
Patterns of Tumor Infiltrating Lymphocytes in Adenoid Cystic Carcinoma of the Head and Neck

 , , , , , , ,
, , , , , , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Samples
2.2. Immunohistochemistry
2.3. Image Processing
2.4. Statistical Analysis
3. Results
3.1. Clinical Parameters
3.2. Analysis of TIL Subtypes
3.3. Correlation of TIL Patterns and Clinical Parameter
3.4. Analysis of TIL Patterns with Regards to Recurrence and Metastasis
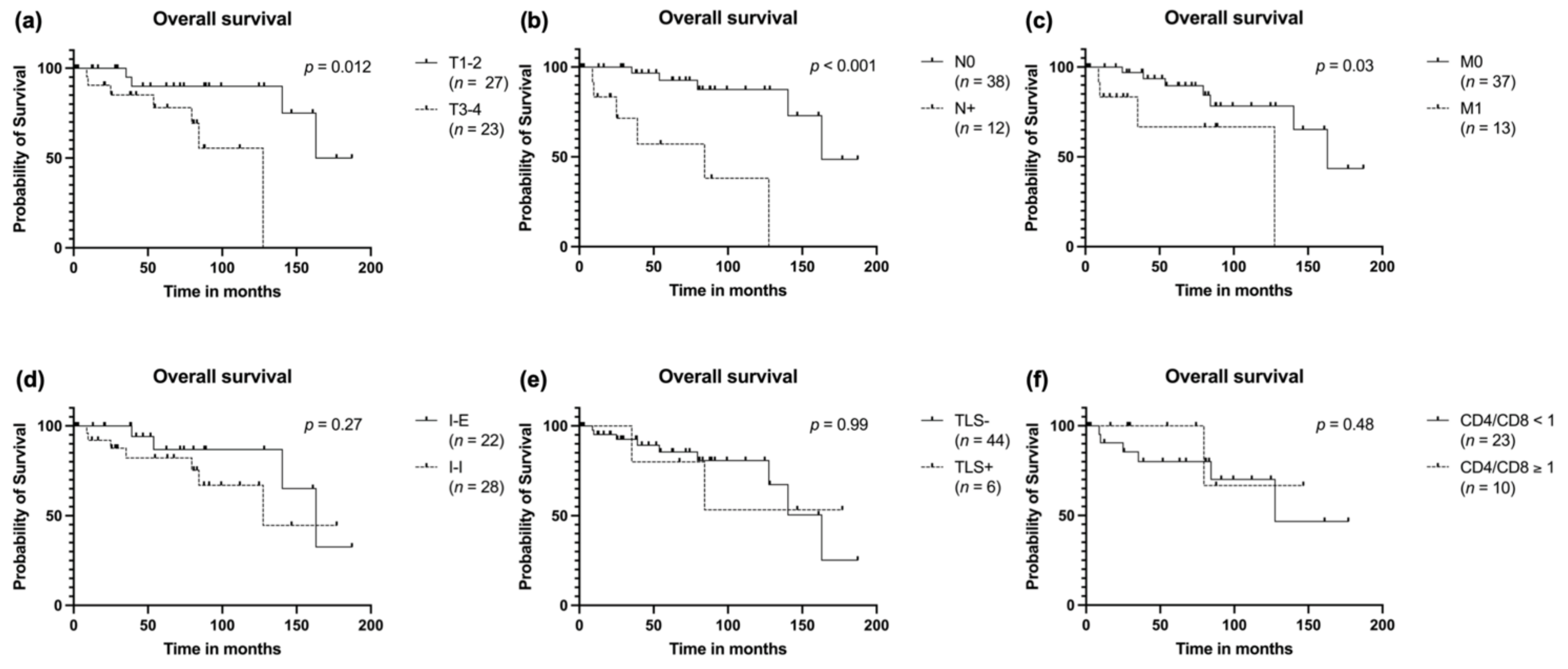
3.5. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spiro, R.H.; Huvos, A.G.; Strong, E.W. Adenoid cystic carcinoma of salivary origin. Am. J. Surg. 1974, 128, 512–520. [Google Scholar] [CrossRef]
- Akbaba, S.; Bostel, T.; Lang, K.; Bahadir, S.; Lipman, D.; Schmidberger, H.; Matthias, C.; Rotter, N.; Knopf, A.; Freudlsperger, C.; et al. Large German Multicenter Experience on the Treatment Outcome of 207 Patients With Adenoid Cystic Carcinoma of the Major Salivary Glands. Front. Oncol. 2020, 10, 2497. [Google Scholar] [CrossRef]
- Lloyd, S.; Yu, J.B.; Wilson, L.D.; Decker, R.H. Determinants and patterns of survival in adenoid cystic carcinoma of the head and neck, including an analysis of adjuvant radiation therapy. Am. J. Clin. Oncol. Cancer Clin. Trials 2011, 34, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Wang, S.; Luo, Y.; Yin, J.; Belkacemi, Y.; Lu, S.; Feng, M.; Lang, J. Outcome of Adenoid Cystic Carcinoma of Head and Neck After Postoperative Intensity Modulation Radiotherapy: A Single Institution Study. Cancer Manag. Res. 2021, 13, 2411. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, S.; Shinohara, S.; Tamaki, H.; Tateya, I.; Kitamura, M.; Mizuta, M.; Tanaka, S.; Kojima, T.; Asato, R.; Maetani, T.; et al. Adenoid cystic carcinoma of the head and neck: A retrospective multicenter study. Acta Oto-Laryngol. 2017, 138, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.; Kim, J.S.; Choi, Y.J.; Cho, J.-G.; Woo, J.-S.; Kim, A.; Kim, J.S.; Kang, E.J. Overexpression of PD-L2 is associated with shorter relapse-free survival in patients with malignant salivary gland tumors. Onco. Targets. Ther. 2017, 10, 2983–2992. [Google Scholar] [CrossRef] [Green Version]
- Nakano, T.; Takizawa, K.; Uezato, A.; Taguchi, K.; Toh, S.; Masuda, M. Prognostic value of programed death ligand-1 and ligand-2 co-expression in salivary gland carcinomas. Oral Oncol. 2019, 90, 30–37. [Google Scholar] [CrossRef]
