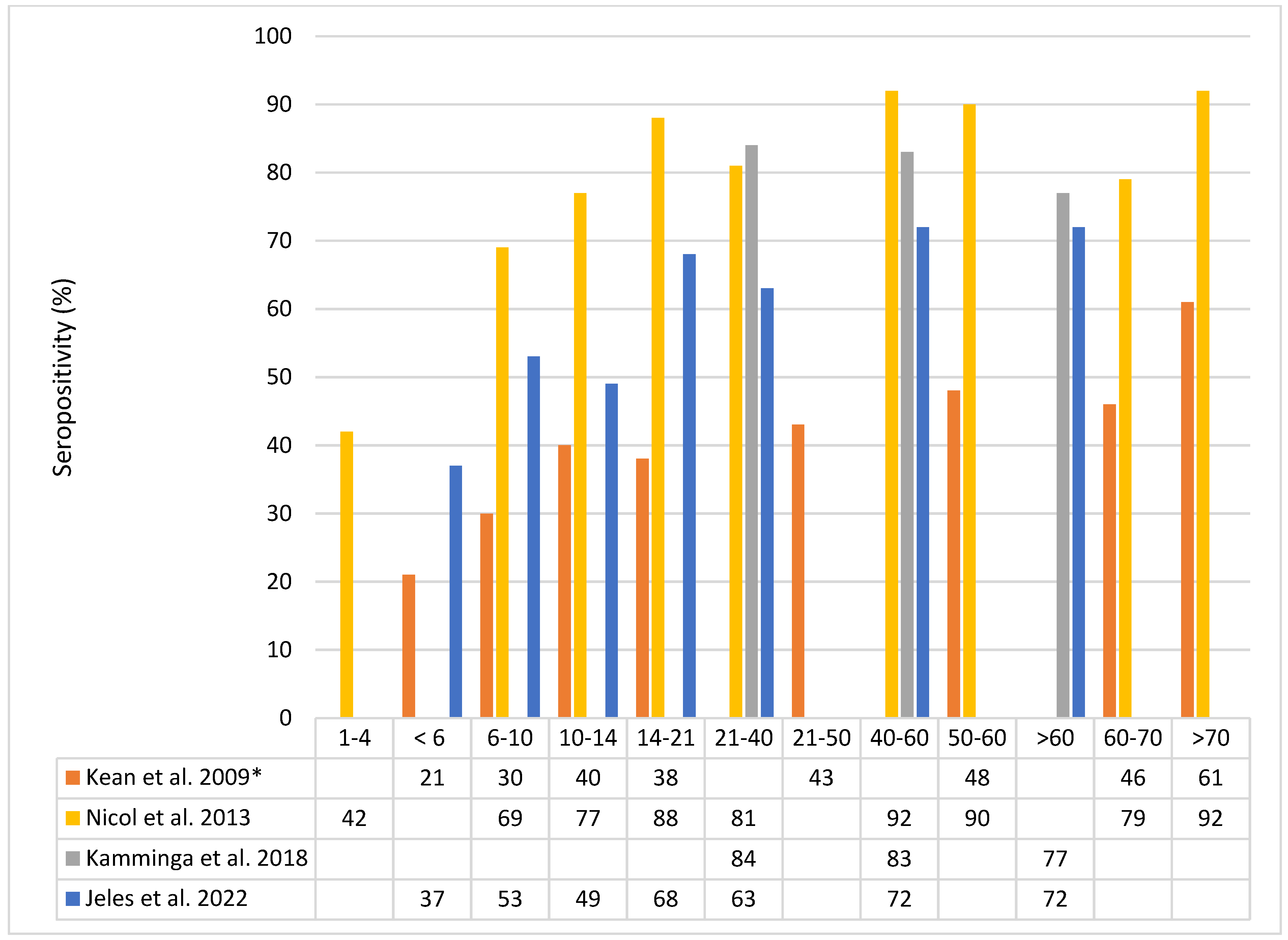
3.2. MCPyV Seroprevalence

3.3. MCPyV Prevalence in Non-Cutaneous Sites
4. Merkel Cell Carcinoma
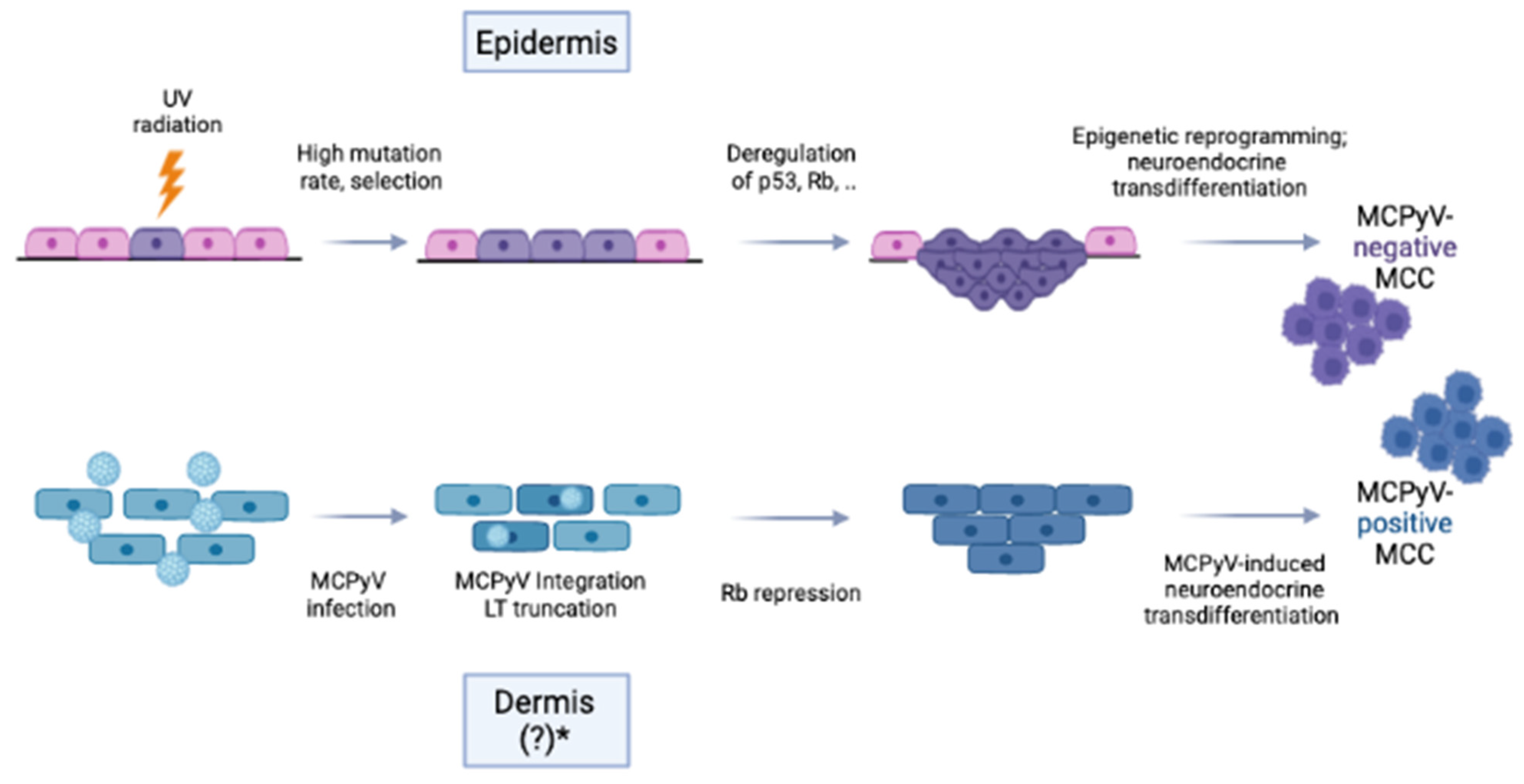
4.1. MCC Entities

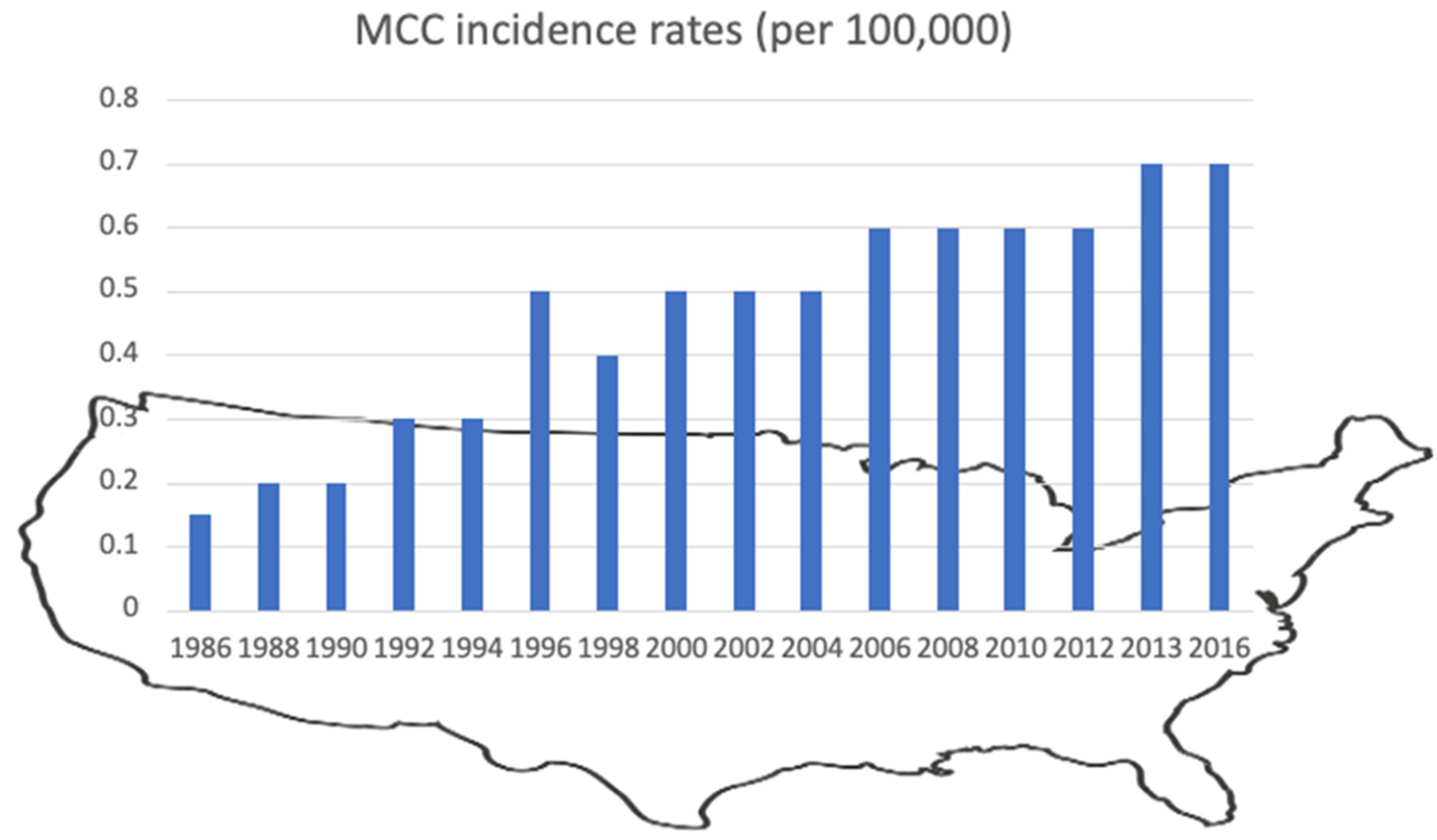
4.2. Trends in MCC Incidence
4.3. MCC Characteristics and Risk Factors
4.4. MCC Recurrence and Survival
4.5. Non-Cutaneous MCC
5. MCPyV in Malignancies Other than MCC
6. Summary/Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Feng, H.; Shuda, M.; Chang, Y.; Moore, P.S. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science 2008, 319, 1096–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shuda, M.; Feng, H.; Kwun, H.J.; Rosen, S.T.; Gjoerup, O.; Moore, P.S.; Chang, Y. T antigen mutations are a human tumor-specific signature for Merkel cell polyomavirus. Proc. Natl. Acad. Sci. USA 2008, 105, 16272–16277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moens, U.; Prezioso, C.; Pietropaolo, V. Genetic Diversity of the Noncoding Control Region of the Novel Human Polyomaviruses. Viruses 2020, 12, 1406. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Yang, R.; Payne, A.S.; Schowalter, R.M.; Spurgeon, M.E.; Lambert, P.F.; Xu, X.; Buck, C.B.; You, J. Identifying the Target Cells and Mechanisms of Merkel Cell Polyomavirus Infection. Cell Host Microbe 2016, 19, 775–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, R.; Lee, E.E.; Kim, J.; Choi, J.H.; Kolitz, E.; Chen, Y.; Crewe, C.; Salisbury, N.J.H.; Scherer, P.E.; Cockerell, C.; et al. Characterization of ALTO-encoding circular RNAs expressed by Merkel cell polyomavirus and trichodysplasia spinulosa polyomavirus. PLoS Pathog. 2021, 17, e1009582. [Google Scholar] [CrossRef]
- Bopp, L.; Wieland, U.; Hellmich, M.; Kreuter, A.; Pfister, H.; Silling, S. Natural History of Cutaneous Human Polyomavirus Infection in Healthy Individuals. Front. Microbiol. 2021, 12, 740947. [Google Scholar] [CrossRef]
- Schowalter, R.M.; Pastrana, D.V.; Pumphrey, K.A.; Moyer, A.L.; Buck, C.B. Merkel cell polyomavirus and two previously unknown polyomaviruses are chronically shed from human skin. Cell Host Microbe 2010, 7, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Hashida, Y.; Imajoh, M.; Kamioka, M.; Taniguchi, A.; Kuroda, N.; Hayashi, K.; Nakajima, H.; Sano, S.; Daibata, M. Phylogenetic analysis of Merkel cell polyomavirus based on full-length LT and VP1 gene sequences derived from neoplastic tumours in Japanese patients. J. Gen. Virol. 2014, 95, 135–141. [Google Scholar] [CrossRef] [Green Version]
- Zwijnenburg, E.M.; Lubeek, S.F.K.; Werner, J.E.M.; Amir, A.L.; Weijs, W.L.J.; Takes, R.P.; Pegge, S.A.H.; van Herpen, C.M.L.; Adema, G.J.; Kaanders, J. Merkel Cell Carcinoma: New Trends. Cancers 2021, 13, 1614. [Google Scholar] [CrossRef]
- Abedi Kiasari, B.; Vallely, P.J.; Klapper, P.E. Merkel cell polyomavirus DNA in immunocompetent and immunocompromised patients with respiratory disease. J. Med. Virol. 2011, 83, 2220–2224. [Google Scholar] [CrossRef]
- Kean, J.M.; Rao, S.; Wang, M.; Garcea, R.L. Seroepidemiology of human polyomaviruses. PLoS Pathog. 2009, 5, e1000363. [Google Scholar] [CrossRef] [Green Version]
- Foulongne, V.; Kluger, N.; Dereure, O.; Mercier, G.; Molès, J.P.; Guillot, B.; Segondy, M. Merkel cell polyomavirus in cutaneous swabs. Emerg. Infect. Dis. 2010, 16, 685–687. [Google Scholar] [CrossRef]
- Wieland, U.; Silling, S.; Scola, N.; Potthoff, A.; Gambichler, T.; Brockmeyer, N.H.; Pfister, H.; Kreuter, A. Merkel cell polyomavirus infection in HIV-positive men. Arch. Dermatol. 2011, 147, 401–406. [Google Scholar] [CrossRef] [Green Version]
- Hampras, S.S.; Michel, A.; Schmitt, M.; Waterboer, T.; Kranz, L.; Gheit, T.; Fisher, K.; Sondak, V.K.; Messina, J.; Fenske, N.; et al. Merkel cell polyomavirus (MCV) T-antigen seroreactivity, MCV DNA in eyebrow hairs, and squamous cell carcinoma. Infect. Agent Cancer 2015, 10, 35. [Google Scholar] [CrossRef] [Green Version]
