
Pre- and Post-Resection Urine Metabolic Profiles of Bladder Cancer Patients: Results of Preliminary Studies on Time Series Metabolomics Analysis


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Characteristics of the Subjects Included into Study
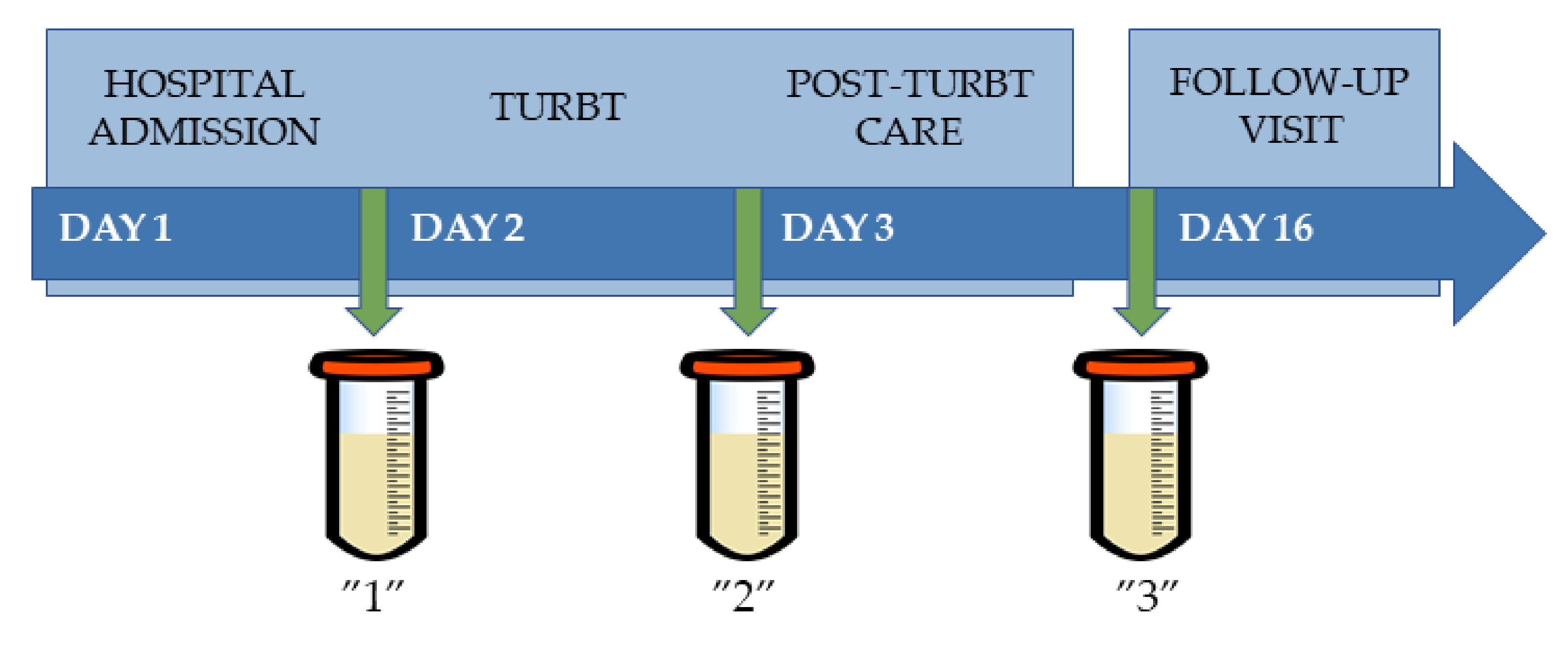
2.2. Samples’ Collection
2.3. Sample Preparation
2.3.1. HPLC-TOF/MS
2.3.2. GC-QqQ/MS
2.3.3. Quality Control Samples
2.4. Materials and Apparatus
2.4.1. HPLC-TOF/MS
2.4.2. GC-QqQ/MS
2.5. Data Processing and Statistical Analysis
2.5.1. Data Pretreatment
2.5.2. Metabolites Annotation
2.5.3. Semi-Targeted Analysis
3. Results
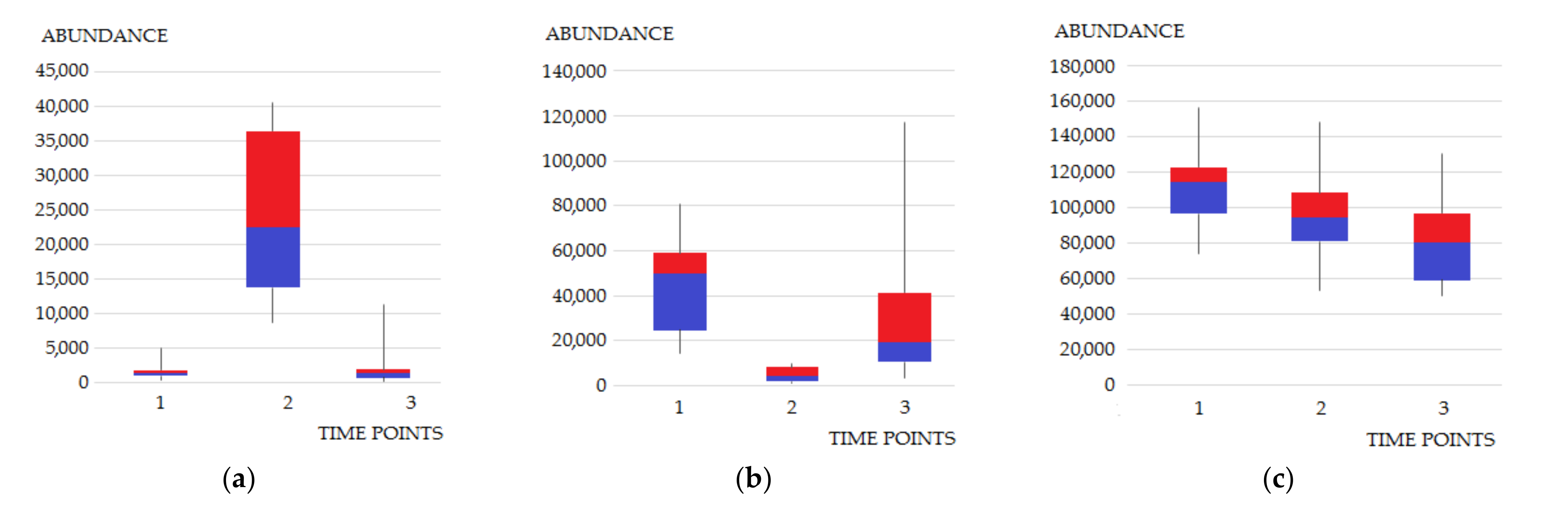
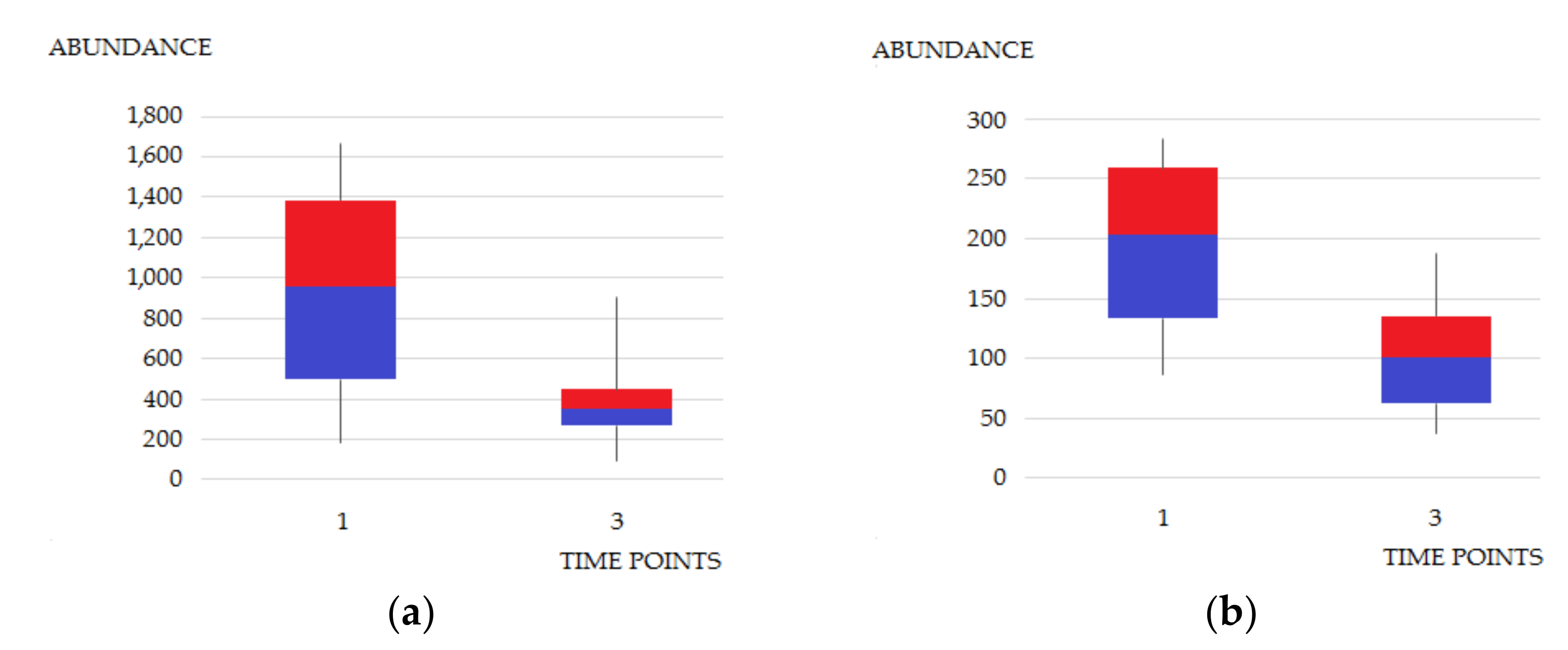
3.1. Semi-Targeted Metabolomics Analysis
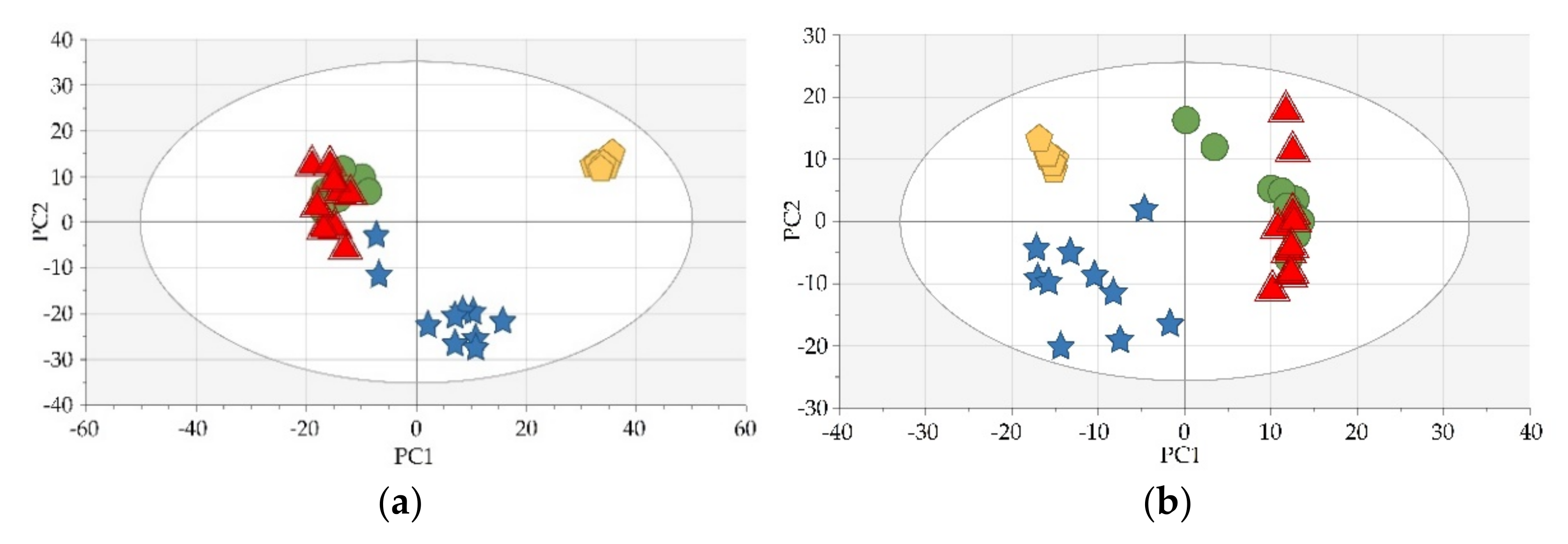
3.2. Untargeted Metabolomics Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Global Cancer Observatory. Available online: https://gco.iarc.fr/today/ (accessed on 27 October 2021).
- Ku, J.H. Bladder Cancer; Academic Press: London, UK, 2018. [Google Scholar] [CrossRef]
- Grotenhuis, A.J.; Ebben, C.W.; Aben, K.K.; Witjes, J.A.; Vrieling, A.; Vermeulen, S.H.; Kiemeney, L.A. The effect of smoking and timing of smoking cessation on clinical outcome in non–muscle-invasive bladder cancer. Urol. Oncol. 