- Linxweiler, M.; Kuo, F.; Katabi, N.; Lee, M.; Nadeem, Z.; Dalin, M.G.; Makarov, V.; Chowell, D.; Dogan, S.; Ganly, I.; et al. The Immune Microenvironment and Neoantigen Landscape of Aggressive Salivary Gland Carcinomas Differ by Subtype. Clin. Cancer Res. 2020, 26, 2859–2870. [Google Scholar] [CrossRef] [Green Version]
- Mosconi, C.; de Arruda, J.A.A.; de Faria, A.C.R.; Oliveira, G.A.Q.; de Paula, H.M.; Fonseca, F.P.; Mesquita, R.A.; Silva, T.A.; Mendonça, E.F.; Batista, A.C. Immune microenvironment and evasion mechanisms in adenoid cystic carcinomas of salivary glands. Oral Oncol. 2019, 88, 95–101. [Google Scholar] [CrossRef]
- Sahara, S.; Herzog, A.E.; Nör, J.E. Systemic therapies for salivary gland adenoid cystic carcinoma. Am. J. Cancer Res. 2021, 11, 4092–4110. [Google Scholar]
- Fayette, J.; Even, C.; Digue, L.; Geoffrois, L.; Rolland, F.; Cupissol, D.; Guigay, J.; Le Tourneau, C.; Dillies, A.-F.; Zanetta, S.; et al. NISCAHN: A phase II, multicenter nonrandomized trial aiming at evaluating nivolumab (N) in two cohorts of patients (pts) with recurrent/metastatic (R/M) salivary gland carcinoma of the head and neck (SGCHN), on behalf of the Unicancer Head & Neck Group. J. Clin. Oncol. 2019, 37, 6083. [Google Scholar] [CrossRef]
- Cohen, R.B.; Delord, J.P.; Doi, T.; Piha-Paul, S.A.; Liu, S.V.; Gilbert, J.; Algazi, A.P.; Damian, S.; Hong, R.L.; Le Tourneau, C.; et al. Pembrolizumab for the treatment of advanced salivary gland carcinoma: Findings of the phase 1b KEYNOTE-028 study. Am. J. Clin. Oncol. 2018, 41, 1083–1088. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, U.; Bang, A.; Chen, Y.H.; Mak, R.H.; Lorch, J.H.; Hanna, G.J.; Nishino, M.; Manuszak, C.; Thrash, E.M.; Severgnini, M.; et al. A Randomized Phase 2 Study of Pembrolizumab With or Without Radiation in Patients With Recurrent or Metastatic Adenoid Cystic Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Tchekmedyian, V.; Sherman, E.J.; Dunn, L.; Fetten, J.V.; Michel, L.S.; Kriplani, A.; Morris, L.; Ostrovnaya, I.; Katabi, N.; Haque, S.; et al. A phase II trial cohort of nivolumab plus ipilimumab in patients (Pts) with recurrent/metastatic adenoid cystic carcinoma (R/M ACC). J. Clin. Oncol. 2019, 37, 6084. [Google Scholar] [CrossRef]
- Lorini, L.; Ardighieri, L.; Bozzola, A.; Romani, C.; Bignotti, E.; Buglione, M.; Guerini, A.; Lombardi, D.; Deganello, A.; Tomasoni, M.; et al. Prognosis and management of recurrent and/or metastatic head and neck adenoid cystic carcinoma. Oral Oncol. 2021, 115, 105213. [Google Scholar] [CrossRef]
- Philip, M.; Schietinger, A. CD8+ T cell differentiation and dysfunction in cancer. Nat. Rev. Immunol. 2021, 1–15. [Google Scholar] [CrossRef]