- Hashida, Y.; Kamioka, M.; Tanaka, M.; Hosokawa, S.; Murakami, M.; Nakajima, K.; Kikuchi, H.; Fujieda, M.; Sano, S.; Daibata, M. Ecology of Merkel Cell Polyomavirus in Healthy Skin Among Individuals in an Asian Cohort. J. Infect Dis. 2016, 213, 1708–1716. [Google Scholar] [CrossRef] [Green Version]
- Pastrana, D.V.; Peretti, A.; Welch, N.L.; Borgogna, C.; Olivero, C.; Badolato, R.; Notarangelo, L.D.; Gariglio, M.; FitzGerald, P.C.; McIntosh, C.E.; et al. Metagenomic Discovery of 83 New Human Papillomavirus Types in Patients with Immunodeficiency. mSphere 2018, 3, e00645-18. [Google Scholar] [CrossRef] [Green Version]
- Kamminga, S.; van der Meijden, E.; Feltkamp, M.C.W.; Zaaijer, H.L. Seroprevalence of fourteen human polyomaviruses determined in blood donors. PLoS ONE 2018, 13, e0206273. [Google Scholar] [CrossRef] [Green Version]
- Jeles, K.; Katona, M.; Csoma, E. Seroprevalence of Four Polyomaviruses Linked to Dermatological Diseases: New Findings and a Comprehensive Analysis. Viruses 2022, 14, 2282. [Google Scholar] [CrossRef]
- Nicol, J.T.; Robinot, R.; Carpentier, A.; Carandina, G.; Mazzoni, E.; Tognon, M.; Touzé, A.; Coursaget, P. Age-specific seroprevalences of merkel cell polyomavirus, human polyomaviruses 6, 7, and 9, and trichodysplasia spinulosa-associated polyomavirus. Clin. Vaccine Immunol. 2013, 20, 363–368. [Google Scholar] [CrossRef]
- Pastrana, D.V.; Tolstov, Y.L.; Becker, J.C.; Moore, P.S.; Chang, Y.; Buck, C.B. Quantitation of human seroresponsiveness to Merkel cell polyomavirus. PLoS Pathog. 2009, 5, e1000578. [Google Scholar] [CrossRef]
- Pastrana, D.V.; Wieland, U.; Silling, S.; Buck, C.B.; Pfister, H. Positive correlation between Merkel cell polyomavirus viral load and capsid-specific antibody titer. Med. Microbiol. Immunol. 2012, 201, 17–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faust, H.; Pastrana, D.V.; Buck, C.B.; Dillner, J.; Ekström, J. Antibodies to Merkel cell polyomavirus correlate to presence of viral DNA in the skin. J. Infect Dis. 2011, 203, 1096–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulson, K.G.; Lewis, C.W.; Redman, M.W.; Simonson, W.T.; Lisberg, A.; Ritter, D.; Morishima, C.; Hutchinson, K.; Mudgistratova, L.; Blom, A.; et al. Viral oncoprotein antibodies as a marker for recurrence of Merkel cell carcinoma: A prospective validation study. Cancer 2017, 123, 1464–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nghiem, P.; Park, S.Y. Less Toxic, More Effective Treatment-A Win-Win for Patients with Merkel Cell Carcinoma. JAMA Dermatol. 2019, 155, 1223–1224. [Google Scholar] [CrossRef] [PubMed]
- Csoboz, B.; Rasheed, K.; Sveinbjørnsson, B.; Moens, U. Merkel cell polyomavirus and non-Merkel cell carcinomas: Guilty or circumstantial evidence? Apmis 2020, 128, 104–120. [Google Scholar] [CrossRef] [Green Version]
- Bialasiewicz, S.; Lambert, S.B.; Whiley, D.M.; Nissen, M.D.; Sloots, T.P. Merkel cell polyomavirus DNA in respiratory specimens from children and adults. Emerg. Infect Dis. 2009, 15, 492–494. [Google Scholar] [CrossRef]
- Goh, S.; Lindau, C.; Tiveljung-Lindell, A.; Allander, T. Merkel cell polyomavirus in respiratory tract secretions. Emerg. Infect. Dis. 2009, 15, 489–491. [Google Scholar] [CrossRef]
- Kantola, K.; Sadeghi, M.; Lahtinen, A.; Koskenvuo, M.; Aaltonen, L.M.; Möttönen, M.; Rahiala, J.; Saarinen-Pihkala, U.; Riikonen, P.; Jartti, T.; et al. Merkel cell polyomavirus DNA in tumor-free tonsillar tissues and upper respiratory tract samples: Implications for respiratory transmission and latency. J. Clin. Virol. 2009, 45, 292–295. [Google Scholar] [CrossRef]
- Babakir-Mina, M.; Ciccozzi, M.; Lo Presti, A.; Greco, F.; Perno, C.F.; Ciotti, M. Identification of Merkel cell polyomavirus in the lower respiratory tract of Italian patients. J. Med. Virol. 2010, 82, 505–509. [Google Scholar] [CrossRef]
