
Fish Consumption and Colorectal Cancer Risk: Meta-Analysis of Prospective Epidemiological Studies and Review of Evidence from Animal Studies

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Fish Consumption and Colorectal Cancer Risk among Humans
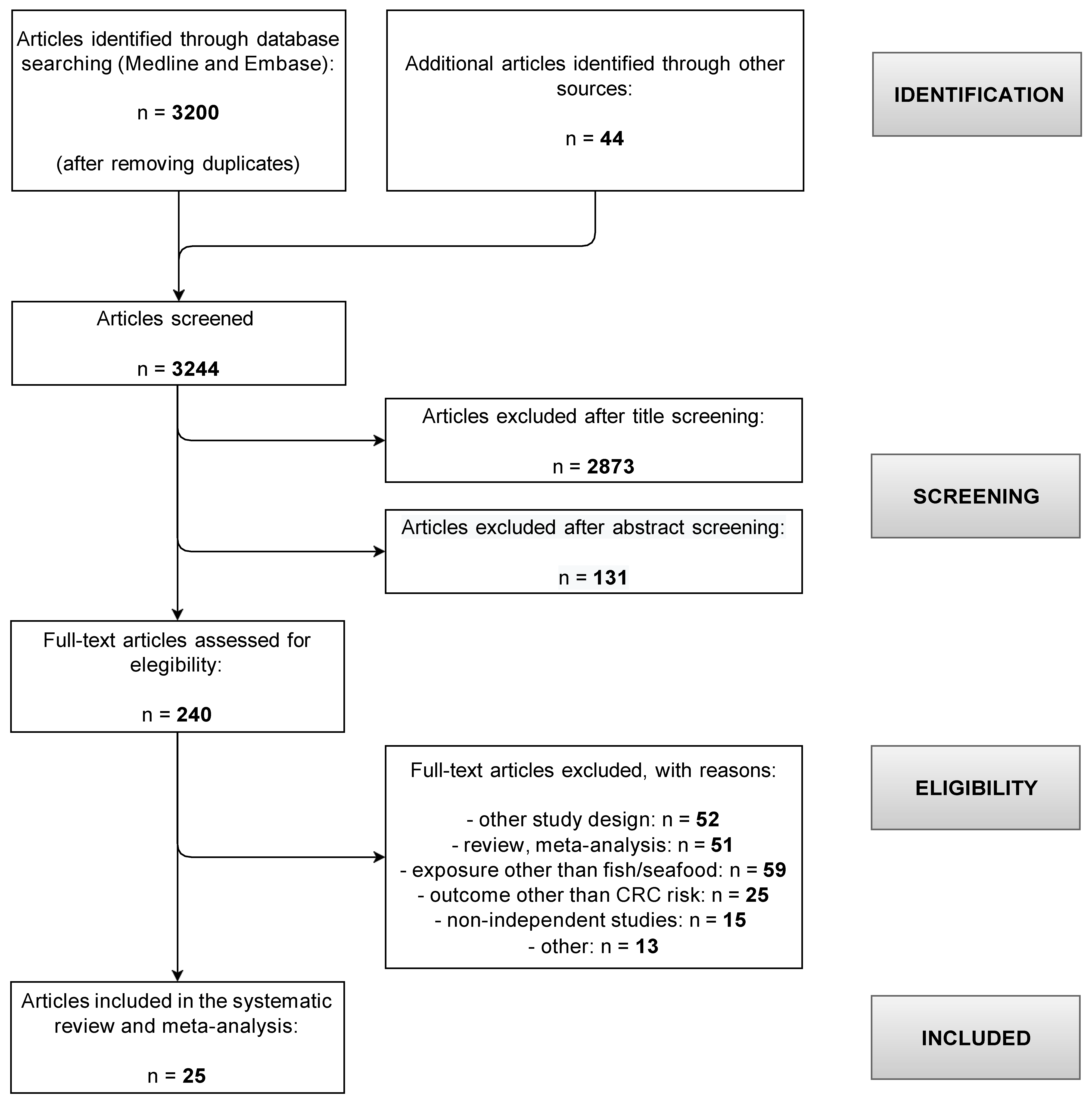
2.1.1. Literature Search and Inclusion Criteria
2.1.2. Data Extraction and Statistical Analysis
2.2. Fish and Fish-Oil Intake and Colorectal Carcinogenesis in Animal Models
