
Simultaneous Resection of Pancreatic Neuroendocrine Tumors with Synchronous Liver Metastases: Safety and Oncological Efficacy

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
Operative Procedures and Postoperative Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cloyd, J.M.; Poultsides, G.A. The Landmark Series: Pancreatic Neuroendocrine Tumors. Ann. Surg. Oncol. 2021, 28, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Megdanova-Chipeva, V.G.; Lamarca, A.; Backen, A.; McNamara, M.G.; Barriuso, J.; Sergieva, S.; Gocheva, L.; Mansoor, W.; Manoharan, P.; Valle, J.W. Systemic Treatment Selection for Patients with Advanced Pancreatic Neuroendocrine Tumours (PanNETs). Cancers 2020, 12, 1988. [Google Scholar] [CrossRef] [PubMed]
- Grandhi, M.S.; Lafaro, K.J.; Pawlik, T.M. Role of Locoregional and Systemic Approaches for the Treatment of Patients with Metastatic Neuroendocrine Tumors. J. Gastrointest. Surg. 2015, 19, 2273–2282. [Google Scholar] [CrossRef] [PubMed]
- Addeo, P.; d’Alessandro, A.; Averous, G.; Imperiale, A.; Faitot, F.; Goichot, B.; Bachellier, P. Macrovascular venous invasion of pancreatic neuroendocrine tumours: Impact on surgical outcomes and survival. HPB 2019, 21, 653–661. [Google Scholar] [CrossRef]
- Bruzoni, M.; Parikh, P.; Celis, R.; Are, C.; Ly, Q.P.; Meza, J.L.; Sasson, A.R. Management of the primary tumor in patients with metastatic pancreatic neuroendocrine tumor: A contemporary single-institution review. Am. J. Surg. 2009, 197, 376–381. [Google Scholar] [CrossRef]
- D’Souza, M.A.; Valdimarsson, V.T.; Campagnaro, T.; Cauchy, F.; Chatzizacharias, N.A.; D’Hondt, M.; Dasari, B.; Ferrero, A.; Franken, L.C.; Fusai, G.; et al. Hepatopancreatoduodenectomy a controversial treatment for bile duct and gallbladder cancer from a European perspective. HPB 2020, 22, 1339–1348. [Google Scholar] [CrossRef]
- Gaujoux, S.; Gonen, M.; Tang, L.; Klimstra, D.; Brennan, M.F.; D’Angelica, M.; Dematteo, R.; Allen, P.J.; Jarnagin, W.; Fong, Y. Synchronous resection of primary and liver metastases for neuroendocrine tumors. Ann. Surg. Oncol. 2012, 19, 4270–4277. [Google Scholar] [CrossRef]
- Kianmanesh, R.; Sauvanet, A.; Hentic, O.; Couvelard, A.; Levy, P.; Vilgrain, V.; Ruszniewski, P.; Belghiti, J. Two-step surgery for synchronous bilobar liver metastases from digestive endocrine tumors: A safe approach for radical resection. Ann. Surg. 2008, 247, 659–665. [Google Scholar] [CrossRef]