- Saláková, M.; Košlabová, E.; Vojtěchová, Z.; Tachezy, R.; Šroller, V. Detection of human polyomaviruses MCPyV, HPyV6, and HPyV7 in malignant and non-malignant tonsillar tissues. J. Med. Virol. 2016, 88, 695–702. [Google Scholar] [CrossRef]
- Herberhold, S.; Hellmich, M.; Panning, M.; Bartok, E.; Silling, S.; Akgül, B.; Wieland, U. Human polyomavirus and human papillomavirus prevalence and viral load in non-malignant tonsillar tissue and tonsillar carcinoma. Med. Microbiol. Immunol. 2017, 206, 93–103. [Google Scholar] [CrossRef]
- Moustafa, A.; Xie, C.; Kirkness, E.; Biggs, W.; Wong, E.; Turpaz, Y.; Bloom, K.; Delwart, E.; Nelson, K.E.; Venter, J.C.; et al. The blood DNA virome in 8000 humans. PLoS Pathog. 2017, 13, e1006292. [Google Scholar] [CrossRef] [Green Version]
- Fukumoto, H.; Sato, Y.; Hasegawa, H.; Katano, H. Frequent detection of Merkel cell polyomavirus DNA in sera of HIV-1-positive patients. Virol. J. 2013, 10, 84. [Google Scholar] [CrossRef] [Green Version]
- Pancaldi, C.; Corazzari, V.; Maniero, S.; Mazzoni, E.; Comar, M.; Martini, F.; Tognon, M. Merkel cell polyomavirus DNA sequences in the buffy coats of healthy blood donors. Blood 2011, 117, 7099–7101. [Google Scholar] [CrossRef]
- Shuda, M.; Arora, R.; Kwun, H.J.; Feng, H.; Sarid, R.; Fernandez-Figueras, M.T.; Tolstov, Y.; Gjoerup, O.; Mansukhani, M.M.; Swerdlow, S.H.; et al. Human Merkel cell polyomavirus infection I. MCV T antigen expression in Merkel cell carcinoma, lymphoid tissues and lymphoid tumors. Int. J. Cancer 2009, 125, 1243–1249. [Google Scholar] [CrossRef]
- Matsushita, M.; Kuwamoto, S.; Iwasaki, T.; Higaki-Mori, H.; Yashima, S.; Kato, M.; Murakami, I.; Horie, Y.; Kitamura, Y.; Hayashi, K. Detection of Merkel cell polyomavirus in the human tissues from 41 Japanese autopsy cases using polymerase chain reaction. Intervirology 2013, 56, 1–5. [Google Scholar] [CrossRef]
- Sunshine, J.C.; Jahchan, N.S.; Sage, J.; Choi, J. Are there multiple cells of origin of Merkel cell carcinoma? Oncogene 2018, 37, 1409–1416. [Google Scholar] [CrossRef]
- Wijaya, W.A.; Liu, Y.; Qing, Y.; Li, Z. Prevalence of Merkel Cell Polyomavirus in Normal and Lesional Skin: A Systematic Review and Meta-Analysis. Front. Oncol. 2022, 12, 868781. [Google Scholar] [CrossRef]
- Duncavage, E.J.; Zehnbauer, B.A.; Pfeifer, J.D. Prevalence of Merkel cell polyomavirus in Merkel cell carcinoma. Mod. Pathol. 2009, 22, 516–521. [Google Scholar] [CrossRef] [Green Version]
- Becker, J.C.; Stang, A.; DeCaprio, J.A.; Cerroni, L.; Lebbé, C.; Veness, M.; Nghiem, P. Merkel cell carcinoma. Nat. Rev. Dis. Primers 2017, 3, 17077. [Google Scholar] [CrossRef]
- Becker, J.C.; Stang, A.; Hausen, A.Z.; Fischer, N.; DeCaprio, J.A.; Tothill, R.W.; Lyngaa, R.; Hansen, U.K.; Ritter, C.; Nghiem, P.; et al. Epidemiology, biology and therapy of Merkel cell carcinoma: Conclusions from the EU project IMMOMEC. Cancer Immunol. Immunother. 2018, 67, 341–351. [Google Scholar] [CrossRef] [PubMed]
- González-Vela, M.D.C.; Curiel-Olmo, S.; Derdak, S.; Beltran, S.; Santibañez, M.; Martínez, N.; Castillo-Trujillo, A.; Gut, M.; Sánchez-Pacheco, R.; Almaraz, C.; et al. Shared Oncogenic Pathways Implicated in Both Virus-Positive and UV-Induced Merkel Cell Carcinomas. J. Investig. Dermatol. 2017, 137, 197–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krump, N.A.; You, J. From Merkel Cell Polyomavirus Infection to Merkel Cell Carcinoma Oncogenesis. Front. Microbiol. 2021, 12, 739695. [Google Scholar] [CrossRef] [PubMed]
- Pulitzer, M.P.; Amin, B.D.; Busam, K.J. Merkel cell carcinoma: Review. Adv. Anat. Pathol. 2009, 16, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Gravemeyer, J.; Spassova, I.; Verhaegen, M.E.; Dlugosz, A.A.; Hoffmann, D.; Lange, A.; Becker, J.C. DNA-methylation patterns imply a common cellular origin of virus- and UV-associated Merkel cell carcinoma. Oncogene 2022, 41, 37–45. [Google Scholar] [CrossRef]
