
Hemodynamic Imaging in Cerebral Diffuse Glioma—Part A: Concept, Differential Diagnosis and Tumor Grading

 , ,
, ,  , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Overview of the Techniques and Parameters
2.1. Perfusion Imaging
2.2. Cerebrovascular Reactivity Imaging
3. Clinical Applications of Hemodynamic Imaging in Cerebral Diffuse Gliomas—Part 1
3.1. Differential Diagnosis versus Other Neoplastic and Non-Neoplastic Lesions
3.1.1. Metastases
3.1.2. Primary Central Nervous System Lymphomas
3.1.3. Non-Neoplastic Lesions: Abscesses and Autoimmune Lesions
3.2. Glioma Grading/Subtype
4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ostrom, Q.T.; Patil, N.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2013–2017. Neuro-Oncology 2020, 22, iv1–iv96. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO Guidelines on the Diagnosis and Treatment of Diffuse Gliomas of Adulthood. Nat. Rev. Clin. Oncol. 2020, 18, 170–186. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.I.; Kumthekar, P.; Stell, B.V.; Grimm, S.A.; Rademaker, A.W.; Rice, L.; Chandler, J.P.; Muro, K.; Marymont, M.; Helenowski, I.B.; et al. Concordance of Patient and Caregiver Reports in Evaluating Quality of Life in Patients with Malignant Gliomas and an Assessment of Caregiver Burden. Neuro-Oncol. Pract. 2014, 1, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Gately, L.; McLachlan, S.; Dowling, A.; Philip, J. Life beyond a Diagnosis of Glioblastoma: A Systematic Review of the Literature. J. Cancer Surviv. 2017, 11, 447–452. [Google Scholar] [CrossRef]
- Lundy, P.; Domino, J.; Ryken, T.; Fouke, S.; McCracken, D.J.; Ormond, D.R.; Olson, J.J. The Role of Imaging for the Management of Newly Diagnosed Glioblastoma in Adults: A Systematic Review and Evidence-Based Clinical Practice Guideline Update. J. Neurooncol. 2020, 150, 95–120. [Google Scholar] [CrossRef]
- Heynold, E.; Zimmermann, M.; Hore, N.; Buchfelder, M.; Doerfler, A.; Stadlbauer, A.; Kremenevski, N. Physiological MRI Biomarkers in the Differentiation Between Glioblastomas and Solitary Brain Metastases. Mol. Imaging Biol. 2021, 23, 787–795. [Google Scholar] [CrossRef]
- Zhang, L.; Yang, L.; Wen, L.; Lv, S.; Hu, J.; Li, Q.; Xu, J.; Xu, R.; Zhang, D. Noninvasively Evaluating the Grading of Glioma by Multiparametric Magnetic Resonance Imaging. Acad. Radiol. 2020, 28, e137–e146. [Google Scholar] [CrossRef]
- Verburg, N.; de Witt Hamer, P.C. State-of-the-Art Imaging for Glioma Surgery. Neurosurg. Rev. 2021, 44, 1331–1343. [Google Scholar] [CrossRef]
- Delgado-López, P.D.; Riñones-Mena, E.; Corrales-García, E.M. Treatment-Related Changes in Glioblastoma: A Review on the Controversies in Response Assessment Criteria and the Concepts of True Progression, Pseudoprogression, Pseudoresponse and Radionecrosis. Clin. Transl. Oncol. 2018, 20, 939–953. [Google Scholar] [CrossRef]
- Strauss, S.B.; Meng, A.; Ebani, E.J.; Chiang, G.C. Imaging Glioblastoma Posttreatment: Progression, Pseudoprogression, Pseudoresponse, Radiation Necrosis. Radiol. Clin. N. Am. 2019, 57, 1199–1216. [Google Scholar] [CrossRef] [PubMed]
- Zikou, A.; Sioka, C.; Alexiou, G.A.; Fotopoulos, A.; Voulgaris, S.; Argyropoulou, M.I. Radiation Necrosis, Pseudoprogression, Pseudoresponse, and Tumor Recurrence: Imaging Challenges for the Evaluation of Treated Gliomas. Contrast Media Mol. Imaging 2018, 2018, e6828396. [Google Scholar] [CrossRef] [PubMed]
- Thust, S.C.; van den Bent, M.J.; Smits, M. Pseudoprogression of Brain Tumors. J. Magn. Reson. Imaging 2018, 48, 571–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuster-Garcia, E.; Juan-Albarracín, J.; García-Ferrando, G.A.; Martí-Bonmatí, L.; Aparici-Robles, F.; García-Gómez, J.M. Improving the Estimation of Prognosis for Glioblastoma Patients by MR Based Hemodynamic Tissue Signatures. NMR Biomed. 2018, 31, e4006. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Yeung, T.P.C.; Bauman, G.; Yartsev, S.; Fainardi, E.; Macdonald, D.; Lee, T.-Y. Dynamic Perfusion CT in Brain Tumors. Eur. J. Radiol. 2015, 84, 2386–2392. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Liu, H.; Tong, H.; Wang, S.; Yang, Y.; Liu, G.; Zhang, W. Clinical Applications of Contrast-Enhanced Perfusion MRI Techniques in Gliomas: Recent Advances and Current Challenges. Contrast Media Mol. Imaging 2017, 2017, e7064120. [Google Scholar] [CrossRef] [Green Version]
- Telischak, N.A.; Detre, J.A.; Zaharchuk, G. Arterial Spin Labeling MRI: Clinical Applications in the Brain. J. Magn. Reson. Imaging 2015, 41, 1165–1180. [Google Scholar] [CrossRef]
- Brandão, L.A.; Shiroishi, M.S.; Law, M. Brain Tumors: A Multimodality Approach with Diffusion-Weighted Imaging, Diffusion Tensor Imaging, Magnetic Resonance Spectroscopy, Dynamic Susceptibility Contrast and Dynamic Contrast-Enhanced Magnetic Resonance Imaging. Magn. Reson. Imaging Clin. N. Am. 2013, 21, 199–239. [Google Scholar] [CrossRef]