2015, 33, 65.e9–65.e17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vignoli, A.; Tenori, L.; Luchinat, C.; Saccenti, E. Age and Sex Effects on Plasma Metabolite Association Networks in Healthy Subjects. J. Proteome Res. 2018, 17, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishur, R.J.; Rea, S.L. Applications of mass spectrometry to metabolomics and metabonomics: Detection of biomarkers of aging and of age-related diseases. Mass Spectrom. Rev. 2011, 31, 70–95. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.-C.; Lan, R.S.; Brasky, T.M.; Marian, C.; Cheema, A.K.; Ressom, H.W.; Loffredo, C.A.; Pickworth, W.B.; Shields, P.G. Metabolomic profiles of current cigarette smokers. Mol. Carcinog. 2017, 56, 594–606. [Google Scholar] [CrossRef] [Green Version]
- Daghir-Wojtkowiak, E.; Wiczling, P.; Waszczuk-Jankowska, M.; Kaliszan, R.; Markuszewski, M.J. Multilevel pharmacokinetics-driven modeling of metabolomics data. Metabolomics 2017, 13, 31. [Google Scholar] [CrossRef] [Green Version]
- Wiczling, P.; Daghir-Wojtkowiak, E.; Mpanga, A.Y.; Szczesny, D.; Kaliszan, R.; Markuszewski, M.J. How to model temporal changes in nontargeted metabolomics study? A Bayesian multilevel perspective. J. Sep. Sci. 2017, 40, 4667–4676. [Google Scholar] [CrossRef]
