
ICOnnecta’t: Development and Initial Results of a Stepped Psychosocial eHealth Ecosystem to Facilitate Risk Assessment and Prevention of Early Emotional Distress in Breast Cancer Survivors’ Journey

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
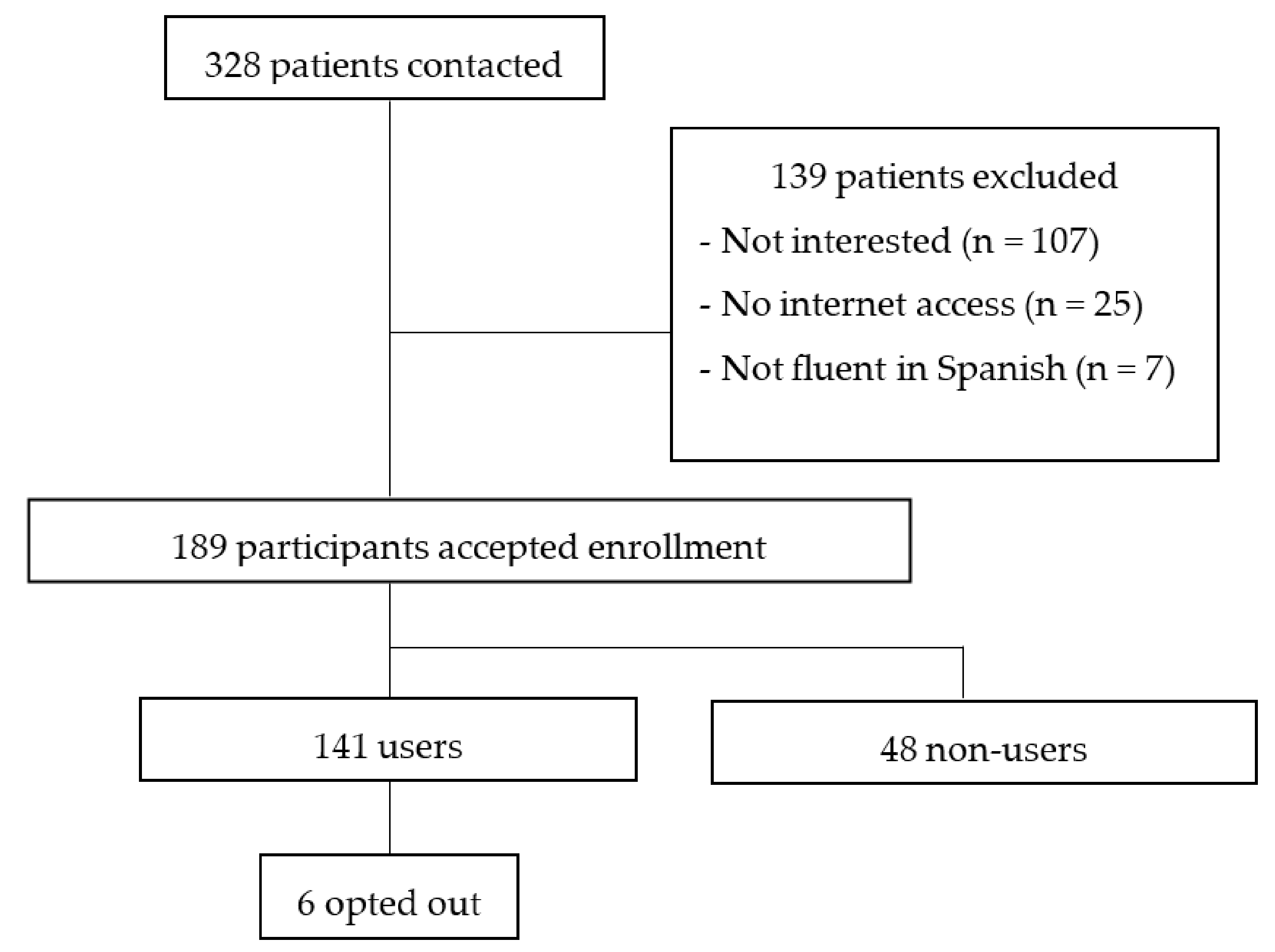
2.2. Participants
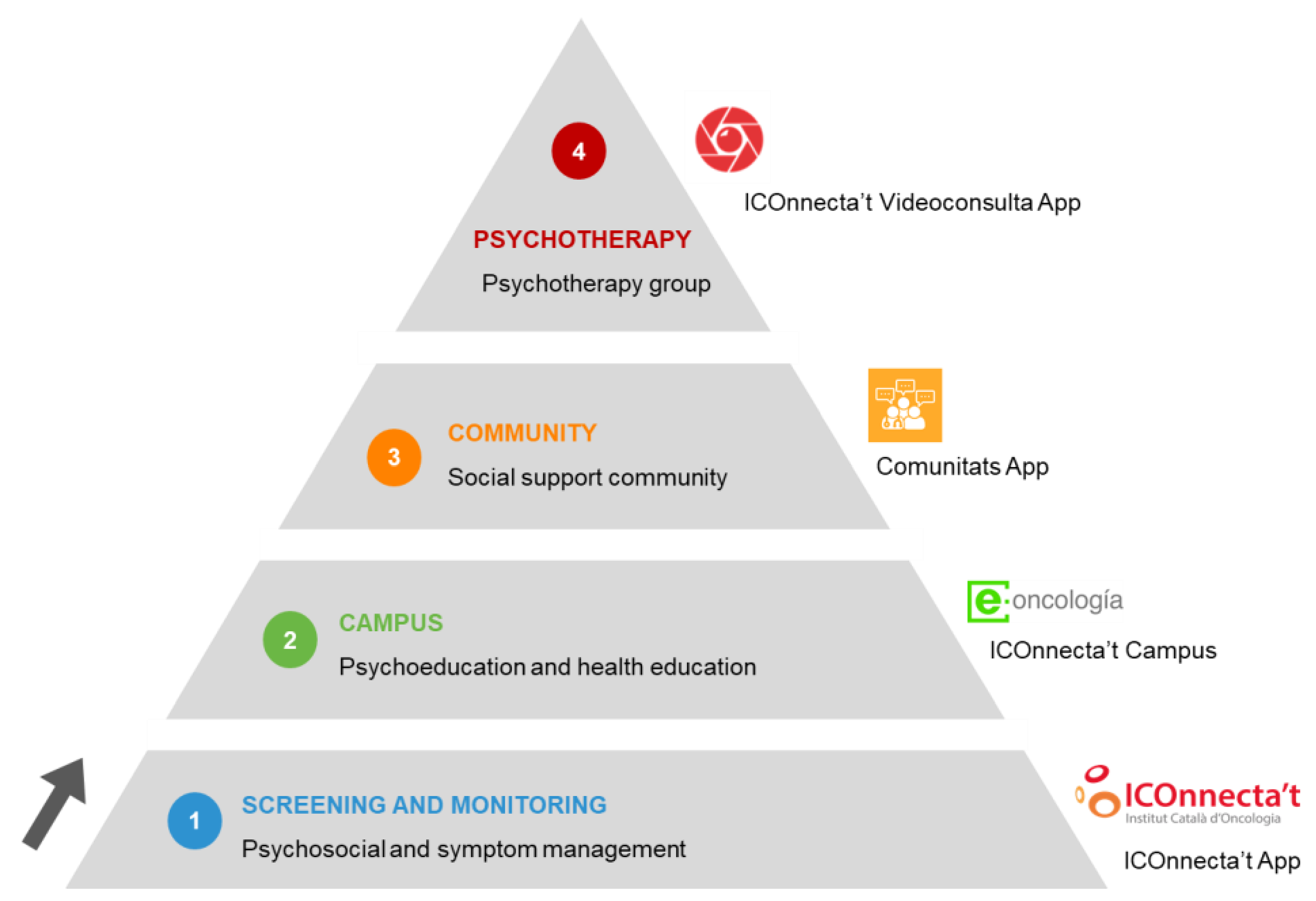
2.3. Intervention

2.4. Acceptance, Use, and Attrition of the eHealth Intervention
2.5. Instruments
2.6. Procedure
2.7. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Symptom and Psychosocial Management
3.3. Users’ Psychosocial Course in ICOnnecta’t after Diagnosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Travado, L.; Reis, J.C.; Watson, M.; Borràs, J. Psychosocial oncology care resources in Europe: A study under the European Partnership for Action Against Cancer (EPAAC). Psychooncology 2017, 26, 523–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFarland, D.C.; Shaffer, K.M.; Tiersten, A.; Holland, J. Prevalence of Physical Problems Detected by the Distress Thermometer and Problem List in Patients with Breast Cancer. Psychooncology 2018, 27, 1394–1403. [Google Scholar] [CrossRef] [PubMed]
- Giese-Davis, J.; Collie, K.; Rancourt, K.M.S.; Neri, E.; Kraemer, H.C.; Spiegel, D. Decrease in Depression Symptoms Is Associated With Longer Survival in Patients With Metastatic Breast Cancer: A Secondary Analysis. J. Clin. Oncol. 2015, 29, 413–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faller, H.; Schuler, M.; Richard, M.; Heckl, U.; Weis, J.; Küffner, R. Effects of Psycho-Oncologic Interventions on Emotional Distress and Quality of Life in Adult Patients With Cancer: Systematic Review and Meta-Analysis. J. Clin. Oncol. 2013, 31, 782–793. [Google Scholar] [CrossRef] [Green Version]