- Essig, M.; Shiroishi, M.S.; Nguyen, T.B.; Saake, M.; Provenzale, J.M.; Enterline, D.; Anzalone, N.; Dörfler, A.; Rovira, À.; Wintermark, M.; et al. Perfusion MRI: The Five Most Frequently Asked Technical Questions. Am. J. Roentgenol. 2013, 200, 24–34. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO Classification of Tumours of the Central Nervous System. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A Summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willie, C.K.; Tzeng, Y.-C.; Fisher, J.A.; Ainslie, P.N. Integrative Regulation of Human Brain Blood Flow. J. Physiol. 2014, 592, 841–859. [Google Scholar] [CrossRef] [PubMed]
- Agnihotri, S.; Zadeh, G. Metabolic Reprogramming in Glioblastoma: The Influence of Cancer Metabolism on Epigenetics and Unanswered Questions. Neuro-Oncology 2016, 18, 160–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darbin, O.; Lonjon, M.; Quentien, M.H.; Michiels, J.F.; Grellier, P.; Negrin, J.; Rostain, J.C.; Risso, J.J. In Vivo Study of Tumor Metabolism: An Application of New Multi-Probe Microdialysis System in the Striatum of Freely Moving Rats Grafted with C6 Cells. Brain Res. 2000, 881, 121–127. [Google Scholar] [CrossRef]
- Arvanitis, C.D.; Ferraro, G.B.; Jain, R.K. The Blood–Brain Barrier and Blood–Tumour Barrier in Brain Tumours and Metastases. Nat. Rev. Cancer 2020, 20, 26–41. [Google Scholar] [CrossRef]
- Jain, R.K.; di Tomaso, E.; Duda, D.G.; Loeffler, J.S.; Sorensen, A.G.; Batchelor, T.T. Angiogenesis in Brain Tumours. Nat. Rev. Neurosci. 2007, 8, 610–622. [Google Scholar] [CrossRef]
- Watkins, S.; Robel, S.; Kimbrough, I.F.; Robert, S.M.; Ellis-Davies, G.; Sontheimer, H. Disruption of Astrocyte–Vascular Coupling and the Blood–Brain Barrier by Invading Glioma Cells. Nat. Commun. 2014, 5, 4196. [Google Scholar] [CrossRef] [Green Version]
- D’Alessandris, Q.G.; Pacioni, S.; Stumpo, V.; Buccarelli, M.; Lauretti, L.; Giordano, M.; Di Bonaventura, R.; Martini, M.; Larocca, L.M.; Giannetti, S.; et al. Dilation of Brain Veins and Perivascular Infiltration by Glioblastoma Cells in an In Vivo Assay of Early Tumor Angiogenesis. Available online: https://www.hindawi.com/journals/bmri/2021/8891045/ (accessed on 5 May 2021).
- Kane, J.R. The Role of Brain Vasculature in Glioblastoma. Mol. Neurobiol. 2019, 56, 6645–6653. [Google Scholar] [CrossRef]
- Seano, G.; Jain, R.K. Vessel Co-Option in Glioblastoma: Emerging Insights and Opportunities. Angiogenesis 2020, 23, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Lund-Smith, C.; Borboa, A.; Gonzalez, A.M.; Baird, A.; Eliceiri, B.P. Glioma-Induced Remodeling of the Neurovascular Unit. Brain Res. 2009, 1288, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, S.; Sair, H.I.; Pillai, J.J. The Problem of Neurovascular Uncoupling. Neuroimaging Clin. N. Am. 2021, 31, 53–67. [Google Scholar] [CrossRef] [PubMed]
- Sorribes, I.C.; Moore, M.N.J.; Byrne, H.M.; Jain, H.V. A Biomechanical Model of Tumor-Induced Intracranial Pressure and Edema in Brain Tissue. Biophys. J. 2019, 116, 1560–1574. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.O.; Adji, A.; O’Rourke, M.F.; Avolio, A.P.; Smielewski, P.; Pickard, J.D.; Czosnyka, M. Principles of Cerebral Hemodynamics When Intracranial Pressure Is Raised: Lessons from the Peripheral Circulation. J. Hypertens. 2015, 33, 1233–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aubert, A.; Costalat, R.; Duffau, H.; Benali, H. Modeling of Pathophysiological Coupling between Brain Electrical Activation, Energy Metabolism and Hemodynamics: Insights for the Interpretation of Intracerebral Tumor Imaging. Acta Biotheor. 2002, 50, 281–295. [Google Scholar] [CrossRef]
- Calamante, F.; Thomas, D.L.; Pell, G.S.; Wiersma, J.; Turner, R. Measuring Cerebral Blood Flow Using Magnetic Resonance Imaging Techniques. J. Cereb. Blood Flow Metab. 1999, 19, 701–735. [Google Scholar] [CrossRef] [Green Version]
- Golay, X.; Petersen, E.T. Arterial Spin Labeling: Benefits and Pitfalls of High Magnetic Field. Neuroimaging Clin. N. Am. 2006, 16, 259–268. [Google Scholar] [CrossRef]
- Meier, P.; Zierler, K.L. On the Theory of the Indicator-Dilution Method for Measurement of Blood Flow and Volume. J. Appl. Physiol. 1954, 6, 731–744. [Google Scholar] [CrossRef]
- Kety, S.S.; Schmidt, C.F. The Nitrous oxide method for the quantitative determination of Cerebral blood flow in man: Theory, procedure and normal values. J. Clin. Investig. 1948, 27, 476–483. [Google Scholar] [CrossRef]
- Wintermark, M.; Sesay, M.; Barbier, E.; Borbély, K.; Dillon, W.P.; Eastwood, J.D.; Glenn, T.C.; Grandin, C.B.; Pedraza, S.; Soustiel, J.F.; et al. Comparative Overview of Brain Perfusion Imaging Techniques. J. Neuroradiol. 2005, 32, 294–314. [Google Scholar] [CrossRef]
- Hoeffner, E.G. Cerebral Perfusion Imaging. J. Neuroophthalmol. 2005, 25, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Cianfoni, A.; Colosimo, C.; Basile, M.; Wintermark, M.; Bonomo, L. Brain Perfusion CT: Principles, Technique and Clinical Applications. Radiol. Med. 2007, 112, 1225–1243. [Google Scholar] [CrossRef] [PubMed]
- Miles, K.A. Perfusion Imaging with Computed Tomography: Brain and Beyond. Eur. Radiol. 2006, 16 (Suppl. S7), M37–M43. [Google Scholar] [CrossRef] [PubMed]
- Quarles, C.C.; Bell, L.C.; Stokes, A.M. Imaging Vascular and Hemodynamic Features of the Brain Using Dynamic Susceptibility Contrast and Dynamic Contrast Enhanced MRI. Neuroimage 2019, 187, 32–55. [Google Scholar] [CrossRef]