- Maltesen, R.G.; Wimmer, R.; Rasmussen, B.S. A longitudinal serum NMR-based metabolomics dataset of ischemia-reperfusion injury in adult cardiac surgery. Sci. Data 2020, 7, 198. [Google Scholar] [CrossRef]
- Darst, B.F.; Koscik, R.L.; Hogan, K.J.; Johnson, S.C.; Engelman, C.D. Longitudinal plasma metabolomics of aging and sex. Aging 2019, 11, 1262–1282. [Google Scholar] [CrossRef]
- Amara, C.S.; Vantaku, V.; Lotan, Y.; Putluri, N. Recent advances in the metabolomic study of bladder cancer. Expert Rev. Proteom. 2019, 16, 315–324. [Google Scholar] [CrossRef]
- Torresano, L.; Nuevo-Tapioles, C.; Santacatterina, F.; Cuezva, J.M. Metabolic reprogramming and disease progression in cancer patients. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2020, 1866, 165721. [Google Scholar] [CrossRef]
- Jacyna, J.; Wawrzyniak, R.; Balayssac, S.; Gilard, V.; Malet-Martino, M.; Sawicka, A.; Kordalewska, M.; Nowicki, Ł.; Kurek, E.; Bulska, E.; et al. Urinary metabolomic signature of muscle-invasive bladder cancer: A multiplatform approach. Talanta 2019, 202, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Böhle, A.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Hernández, V.; Kaasinen, E.; Palou, J.; Rouprêt, M.; et al. EAU Guidelines on Non–Muscle-invasive Urothelial Carcinoma of the Bladder: Update 2016. Eur. Urol. 2017, 71, 447–461. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.H.C.; Patel, M.I. Transurethral resection of bladder tumour (TURBT). Transl. Androl. Urol. 2020, 9, 3056–3072. [Google Scholar] [CrossRef] [PubMed]
- Dunn, W.B.; Broadhurst, D.; Begley, P.; Zelena, E.; Francis-McIntyre, S.; Anderson, N.; Brown, M.; Knowles, J.D.; Halsall, A.; Haselden, J.N.; et al. Procedures for large-scale metabolic profiling of serum and plasma using gas chromatography and liquid chromatography coupled to mass spectrometry. Nat. Protoc. 2011, 6, 1060–1083. [Google Scholar] [CrossRef] [PubMed]
- Dudzik, D.; Barbas-Bernardos, C.; García, A.; Barbas, C. Quality assurance procedures for mass spectrometry untargeted metabolomics—A review. J. Pharm. Biomed. Anal. 2018, 147, 149–173. [Google Scholar] [CrossRef] [PubMed]
- Cone, E.J.; Caplan, Y.H.; Moser, F.; Robert, T.; Shelby, M.K.; Black, D.L. Normalization of Urinary Drug Concentrations with Specific Gravity and Creatinine. J. Anal. Toxicol. 2009, 33, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khamis, M.M.; Holt, T.; Awad, H.; El-Aneed, A.; Adamko, D.J. Comparative analysis of creatinine and osmolality as urine normalization strategies in targeted metabolomics for the differential diagnosis of asthma and COPD. Metabolomics 2018, 14, 115. [Google Scholar] [CrossRef]