- Singer, S.; Danker, H.; Roick, J.; Einenkel, J.; Briest, S.; Spieker, H.; Dietz, A.; Hoffmann, I.; Papsdorf, K.; Meixensberger, J.; et al. Effects of stepped psychooncological care on referral to psychosocial services and emotional well-being in cancer patients: A cluster-randomized phase III trial. Psychooncology 2017, 26, 1675–1683. [Google Scholar] [CrossRef] [Green Version]
- Jansen, F.; Lissenberg-Witte, B.I.; Krebber, A.M.H.; Cuijpers, P.; de Bree, R.; Becker-Commissaris, A.; Smit, E.F.; van Straten, A.; Eeckhout, G.M.; Beekman, A.T.F.; et al. Stepped care targeting psychological distress in head and neck cancer and lung cancer patients: Which groups specifically benefit? Secondary analyses of a randomized controlled trial. Support. Care Cancer 2019, 27, 4543–4553. [Google Scholar] [CrossRef] [Green Version]
- Corbett, T.; Singh, K.; Payne, L.; Bradbury, K.; Foster, C.; Watson, E.; Richardson, A.; Little, P.; Yardley, L. Understanding acceptability of and engagement with Web-based interventions aiming to improve quality of life in cancer survivors: A synthesis of current research. Psychooncology 2018, 27, 22–33. [Google Scholar] [CrossRef]
- Penedo, F.J.; Oswald, L.B.; Kronenfeld, J.P.; Garcia, S.F.; Cella, D.; Yanez, B. The increasing value of eHealth in the delivery of patient-centred cancer care. Lancet Oncol. 2020, 21, e240–e251. [Google Scholar] [CrossRef]
- Schobel, J.; Volz, M.; Hörner, K.; Kuhn, P.; Jobst, F.; Schwab, J.D.; Ikonomi, N.; Werle, S.D.; Fürstberger, A.; Hoenig, K.; et al. Supporting Medical Staff from Psycho-Oncology with Smart Mobile Devices: Insights into the Development Process and First Results. Int. J. Environ. Res. Public Health 2021, 18, 5092. [Google Scholar] [CrossRef]
- Cho, Y.; Zhang, H.; Harris, M.R.; Gong, Y.; Smith, E.L.; Jiang, Y. Acceptance and use of home-based electronic symptom self-reporting systems in patients with cancer: Systematic review. J. Med. Internet Res. 2021, 23, e24638. [Google Scholar] [CrossRef]