- Harms, P.W.; Collie, A.M.; Hovelson, D.H.; Cani, A.K.; Verhaegen, M.E.; Patel, R.M.; Fullen, D.R.; Omata, K.; Dlugosz, A.A.; Tomlins, S.A.; et al. Next generation sequencing of Cytokeratin 20-negative Merkel cell carcinoma reveals ultraviolet-signature mutations and recurrent TP53 and RB1 inactivation. Mod. Pathol. 2016, 29, 240–248. [Google Scholar] [CrossRef] [Green Version]
- Becker, J.C.; Eigentler, T.; Frerich, B.; Gambichler, T.; Grabbe, S.; Höller, U.; Klumpp, B.; Loquai, C.; Krause-Bergmann, A.; Müller-Richter, U.; et al. S2k-Leitlinie Merkelzellkarzinom (MZK, MCC, neuroendokrines Karzinom der Haut)—Update 2018. J. Dtsch. Dermatol. Ges. 2019, 17, 562–577. [Google Scholar] [CrossRef]
- McEvoy, A.M.; Lachance, K.; Hippe, D.S.; Cahill, K.; Moshiri, Y.; Lewis, C.W.; Singh, N.; Park, S.Y.; Thuesmunn, Z.; Cook, M.M.; et al. Recurrence and Mortality Risk of Merkel Cell Carcinoma by Cancer Stage and Time from Diagnosis. JAMA Dermatol. 2022, 158, 382–389. [Google Scholar] [CrossRef]
- Yusuf, M.B.; McKenzie, G.; Rattani, A.; Tennant, P.; Bumpous, J.; Miller, D.; Dunlap, N. Merkel Cell Carcinoma of the Head and Neck: Epidemiology, Pathogenesis, Current State of Treatment and Future Directions. Cancers 2021, 13, 3506. [Google Scholar] [CrossRef]
- Duarte-Bateman, D.; Shen, A.; Bullock, T.; Sadeghi, P.; Escandón, J.M.; Dedkova, E.; Gastman, B.R. Best practices in surgical and nonsurgical management of head and neck Merkel cell carcinoma: An update. Mol. Carcinog. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Harvey, J.A.; Mirza, S.A.; Erwin, P.J.; Chan, A.W.; Murad, M.H.; Brewer, J.D. Recurrence and mortality rates with different treatment approaches of Merkel cell carcinoma: A systematic review and meta-analysis. Int. J. Dermatol. 2022, 61, 687–697. [Google Scholar] [CrossRef]
- Hernandez, L.E.; Mohsin, N.; Yaghi, M.; Frech, F.S.; Dreyfuss, I.; Nouri, K. Merkel cell carcinoma: An updated review of pathogenesis, diagnosis, and treatment options. Dermatol. Ther. 2022, 35, e15292. [Google Scholar] [CrossRef]
- Park, S.Y.; Doolittle-Amieva, C.; Moshiri, Y.; Akaike, T.; Parvathaneni, U.; Bhatia, S.; Zaba, L.C.; Nghiem, P. How we treat Merkel cell carcinoma: Within and beyond current guidelines. Future Oncol. 2021, 17, 1363–1377. [Google Scholar] [CrossRef]
- Turshudzhyan, A.; Hadfield, M.; Grant-Kels, J. Updates on the diagnosis, current and future therapeutic options in Merkel-cell carcinoma. Melanoma Res. 2021, 31, 421–425. [Google Scholar] [CrossRef]
- Stang, A.; Becker, J.C.; Nghiem, P.; Ferlay, J. The association between geographic location and incidence of Merkel cell carcinoma in comparison to melanoma: An international assessment. Eur. J. Cancer 2018, 94, 47–60. [Google Scholar] [CrossRef]
- Olsen, C.M.; Pandeya, N.; Whiteman, D.C. International Increases in Merkel Cell Carcinoma Incidence Rates between 1997 and 2016. J. Investig. Dermatol. 2021, 141, 2596–2601.e2591. [Google Scholar] [CrossRef]
- Paulson, K.G.; Park, S.Y.; Vandeven, N.A.; Lachance, K.; Thomas, H.; Chapuis, A.G.; Harms, K.L.; Thompson, J.A.; Bhatia, S.; Stang, A.; et al. Merkel cell carcinoma: Current US incidence and projected increases based on changing demographics. J. Am. Acad. Dermatol. 2018, 78, 457–463.e452. [Google Scholar] [CrossRef]
- Keeling, E.; O’Leary, E.; Deady, S.; JP, O.N.; Conlon, P.J.; Moloney, F.J. Gender and immunosuppression impact on Merkel cell carcinoma diagnosis and prognosis. A population based cohort study. Skin Health Dis. 2022, 2, e80. [Google Scholar] [CrossRef]
- Girschik, J.; Thorn, K.; Beer, T.W.; Heenan, P.J.; Fritschi, L. Merkel cell carcinoma in Western Australia: A population-based study of incidence and survival. Br. J. Dermatol. 2011, 165, 1051–1057. [Google Scholar] [CrossRef]
- Youlden, D.R.; Soyer, H.P.; Youl, P.H.; Fritschi, L.; Baade, P.D. Incidence and survival for Merkel cell carcinoma in Queensland, Australia, 1993–2010. JAMA Dermatol. 2014, 150, 864–872. [Google Scholar] [CrossRef]