- Gil-De-La-Fuente, A.; Godzien, J.; Saugar, S.; Garcia-Carmona, R.; Badran, H.; Wishart, D.S.; Barbas, C.; Otero, A. CEU Mass Mediator 3.0: A Metabolite Annotation Tool. J. Proteome Res. 2019, 18, 797–802. [Google Scholar] [CrossRef]
- Godzień, J.; Gil de la Fuente, A.; Otero, A.; Barbas, C. Metabolite Annotation and Identification. In Data Analysis for Omic Sciences: Methods and Applications; Jaumot, J., Bedia, C., Tauler, R., Eds.; Comprehensive Analytical Chemistry; Elsevier: Amsterdam, The Netherlands, 2018; Volume 82, pp. 414–445. [Google Scholar] [CrossRef]
- Lieu, E.L.; Nguyen, T.; Rhyne, S.; Kim, J. Amino acids in cancer. Exp. Mol. Med. 2020, 52, 15–30. [Google Scholar] [CrossRef]
- Wei, Z.; Liu, X.; Cheng, C.; Yu, W.; Yi, P. Metabolism of Amino Acids in Cancer. Front. Cell Dev. Biol. 2021, 8, 603837. [Google Scholar] [CrossRef]
- Cheng, Y.; Yang, X.; Deng, X.; Zhang, X.; Li, P.; Tao, J.; Qin, C.; Wei, J.; Lu, Q. Metabolomics in bladder cancer: A systematic review. Int. J. Clin. Exp. Med. 2015, 8, 11052–11063. [Google Scholar] [PubMed]
- The Human Metabolome Database. Available online: https://hmdb.ca/ (accessed on 27 October 2021).