- Aksoy, F.G.; Lev, M.H. Dynamic Contrast-Enhanced Brain Perfusion Imaging: Technique and Clinical Applications. Semin. Ultrasound CT MR 2000, 21, 462–477. [Google Scholar] [CrossRef]
- Sourbron, S.P.; Buckley, D.L. Classic Models for Dynamic Contrast-Enhanced MRI. NMR Biomed. 2013, 26, 1004–1027. [Google Scholar] [CrossRef]
- Havsteen, I.; Damm Nybing, J.; Christensen, H.; Christensen, A.F. Arterial Spin Labeling: A Technical Overview. Acta Radiol. 2018, 59, 1232–1238. [Google Scholar] [CrossRef]
- Grade, M.; Hernandez Tamames, J.A.; Pizzini, F.B.; Achten, E.; Golay, X.; Smits, M. A Neuroradiologist’s Guide to Arterial Spin Labeling MRI in Clinical Practice. Neuroradiology 2015, 57, 1181–1202. [Google Scholar] [CrossRef] [Green Version]
- Lüdemann, L.; Warmuth, C.; Plotkin, M.; Förschler, A.; Gutberlet, M.; Wust, P.; Amthauer, H. Brain Tumor Perfusion: Comparison of Dynamic Contrast Enhanced Magnetic Resonance Imaging Using T1, T2, and T2* Contrast, Pulsed Arterial Spin Labeling, and H2(15)O Positron Emission Tomography. Eur. J. Radiol. 2009, 70, 465–474. [Google Scholar] [CrossRef]
- Jain, R. Perfusion CT Imaging of Brain Tumors: An Overview. AJNR Am. J. Neuroradiol. 2011, 32, 1570–1577. [Google Scholar] [CrossRef] [Green Version]
- Assimakopoulou, M.; Sotiropoulou-Bonikou, G.; Maraziotis, T.; Papadakis, N.; Varakis, I. Microvessel Density in Brain Tumors. Anticancer Res. 1997, 17, 4747–4753. [Google Scholar] [PubMed]
- Leon, S.P.; Folkerth, R.D.; Black, P.M. Microvessel Density is a Prognostic Indicator for Patients with Astroglial Brain Tumors. Cancer 1996, 77, 362–372. [Google Scholar] [CrossRef]
- Li, V.W.; Folkerth, R.D.; Watanabe, H.; Yu, C.; Rupnick, M.; Barnes, P.; Scott, R.M.; Black, P.M.; Sallan, S.E.; Folkman, J. Microvessel Count and Cerebrospinal Fluid Basic Fibroblast Growth Factor in Children with Brain Tumours. Lancet 1994, 344, 82–86. [Google Scholar] [CrossRef]
- Fan, C.; Zhang, J.; Liu, Z.; He, M.; Kang, T.; Du, T.; Song, Y.; Fan, Y.; Xu, J. Prognostic Role of Microvessel Density in Patients with Glioma. Medicine 2019, 98, e14695. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, L. Principles of Cerebral Perfusion Imaging by Bolus Tracking. J. Magn. Reson. Imaging 2005, 22, 710–717. [Google Scholar] [CrossRef]
- Calamante, F. Arterial Input Function in Perfusion MRI: A Comprehensive Review. Prog. Nucl. Magn. Reson. Spectrosc. 2013, 74, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Perthen, J.E.; Calamante, F.; Gadian, D.G.; Connelly, A. Is Quantification of Bolus Tracking MRI Reliable without Deconvolution? Magn. Reson. Med. 2002, 47, 61–67. [Google Scholar] [CrossRef]
- Jackson, A.; O’Connor, J.; Thompson, G.; Mills, S. Magnetic Resonance Perfusion Imaging in Neuro-Oncology. Cancer Imaging 2008, 8, 186–199. [Google Scholar] [CrossRef]
- Wetzel, S.G.; Cha, S.; Johnson, G.; Lee, P.; Law, M.; Kasow, D.L.; Pierce, S.D.; Xue, X. Relative Cerebral Blood Volume Measurements in Intracranial Mass Lesions: Interobserver and Intraobserver Reproducibility Study. Radiology 2002, 224, 797–803. [Google Scholar] [CrossRef]
- Fürst, H.; Hartl, W.H.; Janssen, I. Patterns of Cerebrovascular Reactivity in Patients with Unilateral Asymptomatic Carotid Artery Stenosis. Stroke 1994, 25, 1193–1200. [Google Scholar] [CrossRef] [Green Version]
- Shiroishi, M.S.; Castellazzi, G.; Boxerman, J.L.; D’Amore, F.; Essig, M.; Nguyen, T.B.; Provenzale, J.M.; Enterline, D.S.; Anzalone, N.; Dörfler, A.; et al. Principles of T2 *-Weighted Dynamic Susceptibility Contrast MRI Technique in Brain Tumor Imaging. J. Magn. Reson. Imaging 2015, 41, 296–313. [Google Scholar] [CrossRef] [PubMed]
- Buxton, R.B.; Frank, L.R.; Wong, E.C.; Siewert, B.; Warach, S.; Edelman, R.R. A General Kinetic Model for Quantitative Perfusion Imaging with Arterial Spin Labeling. Magn. Reson. Med. 1998, 40, 383–396. [Google Scholar] [CrossRef]
- Buxton, R.B. The Physics of Functional Magnetic Resonance Imaging (FMRI). Rep. Prog. Phys. 2013, 76, 096601. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.A.; Venkatraghavan, L.; Mikulis, D.J. Magnetic Resonance Imaging–Based Cerebrovascular Reactivity and Hemodynamic Reserve. Stroke 2018, 49, 2011–2018. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.A.; Mikulis, D.J. Cerebrovascular Reactivity: Purpose, Optimizing Methods, and Limitations to Interpretation—A Personal 20-Year Odyssey of (Re)Searching. Front. Physiol. 2021, 12, 629651. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Traylor, K.S.; Mountz, J.M. PET and SPECT Imaging of Brain Tumors. Semin. Ultrasound CT MRI 2020, 41, 530–540. [Google Scholar] [CrossRef]
- Tzeng, Y.-C.; Ainslie, P.N. Blood Pressure Regulation IX: Cerebral Autoregulation under Blood Pressure Challenges. Eur. J. Appl. Physiol. 2014, 114, 545–559. [Google Scholar] [CrossRef] [Green Version]
- Attwell, D.; Buchan, A.M.; Charpak, S.; Lauritzen, M.; MacVicar, B.A.; Newman, E.A. Glial and Neuronal Control of Brain Blood Flow. Nature 2010, 468, 232–243. [Google Scholar] [CrossRef] [Green Version]