3. Results
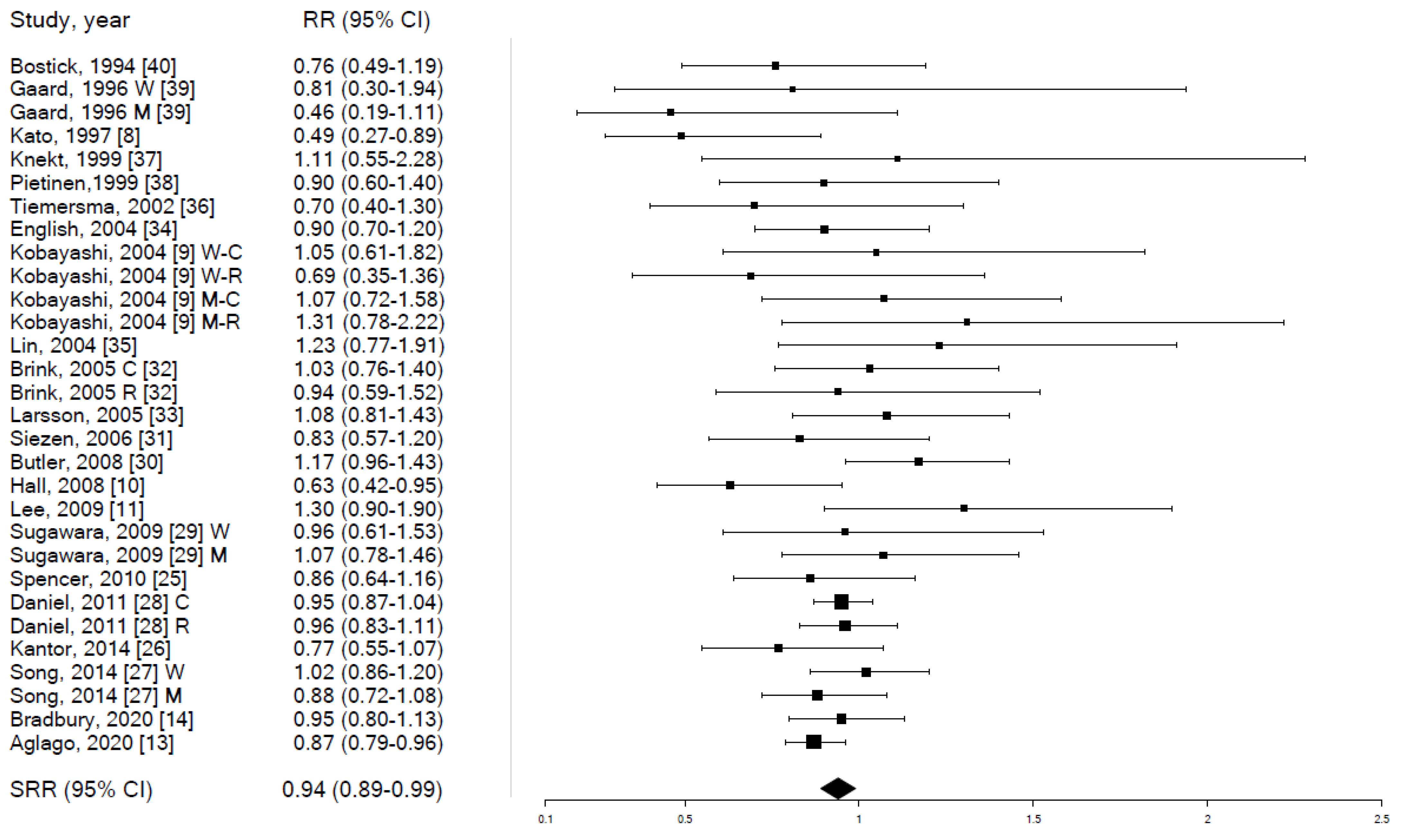
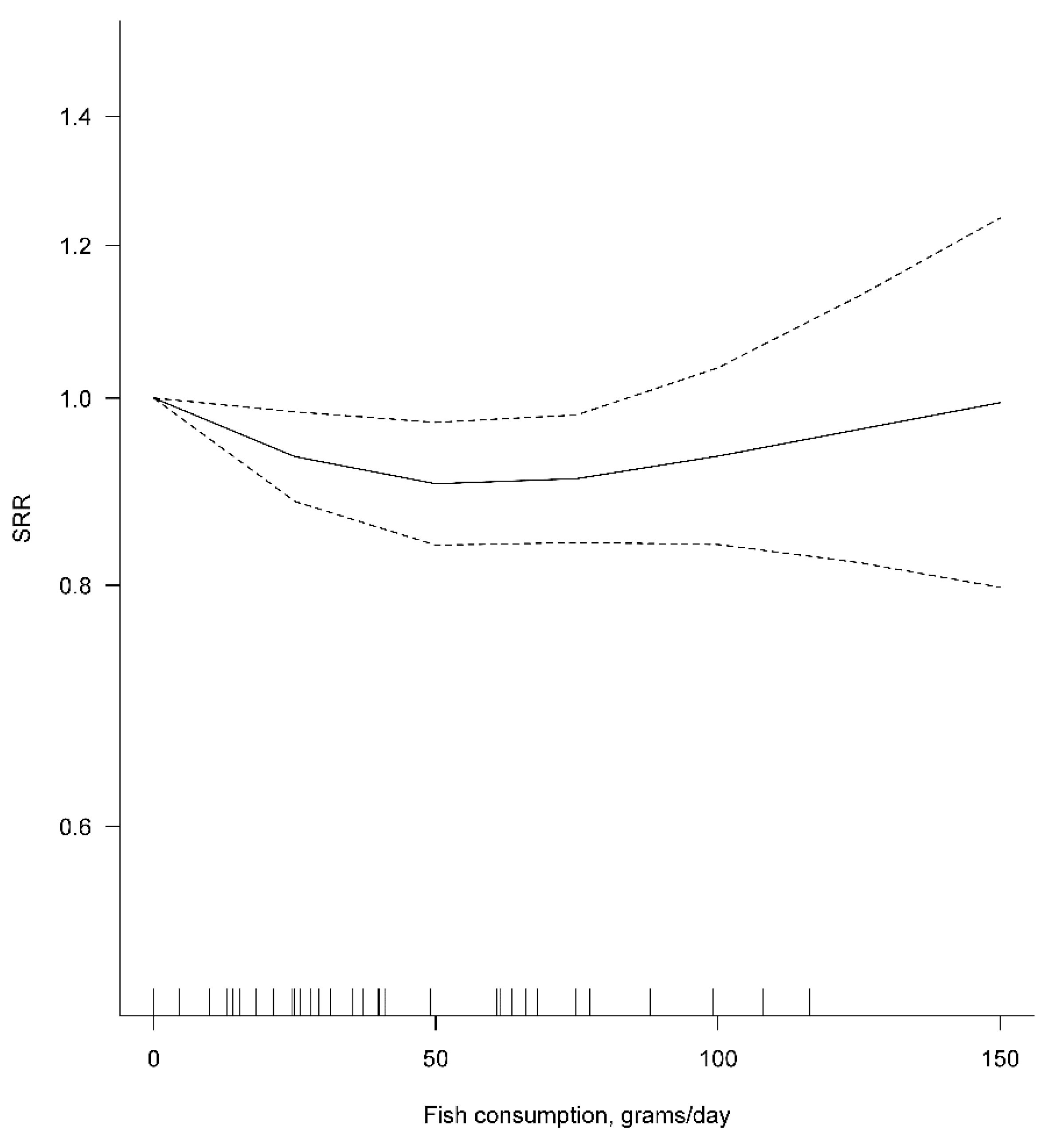
3.1. Fish Consumption and Colorectal Cancer Risk among Humans
3.2. Fish and Fish-Oil Intake and Colorectal Carcinogenesis in Animal Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Global Cancer Observatory (GCO). Colorectal Cancer Factsheet 2020. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/10_8_9-Colorectum-fact-sheet.pdf (accessed on 31 August 2021).