- Cox, A.; Lucas, G.; Marcu, A.; Piano, M.; Grosvenor, W.; Mold, F.; Maguire, R.; Ream, E. Cancer survivors’ experience with telehealth: A systematic review and thematic synthesis. J. Med. Internet Res. 2017, 19, e11. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F. User Acceptance of Information Technology: Toward a Unified View. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, S.; Hanlon, P.; O’Donnell, C.A.; Garcia, S.; Glanville, J.; Mair, F.S. Understanding factors affecting patient and public engagement and recruitment to digital health interventions: A systematic review of qualitative studies. BMC Med. Inform. Decis. Mak. 2016, 16, 120. [Google Scholar] [CrossRef] [Green Version]
- Eysenbach, G. The law of attrition. J. Med. Internet Res. 2005, 7, e11. [Google Scholar] [CrossRef]
- Matis, J.; Svetlak, M.; Slezackova, A.; Svoboda, M.; Šumec, R. Mindfulness-Based Programs for Patients With Cancer via eHealth and Mobile Health: Systematic Review and Synthesis of Quantitative Research. J. Med. Internet Res. 2020, 22, e20709. [Google Scholar] [CrossRef]
- Meyerowitz-Katz, G.; Ravi, S.; Arnolda, L.; Feng, X.; Maberly, G.; Astell-Burt, T. Rates of attrition and dropout in app-based interventions for chronic disease: Systematic review and meta-analysis. J. Med. Internet Res. 2020, 22, e20283. [Google Scholar] [CrossRef]
- Lleras de Frutos, M.; Casellas-Grau, A.; Sumalla, E.C.; Gracia, M.; Borràs, J.M.; Ochoa Arnedo, C. A systematic and comprehensive review of internet use in cancer patients: Psychological factors. Psychooncology 2020, 29, 6–16. [Google Scholar] [CrossRef]
- Wang, Y.; Lin, Y.; Chen, J.; Wang, C.; Hu, R.; Wu, Y. Effects of Internet-based psycho-educational interventions on mental health and quality of life among cancer patients: A systematic review and meta-analysis. Support. Care Cancer 2020, 28, 2541–2552. [Google Scholar] [CrossRef]