- Kleine, M.; Schrem, H.; Vondran, F.W.; Krech, T.; Klempnauer, J.; Bektas, H. Extended surgery for advanced pancreatic endocrine tumours. Br. J. Surg. 2012, 99, 88–94. [Google Scholar] [CrossRef]
- Heidenreich, B.M.; Kemp Bohan, P.M.; Flor, R.J.; Bader, J.O.; Vreeland, T.J.; O’Connor, V.V.; Nelson, D.W. Examining Perioperative Risk Associated with Simultaneous Resection of Primary Neuroendocrine Tumors and Synchronous Hepatic Metastases. World J. Surg. 2021, 45, 531–542. [Google Scholar] [CrossRef]
- Birnbaum, D.J.; Turrini, O.; Vigano, L.; Russolillo, N.; Autret, A.; Moutardier, V.; Capussotti, L.; Le Treut, Y.P.; Delpero, J.R.; Hardwigsen, J. Surgical management of advanced pancreatic neuroendocrine tumors: Short-term and long-term results from an international multi-institutional study. Ann. Surg. Oncol. 2015, 22, 1000–1007. [Google Scholar] [CrossRef] [PubMed]
- Schurr, P.G.; Strate, T.; Rese, K.; Kaifi, J.T.; Reichelt, U.; Petri, S.; Kleinhans, H.; Yekebas, E.F.; Izbicki, J.R. Aggressive surgery improves long-term survival in neuroendocrine pancreatic tumors: An institutional experience. Ann. Surg. 2007, 245, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Bassi, C.; Marchegiani, G.; Dervenis, C.; Sarr, M.; Abu Hilal, M.; Adham, M.; Allen, P.; Andersson, R.; Asbun, H.J.; Besselink, M.G.; et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years After. Surgery 2017, 161, 584–591. [Google Scholar] [CrossRef] [Green Version]
- Wente, M.N.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; Traverso, L.W.; et al. Delayed gastric emptying (DGE) after pancreatic surgery: A suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007, 142, 761–768. [Google Scholar] [CrossRef]
- Wente, M.N.; Veit, J.A.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; et al. Postpancreatectomy hemorrhage (PPH): An International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007, 142, 20–25. [Google Scholar] [CrossRef]
- Ricci, C.; Partelli, S.; Landoni, L.; Rinzivillo, M.; Ingaldi, C.; Andreasi, V.; Nessi, C.; Muffatti, F.; Fontana, M.; Tamburrino, D.; et al. Sporadic non-functioning pancreatic neuroendocrine tumours: Multicentre analysis. Br. J. Surg. 2021, 108, 811–816. [Google Scholar] [CrossRef]
- Prakash, L.; Bhosale, P.; Cloyd, J.; Kim, M.; Parker, N.; Yao, J.; Dasari, A.; Halperin, D.; Aloia, T.; Lee, J.E.; et al. Role of Fluorouracil, Doxorubicin, and Streptozocin Therapy in the Preoperative Treatment of Localized Pancreatic Neuroendocrine Tumors. J. Gastrointest. Surg. 2017, 21, 155–163. [Google Scholar] [CrossRef]