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity, and Cancer: A Global Perspective. Continuous Update Project (CUP): Colorectal Cancer. Available online: https://www.wcrf.org/dietandcancer/colorectal-cancer/ (accessed on 31 August 2021).
- Institute of Food Research, Norwich, UK. Nutrient Analysis of Fish and Fish Products. 2013. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/167923/Nutrient_analysis_of_fish_and_fish_products_-_Analytical_Report.pdf (accessed on 13 October 2021).
- Saedisomeolia, A.; Wood, L.G.; Garg, M.L.; Gibson, P.G.; Wark, P.A. Anti-inflammatory effects of long-chain n-3 PUFA in rhinovirus-infected cultured airway epithelial cells. Br. J. Nutr. 2009, 101, 533–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, T.Y.; Davidson, L.A.; Kim, E.; Fan, Y.Y.; Fuentes, N.R.; Triff, K.; Chapkin, R.S. Nutrient-Gene Interaction in Colon Cancer, from the Membrane to Cellular Physiology. Annu. Rev. Nutr. 2016, 36, 543–570. [Google Scholar] [CrossRef] [Green Version]
- Irún, P.; Lanas, A.; Piazuelo, E. Omega-3 Polyunsaturated Fatty Acids and Their Bioactive Metabolites in Gastrointestinal Malignancies Related to Unresolved Inflammation. A Review. Front. Pharmacol. 2019, 10, 852. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, J. Intake or Blood Levels of n-3 Polyunsaturated Fatty Acids and Risk of Colorectal Cancer: A Systematic Review and Meta-analysis of Prospective Studies. Cancer Epidemiol. Biomark. Prev. 2020, 29, 288–299. [Google Scholar] [CrossRef] [PubMed]
- Kato, I.; Akhmedkhanov, A.; Koenig, K.; Toniolo, P.G.; Shore, R.E.; Riboli, E. Prospective study of diet and female colorectal cancer: The New York University Women’s Health Study. Nutr. Cancer 1997, 28, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Tsubono, Y.; Otani, T.; Hanaoka, T.; Sobue, T.; Tsugane, S.; JPHC Study Group. Fish, long-chain n-3 polyunsaturated fatty acids, and risk of colorectal cancer in middle-aged Japanese: The JPHC study. Nutr. Cancer 2004, 49, 32–40. [Google Scholar] [CrossRef]
- Hall, M.N.; Chavarro, J.E.; Lee, I.M.; Willett, W.C.; Ma, J. A 22-year prospective study of fish, n-3 fatty acid intake, and colorectal cancer risk in men. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1136–1143. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.A.; Shu, X.O.; Yang, G.; Li, H.; Gao, Y.T.; Zheng, W. Animal origin foods and colorectal cancer risk: A report from the Shanghai Women’s Health Study. Nutr. Cancer 2009, 61, 194–205. [Google Scholar] [CrossRef]
- Vieira, A.R.; Abar, L.; Chan, D.S.M.; Vingeliene, S.; Polemiti, E.; Stevens, C.; Greenwood, D.; Norat, T. Foods and beverages and colorectal cancer risk: A systematic review and meta-analysis of cohort studies, an update of the evidence of the WCRF-AICR Continuous Update Project. Ann. Oncol. 2017, 28, 1788–1802. [Google Scholar] [CrossRef]
- Aglago, E.K.; Huybrechts, I.; Murphy, N.; Casagrande, C.; Nicolas, G.; Pischon, T.; Fedirko, V.; Severi, G.; Boutron-Ruault, M.C.; Fournier, A.; et al. Consumption of fish and long-chain n-3 polyunsaturated fatty acids is associated with reduced risk of colorectal cancer in a large European cohort. Clin. Gastroenterol. Hepatol. 2020, 18, 654–666.e6. [Google Scholar] [CrossRef]
- Bradbury, K.E.; Murphy, N.; Key, T.J. Diet and colorectal cancer in UK Biobank: A prospective study. Int. J. Epidemiol. 2020, 49, 246–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Greenland, S. Quantitative methods in the review of epidemiologic literature. Epidemiol. Rev. 1987, 9, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Greenland, S.; Longnecker, M.P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analysis. 2020. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 2 July 2021).
- The Comprehensive R Archive Network (CRAN). Package Dosresmeta. Available online: https://cran.r-project.org/web/packages/dosresmeta/dosresmeta.pdf (accessed on 9 June 2021).