- Xu, A.; Wang, Y.; Wu, X. Effectiveness of e-health based self-management to improve cancer-related fatigue, self-efficacy and quality of life in cancer patients: Systematic review and meta-analysis. J. Adv. Nurs. 2019, 75, 3434–3447. [Google Scholar] [CrossRef]
- Hauffman, A.; Alfonsson, S.; Bill-Axelson, A.; Bergkvist, L.; Forslund, M.; Mattsson, S.; von Essen, L.; Nygren, P.; Igelström, H.; Johansson, B. Cocreated internet-based stepped care for individuals with cancer and concurrent symptoms of anxiety and depression: Results from the U-CARE AdultCan randomized controlled trial. Psychooncology 2020, 29, 2012–2018. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 Statement: Defining Standard Protocol Items for Clinical Trials. Ann. Intern. Med. 2013, 158, 200. [Google Scholar] [CrossRef] [Green Version]
- Ochoa-Arnedo, C.; Medina, J.C.; Flix-Valle, A.; Anastasiadou, D. E-health ecosystem with integrated and stepped psychosocial services for breast cancer survivors: Study protocol of a multicentre randomised controlled trial. BMJ Open 2021, 11, e041548. [Google Scholar] [CrossRef]
- Ochoa-Arnedo, C.; Flix-Valle, A.; Medina, J.C.; Escriche, E.; Rodríguez, A.; Villanueva, C.; Sumalla, E.C.; Alabèrnia-Segura, M.; Prats, C.; Corral, M.J.; et al. Programa E-Health ICOnnecta’t: Un ecosistema para fomentar el bienestar en cáncer a través de la propuesta europea ONCOMMUN. Psicooncología 2020, 17, 41–58. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Institute (U.S.). Common Terminology Criteria for Adverse Events (CTCAE); Version 5.0; U.S. Department of Health and Human Services: Washington, DC, USA, 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 5 February 2022).