- Garbutcheon-Singh, K.B.; Curchin, D.J.; McCormack, C.J.; Smith, S.D. Trends in the incidence of Merkel cell carcinoma in Victoria, Australia, between 1986 and 2016. Australas J. Dermatol. 2020, 61, e34–e38. [Google Scholar] [CrossRef] [PubMed]
- Robertson, J.P.; Liang, E.S.; Martin, R.C. Epidemiology of Merkel cell carcinoma in New Zealand: A population-based study. Br. J. Dermatol. 2015, 173, 835–837. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Chao, P.; Coomarasamy, C.; Mathy, J.A. Epidemiology and survival of Merkel cell carcinoma in New Zealand: A population-based study between 2000 and 2015 with international comparison. Australas J. Dermatol. 2019, 60, e284–e291. [Google Scholar] [CrossRef] [PubMed]
- Schadendorf, D.; Lebbé, C.; Zur Hausen, A.; Avril, M.F.; Hariharan, S.; Bharmal, M.; Becker, J.C. Merkel cell carcinoma: Epidemiology, prognosis, therapy and unmet medical needs. Eur. J. Cancer 2017, 71, 53–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ascoli, V.; Minelli, G.; Kanieff, M.; Frova, L.; Conti, S. Merkel cell carcinoma: A population-based study on mortality and the association with other cancers. Cancer Causes Control. 2011, 22, 1521–1527. [Google Scholar] [CrossRef] [Green Version]
- Kaae, J.; Hansen, A.V.; Biggar, R.J.; Boyd, H.A.; Moore, P.S.; Wohlfahrt, J.; Melbye, M. Merkel cell carcinoma: Incidence, mortality, and risk of other cancers. J. Natl. Cancer Inst. 2010, 102, 793–801. [Google Scholar] [CrossRef] [Green Version]
- Kukko, H.; Böhling, T.; Koljonen, V.; Tukiainen, E.; Haglund, C.; Pokhrel, A.; Sankila, R.; Pukkala, E. Merkel cell carcinoma—A population-based epidemiological study in Finland with a clinical series of 181 cases. Eur. J. Cancer 2012, 48, 737–742. [Google Scholar] [CrossRef]
- Fondain, M.; Dereure, O.; Uhry, Z.; Guizard, A.V.; Woronoff, A.S.; Colonna, M.; Molinie, F.; Bara, S.; Velten, M.; Marrer, E.; et al. Merkel cell carcinoma in France: A registries-based, comprehensive epidemiological survey. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1292–1296. [Google Scholar] [CrossRef]
- Kieny, A.; Cribier, B.; Meyer, N.; Velten, M.; Jégu, J.; Lipsker, D. Epidemiology of Merkel cell carcinoma. A population-based study from 1985 to 2013, in northeastern of France. Int. J. Cancer 2019, 144, 741–745. [Google Scholar] [CrossRef] [Green Version]
- Eisemann, N.; Waldmann, A.; Geller, A.C.; Weinstock, M.A.; Volkmer, B.; Greinert, R.; Breitbart, E.W.; Katalinic, A. Non-melanoma skin cancer incidence and impact of skin cancer screening on incidence. J. Investig. Dermatol. 2014, 134, 43–50. [Google Scholar] [CrossRef]
- Reichgelt, B.A.; Visser, O. Epidemiology and survival of Merkel cell carcinoma in the Netherlands. A population-based study of 808 cases in 1993–2007. Eur. J. Cancer 2011, 47, 579–585. [Google Scholar] [CrossRef]
- Mills, L.A.; Durrani, A.J.; Watson, J.D. Merkel cell carcinoma in South East Scotland, 1993–2003. Surgeon 2006, 4, 133–138. [Google Scholar] [CrossRef]
- Goon, P.K.; Greenberg, D.C.; Igali, L.; Levell, N.J. Merkel Cell Carcinoma: Rising incidence in the East of England. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 2052–2055. [Google Scholar] [CrossRef]
- Alsina, M.; Marcos-Gragera, R.; Capdevila, J.; Buxó, M.; Ortiz, R.M.; Barretina, P.; Vilardell, L.; Brunet, J.; Beltran, M.; Izquierdo, Á. Neuroendocrine tumors: A population-based study of incidence and survival in Girona Province, 1994–2004. Cancer Epidemiol. 2011, 35, e49–e54. [Google Scholar] [CrossRef]
- Hussain, S.K.; Sundquist, J.; Hemminki, K. Incidence trends of squamous cell and rare skin cancers in the Swedish national cancer registry point to calendar year and age-dependent increases. J. Investig. Dermatol. 2010, 130, 1323–1328. [Google Scholar] [CrossRef] [Green Version]