- Dieu-Nosjean, M.C.; Giraldo, N.A.; Kaplon, H.; Germain, C.; Fridman, W.H.; Sautès-Fridman, C. Tertiary lymphoid structures, drivers of the anti-tumor responses in human cancers. Immunol. Rev. 2016, 271, 260–275. [Google Scholar] [CrossRef]
- Binnewies, M.; Roberts, E.W.; Kersten, K.; Chan, V.; Fearon, D.F.; Merad, M.; Coussens, L.M.; Gabrilovich, D.I.; Ostrand-Rosenberg, S.; Hedrick, C.C.; et al. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat. Med. 2018, 24, 541–550. [Google Scholar] [CrossRef]
- Wagner, D.-C.; Roth, W. Prognostic significance of immune cell infiltrates in tumor pathology. Pathologe 2018, 39, 532–538. [Google Scholar] [CrossRef]
- Bardou, P.; Mariette, J.; Escudié, F.; Djemiel, C.; Klopp, C. Jvenn: An interactive Venn diagram viewer. BMC Bioinform. 2014, 15, 293. [Google Scholar] [CrossRef] [Green Version]
- Colbeck, E.J.; Ager, A.; Gallimore, A.; Jones, G.W. Tertiary lymphoid structures in cancer: Drivers of antitumor immunity, immunosuppression, or Bystander Sentinels in disease? Front. Immunol. 2017, 8, 1830. [Google Scholar] [CrossRef] [Green Version]
- Ruffin, A.T.; Cillo, A.R.; Tabib, T.; Liu, A.; Onkar, S.; Kunning, S.R.; Lampenfeld, C.; Atiya, H.I.; Abecassis, I.; Kürten, C.H.L.; et al. B cell signatures and tertiary lymphoid structures contribute to outcome in head and neck squamous cell carcinoma. Nat. Commun. 2021, 12, 3349. [Google Scholar] [CrossRef] [PubMed]
- Germain, C.; Devi-Marulkar, P.; Knockaert, S.; Biton, J.; Kaplon, H.; Letaïef, L.; Goc, J.; Seguin-Givelet, A.; Gossot, D.; Girard, N.; et al. Tertiary Lymphoid Structure-B Cells Narrow Regulatory T Cells Impact in Lung Cancer Patients. Front. Immunol. 2021, 12, 520. [Google Scholar] [CrossRef] [PubMed]
- Lynch, K.T.; Young, S.J.; Meneveau, M.O.; Wages, N.A.; Engelhard, V.H.; Slingluff, C.L., Jr.; Mauldin, I.S. Heterogeneity in tertiary lymphoid structure B-cells correlates with patient survival in metastatic melanoma. J. Immunother. Cancer 2021, 9, e002273. [Google Scholar] [CrossRef] [PubMed]
- Mustapha, R.; Ng, K.; Monypenny, J.; Ng, T. Insights Into Unveiling a Potential Role of Tertiary Lymphoid Structures in Metastasis. Front. Mol. Biosci. 2021, 8, 843. [Google Scholar] [CrossRef]
- Engelhard, V.H.; Rodriguez, A.B.; Mauldin, I.S.; Woods, A.N.; Peske, J.D.; Slingluff, C.L. Immune Cell Infiltration and Tertiary Lymphoid Structures as Determinants of Antitumor Immunity. J. Immunol. 2018, 200, 432–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munoz-Erazo, L.; Rhodes, J.L.; Marion, V.C.; Kemp, R.A. Tertiary lymphoid structures in cancer—Considerations for patient prognosis. Cell. Mol. Immunol. 2020, 17, 570–575. [Google Scholar] [CrossRef]