- Bamia, C.; Lagiou, P.; Buckland, G.; Grioni, S.; Agnoli, C.; Taylor, A.J.; Dahm, C.C.; Overvad, K.; Olsen, A.; Tjønneland, A.; et al. Mediterranean diet and colorectal cancer risk: Results from a European cohort. Eur. J. Epidemiol. 2013, 28, 317–328. [Google Scholar] [CrossRef]
- Engeset, D.; Andersen, V.; Hjartåker, A.; Lund, E. Consumption of fish and risk of colon cancer in the Norwegian Women and Cancer (NOWAC) study. Br. J. Nutr. 2007, 98, 576–582. [Google Scholar] [CrossRef] [Green Version]
- Murff, H.J.; Shu, X.O.; Li, H.; Dai, Q.; Kallianpur, A.; Yang, G.; Cai, H.; Wen, W.; Gao, Y.T.; Zheng, W. A prospective study of dietary polyunsaturated fatty acids and colorectal cancer risk in Chinese women. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2283–2291. [Google Scholar] [CrossRef] [Green Version]
- Spencer, E.A.; Key, T.J.; Appleby, P.N.; Dahm, C.C.; Keogh, R.H.; Fentiman, I.S.; Akbaraly, T.; Brunner, E.J.; Burley, V.; Cade, J.E.; et al. Meat, poultry and fish and risk of colorectal cancer: Pooled analysis of data from the UK dietary cohort consortium. Cancer Causes Control 2010, 21, 1417–1425. [Google Scholar] [CrossRef] [Green Version]
- Kantor, E.D.; Lampe, J.W.; Peters, U.; Vaughan, T.L.; White, E. Long-chain omega-3 polyunsaturated fatty acid intake and risk of colorectal cancer. Nutr. Cancer 2014, 66, 716–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, M.; Chan, A.T.; Fuchs, C.S.; Ogino, S.; Hu, F.B.; Mozaffarian, D.; Ma, J.; Willett, W.C.; Giovannucci, E.L.; Wu, K. Dietary intake of fish, ω-3 and ω-6 fatty acids and risk of colorectal cancer: A prospective study in U.S. men and women. Int. J. Cancer 2014, 135, 2413–2423. [Google Scholar] [CrossRef] [PubMed]
- Daniel, C.R.; Cross, A.J.; Graubard, B.I.; Hollenbeck, A.R.; Park, Y.; Sinha, R. Prospective investigation of poultry and fish intake in relation to cancer risk. Cancer Prev. Res. 2011, 4, 1903–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugawara, Y.; Kuriyama, S.; Kakizaki, M.; Nagai, M.; Ohmori-Matsuda, K.; Sone, T.; Hozawa, A.; Nishino, Y.; Tsuji, I. Fish consumption and the risk of colorectal cancer: The Ohsaki Cohort Study. Br. J. Cancer 2009, 101, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Butler, L.M.; Wang, R.; Koh, W.P.; Yu, M.C. Prospective study of dietary patterns and colorectal cancer among Singapore Chinese. Br. J. Cancer 2008, 99, 1511–1516. [Google Scholar] [CrossRef] [Green Version]
- Siezen, C.L.; Bueno-de-Mesquita, H.B.; Peeters, P.H.; Kram, N.R.; van Doeselaar, M.; van Kranen, H.J. Polymorphisms in the genes involved in the arachidonic acid-pathway, fish consumption and the risk of colorectal cancer. Int. J. Cancer 2006, 119, 297–303. [Google Scholar] [CrossRef] [Green Version]
- Brink, M.; Weijenberg, M.P.; de Goeij, A.F.; Roemen, G.M.; Lentjes, M.H.; de Bruïne, A.P.; Goldbohm, R.A.; van den Brandt, P.A. Meat consumption and K-ras mutations in sporadic colon and rectal cancer in The Netherlands Cohort Study. Br. J. Cancer 2005, 92, 1310–1320. [Google Scholar] [CrossRef] [Green Version]
- Larsson, S.C.; Rafter, J.; Holmberg, L.; Bergkvist, L.; Wolk, A. Red meat consumption and risk of cancers of the proximal colon, distal colon and rectum: The Swedish Mammography Cohort. Int. J. Cancer 2005, 113, 829–834. [Google Scholar] [CrossRef]
- English, D.R.; MacInnis, R.J.; Hodge, A.M.; Hopper, J.L.; Haydon, A.M.; Giles, G.G. Red meat, chicken, and fish consumption and risk of colorectal cancer. Cancer Epidemiol. Biomark. Prev. 2004, 13, 1509–1514. [Google Scholar]
- Lin, J.; Zhang, S.M.; Cook, N.R.; Lee, I.M.; Buring, J.E. Dietary fat and fatty acids and risk of colorectal cancer in women. Am. J. Epidemiol. 2004, 160, 1011–1022. [Google Scholar] [CrossRef] [Green Version]
- Tiemersma, E.W.; Kampman, E.; Bueno de Mesquita, H.B.; Bunschoten, A.; van Schothorst, E.M.; Kok, F.J.; Kromhout, D. Meat consumption, cigarette smoking, and genetic susceptibility in the etiology of colorectal cancer: Results from a Dutch prospective study. Cancer Causes Control 2002, 13, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Knekt, P.; Järvinen, R.; Dich, J.; Hakulinen, T. Risk of colorectal and other gastro-intestinal cancers after exposure to nitrate, nitrite and N-nitroso compounds: A follow-up study. Int. J. Cancer 1999, 80, 852–856. [Google Scholar] [CrossRef]
- Pietinen, P.; Malila, N.; Virtanen, M.; Hartman, T.J.; Tangrea, J.A.; Albanes, D.; Virtamo, J. Diet and risk of colorectal cancer in a cohort of Finnish men. Cancer Causes Control 1999, 10, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Gaard, M.; Tretli, S.; Løken, E.B. Dietary factors and risk of colon cancer: A prospective study of 50,535 young Norwegian men and women. Eur. J. Cancer Prev. 1996, 5, 445–454. [Google Scholar] [PubMed]
- Bostick, R.M.; Potter, J.D.; Kushi, L.H.; Sellers, T.A.; Steinmetz, K.A.; McKenzie, D.R.; Gapstur, S.M.; Folsom, A.R. Sugar, meat, and fat intake, and non-dietary risk factors for colon cancer incidence in Iowa women (United States). Cancer Causes Control 1994, 5, 38–52. [Google Scholar] [CrossRef] [PubMed]