- Loras, A.; Martínez-Bisbal, M.C.; Quintás, G.; Gil, S.; Martínez-Máñez, R.; Ruiz-Cerdá, J.L. Urinary Metabolic Signatures Detect Recurrences in Non-Muscle Invasive Bladder Cancer. Cancers 2019, 11, 914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massari, F.; Ciccarese, C.; Santoni, M.; Iacovelli, R.; Mazzucchelli, R.; Piva, F.; Scarpelli, M.; Berardi, R.; Tortora, G.; López-Beltrán, A.; et al. Metabolic phenotype of bladder cancer. Cancer Treat. Rev. 2016, 45, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Ren, W.; Huang, X.; Deng, J.; Li, T.; Yin, Y. Potential Mechanisms Connecting Purine Metabolism and Cancer Therapy. Front. Immunol. 2018, 9, 1697. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Zhong, M.; Xiong, Y.; Gao, Z.; Wu, Z.; Liu, Y.; Hong, X. Emerging roles of nucleotide metabolism in cancer development: Progress and prospect. Aging 2021, 13, 13349–13358. [Google Scholar] [CrossRef] [PubMed]
- Aird, K.M.; Zhang, R. Nucleotide metabolism, oncogene-induced senescence and cancer. Cancer Lett. 2015, 356, 204–210. [Google Scholar] [CrossRef] [Green Version]
- Xie, B.; Deng, Z.; Pan, Y.; Fu, C.; Fan, S.; Tao, Y.; Zhou, J.; Xiao, D. Post-transcriptional regulation DPC4 gene by miR-190 in colorectal cancer cells. J. Cancer Res. Ther. 2018, 14, 838–843. [Google Scholar] [CrossRef]
- He, L.; Li, H.; Wu, A.; Peng, Y.; Shu, G.; Yin, G. Functions of N6-methyladenosine and its role in cancer. Mol. Cancer 2019, 18, 176. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.-R.; Shi, L.; Wu, H.; Tang, D.-D.; Wang, S.-M.; Liu, H.-M.; Zhang, L.-R.; Song, D.-K. Urinary Modified Nucleosides as Novel Biomarkers for Diagnosis and Prognostic Monitoring of Urothelial Bladder Cancer. Tumori 2014, 100, 660–666. [Google Scholar] [CrossRef]
- Struck-Lewicka, W.; Kaliszan, R.; Markuszewski, M.J. Analysis of urinary nucleosides as potential cancer markers determined using LC–MS technique. J. Pharm. Biomed. Anal. 2014, 101, 50–57. [Google Scholar] [CrossRef]
- Alonso-Aperte, E.; González, M.P.; Póo-Prieto, R.; Varela-Moreiras, G. Folate status and S-adenosylmethionine/S-adenosylhomocysteine ratio in colorectal adenocarcinoma in humans. Eur. J. Clin. Nutr. 2008, 62, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Tian, B.; Brasier, A.; Sowers, L.C.; Zhang, K. Measurement of Histone Methylation Dynamics by One-Carbon Metabolic Isotope Labeling and High-energy Collisional Dissociation Methylation Signature Ion Detection. Sci. Rep. 2016, 6, 31537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, C.; Tu, B.P. Sink into the Epigenome: Histones as Repositories That Influence Cellular Metabolism. Trends Endocrinol. Metab. 2018, 29, 626–637. [Google Scholar] [CrossRef] [PubMed]