- Fierstra, J.; Sobczyk, O.; Battisti-Charbonney, A.; Mandell, D.M.; Poublanc, J.; Crawley, A.P.; Mikulis, D.J.; Duffin, J.; Fisher, J.A. Measuring Cerebrovascular Reactivity: What Stimulus to Use? J. Physiol. 2013, 591, 5809–5821. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.J.; Gauthier, C.J. The Role of Cerebrovascular-Reactivity Mapping in Functional MRI: Calibrated FMRI and Resting-State FMRI. Front. Physiol. 2021, 12, 657362. [Google Scholar] [CrossRef]
- Sobczyk, O.; Fierstra, J.; Venkatraghavan, L.; Poublanc, J.; Duffin, J.; Fisher, J.A.; Mikulis, D.J. Measuring Cerebrovascular Reactivity: Sixteen Avoidable Pitfalls. Front. Physiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Slessarev, M.; Han, J.; Mardimae, A.; Prisman, E.; Preiss, D.; Volgyesi, G.; Ansel, C.; Duffin, J.; Fisher, J.A. Prospective Targeting and Control of End-Tidal CO2 and O2 Concentrations. J. Physiol. 2007, 581, 1207–1219. [Google Scholar] [CrossRef] [PubMed]
- Muscas, G.; van Niftrik, C.H.B.; Sebök, M.; Seystahl, K.; Piccirelli, M.; Stippich, C.; Weller, M.; Regli, L.; Fierstra, J. Hemodynamic Investigation of Peritumoral Impaired Blood Oxygenation-Level Dependent Cerebrovascular Reactivity in Patients with Diffuse Glioma. Magn. Reson. Imaging 2020, 70, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Sebök, M.; van Niftrik, C.H.B.; Muscas, G.; Pangalu, A.; Seystahl, K.; Weller, M.; Regli, L.; Fierstra, J. Hypermetabolism and Impaired Cerebrovascular Reactivity beyond the Standard MRI-Identified Tumor Border Indicate Diffuse Glioma Extended Tissue Infiltration. Neuro-Oncol. Adv. 2021, 3, vdab048. [Google Scholar] [CrossRef]
- Stumpo, V.; Sebök, M.; van Niftrik, C.H.B.; Seystahl, K.; Hainc, N.; Kulcsar, Z.; Weller, M.; Regli, L.; Fierstra, J. Feasibility of Glioblastoma Tissue Response Mapping with Physiologic BOLD Imaging Using Precise Oxygen and Carbon Dioxide Challenge. Magn. Reson. Mater. Phy. 2022, 35, 29–44. [Google Scholar] [CrossRef]
- Surendra, K.L.; Patwari, S.; Agrawal, S.; Chadaga, H.; Nagadi, A. Percentage Signal Intensity Recovery: A Step Ahead of RCBV in DSC MR Perfusion Imaging for the Differentiation of Common Neoplasms of Brain. Indian J. Cancer 2020, 57, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Karegowda, L.H.; Kadavigere, R.; Shenoy, P.M.; Paruthikunnan, S.M. Efficacy of Perfusion Computed Tomography (PCT) in Differentiating High-Grade Gliomas from Low Grade Gliomas, Lymphomas, Metastases and Abscess. J. Clin. Diagn. Res. 2017, 11, TC28–TC33. [Google Scholar] [CrossRef]
- Lin, L.; Xue, Y.; Duan, Q.; Sun, B.; Lin, H.; Huang, X.; Chen, X. The Role of Cerebral Blood Flow Gradient in Peritumoral Edema for Differentiation of Glioblastomas from Solitary Metastatic Lesions. Oncotarget 2016, 7, 69051–69059. [Google Scholar] [CrossRef] [Green Version]
- Jung, B.C.; Arevalo-Perez, J.; Lyo, J.K.; Holodny, A.I.; Karimi, S.; Young, R.J.; Peck, K.K. Comparison of Glioblastomas and Brain Metastases Using Dynamic Contrast-Enhanced Perfusion MRI. J. Neuroimaging 2016, 26, 240–246. [Google Scholar] [CrossRef] [Green Version]
- Kamble, R.B.; Jayakumar, P.N.; Shivashankar, R. Role of Dynamic CT Perfusion Study in Evaluating Various Intracranial Space-Occupying Lesions. Indian J. Radiol. Imaging 2015, 25, 162. [Google Scholar] [CrossRef]
- Zhao, J.; Yang, Z.; Luo, B.; Yang, J.; Chu, J. Quantitative Evaluation of Diffusion and Dynamic Contrast-Enhanced MR in Tumor Parenchyma and Peritumoral Area for Distinction of Brain Tumors. PLoS ONE 2015, 10, e0138573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halshtok Neiman, O.; Sadetzki, S.; Chetrit, A.; Raskin, S.; Yaniv, G.; Hoffmann, C. Perfusion-Weighted Imaging of Peritumoral Edema Can Aid in the Differential Diagnosis of Glioblastoma Mulltiforme versus Brain Metastasis. Isr. Med. Assoc. J. 2013, 15, 103–105. [Google Scholar] [PubMed]
- Bendini, M.; Marton, E.; Feletti, A.; Rossi, S.; Curtolo, S.; Inches, I.; Ronzon, M.; Longatti, P.; Di Paola, F. Primary and Metastatic Intraaxial Brain Tumors: Prospective Comparison of Multivoxel 2D Chemical-Shift Imaging (CSI) Proton MR Spectroscopy, Perfusion MRI, and Histopathological Findings in a Group of 159 Patients. Acta Neurochir. 2011, 153, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Schramm, P.; Xyda, A.; Klotz, E.; Tronnier, V.; Knauth, M.; Hartmann, M. Dynamic CT Perfusion Imaging of Intra-Axial Brain Tumours: Differentiation of High-Grade Gliomas from Primary CNS Lymphomas. Eur. Radiol. 2010, 20, 2482–2490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fainardi, E.; Di Biase, F.; Borrelli, M.; Saletti, A.; Cavallo, M.; Sarubbo, S.; Ceruti, S.; Tamarozzi, R.; Chieregato, A. Potential Role of CT Perfusion Parameters in the Identification of Solitary Intra-Axial Brain Tumor Grading. Acta Neurochir. Supp.l 2010, 106, 283–287. [Google Scholar] [CrossRef]
- Chiang, I.-C.; Hsieh, T.-J.; Chiu, M.-L.; Liu, G.-C.; Kuo, Y.-T.; Lin, W.-C. Distinction between Pyogenic Brain Abscess and Necrotic Brain Tumour Using 3-Tesla MR Spectroscopy, Diffusion and Perfusion Imaging. BJR 2009, 82, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Hakyemez, B.; Erdogan, C.; Bolca, N.; Yildirim, N.; Gokalp, G.; Parlak, M. Evaluation of Different Cerebral Mass Lesions by Perfusion-Weighted MR Imaging. J. Magn. Reson. Imaging 2006, 24, 817–824. [Google Scholar] [CrossRef]