- Reddy, B.S.; Maruyama, H. Effect of dietary fish oil on azoxymethane-induced colon carcinogenesis in male F344 rats. Cancer Res. 1986, 46, 3367–3370. [Google Scholar] [PubMed]
- Reddy, B.S.; Sugie, S. Effect of different levels of omega-3 and omega-6 fatty acids on azoxymethane-induced colon carcinogenesis in F344 rats. Cancer Res. 1988, 48, 6642–6647. [Google Scholar]
- Minoura, T.; Takata, T.; Sakaguchi, M.; Takada, H.; Yamamura, M.; Hioki, K.; Yamamoto, M. Effect of dietary eicosapentaenoic acid on azoxymethane-induced colon carcinogenesis in rats. Cancer Res. 1988, 48, 4790–4794. [Google Scholar]
- Deschner, E.E.; Lytle, J.S.; Wong, G.; Ruperto, J.F.; Newmark, H.L. The effect of dietary omega-3 fatty acids (fish oil) on azoxymethanol-induced focal areas of dysplasia and colon tumor incidence. Cancer 1990, 66, 2350–2356. [Google Scholar] [CrossRef]
- Reddy, B.S.; Burill, C.; Rigotty, J. Effect of diets high in omega-3 and omega-6 fatty acids on initiation and postinitiation stages of colon carcinogenesis. Cancer Res. 1991, 51, 487–491. [Google Scholar]
- Takahashi, M.; Minamoto, T.; Yamashita, N.; Yazawa, K.; Sugimura, T.; Esumi, H. Reduction in formation and growth of 1,2-dimethylhydrazine-induced aberrant crypt foci in rat colon by docosahexaenoic acid. Cancer Res. 1993, 53, 2786–2789. [Google Scholar] [PubMed]
- Takahashi, M.; Minamoto, T.; Yamashita, N.; Kato, T.; Yazawa, K.; Esumi, H. Effect of docosahexaenoic acid on azoxymethane-induced colon carcinogenesis in rats. Cancer Lett. 1994, 83, 177–184. [Google Scholar] [CrossRef]
- Takahashi, M.; Fukutake, M.; Isoi, T.; Fukuda, K.; Sato, H.; Yazawa, K.; Sugimura, T.; Wakabayashi, K. Suppression of azoxymethane-induced rat colon carcinoma development by a fish oil component, docosahexaenoic acid (DHA). Carcinogenesis 1997, 18, 1337–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, M.; Totsuka, Y.; Masuda, M.; Fukuda, K.; Oguri, A.; Yazawa, K.; Sugimura, T.; Wakabayashi, K. Reduction in formation of 2-amino-1-methyl-6-phenylimidazo [4,5-b]pyridine (PhIP)-induced aberrant crypt foci in the rat colon by docosahexaenoic acid (DHA). Carcinogenesis 1997, 18, 1937–1941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, W.L.; Chapkin, R.S.; Lupton, J.R. Fish oil blocks azoxymethane-induced rat colon tumorigenesis by increasing cell differentiation and apoptosis rather than decreasing cell proliferation. J. Nutr. 1998, 128, 491–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, C.V.; Hirose, Y.; Indranie, C.; Reddy, B.S. Modulation of experimental colon tumorigenesis by types and amounts of dietary fatty acids. Cancer Res. 2001, 61, 1927–1933. [Google Scholar]
- Oshima, M.; Takahashi, M.; Oshima, H.; Tsutsumi, M.; Yazawa, K.; Sugimura, T.; Nishimura, S.; Wakabayashi, K.; Taketo, M.M. Effects of docosahexaenoic acid (DHA) on intestinal polyp development in Apc delta 716 knockout mice. Carcinogenesis 1995, 16, 2605–2607. [Google Scholar] [CrossRef]
- Paulsen, J.E.; Elvsaas, I.K.; Steffensen, I.L.; Alexander, J. A fish oil derived concentrate enriched in eicosapentaenoic and docosahexaenoic acid as ethyl ester suppresses the formation and growth of intestinal polyps in the Min mouse. Carcinogenesis 1997, 18, 1905–1910. [Google Scholar] [CrossRef] [Green Version]
- Petrik, M.B.; McEntee, M.F.; Chiu, C.H.; Whelan, J. Antagonism of arachidonic acid is linked to the antitumorigenic effect of dietary eicosapentaenoic acid in Apc(Min/+) mice. J. Nutr. 2000, 130, 1153–1158. [Google Scholar] [CrossRef]
- Fini, L.; Piazzi, G.; Daoud, Y.; Selgrad, M.; Maegawa, S.; Garcia, M.; Fogliano, V.; Romano, M.; Graziani, G.; Vitaglione, P.; et al. Chemoprevention of intestinal polyps in ApcMin/+ mice fed with western or balanced diets by drinking annurca apple polyphenol extract. Cancer Prev. Res. 2011, 4, 907–915. [Google Scholar] [CrossRef] [Green Version]
- Piazzi, G.; D’Argenio, G.; Prossomariti, A.; Lembo, V.; Mazzone, G.; Candela, M.; Biagi, E.; Brigidi, P.; Vitaglione, P.; Fogliano, V.; et al. Eicosapentaenoic acid free fatty acid prevents and suppresses colonic neoplasia in colitis-associated colorectal cancer acting on Notch signaling and gut microbiota. Int. J. Cancer 2014, 135, 2004–2013. [Google Scholar] [CrossRef] [PubMed]
- Steppeler, C.; Sødring, M.; Egelandsdal, B.; Kirkhus, B.; Oostindjer, M.; Alvseike, O.; Gangsei, L.E.; Hovland, E.M.; Pierre, F.; Paulsen, J.E. Effects of dietary beef, pork, chicken and salmon on intestinal carcinogenesis in A/J Min/+ mice. PLoS ONE 2017, 12, e0176001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masuda, J.; Umemura, C.; Yokozawa, M.; Yamauchi, K.; Seko, T.; Yamashita, M.; Yamashita, Y. Dietary Supplementation of Selenoneine-Containing Tuna Dark Muscle Extract Effectively Reduces Pathology of Experimental Colorectal Cancers in Mice. Nutrients 2018, 10, 1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannizzo, F., Jr.; Broitman, S.A. Postpromotional effects of dietary marine or safflower oils on large bowel or pulmonary implants of CT-26 in mice. Cancer Res. 1989, 49, 4289–4294. [Google Scholar] [PubMed]