- Shlomi, T.; Rabinowitz, J.D. Cancer mistunes methylation. Nat. Chem. Biol. 2013, 9, 293–294. [Google Scholar] [CrossRef] [PubMed]
- Ulanovskaya, O.A.; Zuhl, A.M.; Cravatt, B.F. NNMT promotes epigenetic remodeling in cancer by creating a metabolic methylation sink. Nat. Chem. Biol. 2013, 9, 300–306. [Google Scholar] [CrossRef] [Green Version]
- Ambati, C.R.; Vantaku, V.; Donepudi, S.R.; Amara, C.S.; Ravi, S.S.; Mandalapu, A.; Perla, M.; Putluri, V.; Sreekumar, A.; Putluri, N. Measurement of methylated metabolites using liquid chromatography-mass spectrometry and its biological application. Anal. Methods 2019, 11, 49–57. [Google Scholar] [CrossRef]
- Kandimalla, R.; Van Tilborg, A.A.; Zwarthoff, E.C. DNA methylation-based biomarkers in bladder cancer. Nat. Rev. Urol. 2013, 10, 327–335. [Google Scholar] [CrossRef]
- Patel, D.; Thompson, M.D.; Manna, S.K.; Krausz, K.W.; Zhang, L.; Nilubol, N.; Gonzalez, F.J.; Kebebew, E. Unique and Novel Urinary Metabolomic Features in Malignant versus Benign Adrenal Neoplasms. Clin. Cancer Res. 2017, 23, 5302–5310. [Google Scholar] [CrossRef] [Green Version]
- Haznadar, M.; Diehl, C.M.; Parker, A.L.; Krausz, K.W.; Bowman, E.D.; Rabibhadana, S.; Forgues, M.; Bhudhisawasdi, V.; Gonzalez, F.J.; Mahidol, C.; et al. Urinary Metabolites Diagnostic and Prognostic of Intrahepatic Cholangiocarcinoma. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1704–1711. [Google Scholar] [CrossRef] [Green Version]
- Haznadar, M.; Cai, Q.; Krausz, K.W.; Bowman, E.D.; Margono, E.; Noro, R.; Thompson, M.D.; Mathe, E.; Munro, H.M.; Steinwandel, M.D.; et al. Urinary Metabolite Risk Biomarkers of Lung Cancer: A Prospective Cohort Study. Cancer Epidemiol. Biomark. Prev. 2016, 25, 978–986. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metabolite | p-Value | ||
|---|---|---|---|
| SG | CR (PUA) | CR (MS) | |
| Benzenediol | 0.78 | 0.76 | 0.75 |
| 2-deoxy-ribonic acid | 0.67 | 0.83 | 0.59 |
| Diacetylspermine | 0.08 | 0.10 | 0.08 |
| Meso-erythritol | 0.22 | 0.17 | 0.19 |
| Glutamine | 0.06 | 0.06 | 0.07 |
| Hippuric acid | 0.03 | 0.07 | 0.07 |
| Lactic acid | 0.72 | 0.78 | 0.46 |
| Pentanedioic acid | 0.06 | 0.11 | 0.02 |
| Phenylacetylglutamine | 0.06 | 0.08 | 0.11 |
| Pipecolic acid | 0.07 | 0.15 | 0.11 |
| Propanoic acid | 0.57 | 0.99 | 0.55 |
| Threonic acid | 0.10 | 0.12 | 0.12 |
| Tyrosine | 0.57 | 0.68 | 0.59 |
| Uric acid | 0.09 | 0.07 | 0.06 |
| Uridine | 0.02 | 0.04 | 0.07 |
| Metabolite | p-Value | Average Signal Intensity | Diff | SD Diff | |