- Harju, E.; Michel, G.; Roser, K. A systematic review on the use of the emotion thermometer in individuals diagnosed with cancer. Psychooncology 2019, 28, 1803–1818. [Google Scholar] [CrossRef] [Green Version]
- Gil, F.; Grassi, L.; Travado, L.; Tomamichel, M.; Gonzalez, J.R.; Zanotti, P.; Lluch, P.; Hollenstein, M.F.; Maté, J.; Magnani, K.; et al. Use of distress and depression thermometers to measure psychosocial morbidity among southern European cancer patients. Support. Care Cancer 2005, 13, 600–606. [Google Scholar] [CrossRef]
- Requena, G.C.; Martín, X.P.; Baró, M.S.; Moncayo, F.L.G. Discriminación del malestar emocional en pacientes oncológicos utilizando la escala de ansiedad y depresión hospitalaria (HADS). Ansiedad Estres 2009, 15, 217–229. [Google Scholar]
- Terol-Cantero, M.C.; Cabrera-Perona, V.; Martín-Aragón, M. Revisión de estudios de la Escala de Ansiedad y Depresión Hospitalaria (HAD) en muestras españolas. An. Psicol. 2015, 31, 494. [Google Scholar] [CrossRef] [Green Version]
- Ochoa Arnedo, C.; Casellas-Grau, A. Positive Psychotherapy in Cancer: Facilitating Posttraumatic Growth in Assimilation and Accommodation of Traumatic Experience. In Comprehensive Guide to Post-Traumatic Stress Disorder; Springer International Publishing: Cham, Switzerland, 2015; pp. 1–14. [Google Scholar]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Linnemørken, L.T.B.; Granan, L.-P.; Reme, S.E. Prevalence of Posttraumatic Stress Symptoms and Associated Characteristics Among Patients With Chronic Pain Conditions in a Norwegian University Hospital Outpatient Pain Clinic. Front. Psychol. 2020, 11, 1–14. [Google Scholar] [CrossRef]
- Costa-Requena, G.; Gil Moncayo, F.L. Crecimiento postraumático en pacientes oncológicos. Análisis Modif. Conduct. 2007, 33, 148. [Google Scholar] [CrossRef]
- Mazor, Y.; Gelkopf, M.; Mueser, K.T.; Roe, D. Posttraumatic Growth in Psychosis. Front. Psychiatry 2016, 7, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badia, X.; Schiaffino, A.; Alonso, J.; Herdman, M. Using the EuroQoI 5-D in the Catalan general population: Feasibility and construct validity. Qual. Life Res. 1998, 7, 311–322. [Google Scholar] [CrossRef]
- Szende, A.; Janssen, B.; Cabases, J. (Eds.) Self-Reported Population Health: An International Perspective based on EQ-5D; Springer Netherlands: Dordrecht, The Netherlands, 2014; ISBN 978-94-007-7595-4. [Google Scholar]
- Costa Requena, G.; Salamero, M.; Gil, F. Validación del cuestionario MOS-SSS de apoyo social en pacientes con cáncer. Med. Clin. 2007, 128, 687–691. [Google Scholar] [CrossRef] [PubMed]
- R Core Team, R. A Language and Environment for Statistical Computing 2020; R Core Team: Vienna, Austria, 2020. [Google Scholar]
- Carlson, L.E.; Waller, A.; Groff, S.L.; Giese-Davis, J.; Bultz, B.D. What goes up does not always come down: Patterns of distress, physical and psychosocial morbidity in people with cancer over a one year period. Psychooncology 2013, 22, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Syrowatka, A.; Motulsky, A.; Kurteva, S.; Hanley, J.A.; Dixon, W.G.; Meguerditchian, A.N.; Tamblyn, R. Predictors of distress in female breast cancer survivors: A systematic review. Breast Cancer Res. Treat. 2017, 165, 229–245. [Google Scholar] [CrossRef] [PubMed]
- Pais-Ribeiro, J.L.; Silva, A.C. Social Support Survey With a Sample of Aged People. Psicol. Saúde Doenças 2009, 10, 163–174. [Google Scholar]