- Iigo, M.; Nakagawa, T.; Ishikawa, C.; Iwahori, Y.; Asamoto, M.; Yazawa, K.; Araki, E.; Tsuda, H. Inhibitory effects of docosahexaenoic acid on colon carcinoma 26 metastasis to the lung. Br. J. Cancer 1997, 75, 650–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, I.; Iigo, M.; Ishikawa, C.; Kuhara, T.; Asamoto, M.; Kunimoto, T.; Moore, M.A.; Yazawa, K.; Araki, E.; Tsuda, H. Inhibitory effects of oleic and docosahexaenoic acids on lung metastasis by colon-carcinoma-26 cells are associated with reduced matrix metalloproteinase-2 and -9 activities. Int. J. Cancer 1997, 73, 607–612. [Google Scholar] [CrossRef]
- Iwamoto, S.; Senzaki, H.; Kiyozuka, Y.; Ogura, E.; Takada, H.; Hioki, K.; Tsubura, A. Effects of fatty acids on liver metastasis of ACL-15 rat colon cancer cells. Nutr. Cancer 1998, 31, 143–150. [Google Scholar] [CrossRef]
- Griffini, P.; Fehres, O.; Klieverik, L.; Vogels, I.M.; Tigchelaar, W.; Smorenburg, S.M.; Van Noorden, C.J. Dietary omega-3 polyunsaturated fatty acids promote colon carcinoma metastasis in rat liver. Cancer Res. 1998, 58, 3312–3319. [Google Scholar]
- Gutt, C.N.; Brinkmann, L.; Mehrabi, A.; Fonouni, H.; Müller-Stich, B.P.; Vetter, G.; Stein, J.M.; Schemmer, P.; Büchler, M.W. Dietary omega-3-polyunsaturated fatty acids prevent the development of metastases of colon carcinoma in rat liver. Eur. J. Nutr. 2007, 46, 279–285. [Google Scholar] [CrossRef]
- Hawcroft, G.; Volpato, M.; Marston, G.; Ingram, N.; Perry, S.L.; Cockbain, A.J.; Race, A.D.; Munarini, A.; Belluzzi, A.; Loadman, P.M.; et al. The omega-3 polyunsaturated fatty acid eicosapentaenoic acid inhibits mouse MC-26 colorectal cancer cell liver metastasis via inhibition of PGE2-dependent cell motility. Br. J. Pharmacol. 2012, 166, 1724–1737. [Google Scholar] [CrossRef] [Green Version]
- Sødring, M.; Gunnes, G.; Paulsen, J.E. Spontaneous initiation, promotion and progression of colorectal cancer in the novel A/J Min/+ mouse. Int. J. Cancer 2016, 138, 1936–1946. [Google Scholar] [CrossRef] [PubMed]
- Wennberg, M.; Tornevi, A.; Johansson, I.; Hörnell, A.; Norberg, M.; Bergdahl, I.A. Diet and lifestyle factors associated with fish consumption in men and women: A study of whether gender differences can result in gender-specific confounding. Nutr. J. 2012, 11, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tani, S.; Kawauchi, K.; Atsumi, W.; Matsuo, R.; Ashida, T.; Imatake, K.; Suzuki, Y.; Yagi, T.; Takahashi, A.; Matsumoto, N.; et al. Association among daily fish intake, white blood cell count, and healthy lifestyle behaviors in an apparently healthy Japanese population: Implication for the anti-atherosclerotic effect of fish consumption. Heart Vessels 2021, 36, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Femia, A.P.; Caderni, G. Rodent models of colon carcinogenesis for the study of chemopreventive activity of natural products. Planta Med. 2008, 74, 1602–1607. [Google Scholar] [CrossRef] [Green Version]
- Reddy, B.S. Studies with the azoxymethane-rat preclinical model for assessing colon tumor development and chemoprevention. Environ. Mol. Mutagen. 2004, 44, 26–35. [Google Scholar] [CrossRef]
- Song, M.; Chan, A.T. Environmental Factors, Gut Microbiota, and Colorectal Cancer Prevention. Clin. Gastroenterol. Hepatol. 2019, 17, 275–289. [Google Scholar] [CrossRef]
- Yang, P.; Jiang, Y.; Fischer, S.M. Prostaglandin E3 metabolism and cancer. Cancer Lett. 2014, 348, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Piazzi, G.; Prossomariti, A.; Baldassarre, M.; Montagna, C.; Vitaglione, P.; Fogliano, V.; Biagi, E.; Candela, M.; Brigidi, P.; Balbi, T.; et al. A Mediterranean Diet Mix Has Chemopreventive effects in a murine model of colorectal cancer modulating apoptosis and the gut microbiota. Front. Oncol. 2019, 9, 140. [Google Scholar] [CrossRef] [Green Version]
- Thorning, T.K.; Bertram, H.C.; Bonjour, J.P.; de Groot, L.; Dupont, D.; Feeney, E.; Ipsen, R.; Lecerf, J.M.; Mackie, A.; McKinley, M.C.; et al. Whole dairy matrix or single nutrients in assessment of health effects: Current evidence and knowledge gaps. Am. J. Clin. Nutr. 2017, 105, 1033–1045. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Country | Study Name | Study Size (a) | Men (%) | Age Range (at Cohort Inception) | Study Length | Follow-Up Time (Years) | Fish Consumption Assessment (b) | No. Cases | Anatomic Site Distribution of Colorectal Cancers | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Colon | Rectal | Ns or Other | ||||||||||
| Aglago, 2020 [13] (c) | Europe | European Prospective Investigation into Cancer and Nutrition (EPIC) | 476,160 | 29.9% | 25–70 | 1992–ns | median 14.9 | intake + frequency | 6291 | 66.7% | 33.3% | 0.0% |
| Bradbury, 2020 [14] | UK | UK biobank study | 475,581 | 46.0% | 40–69 | 2006–2014 | mean 5.7 | intake + frequency | 2609 | 66.8% | 33.2% | 0.0% |
| Kantor, 2014 [26] | USA | VITamins And Lifestyle cohort | 68,109 | 49.0% | 50–70 | 2001–2008 | mean 6.7 | frequency | 488 | 63.7% | 26.3% | 10.0% |
| Song, 2014 [27] | USA | Nurses’ Health Study | 76,386 | 0.0% | 30–55 | 1976–2010 | mean 14.8 | intake | 1469 | 76.9% | 21.1% | 2.0% |