- Wang, K.; Shen, T.; Siegal, G.P.; Wei, S. The CD4/CD8 ratio of tumor-infiltrating lymphocytes at the tumor-host interface has prognostic value in triple-negative breast cancer. Hum. Pathol. 2017, 69, 110–117. [Google Scholar] [CrossRef]
- Sridharan, V.; Gjini, E.; Liao, X.; Chau, N.G.; Haddad, R.I.; Severgnini, M.; Hammerman, P.; El-Naggar, A.; Freeman, G.J.; Hodi, F.S.; et al. Immune Profiling of Adenoid Cystic Carcinoma: PD-L2 Expression and Associations with Tumor-Infiltrating Lymphocytes. Cancer Immunol. Res. 2016, 4, 679–687. [Google Scholar] [CrossRef] [Green Version]
- Fonseca, I.; Bell, D.; Bishop, J.A.; Gnepp, D.R. Tumors of salivary glands, Benign tumors, Myoepithelioma. In WHO Classification of Head and Neck Tumors; El-Naggar, A.K., Chan, J.K.C., Grandis, J.R., Takata, T., Slootweg, P.J., Eds.; International Agency for Research on Cancer (IARC): Lyon, France, 2017; pp. 186–187. ISBN 978-92-832-2438-9. [Google Scholar]
- Clarke, J.; Panwar, B.; Madrigal, A.; Singh, D.; Gujar, R.; Wood, O.; Chee, S.J.; Eschweiler, S.; King, E.V.; Awad, A.S.; et al. Single-cell transcriptomic analysis of tissue-resident memory T cells in human lung cancer. J. Exp. Med. 2019, 216, 2128–2149. [Google Scholar] [CrossRef]
- Ganesan, A.P.; Clarke, J.; Wood, O.; Garrido-Martin, E.M.; Chee, S.J.; Mellows, T.; Samaniego-Castruita, D.; Singh, D.; Seumois, G.; Alzetani, A.; et al. Tissue-resident memory features are linked to the magnitude of cytotoxic T cell responses in human lung cancer. Nat. Immunol. 2017, 18, 940–950. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Fung, A.S.; McIntyre, J.B.; Simpson, R.; Afzal, A.R.; Hao, D.; Lau, H. Assessment Of Tumour Infiltrating Lymphocytes And Pd-l1 Expression In Adenoid Cystic Carcinoma Of The Salivary Gland. Clin. Investig. Med. 2021, 44, E38–E41. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Parameter | Infiltrated-Excluded (n = 22) | Infiltrated-Inflamed (n = 28) | p-Value 1 |
|---|---|---|---|
| Gender | 0.95 | ||
| Male | 10 (43.5%) | 13 (56.5%) | |
| Female | 12 (44.4%) | 15 (55.6%) | |
| Age (average in years) | 55.23 | 59.68 | 0.34 |
| Tumor site | 0.21 | ||
| Submandibular gland | 4 (23.5%) | 13 (76.5%) | |
| Parotid gland | 6 (66.7%) | 3 (33.3%) | |
| Paranasal sinus | 1 (16.7%) | 5 (83.3%) | |
| Base of tongue | 3 (60%) | 2 (40%) | |
| Nasal cavity | 2 (66.7%) | 1 (33.3%) | |
| Hard palate | 2 (100%) | 0 (0%) | |
| Sublingual gland | 1 (50%) | 1 (50%) | |