- Rollin, N.; Guyotat, J.; Streichenberger, N.; Honnorat, J.; Tran Minh, V.-A.; Cotton, F. Clinical Relevance of Diffusion and Perfusion Magnetic Resonance Imaging in Assessing Intra-Axial Brain Tumors. Neuroradiology 2006, 48, 150–159. [Google Scholar] [CrossRef]
- Bulakbasi, N.; Kocaoglu, M.; Farzaliyev, A.; Tayfun, C.; Ucoz, T.; Somuncu, I. Assessment of Diagnostic Accuracy of Perfusion MR Imaging in Primary and Metastatic Solitary Malignant Brain Tumors. Am. J. Neuroradiol. 2005, 26, 2187–2199. [Google Scholar]
- Kremer, S.; Grand, S.; Remy, C.; Esteve, F.; Lefournier, V.; Pasquier, B.; Hoffmann, D.; Benabid, A.L.; Le Bas, J.-F. Cerebral Blood Volume Mapping by MR Imaging in the Initial Evaluation of Brain Tumors. J. Neuroradiol. 2002, 29, 105–113. [Google Scholar]
- Cho, S.K.; Na, D.G.; Ryoo, J.W.; Roh, H.G.; Moon, C.H.; Byun, H.S.; Kim, J.H. Perfusion MR Imaging: Clinical Utility for the Differential Diagnosis of Various Brain Tumors. Korean J. Radiol. 2002, 3, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Sunwoo, L.; Yun, T.J.; You, S.-H.; Yoo, R.-E.; Kang, K.M.; Choi, S.H.; Kim, J.; Sohn, C.-H.; Park, S.-W.; Jung, C.; et al. Differentiation of Glioblastoma from Brain Metastasis: Qualitative and Quantitative Analysis Using Arterial Spin Labeling MR Imaging. PLoS ONE 2016, 11, e0166662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tupý, R.; Mírka, H.; Mraček, J.; Přibáň, V.; Hes, O.; Vokurka, S.; Ferda, J. Tumor-Related Perfusion Changes in White Matter Adjacent to Brain Tumors: Pharmacodynamic Analysis of Dynamic 3T Magnetic Resonance Imaging. Anticancer. Res. 2018, 38, 4149–4152. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.H.; Erly, W.; Moser, F.G.; Maya, M.; Nael, K. Differentiation of Solitary Brain Metastasis from Glioblastoma Multiforme: A Predictive Multiparametric Approach Using Combined MR Diffusion and Perfusion. Neuroradiology 2015, 57, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Neska-Matuszewska, M.; Bladowska, J.; Sąsiadek, M.; Zimny, A. Differentiation of Glioblastoma Multiforme, Metastases and Primary Central Nervous System Lymphomas Using Multiparametric Perfusion and Diffusion MR Imaging of a Tumor Core and a Peritumoral Zone—Searching for a Practical Approach. PLoS ONE 2018, 13, e0191341. [Google Scholar] [CrossRef]
- Mangla, R.; Kolar, B.; Zhu, T.; Zhong, J.; Almast, J.; Ekholm, S. Percentage Signal Recovery Derived from MR Dynamic Susceptibility Contrast Imaging Is Useful to Differentiate Common Enhancing Malignant Lesions of the Brain. Am. J. Neuroradiol. 2011. [Google Scholar] [CrossRef] [Green Version]
- Gaudino, S.; Benenati, M.; Martucci, M.; Botto, A.; Infante, A.; Marrazzo, A.; Ramaglia, A.; Marziali, G.; Guadalupi, P.; Colosimo, C. Investigating Dynamic Susceptibility Contrast-Enhanced Perfusion-Weighted Magnetic Resonance Imaging in Posterior Fossa Tumors: Differences and Similarities with Supratentorial Tumors. Radiol. Med. 2020, 125, 416–422. [Google Scholar] [CrossRef]
- Askaner, K.; Rydelius, A.; Engelholm, S.; Knutsson, L.; Lätt, J.; Abul-Kasim, K.; Sundgren, P. Differentiation between Glioblastomas and Brain Metastases and Regarding Their Primary Site of Malignancy Using Dynamic Susceptibility Contrast MRI at 3T. J. Neuroradiol. 2019, 46, 367–372. [Google Scholar] [CrossRef]
- Onishi, S.; Kajiwara, Y.; Takayasu, T.; Kolakshyapati, M.; Ishifuro, M.; Amatya, V.J.; Takeshima, Y.; Sugiyama, K.; Kurisu, K.; Yamasaki, F. Perfusion Computed Tomography Parameters Are Useful for Differentiating Glioblastoma, Lymphoma, and Metastasis. World Neurosurg. 2018, 119, e890–e897. [Google Scholar] [CrossRef]
- Gaa, J.; Warach, S.; Wen, P.; Thangaraj, V.; Wielopolski, P.; Edelman, R.R. Noninvasive Perfusion Imaging of Human Brain Tumors with EPISTAR. Eur. Radiol. 1996, 6, 518–522. [Google Scholar] [CrossRef]
- Xi, Y.; Kang, X.; Wang, N.; Liu, T.; Zhu, Y.; Cheng, G.; Wang, K.; Li, C.; Guo, F.; Yin, H. Differentiation of Primary Central Nervous System Lymphoma from High-Grade Glioma and Brain Metastasis Using Arterial Spin Labeling and Dynamic Contrast-Enhanced Magnetic Resonance Imaging. Eur. J. Radiol. 2019, 112, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Toh, C.H.; Wei, K.-C.; Chang, C.-N.; Ng, S.-H.; Wong, H.-F. Differentiation of Primary Central Nervous System Lymphomas and Glioblastomas: Comparisons of Diagnostic Performance of Dynamic Susceptibility Contrast-Enhanced Perfusion MR Imaging without and with Contrast-Leakage Correction. Am. J. Neuroradiol. 2013, 34, 1145–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xyda, A.; Haberland, U.; Klotz, E.; Jung, K.; Bock, H.C.; Schramm, R.; Knauth, M.; Schramm, P. Diagnostic Performance of Whole Brain Volume Perfusion CT in Intra-Axial Brain Tumors: Preoperative Classification Accuracy and Histopathologic Correlation. Eur. J. Radiol. 2012, 81, 4105–4111. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, L.; Crasto, S.G.; Moruno, P.G.; Cassoni, P.; Rudà, R.; Boccaletti, R.; Brosio, M.; De Lucchi, R.; Fava, C. Role of Diffusion- and Perfusion-Weighted MR Imaging for Brain Tumour Characterisation. Radiol. Med. 2009, 114, 645–659. [Google Scholar] [CrossRef]