| Health Professionals Follow-up Study | 47,143 | 100.0% | 40–75 | 1986–2010 | 987 | 65.2% | 21.8% | 13.0% | ||||
| Bamia, 2013 [22] (c) | Europe | European Prospective Investigation into Cancer and Nutrition | 480,308 | 30.0% | 25–70 | 1992–2010 | mean 11.6 | intake | 4355 | 63.2% | 36.8% | 0.0% |
| Daniel, 2011 [28] | USA | National Institutes of Health (NIH)-AARP Diet and Health Study | 492,186 | 59.6% | 50–71 | 1995–2006 | mean 9.1 | intake | 7143 | 71.3% | 26.4% | 2.3% |
| Spencer, 2010 [25] | UK | UK Dietary Cohort Consortium | 2575 | 45.9% | ns | 1985–2006 | ns | intake | 579 | ns | ns | 100.0% |
| Murff, 2009 [24] (d) | China | Shanghai Women’s Health Study | 73,243 | 0.0% | 40–70 | 1996–2007 | ns | intake | 396 | ns | ns | 100.0% |
| Lee, 2009 [11] (d) | China | Shanghai Women’s Health Study | 74,942 | 0.0% | 45–65 | 1997–2005 | mean 7.4 | intake | 394 | 59.9% | 40.1% | 0.0% |
| Sugawara, 2009 [29] | Japan | Ohsaki National Health Insurance Cohort Study | 39,498 | 47.7% | 40–79 | 1995–2003 | mean 7.7 | intake | 566 | 59.5% | 40.5% | 0.0% |
| Butler, 2008 [30] | Singapore | Singapore Chinese Health Study | 61,321 | ns | 45–74 | 1993–ns | mean 9.8 | intake | 961 | 61.5% | 38.5% | 0.0% |
| Hall, 2008 [10] | USA | Physicians’ Health Study | 21,406 | 100.0% | ns | 1982–2006 | ns | frequency | 500 | 77.6% | 22.4% | 0.0% |
| Engeset, 2007 [23] (c) | Norway | The Norwegian Women and Cancer | 64,168 | 0.0% | 40–71 | 1991–2004 | ns | intake | 254 | ns | ns | 100.0% |
| Siezen, 2006 [31] | The Netherlands | Monitoring Project on Cardiovascular Disease Risk Factors + Diagnostisch Onderzoek Mammacarcinoom | 160 | ns | ns | 1976–2003 | ns | frequency | 160 | ns | ns | 100.0% |
| Brink, 2005 [32] | The Netherlands | The Netherlands Cohort Study | 2948 | 48.4% | 55–69 | 1986–1993 | mean 5.0 | intake | 608 | 73.7% | 26.3% | 0.0% |
| Larsson, 2005 [33] | Sweden | The Swedish Mammography Cohort | 61,433 | 0.0% | 40–75 | 1987–2003 | mean 13.9 | frequency | 733 | 53.1% | 31.4% | 15.5% |
| English, 2004 [34] | Australia | The Melbourne Collaborative Cohort Study | 37,112 | 39.5% | 27–75 | 1990–2003 | mean 9.0 | frequency | 451 | 62.5% | 37.3% | 0.2% |
| Kobayashi, 2004 [9] | Japan | The Japan Public Health Center-based prospective study | 116,194 | 49.3% | 40–69 | 1990–1999 | ns | intake | 705 | ns | ns | 100.0% |
| Lin, 2004 [35] | USA | Women’s Health Study | 37,547 | 0.0% | 45–ns | 1993–2003 | mean 8.7 | frequency | 202 | 80.2% | 19.8% | 0.0% |
| Tiemersma, 2002 [36] | The Netherlands | Monitoring Project on Cardiovascular Disease Risk Factors | 102 | 54.9% | 20–59 | 1987–1998 | mean 8.5 | frequency | 102 | 61.8% | ns | ns |
| Knekt, 1999 [37] | Finland | Cohort assembled within the Mobile Health Clinic of the Social Insurance Institution | 9985 | 52.8% | 15–99 | 1967–1990 | ns | intake | 189 | 38.6% | ns | 61.4% |
| Pietinen, 1999 [38] | Finland | The Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study | 27,111 | 100.0% | 50–69 | 1985–1995 | mean 8.0 | intake | 185 | ns | ns | ns |
| Kato, 1997 [8] | USA | New York University Women’s Health Study | 14,727 | 0.0% | 34–65 | 1985–1994 | mean 7.1 | frequency | 100 | 84.0% | 16.0% | 0.0% |
| Gaard, 1996 [39] | Norway | Cohort assembled within the Norwegian National Health Screening Service | 50,535 | 50.1% | 20–54 | 1977–ns | mean 11.4 | frequency | 143 | 100.0% | 0.0% | 0.0% |
| Bostick, 1994 [40] | USA | Iowa Women’s Health Study | 35,216 | 0.0% | 55–69 | 1986–1990 | mean 4.8 | frequency | 212 | 100.0% | 0.0% | 0.0% |
| N Studies | SRR | Lower 95% CI | Upper 95% CI | p-Value | I2 | |
|---|---|---|---|---|---|---|
| Colorectal cancer | 22 | 0.94 | 0.89 | 0.99 | 0.023 | 11.7% |
| women | 13 | 0.95 | 0.87 | 1.05 | 0.310 | 13.9% |
| men | 10 | 0.91 | 0.82 | 1.01 | 0.088 | 27.2% |
| Colon cancer | 15 | 0.94 | 0.88 | 1.01 | 0.089 | 12.9% |
| women | 7 | 1.02 | 0.88 | 1.19 | 0.763 | 12.5% |
| men | 4 | 1.02 | 0.85 | 1.22 | 0.866 | 0.0% |
| Rectal cancer | 13 | 0.94 | 0.87 | 1.03 | 0.173 | 0.0% |
| women | 5 | 0.99 | 0.79 | 1.26 | 0.966 | 0.0% |
| men | 3 | 0.90 | 0.57 | 1.43 | 0.663 | 63.2% |
| N Studies | SRR (for an Increase by 50 g/day) | Lower 95% CI | Upper 95% CI | p-Value | I2 | p-Value for Non-Linearity | |
|---|---|---|---|---|---|---|---|
| Colorectal cancer | 7 | 0.96 | 0.92 | 0.99 | 0.021 | 0.0% | 0.071 |
| women | 5 | 0.95 | 0.90 | 1.01 | 0.078 | 0.0% | 0.880 |
| men | 6 | 0.97 | 0.92 | 1.02 | 0.188 | 0.0% | 0.280 |
| Colon cancer | 6 | 0.96 | 0.92 | 1.01 | 0.140 | 0.0% | 0.991 |
| Rectal cancer | 6 | 0.95 | 0.89 | 1.02 | 0.174 | 0.0% | 0.248 |
| Experimental Model | Dietary Intervention and Duration of Treatment | Effects on Carcinogenesis | Reference |
|---|---|---|---|
| AOM-induced rats | Diets containing Menhaden or Corn oils | Reduction in CRC in rats fed Menhaden Oil. | Reddy, 1986 [41] |
| -+AOM-induced rats | Different levels of FO or CO in the diet. | Reduction in CRC in rats fed high FO. | Reddy, 1988 [42] |
| AOM-induced rats | Diets containing EPA or LA | Reduction in colon carcinogenesis in the EPA group. | Minoura, 1988 [43] |