- Cloyd, J.M.; Omichi, K.; Mizuno, T.; Kawaguchi, Y.; Tzeng, C.D.; Conrad, C.; Chun, Y.S.; Aloia, T.A.; Katz, M.H.G.; Lee, J.E.; et al. Preoperative Fluorouracil, Doxorubicin, and Streptozocin for the Treatment of Pancreatic Neuroendocrine Liver Metastases. Ann. Surg. Oncol. 2018, 25, 1709–1715. [Google Scholar] [CrossRef]
- Zaidi, M.Y.; Lopez-Aguiar, A.G.; Switchenko, J.M.; Lipscomb, J.; Andreasi, V.; Partelli, S.; Gamboa, A.C.; Lee, R.M.; Poultsides, G.A.; Dillhoff, M.; et al. A Novel Validated Recurrence Risk Score to Guide a Pragmatic Surveillance Strategy After Resection of Pancreatic Neuroendocrine Tumors: An International Study of 1006 Patients. Ann. Surg. 2019, 270, 422–433. [Google Scholar] [CrossRef]
- Bertani, E.; Fazio, N.; Radice, D.; Zardini, C.; Spinoglio, G.; Chiappa, A.; Ribero, D.; Biffi, R.; Partelli, S.; Falconi, M. Assessing the role of primary tumour resection in patients with synchronous unresectable liver metastases from pancreatic neuroendocrine tumour of the body and tail. A propensity score survival evaluation. Eur. J. Surg. Oncol. 2017, 43, 372–379. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age 1 | 54 (27–80) |
| F/M | 25/26 |
| Bilairy Stent | 4 (8%) |
| Tumor localization | |
| Head | 18 (35%) |
| Left pancreas | 31 (61%) |
| Multifocal | 2 (4%) |
| Chromogranine A (µ/L) 1 | 150 (19–15,500) |
| Functional | 6 (11.7%) |
| Type of pancreatectomy | |
| Pancreaticoduodenectomy | 16 (31.3%) |
| Splenopancreatectomy | 32 (63%) |
| Total pancreatectomy | 3 (6%) |
| Operative time 1 | 465 min (180–755) |
| Venous resection | 16 (31.3%) |
| Arterial resection | 3 (6%) |
| Liver resection | |
| Exclusive resection | 23 (45%) |
| Exclusive radiofrequency ablation | 7 (13.7%) |
| Resection and radiofrequency | 21 (41.1%) |
| Associated visceral resection | 17 (18,4%) |
| Transfusions | 14 (27.4%) |
| Mortality | 1 (2%) |
| Morbidity | 27 (53%) |
| Major morbidity | 11 (22%) |
| Pancreatic fistula | 9 (17.6%) |
| Grade A | 3 |
| Grade B | 5 |
| Grade C | 1 |
| Reoperation | 5 (9.8%) |
| Tumor size (mm) 1 | 50 (20–170) |
| No lymphnodes involvement (N0) | 13 |
| Lymphnodes invovled (Npos) 1 | 3.5 (1–25) |
| Lymphnodes harvested (Ntot) 1 | 23 (5–85) |
| Ki-67% 1 | 7% (1–80) |
| G1 | 9 (18%) |
| G2 | 37 (72%) |
| G3 | 5 (9%) |
| Characteristics | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|