|---|---|---|---|---|---|
| Before TURBT | After TURBT | ||||
| N-Acetylneuraminic acid | 0.02 | 0.58 | 0.31 | 0.27 | 0.30 |
| Androsterone 3-glucuronide | 0.03 | 0.35 | 0.25 | 0.10 | 0.11 |
| Creatine riboside | 0.01 | 0.48 | 0.19 | 0.29 | 0.25 |
| Creatinine | 0.05 | 0.51 | 0.27 | 0.24 | 0.27 |
| 5,6-Dihydrouridine | 0.03 | 0.55 | 0.30 | 0.25 | 0.26 |
| N6,N6-Dimethyl-L-Lysine | 0.04 | 0.43 | 0.28 | 0.15 | 0.20 |
| 1,3-Dimethyluracil | 0.02 | 0.54 | 0.19 | 0.35 | 0.39 |
| Glucosylgalactosyl hydroxylysine | 0.04 | 0.33 | 0.18 | 0.15 | 0.17 |
| Glutarylcarnitine | 0.02 | 0.32 | 0.11 | 0.21 | 0.24 |
| Guanidinosuccinic acid | 0.03 | 0.47 | 0.22 | 0.25 | 0.26 |
| Indolelactic acid | 0.02 | 0.24 | 0.16 | 0.08 | 0.10 |
| Indoxyl sulfate | 0.01 | 0.32 | 0.18 | 0.14 | 0.14 |
| N6-Methyladenosine | 0.01 | 0.47 | 0.23 | 0.24 | 0.24 |
| 3-Methylglutarylcarnitine | 0.02 | 0.34 | 0.10 | 0.24 | 0.27 |
| 1-Methylguanine | 0.04 | 0.52 | 0.31 | 0.21 | 0.27 |
| 1-Methylinosine | 0.02 | 0.38 | 0.19 | 0.19 | 0.19 |
| N6-Methyl-L-Lysine | 0.04 | 0.62 | 0.33 | 0.29 | 0.38 |
| Succinylcarnitine 1 | 0.01 | 0.51 | 0.27 | 0.24 | 0.22 |
| N-Methylnicotinamide | 0.04 | 0.44 | 0.23 | 0.21 | 0.28 |
| N1-Methyl-2-pyridone-5-carboxamide 2 | 0.01 | 0.64 | 0.22 | 0.42 | 0.32 |
| L-Glutamic acid | 0.04 | 0.64 | 0.40 | 0.24 | 0.32 |
| O-Sebacoylcarnitine | 0.03 | 0.54 | 0.17 | 0.37 | 0.34 |
| Succinyladenosine | 0.02 | 0.50 | 0.26 | 0.24 | 0.22 |
| Tryptophan | 0.02 | 0.25 | 0.16 | 0.09 | 0.10 |
| L-Valine 3 | 0.04 | 0.50 | 0.18 | 0.32 | 0.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacyna, J.; Kordalewska, M.; Artymowicz, M.; Markuszewski, M.; Matuszewski, M.; Markuszewski, M.J. Pre- and Post-Resection Urine Metabolic Profiles of Bladder Cancer Patients: Results of Preliminary Studies on Time Series Metabolomics Analysis. Cancers 2022, 14, 1210. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14051210
Jacyna J, Kordalewska M, Artymowicz M, Markuszewski M, Matuszewski M, Markuszewski MJ. Pre- and Post-Resection Urine Metabolic Profiles of Bladder Cancer Patients: Results of Preliminary Studies on Time Series Metabolomics Analysis. Cancers. 2022; 14(5):1210. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14051210
Chicago/Turabian StyleJacyna, Julia, Marta Kordalewska, Małgorzata Artymowicz, Marcin Markuszewski, Marcin Matuszewski, and Michał J. Markuszewski. 2022. "Pre- and Post-Resection Urine Metabolic Profiles of Bladder Cancer Patients: Results of Preliminary Studies on Time Series Metabolomics Analysis" Cancers 14, no. 5: 1210. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14051210