| AOM-induced mice | Commercial preparations of FO or CO. | Reduction in dysplastic areas and carcinogenesis in the FO group. | Deschner, 1990 [44] |
| AOM-induced rats | Diets containing FO and/or CO. | Reduction in colon carcinogenesis in rats fed high FO. | Reddy, 1991 [45] |
| DMH-induced rats | DHA (0.7 mL by gavage) 5 times a wk. | Reduction in ACF. | Takahashi, 1993 [46] |
| AOM-induced rats | DHA (0.7 mL of by gavage) twice a wk. | Slight non-significant reduction of CRC. | Takahashi, 1994 [47] |
| Significant reduction in ACF. | |||
| AOM-induced rats | DHA (1 mL by gavage) 5 times a wk. | Significant reduction in ACF and in CRC. | Takahashi, 1997a [48] |
| 2-amino-1-methyl-6-phenylimidazo [4,5-b]pyridine (PhIP)-induced rats | DHA (1 mL by gavage) 5 times a wk. | Reduction in ACF. | Takahashi, 1997b [49] |
| AOM-induced rats | Diet supplemented with FO or CO; cellulose or pectin also tested. | FO reduced CRC. | Chang, 1998 [50] |
| AOM-induced rats | FO vs. HFML. | Reduction in carcinogenesis and ACF in rats fed FO. | Rao, 2001 [51] |
| Apc∆716 mice of both sexes | Diet with 3% DHA for 7 wks. | Reduction in SI polyps, only in female mice fed DHA. | Oshima, 1995 [52] |
| Min mice mutated in Apc | Diet containing a commercial FO preparation. | Reduction in SI tumors in treated mice. | Paulsen, 1997 [53] |
| Min mice mutated in Apc | Diets containing EPA (1.5%) or different PUFA for 8 wks. | Reduction in SI tumors in the EPA group. | Petrik, 2000 [54] |
| Min mice mutated in Apc | EPA-FFA fed for 12 wks. | Reduction in polyp number in SI and colon. | Fini, 2011 [55] |
| Mice treated with AOM/DSS to induce CAC | EPA-FFA in the diet tested in the initiation and post-initiation phases. | Reduction in tumorigenesis | Piazzi, 2014 [56] |
| A/J Min/+ mice of both sexes | Salmon compared with beef or chicken muscles fed from weaning for 10 wks. | Salmon muscle decreased tumor load and size in the SI. | Steppler, 2017 [57] |
| Mice treated with AOM-DSS to induce CAC | Tuna muscle extract rich in Selenoeine fed for 14 wks. | Reduction in carcinogenesis. | Masuda, 2018 [58] |
| Experimental Model | Dietary Intervention and Duration of Treatment | Effects on Colon Cancer and Metastasis | Reference |
|---|---|---|---|
| Mice inoculated with CT-26 tumor cells | Diets containing fish or safflower oils fed for 30 days before and after CT-26 transplantation. | Fish oil (FO) reduced tumor growth and pulmonary colonization. | Cannizzo, 1989 [59] |
| Mice s.c. implanted with Co 26 Lu tumor cells | Diets containing EPA and DHA during and after cancer cell transplantation. | Inhibition of tumor growth and decrease in lung metastatic nodules. | Iigo, 1997 [60] |
| Mice s.c. implanted with Co 26 Lu tumor cells | Diets containing EPA, DHA, LA, or oleic acid (OA) from day 5 for a total of 3 wks after cell implantation. | EPA, DHA, and OA reduced metastasis. Tumor cells treated with DHA showed a very low potential for lung colony formation when injected i.v. | Suzuki, 1997 [61] |
| Rats inoculated with ACL-15 tumor cells | Diets containing EPA, LA, or PA. ACL-15 tumor cells inoculated at 6 wks and rats sacrificed at 9 wks. | EPA reduced metastatic foci in liver. EPA and PA diet groups had smaller liver metastatic foci. | Iwamoto,1998 [62] |
| Rats injected (via portal vein) with CC531 tumor cells | Diets containing FO or safflower oil for 3 wks before CC531 inoculation until sacrifice after 1 or 3 wks. | FO increased metastasis (number and size) at 1 wk after implantation; both FO and the safflower oil diets increased metastasis 3 wks after implantation. | Griffini, 1998 [63] |
| Rats injected (into the spleen) with CC531 tumor cells | Diets containing PUFA or coconut oil in the diet 3 days before and 28 days after CC 531 injection. | Reduction in tumor growth in the PUFA group. | Gutt, 2007 [64] |
| Mice injected (into the spleen) with MC-26 tumor cells | Diet containing EPA-FFA. Feeding 2 wks before and after cell injection. | EPA-FFA administration caused a reduced MC-26 liver tumor burden. | Hawcroft, 2012 [65] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caini, S.; Chioccioli, S.; Pastore, E.; Fontana, M.; Tortora, K.; Caderni, G.; Masala, G. Fish Consumption and Colorectal Cancer Risk: Meta-Analysis of Prospective Epidemiological Studies and Review of Evidence from Animal Studies. Cancers 2022, 14, 640. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14030640
Caini S, Chioccioli S, Pastore E, Fontana M, Tortora K, Caderni G, Masala G. Fish Consumption and Colorectal Cancer Risk: Meta-Analysis of Prospective Epidemiological Studies and Review of Evidence from Animal Studies. Cancers. 2022; 14(3):640. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14030640
Chicago/Turabian StyleCaini, Saverio, Sofia Chioccioli, Elisa Pastore, Miriam Fontana, Katia Tortora, Giovanna Caderni, and Giovanna Masala. 2022. "Fish Consumption and Colorectal Cancer Risk: Meta-Analysis of Prospective Epidemiological Studies and Review of Evidence from Animal Studies" Cancers 14, no. 3: 640. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14030640