- Zaar, O.; Gillstedt, M.; Lindelöf, B.; Wennberg-Larkö, A.M.; Paoli, J. Merkel cell carcinoma incidence is increasing in Sweden. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1708–1713. [Google Scholar] [CrossRef]
- Fitzgerald, T.L.; Dennis, S.; Kachare, S.D.; Vohra, N.A.; Wong, J.H.; Zervos, E.E. Dramatic Increase in the Incidence and Mortality from Merkel Cell Carcinoma in the United States. Am. Surg. 2015, 81, 802–806. [Google Scholar] [CrossRef]
- Jacobs, D.; Huang, H.; Olino, K.; Weiss, S.; Kluger, H.; Judson, B.L.; Zhang, Y. Assessment of Age, Period, and Birth Cohort Effects and Trends in Merkel Cell Carcinoma Incidence in the United States. JAMA Dermatol. 2021, 157, 59–65. [Google Scholar] [CrossRef]
- Hodgson, N.C. Merkel cell carcinoma: Changing incidence trends. J. Surg. Oncol. 2005, 89, 1–4. [Google Scholar] [CrossRef]
- Freeman, M.B.; Holman, D.M.; Qin, J.; Lunsford, N.B. Merkel cell carcinoma incidence, trends, and survival rates among adults aged ≥50 years from United States Cancer Statistics. J. Am. Acad. Dermatol. 2019, 80, 1154–1156. [Google Scholar] [CrossRef]
- Van der Zwan, J.M.; Trama, A.; Otter, R.; Larrañaga, N.; Tavilla, A.; Marcos-Gragera, R.; Dei Tos, A.P.; Baudin, E.; Poston, G.; Links, T. Rare neuroendocrine tumours: Results of the surveillance of rare cancers in Europe project. Eur. J. Cancer 2013, 49, 2565–2578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mistry, K.; Levell, N.J.; Craig, P.; Steven, N.M.; Venables, Z.C. Merkel cell carcinoma. Skin Health Dis. 2021, 1, e55. [Google Scholar] [CrossRef] [PubMed]
- Akaike, T.; Nghiem, P. Scientific and clinical developments in Merkel cell carcinoma: A polyomavirus-driven, often-lethal skin cancer. J. Dermatol. Sci. 2022, 105, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Albores-Saavedra, J.; Batich, K.; Chable-Montero, F.; Sagy, N.; Schwartz, A.M.; Henson, D.E. Merkel cell carcinoma demographics, morphology, and survival based on 3870 cases: A population based study. J. Cutan Pathol. 2010, 37, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Walsh, N.M. Merkel cell carcinoma of the eyelid and periocular region: A review. Saudi J. Ophthalmol. 2021, 35, 186–192. [Google Scholar] [CrossRef]
- Gambichler, T.; Wieland, U.; Silling, S.; Dreißigacker, M.; Schaller, J.; Schulze, H.J.; Oellig, F.; Kreuter, A.; Stücker, M.; Bechara, F.G.; et al. Left-sided laterality of Merkel cell carcinoma in a German population: More than just sun exposure. J. Cancer Res. Clin. Oncol. 2017, 143, 347–350. [Google Scholar] [CrossRef]
- Go, C.C.; Kim, D.H.; Briceño, C.A. A SEER analysis of survival and prognostic factors in merkel cell carcinoma of the head and neck region. Int. J. Oral Maxillofac. Surg. 2022, 51, 314–322. [Google Scholar] [CrossRef]
- Scampa, M.; Merat, R.; Tzika, E.; Kalbermatten, D.F.; Oranges, C.M. Survival outcomes and epidemiology of Merkel cell carcinoma of the lower limb and hip: A Surveillance, Epidemiology, and End Results analysis 2000–2018. JAAD Int. 2022, 7, 13–21. [Google Scholar] [CrossRef]
- Koljonen, V.; Kukko, H.; Pukkala, E.; Sankila, R.; Böhling, T.; Tukiainen, E.; Sihto, H.; Joensuu, H. Chronic lymphocytic leukaemia patients have a high risk of Merkel-cell polyomavirus DNA-positive Merkel-cell carcinoma. Br. J. Cancer 2009, 101, 1444–1447. [Google Scholar] [CrossRef]
- Koljonen, V.; Rantanen, M.; Sahi, H.; Mellemkjær, L.; Hansen, B.T.; Chen, T.; Hemminki, K.; Pukkala, E. Joint occurrence of Merkel cell carcinoma and non-Hodgkin lymphomas in four Nordic countries. Leuk. Lymphoma 2015, 56, 3315–3319. [Google Scholar] [CrossRef]
- Walsh, N.M.; Cerroni, L. Merkel cell carcinoma: A review. J. Cutan Pathol. 2021, 48, 411–421. [Google Scholar] [CrossRef]
- Luu, Y.T.; Luo, Q.; Horner, M.J.; Shiels, M.; Engels, E.A.; Sargen, M.R. Risk of nonkeratinocyte skin cancers in people living with HIV during the era of antiretroviral therapy. J. Investig. Dermatol. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Izikson, L.; Nornhold, E.; Iyer, J.G.; Nghiem, P.; Zeitouni, N.C. Merkel cell carcinoma associated with HIV: Review of 14 patients. Aids 2011, 25, 119–121. [Google Scholar] [CrossRef]