- Kickingereder, P.; Wiestler, B.; Sahm, F.; Heiland, S.; Roethke, M.; Schlemmer, H.-P.; Wick, W.; Bendszus, M.; Radbruch, A. Primary Central Nervous System Lymphoma and Atypical Glioblastoma: Multiparametric Differentiation by Using Diffusion-, Perfusion-, and Susceptibility-Weighted MR Imaging. Radiology 2014, 272, 843–850. [Google Scholar] [CrossRef] [Green Version]
- Kickingereder, P.; Sahm, F.; Wiestler, B.; Roethke, M.; Heiland, S.; Schlemmer, H.-P.; Wick, W.; von Deimling, A.; Bendszus, M.; Radbruch, A. Evaluation of Microvascular Permeability with Dynamic Contrast-Enhanced MRI for the Differentiation of Primary CNS Lymphoma and Glioblastoma: Radiologic-Pathologic Correlation. Am. J. Neuroradiol. 2014, 35, 1503–1508. [Google Scholar] [CrossRef] [Green Version]
- You, S.-H.; Yun, T.J.; Choi, H.J.; Yoo, R.-E.; Kang, K.M.; Choi, S.H.; Kim, J.; Sohn, C.-H. Differentiation between Primary CNS Lymphoma and Glioblastoma: Qualitative and Quantitative Analysis Using Arterial Spin Labeling MR Imaging. Eur. Radiol. 2018, 28, 3801–3810. [Google Scholar] [CrossRef]
- Toh, C.H.; Wei, K.-C.; Chang, C.-N.; Ng, S.-H.; Wong, H.-F.; Lin, C.-P. Differentiation of Brain Abscesses from Glioblastomas and Metastatic Brain Tumors: Comparisons of Diagnostic Performance of Dynamic Susceptibility Contrast-Enhanced Perfusion MR Imaging before and after Mathematic Contrast Leakage Correction. PLoS ONE 2014, 9, e109172. [Google Scholar] [CrossRef]
- Jain, R.; Ellika, S.; Lehman, N.L.; Scarpace, L.; Schultz, L.R.; Rock, J.P.; Rosenblum, M.; Mikkelsen, T. Can Permeability Measurements Add to Blood Volume Measurements in Differentiating Tumefactive Demyelinating Lesions from High Grade Gliomas Using Perfusion CT? J. Neurooncol. 2010, 97, 383–388. [Google Scholar] [CrossRef]
- Haris, M.; Gupta, R.K.; Singh, A.; Husain, N.; Husain, M.; Pandey, C.M.; Srivastava, C.; Behari, S.; Rathore, R.K.S. Differentiation of Infective from Neoplastic Brain Lesions by Dynamic Contrast-Enhanced MRI. Neuroradiology 2008, 50, 531. [Google Scholar] [CrossRef] [Green Version]
- Rhun, E.L.; Guckenberger, M.; Smits, M.; Dummer, R.; Bachelot, T.; Sahm, F.; Galldiks, N.; de Azambuja, E.; Berghoff, A.S.; Metellus, P.; et al. EANO–ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up of Patients with Brain Metastasis from Solid Tumours. Ann. Oncol. 2021, 32, 1332–1347. [Google Scholar] [CrossRef] [PubMed]
- Artzi, M.; Bokstein, F.; Blumenthal, D.T.; Aizenstein, O.; Liberman, G.; Corn, B.W.; Bashat, D.B. Differentiation between Vasogenic-Edema versus Tumor-Infiltrative Area in Patients with Glioblastoma during Bevacizumab Therapy: A Longitudinal MRI Study. Eur. J. Radiol. 2014, 83, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Villanueva-Meyer, J.E.; Mabray, M.C.; Cha, S. Current Clinical Brain Tumor Imaging. Neurosurgery 2017, 81, 397–415. [Google Scholar] [CrossRef] [Green Version]
- Suh, C.H.; Kim, H.S.; Jung, S.C.; Choi, C.G.; Kim, S.J. Perfusion MRI as a Diagnostic Biomarker for Differentiating Glioma from Brain Metastasis: A Systematic Review and Meta-Analysis. Eur. Radiol. 2018, 28, 3819–3831. [Google Scholar] [CrossRef]
- Lee, M.D.; Baird, G.L.; Bell, L.C.; Quarles, C.C.; Boxerman, J.L. Utility of Percentage Signal Recovery and Baseline Signal in DSC-MRI Optimized for Relative CBV Measurement for Differentiating Glioblastoma, Lymphoma, Metastasis, and Meningioma. Am. J. Neuroradiol. 2019, 40, 1445–1450. [Google Scholar] [CrossRef] [Green Version]
- Cha, S.; Lupo, J.M.; Chen, M.-H.; Lamborn, K.R.; McDermott, M.W.; Berger, M.S.; Nelson, S.J.; Dillon, W.P. Differentiation of Glioblastoma Multiforme and Single Brain Metastasis by Peak Height and Percentage of Signal Intensity Recovery Derived from Dynamic Susceptibility-Weighted Contrast-Enhanced Perfusion MR Imaging. Am. J. Neuroradiol. 2007, 28, 1078–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, S.; Gao, Q.; Yu, J.; Li, Y.; Cao, P.; Shi, H.; Hong, X. Utility of Dynamic Contrast-Enhanced Magnetic Resonance Imaging for Differentiating Glioblastoma, Primary Central Nervous System Lymphoma and Brain Metastatic Tumor. Eur. J. Radiol. 2016, 85, 1722–1727. [Google Scholar] [CrossRef] [PubMed]
- Abdel Razek, A.A.K.; Talaat, M.; El-Serougy, L.; Abdelsalam, M.; Gaballa, G. Differentiating Glioblastomas from Solitary Brain Metastases Using Arterial Spin Labeling Perfusion—And Diffusion Tensor Imaging—Derived Metrics. World Neurosurg. 2019, 127, e593–e598. [Google Scholar] [CrossRef]
- Suh, C.H.; Kim, H.S.; Jung, S.C.; Park, J.E.; Choi, C.G.; Kim, S.J. MRI as a Diagnostic Biomarker for Differentiating Primary Central Nervous System Lymphoma from Glioblastoma: A Systematic Review and Meta-Analysis. J. Magn. Reson. Imaging 2019, 50, 560–572. [Google Scholar] [CrossRef]
- Fu, M.; Han, F.; Feng, C.; Chen, T.; Feng, X. Based on Arterial Spin Labeling Helps to Differentiate High-Grade Gliomas from Brain Solitary Metastasis: A Systematic Review and Meta-Analysis. Medicine 2019, 98, e15580. [Google Scholar] [CrossRef]