| Median Survival Log-Rank (Months) | HR | 95% CI | p | HR | 95% CI | p | |
| Age (years) | |||||||
| <65 vs. | 67.0 | ||||||
| >65 years | 49.0 | 2.37 | (0.89–6.25) | 0.08 | |||
| Jaundice | |||||||
| Yes | 41.0 | ||||||
| Not | 64.0 | 1.96 | (0.64–5.86) | 0.23 | |||
| Functional tumors | |||||||
| Yes | 64.0 | ||||||
| Not | 64.7 | 0.84 | (0.24–2.86) | 0.78 | |||
| Tumor site | |||||||
| Right | 67.1 | ||||||
| Left | 64.1 | 0.59 | (0.25–1.42) | 0.24 | |||
| Type of pancreatectomy | |||||||
| PD | 67.1 | ||||||
| DSP | 64.7 | 0.69 | (0.24–1.52) | 0.28 | |||
| TP | 35.2 | 5.26 | (0.91–30.4) | 0.06 | |||
| Venous Resection | |||||||
| Yes | 67.1 | ||||||
| No | 64.7 | 0.76 | (0.27–2.17) | 0.60 | |||
| Number of LM | |||||||
| 2 | 128.8 | ||||||
| >2 | 64.0 | 2.25 | (0.65–7.74) | 0.19 | |||
| Radiofrequency | |||||||
| ablation | |||||||
| Yes | 60.5 | ||||||
| Not | 119.6 | 0.67 | (0.48–1.34) | 0.40 | |||
| Transfusion | |||||||
| Yes | 64.0 | ||||||
| Not | 128.8 | 0.86 | (0.32–2.34) | 0.77 | |||
| Morbidity | |||||||
| Yes | 64.8 | ||||||
| No | 66.8 | (0.44–2.39) | 0.94 | ||||
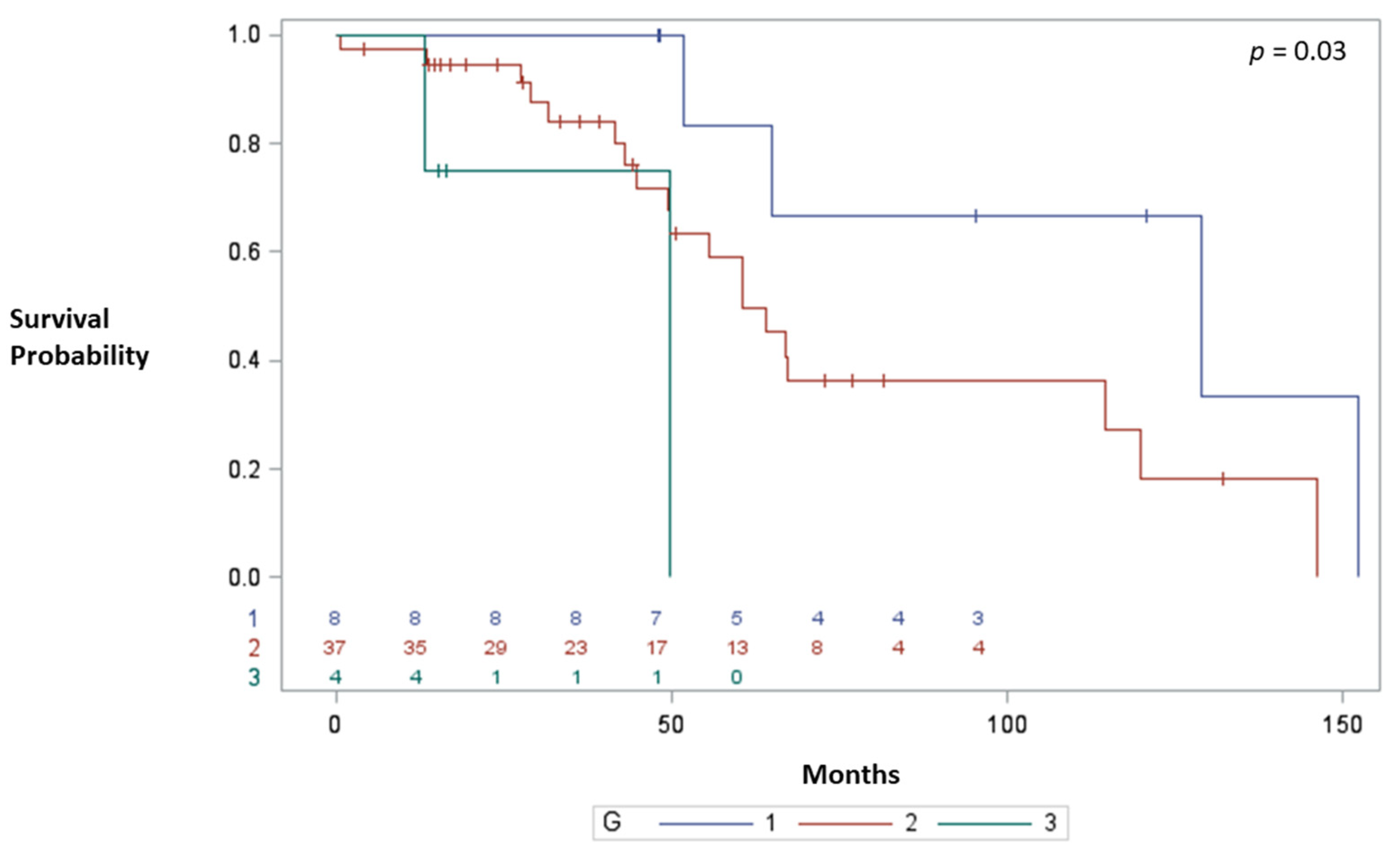
| G (WHO 2010) | |||||||
| G1 | 128.8 | ||||||
| G2 | 60.5 | 2.91 | (0.85–10.04) | 0.08 | |||
| G3 | 49.7 | 10.4 | (1.56–69.4) | 0.01 | 5.56 | (0.91–9.60) | 0.01 |
| Lymphnode invasion | |||||||
| N1 | 60.5 | ||||||
| N0 | 152.2 | 3.16 | (1.21–8.22) | 0.01 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Addeo, P.; Cusumano, C.; Goichot, B.; Guerra, M.; Faitot, F.; Imperiale, A.; Bachellier, P. Simultaneous Resection of Pancreatic Neuroendocrine Tumors with Synchronous Liver Metastases: Safety and Oncological Efficacy. Cancers 2022, 14, 727. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14030727
Addeo P, Cusumano C, Goichot B, Guerra M, Faitot F, Imperiale A, Bachellier P. Simultaneous Resection of Pancreatic Neuroendocrine Tumors with Synchronous Liver Metastases: Safety and Oncological Efficacy. Cancers. 2022; 14(3):727. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14030727
Chicago/Turabian StyleAddeo, Pietro, Caterina Cusumano, Bernard Goichot, Martina Guerra, François Faitot, Alessio Imperiale, and Philippe Bachellier. 2022. "Simultaneous Resection of Pancreatic Neuroendocrine Tumors with Synchronous Liver Metastases: Safety and Oncological Efficacy" Cancers 14, no. 3: 727. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14030727