| Soft palate | 1 (50%) | 1 (50%) | |
| Nasopharynx | 0 (0%) | 1 (100%) | |
| Oral cavity | 0 (0%) | 1 (100%) | |
| Larynx | 1 (100%) | 0 (0%) | |
| External auditory meatus | 1 (100%) | 0 (0%) | |
| T-classification | 0.23 | ||
| T1–2 | 14 (51.9%) | 13 (48.1%) | |
| T3–4 | 8 (34.8%) | 15 (65.2%) | |
| N-classification | 0.64 | ||
| N0 | 18 (47.4%) | 20 (52.6%) | |
| N1 | 1 (25%) | 3 (75%) | |
| N2–3 | 3 (37.5%) | 5 (62.5%) | |
| M-classification | 0.06 | ||
| M0 | 21 (51.2%) | 20 (48.8%) | |
| M1 | 1 (12.5%) | 7 (87.5%) | |
| Stage | 0.03 | ||
| I-IVA | 20 (52.6%) | 18 (47.4%) | |
| IVB-IVC | 2 (16.7%) | 10 (83.3%) | |
| Primary therapy | 0.03 | ||
| Surgery alone | 12 (70.6%) | 5 (29.4%) | |
| Surgery + adj. RT | 8 (29.6%) | 19 (70.4%) | |
| RT | 2 (40%) | 3 (60%) | |
| R-Status 2 | 0.27 | ||
| R0 | 11 (52.4%) | 10 (47.6%) | |
| R0 after re-resection | 5 (55.6%) | 4 (44.4%) | |
| R1 | 3 (25%) | 9 (75%) | |
| R2 | 1 (100%) | 0 (0%) | |
| Pn 2 | 0.47 | ||
| Pn0 | 10 (50%) | 10 (50%) | |
| Pn1 | 9 (39%) | 14 (60.9%) |
| Patterns of Failure | Infiltrated-Inflamed | Infiltrated-Excluded | Presence of TLS † | CD4/CD8 Ratio < 1 * |
|---|---|---|---|---|
| Distant metastasis at initial diagnosis (8/50) | 7 (87.5%) | 1 (12.5%) | 1 (12.5%) | 5/7 (71.4%) |
| Recurrence (15/50) | 7/15 (46.7%) | 8/15 (53.3%) | 2/15 (13.3%) | 9/10 (90%) |
| Local recurrence (11/50) | 7/11 (63.3%) | 4/11 (36.4%) | 1/11 (9.3%) | 7/8 (87.5%) |
| Distant recurrence (6/50) | 2/6 (33.3%) | 4/6 (66.7%) | 1/6 (16.7%) | 3/3 (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doescher, J.; Meyer, M.; Arolt, C.; Quaas, A.; Klußmann, J.P.; Wolber, P.; Bankfalvi, A.; Schildhaus, H.-U.; Bastian, T.; Lang, S.; et al. Patterns of Tumor Infiltrating Lymphocytes in Adenoid Cystic Carcinoma of the Head and Neck. Cancers 2022, 14, 1383. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061383
Doescher J, Meyer M, Arolt C, Quaas A, Klußmann JP, Wolber P, Bankfalvi A, Schildhaus H-U, Bastian T, Lang S, et al. Patterns of Tumor Infiltrating Lymphocytes in Adenoid Cystic Carcinoma of the Head and Neck. Cancers. 2022; 14(6):1383. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061383
Chicago/Turabian StyleDoescher, Johannes, Moritz Meyer, Christoph Arolt, Alexander Quaas, Jens Peter Klußmann, Philipp Wolber, Agnes Bankfalvi, Hans-Ulrich Schildhaus, Tobias Bastian, Stephan Lang, and et al. 2022. "Patterns of Tumor Infiltrating Lymphocytes in Adenoid Cystic Carcinoma of the Head and Neck" Cancers 14, no. 6: 1383. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061383