- Hoang-Xuan, K.; Bessell, E.; Bromberg, J.; Hottinger, A.F.; Preusser, M.; Rudà, R.; Schlegel, U.; Siegal, T.; Soussain, C.; Abacioglu, U.; et al. Diagnosis and Treatment of Primary CNS Lymphoma in Immunocompetent Patients: Guidelines from the European Association for Neuro-Oncology. Lancet Oncol. 2015, 16, e322–e332. [Google Scholar] [CrossRef] [Green Version]
- Weller, M.; Martus, P.; Roth, P.; Thiel, E.; Korfel, A.; for the German PCNSL Study Group. Surgery for Primary CNS Lymphoma? Challenging a Paradigm. Neuro-Oncology 2012, 14, 1481–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, Z.; You, R.X.; Li, J.; Liu, Y.; Cao, D.R. Differentiation of Primary Central Nervous System Lymphomas from High-Grade Gliomas by RCBV and Percentage of Signal Intensity Recovery Derived from Dynamic Susceptibility-Weighted Contrast-Enhanced Perfusion MR Imaging. Clin. Neuroradiol. 2014, 24, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Wang, Q.; Shao, A.; Xu, B.; Zhang, J. The Performance of MR Perfusion-Weighted Imaging for the Differentiation of High-Grade Glioma from Primary Central Nervous System Lymphoma: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0173430. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.; Wetzel, S.G.; Cha, S.; Babb, J.; Tofts, P.S. Measuring Blood Volume and Vascular Transfer Constant from Dynamic, T-Weighted Contrast-Enhanced MRI. Magn. Reson. Med. 2004, 51, 961–968. [Google Scholar] [CrossRef]
- Lin, X.; Lee, M.; Buck, O.; Woo, K.M.; Zhang, Z.; Hatzoglou, V.; Omuro, A.; Arevalo-Perez, J.; Thomas, A.A.; Huse, J.; et al. Diagnostic Accuracy of T1-Weighted Dynamic Contrast-Enhanced–MRI and DWI-ADC for Differentiation of Glioblastoma and Primary CNS Lymphoma. Am. J. Neuroradiol. 2017, 38, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Lee, H.-J.; Ahn, S.S.; Chang, J.H.; Kang, S.-G.; Kim, E.H.; Kim, S.H.; Lee, S.-K. Primary Central Nervous System Lymphoma and Atypical Glioblastoma: Differentiation Using the Initial Area under the Curve Derived from Dynamic Contrast-Enhanced MR and the Apparent Diffusion Coefficient. Eur. Radiol. 2017, 27, 1344–1351. [Google Scholar] [CrossRef]
- Okuchi, S.; Rojas-Garcia, A.; Ulyte, A.; Lopez, I.; Ušinskienė, J.; Lewis, M.; Hassanein, S.M.; Sanverdi, E.; Golay, X.; Thust, S.; et al. Diagnostic Accuracy of Dynamic Contrast-Enhanced Perfusion MRI in Stratifying Gliomas: A Systematic Review and Meta-Analysis. Cancer Med. 2019, 8, 5564–5573. [Google Scholar] [CrossRef]
- Di, N.; Cheng, W.; Chen, H.; Zhai, F.; Liu, Y.; Mu, X.; Chu, Z.; Lu, N.; Liu, X.; Wang, B. Utility of Arterial Spin Labelling MRI for Discriminating Atypical High-Grade Glioma from Primary Central Nervous System Lymphoma. Clin. Radiol. 2019, 74, 165.e1–165.e9. [Google Scholar] [CrossRef]
- Warnke, P.C.; Timmer, J.; Ostertag, C.B.; Kopitzki, K. Capillary Physiology and Drug Delivery in Central Nervous System Lymphomas. Ann. Neurol. 2005, 57, 136–139. [Google Scholar] [CrossRef]
- Muccio, C.F.; Caranci, F.; D’Arco, F.; Cerase, A.; De Lipsis, L.; Esposito, G.; Tedeschi, E.; Andreula, C. Magnetic Resonance Features of Pyogenic Brain Abscesses and Differential Diagnosis Using Morphological and Functional Imaging Studies: A Pictorial Essay. J. Neuroradiol. 2014, 41, 153–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.-X.; Li, B.; Yang, H.-F.; Du, Y.; Li, Y.; Wang, W.-X.; Zheng, H.-J.; Gong, Q.-Y. Can Diffusion-Weighted Imaging Be Used to Differentiate Brain Abscess from Other Ring-Enhancing Brain Lesions? A Meta-Analysis. Clin. Radiol. 2014, 69, 909–915. [Google Scholar] [CrossRef]
- Erdogan, C.; Hakyemez, B.; Yildirim, N.; Parlak, M. Brain Abscess and Cystic Brain Tumor: Discrimination With Dynamic Susceptibility Contrast Perfusion-Weighted MRI. J. Comput. Assist. Tomogr. 2005, 29, 663–667. [Google Scholar] [CrossRef]
- Holmes, T.M.; Petrella, J.R.; Provenzale, J.M. Distinction Between Cerebral Abscesses and High-Grade Neoplasms by Dynamic Susceptibility Contrast Perfusion MRI. Am. J. Roentgenol. 2004, 183, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Chawalparit, O.; Artkaew, C.; Anekthananon, T.; Tisavipat, N.; Charnchaowanish, P.; Sangruchi, T. Diagnostic Accuracy of Perfusion CT in Differentiating Brain Abscess from Necrotic Tumor. J. Med. Assoc. Thai. 2009, 92, 537–542. [Google Scholar] [PubMed]
- Blasel, S.; Pfeilschifter, W.; Jansen, V.; Mueller, K.; Zanella, F.; Hattingen, E. Metabolism and Regional Cerebral Blood Volume in Autoimmune Inflammatory Demyelinating Lesions Mimicking Malignant Gliomas. J. Neurol. 2011, 258, 113–122. [Google Scholar] [CrossRef]
- Hiremath, S.B.; Muraleedharan, A.; Kumar, S.; Nagesh, C.; Kesavadas, C.; Abraham, M.; Kapilamoorthy, T.R.; Thomas, B. Combining Diffusion Tensor Metrics and DSC Perfusion Imaging: Can It Improve the Diagnostic Accuracy in Differentiating Tumefactive Demyelination from High-Grade Glioma? Am. J. Neuroradiol. 2017, 38, 685–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cha, S.; Pierce, S.; Knopp, E.A.; Johnson, G.; Yang, C.; Ton, A.; Litt, A.W.; Zagzag, D. Dynamic Contrast-Enhanced T2*-Weighted MR Imaging of Tumefactive Demyelinating Lesions. Am. J. Neuroradiol. 2001, 22, 1109–1116. [Google Scholar] [PubMed]