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- Nouri, S.S.; Adler-Milstein, J.; Thao, C.; Acharya, P.; Barr-Walker, J.; Sarkar, U.; Lyles, C. Patient characteristics associated with objective measures of digital health tool use in the United States: A literature review. J. Am. Med. Inform. Assoc. 2020, 27, 834–841. [Google Scholar] [CrossRef]
- Swartzman, S.; Booth, J.N.; Munro, A.; Sani, F. Posttraumatic stress disorder after cancer diagnosis in adults: A meta-analysis. Depress. Anxiety 2017, 34, 327–339. [Google Scholar] [CrossRef] [Green Version]
- Lleras de Frutos, M.; Medina, J.C.; Vives, J.; Casellas-Grau, A.; Marzo, J.L.; Borràs, J.M.; Ochoa-Arnedo, C. Video conference vs face-to-face group psychotherapy for distressed cancer survivors: A randomized controlled trial. Psychooncology 2020, 29, 1995–2003. [Google Scholar] [CrossRef]
- Ho, P.J.; Gernaat, S.A.M.; Hartman, M.; Verkooijen, H.M. Health-related quality of life in Asian patients with breast cancer: A systematic review. BMJ Open 2018, 8, e020512. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Users (n = 141) | Non-Users (n = 48) | t | X2 | p | |
|---|---|---|---|---|---|
| Age M (SD) | 52.35 (8.57) | 55.15 (9.55) | 1.90 | 0.059 | |
| Marital status n (%) | 0.87 | 0.929 | |||
| Single | 9 (6.38) | 2 (4.17) | |||
| Married/partnered | 101 (71.63) | 33 (68.75) | |||
| Divorced/separated | 6 (4.26) | 3 (6.25) | |||
| Widowed | 2 (1.42) | 1 (2.08) | |||
| Unknown | 23 (16.31) | 9 (18.75) | |||
| Education n (%) | 7.30 | 0.063 | |||
| Primary or no studies | 5 (3.55) | 2 (4.17) | |||
| Secondary | 17 (12.06) | 3 (6.25) | |||
| Tertiary | 43 (30.50) | 7 (14.58) | |||
| Unknown | 76 (53.90) | 36 (75.00) | |||
| Work status n (%) | 5.83 | 0.323 | |||
| Active | 54 (38.30) | 12 (25.00) | |||
| Passive | 13 (9.22) | 6 (12.50) | |||
| Occupational disability | 4 (2.84) | 3 (6.25) | |||
| Work leave | 21 (14.89) | 5 (10.42) | |||
| Retired | 9 (6.38) | 6 (12.50) | |||
| Unknown | 40 (28.37) | 16 (33.33) | |||
| Cancer stage n (%) | 3.77 | 0.438 | |||
| 0 | 16 (11.35) | 3 (6.25) | |||
| I | 53 (37.59) | 22 (45.83) | |||
| II | 52 (36.88) | 15 (31.25) | |||
| III | 15 (10.64) | 4 (8.33) | |||
| IV | 5 (3.55) | 4 (8.33) |
| Mean | SD | |
|---|---|---|
| HADS | 9.89 | 6.52 |
| PCL-5 | 24.6 | 15.6 |
| PTGI | 37.8 | 23.9 |
| EQ-5D-3L | 0.82 | 0.22 |
| MOS-SSS | 81.4 | 12.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medina, J.C.; Flix-Valle, A.; Rodríguez-Ortega, A.; Hernández-Ribas, R.; Lleras de Frutos, M.; Ochoa-Arnedo, C. ICOnnecta’t: Development and Initial Results of a Stepped Psychosocial eHealth Ecosystem to Facilitate Risk Assessment and Prevention of Early Emotional Distress in Breast Cancer Survivors’ Journey. Cancers 2022, 14, 974. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14040974
Medina JC, Flix-Valle A, Rodríguez-Ortega A, Hernández-Ribas R, Lleras de Frutos M, Ochoa-Arnedo C. ICOnnecta’t: Development and Initial Results of a Stepped Psychosocial eHealth Ecosystem to Facilitate Risk Assessment and Prevention of Early Emotional Distress in Breast Cancer Survivors’ Journey. Cancers. 2022; 14(4):974. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14040974
Chicago/Turabian StyleMedina, Joan C., Aida Flix-Valle, Ana Rodríguez-Ortega, Rosa Hernández-Ribas, María Lleras de Frutos, and Cristian Ochoa-Arnedo. 2022. "ICOnnecta’t: Development and Initial Results of a Stepped Psychosocial eHealth Ecosystem to Facilitate Risk Assessment and Prevention of Early Emotional Distress in Breast Cancer Survivors’ Journey" Cancers 14, no. 4: 974. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14040974