- Li, M.; Saghafi, N.; Freymiller, E.; Basile, J.R.; Lin, Y.L. Metastatic Merkel cell carcinoma of the oral cavity in a human immunodeficiency virus-positive patient and the detection of Merkel cell polyomavirus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, e66-71. [Google Scholar] [CrossRef]
- Manganoni, M.A.; Farisoglio, C.; Tucci, G.; Venturini, M.; Marocolo, D.; Aquilano, M.C.; El-Hamad, I.; Ferrari, V.D.; Calzavara Pinton, P.G. Merkel cell carcinoma and HIV infection: A case report and review of the literature. AIDS Patient Care STDS 2007, 21, 447–451. [Google Scholar] [CrossRef]
- Wieland, U.; Kreuter, A. Merkel cell polyomavirus infection and Merkel cell carcinoma in HIV-positive individuals. Curr. Opin. Oncol. 2011, 23, 488–493. [Google Scholar] [CrossRef]
- Gambichler, T.; Schmitt, K.; Rüddel, I.; Dreibigacker, M.; Stockfleth, E.; Becker, J.C. Decreased 5-hydroxymethylcytosine immunoreactivity in primary Merkel cell carcinoma is a strong predictor for disease-specific death. Br. J. Dermatol. 2019, 181, 389–390. [Google Scholar] [CrossRef]
- Schrama, D.; Ugurel, S.; Becker, J.C. Merkel cell carcinoma: Recent insights and new treatment options. Curr. Opin. Oncol. 2012, 24, 141–149. [Google Scholar] [CrossRef]
- Tam, M.; Luu, M.; Barker, C.A.; Gharavi, N.M.; Hamid, O.; Shiao, S.L.; Nguyen, A.T.; Lu, D.J.; Ho, A.S.; Zumsteg, Z.S. Improved survival in women versus men with merkel cell carcinoma. J. Am. Acad. Dermatol. 2021, 84, 321–329. [Google Scholar] [CrossRef]
- Cullison, C.R.; Zheng, D.X.; Levoska, M.A.; Scott, J.F.; Bordeaux, J.S. Tumor primary site as a prognostic factor for Merkel cell carcinoma disease-specific death. J. Am. Acad. Dermatol. 2021, 85, 1259–1266. [Google Scholar] [CrossRef]
- Yang, A.; Wijaya, W.A.; Yang, L.; He, Y.; Cen, Y.; Chen, J. The impact of merkel cell polyomavirus positivity on prognosis of merkel cell carcinoma: A systematic review and meta-analysis. Front Oncol. 2022, 12, 1020805. [Google Scholar] [CrossRef]
- Ferrándiz-Pulido, C.; Gómez-Tomás, A.; Llombart, B.; Mendoza, D.; Marcoval, J.; Piaserico, S.; Baykal, C.; Bouwes-Bavinck, J.N.; Rácz, E.; Kanitakis, J.; et al. Clinicopathological features, MCPyV status and outcomes of Merkel cell carcinoma in solid-organ transplant recipients: A retrospective, multicentre cohort study. J Eur. Acad. Dermatol. Venereol. 2022, 36, 1991–2001. [Google Scholar] [CrossRef] [PubMed]
- Sundqvist, B.; Sihto, H.; von Willebrand, M.; Böhling, T.; Koljonen, V. LRIG1 is a positive prognostic marker in Merkel cell carcinoma and Merkel cell carcinoma expresses epithelial stem cell markers. Virchows Arch. 2021, 479, 1197–1207. [Google Scholar] [CrossRef] [PubMed]
- Fazio, N.; Maisonneuve, P.; Spada, F.; Gervaso, L.; Cella, C.A.; Pozzari, M.; Zerini, D.; Pisa, E.; Fumagalli, C.; Barberis, M.; et al. Nodal Merkel Cell Carcinoma with Unknown Primary Site and No Distant Metastasis: A Single-Center Series. Cancers 2022, 14, 4777. [Google Scholar] [CrossRef] [PubMed]
- Scola, N.; Wieland, U.; Silling, S.; Altmeyer, P.; Stücker, M.; Kreuter, A. Prevalence of human polyomaviruses in common and rare types of non-Merkel cell carcinoma skin cancer. Br. J. Dermatol. 2012, 167, 1315–1320. [Google Scholar] [CrossRef]
- Wieland, U.; Scola, N.; Stolte, B.; Stücker, M.; Silling, S.; Kreuter, A. No evidence for a causal role of Merkel cell polyomavirus in keratoacanthoma. J. Am. Acad. Dermatol. 2012, 67, 41–46. [Google Scholar] [CrossRef]
- Kreuter, A.; Silling, S.; Dewan, M.; Stücker, M.; Wieland, U. Evaluation of 4 recently discovered human polyomaviruses in primary cutaneous B-cell and T-cell lymphoma. Arch. Dermatol. 2011, 147, 1449–1451. [Google Scholar] [CrossRef] [Green Version]
- Du-Thanh, A.; Dereure, O.; Guillot, B.; Foulongne, V. Merkel cell polyomavirus: Its putative involvement in a particular subset of cutaneous lymphoma with possibly unfavorable outcome. J. Clin. Virol. 2014, 61, 161–165. [Google Scholar] [CrossRef]
- Tanio, S.; Matsushita, M.; Kuwamoto, S.; Horie, Y.; Kodani, I.; Murakami, I.; Ryoke, K.; Hayashi, K. Low prevalence of Merkel cell polyomavirus with low viral loads in oral and maxillofacial tumours or tumour-like lesions from immunocompetent patients: Absence of Merkel cell polyomavirus-associated neoplasms. Mol. Clin. Oncol. 2015, 3, 1301–1306. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country/Region | Age-Adjusted Incidence Rate * | Annual Percentage Increase (CI 95%) | Gender-Specific Incidence Rates *(CI 95%) | MCC Cases Included (n) | Surveillance Period | References | |
|---|---|---|---|---|---|---|---|
| men | women | ||||||
| Australia (Western) | 1.0 | 0.63 | 215 | 1993–2007 | [59] | ||
| Australia (Queensland) | 1.6 | 2.6% | 2.5 | 0.9 | 340 | 2006–2010 | [60] |
| Australia (Queensland) | 1.8% (0.7–2.8) | 2.99 | 0.90 | 1997–2016 | [56] | ||
| Australia (Victoria) | 2.5 | 4.2% (2.8–5.8) ** | 3.9 | 1.5 | 1095 | 1986–2016 | [61] |
| New Zealand | 0.88 | 1.05 | 0.74 | 356 | 2002–2011 | [62] | |
| New Zealand | 0.96 ° (0.88–1.04) | 1.45 times that of females (1.23–1.7) | 601 | 2000–2015 | [63] | ||
| New Zealand | 2.0% (0.4–3.7) | 1.37 | 0.95 | 1997–2016 | [56] | ||
| Europe | 0.13 °° | 1995–2002 | [64,65] | ||||
| Denmark | 0.22 | 0.2 | 0.25 | 185 | 1995–2006 | [66] | |
| Finland | 0.11 | 0.12 | 181 | 1989–2008 | [67] | ||
| France | 0.26 and 0.43 *** | 0.24 and 0.38 *** | 290 | 2006–2010 | [68] | ||
| France (Bas-Rhin) | 0.23 (0.13–0.33) | 5.14% (2.31–8.34%) | 0.18 (0.13–0.33) | 0.16 (0.12–0.21) | 111 | 2010–2013 | [69] |
| Germany | 0.40 | 0.30 | 1848 | 1988–2010 | [70] | ||
| Ireland | 0.41 (0.31–0.51) | 0.58 (0.5–0.75) | 0.28 (0.18–0.38) | 314 | 2009–2014 | [58] | |
| Italy | 0.28 (0.25–0.32) | 2001–2005 | [65] | ||||
| Netherlands | 0.17/0.35 | 808 | 1993–1997/2003–2007 | [71] | |||
| Norway | 4.0% (2.1–5.9) | 0.45 | 0.22 | 1997–2016 | [56] | ||
| Great Britain (Scotland) | 3.7% (2.0–5.5) | 0.50 | 0.44 | 1997–2016 | [56] | ||
| Great Britain (Southeast-Scotland) | 0.133 | 20 | 1993–2003 | [72] | |||
| Great Britain (England) | 0.10–0.20 | 1999–2008 | [64] | ||||
| Great Britain (East-England) | 0.21 | 0.19 | 0.24 | 73 | 2004–2013 | [73] | |
| Spain | 0.11 °° | 15 | 1994–2004 | [74] | |||
| Sweden | 0.45 (age ≥ 85 years) | 0.42 (0.41–0.43) | 0.33 (0.32–0.33) | 1990–2005 | [75] | ||
| Sweden | 0.11 to 0.19 | 73% § | 0.09 to 0.20 | 0.12 to 0.17 | 1993–2012 | [76] | |
| United States | 0.6 | 1500/y | 2009 | [64] | |||
| United States | 0.79 | 2011 | [77] | ||||
| United States | 0.7 (0.7–0.8) | 2013 | [57] | ||||
| United States | 2.7% (2.0–3.3) | 1.03 | 0.45 | 3063 | 1997–2016 | [56] | |
| US Non-Hispanic Whites | 3.0% (2.4–3.7) | 1.22 | 0.54 | 3063 | 1997–2016 | [56] | |
| United States | 0.66 (0.62–0.70) | 3720 | 2012–2016 | [78] | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silling, S.; Kreuter, A.; Gambichler, T.; Meyer, T.; Stockfleth, E.; Wieland, U. Epidemiology of Merkel Cell Polyomavirus Infection and Merkel Cell Carcinoma. Cancers 2022, 14, 6176. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14246176
Silling S, Kreuter A, Gambichler T, Meyer T, Stockfleth E, Wieland U. Epidemiology of Merkel Cell Polyomavirus Infection and Merkel Cell Carcinoma. Cancers. 2022; 14(24):6176. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14246176
Chicago/Turabian StyleSilling, Steffi, Alexander Kreuter, Thilo Gambichler, Thomas Meyer, Eggert Stockfleth, and Ulrike Wieland. 2022. "Epidemiology of Merkel Cell Polyomavirus Infection and Merkel Cell Carcinoma" Cancers 14, no. 24: 6176. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14246176