- Parks, N.E.; Bhan, V.; Shankar, J.J. Perfusion Imaging of Tumefactive Demyelinating Lesions Compared to High Grade Gliomas. Can. J. Neurol. Sci. 2016, 43, 316–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, R.; Griffith, B.; Alotaibi, F.; Zagzag, D.; Fine, H.; Golfinos, J.; Schultz, L. Glioma Angiogenesis and Perfusion Imaging: Understanding the Relationship between Tumor Blood Volume and Leakiness with Increasing Glioma Grade. Am. J. Neuroradiol. 2015, 36, 2030–2035. [Google Scholar] [CrossRef] [Green Version]
- Rani, N.; Singh, B.; Kumar, N.; Singh, P.; Hazari, P.P.; Jaswal, A.; Gupta, S.K.; Chhabra, R.; Radotra, B.D.; Mishra, A.K. The Diagnostic Performance of 99mTc-Methionine Single-Photon Emission Tomography in Grading Glioma Preoperatively: A Comparison with Histopathology and Ki-67 Indices. Nucl. Med. Commun. 2020, 41, 848–857. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Dong, H. Ki-67 Labeling Index and the Grading of Cerebral Gliomas by Using Intravoxel Incoherent Motion Diffusion-Weighted Imaging and Three-Dimensional Arterial Spin Labeling Magnetic Resonance Imaging. Acta Radiol. 2020, 61, 1057–1063. [Google Scholar] [CrossRef] [PubMed]
- Sasi, S.D.; Ramaniharan, A.K.; Bhattacharjee, R.; Gupta, R.K.; Saha, I.; Van Cauteren, M.; Shah, T.; Gopalakrishnan, K.; Gupta, A.; Singh, A. Evaluating Feasibility of High Resolution T1-Perfusion MRI with Whole Brain Coverage Using Compressed SENSE: Application to Glioma Grading. Eur. J. Radiol. 2020, 129, 109049. [Google Scholar] [CrossRef]
- Kang, X.; Xi, Y.; Liu, T.; Wang, N.; Zhu, Y.; Wang, X.; Guo, F. Grading of Glioma: Combined Diagnostic Value of Amide Proton Transfer Weighted, Arterial Spin Labeling and Diffusion Weighted Magnetic Resonance Imaging. BMC Med. Imaging 2020, 20, 50. [Google Scholar] [CrossRef]
- Grewal, D.S.; Rajesh, U.; Sreedhar, C.; Awasthi, S.; Vijayakumar, C. Evaluation of Brain Tumours Using Magnetic Resonance Perfusion Imaging: A Prospective Study. JCDR 2020, 14, 1–4. [Google Scholar] [CrossRef]
- Hashido, T.; Saito, S.; Ishida, T. A Radiomics-Based Comparative Study on Arterial Spin Labeling and Dynamic Susceptibility Contrast Perfusion-Weighted Imaging in Gliomas. Sci. Rep. 2020, 10, 6121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, S.; Wang, L.; Yang, H.; Shan, Y.; Cheng, Y.; Xu, L.; Dong, C.; Zhao, G.; Lu, J. Static 18F-FET PET and DSC-PWI Based on Hybrid PET/MR for the Prediction of Gliomas Defined by IDH and 1p/19q Status. Eur. Radiol. 2020, 31, 4087–4096. [Google Scholar] [CrossRef]
- Alkanhal, H.; Das, K.; Poptani, H. Diffusion- and Perfusion-Weighted Magnetic Resonance Imaging Methods in Nonenhancing Gliomas. World Neurosurg. 2020, 141, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Alkanhal, H.; Das, K.; Rathi, N.; Syed, K.; Poptani, H. Differentiating Nonenhancing Grade II Gliomas from Grade III Gliomas Using Diffusion Tensor Imaging and Dynamic Susceptibility Contrast MRI. World Neurosurg. 2020, 146, e555–e564. [Google Scholar] [CrossRef]
- Hasan, A.-M.S.; Hasan, A.K.; Megally, H.I.; Khallaf, M.; Haseib, A. The Combined Role of MR Spectroscopy and Perfusion Imaging in Preoperative Differentiation between High- and Low-Grade Gliomas. Egypt. J. Radiol. Nucl. Med. 2019, 50, 72. [Google Scholar] [CrossRef]
- Conte, G.M.; Altabella, L.; Castellano, A.; Cuccarini, V.; Bizzi, A.; Grimaldi, M.; Costa, A.; Caulo, M.; Falini, A.; Anzalone, N. Comparison of T1 Mapping and Fixed T1 Method for Dynamic Contrast-Enhanced MRI Perfusion in Brain Gliomas. Eur. Radiol. 2019, 29, 3467–3479. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Xie, S.; Liu, H.; Chen, G.; Zhang, W. Arterial Spin Labeling for Glioma Grade Discrimination: Correlations with IDH1 Genotype and 1p/19q Status. Transl. Oncol. 2019, 12, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Zhou, L.; Jiang, J.; Quan, G.; Wei, X. Combination of Three-Dimensional Arterial Spin Labeling and Stretched-Exponential Model in Grading of Gliomas. Medicine 2019, 98, e16012. [Google Scholar] [CrossRef] [PubMed]
- Saini, J.; Gupta, R.K.; Kumar, M.; Singh, A.; Saha, I.; Santosh, V.; Beniwal, M.; Kandavel, T.; Cauteren, M.V. Comparative Evaluation of Cerebral Gliomas Using RCBV Measurements during Sequential Acquisition of T1-Perfusion and T2*-Perfusion MRI. PLoS ONE 2019, 14, e0215400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komatsu, K.; Wanibuchi, M.; Mikami, T.; Akiyama, Y.; Iihoshi, S.; Miyata, K.; Sugino, T.; Suzuki, K.; Kanno, A.; Noshiro, S.; et al. Arterial Spin Labeling Method as a Supplemental Predictor to Distinguish Between High- and Low-Grade Gliomas. World Neurosurg. 2018, 114, e495–e500. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, K.; Hiwatashi, A.; Togao, O.; Yamashita, K.; Kamei, R.; Kitajima, M.; Kanoto, M.; Takahashi, H.; Uchiyama, Y.; Harada, M.; et al. Usefulness of Perfusion- and Diffusion-Weighted Imaging to Differentiate between Pilocytic Astrocytomas and High-Grade Gliomas: A Multicenter Study in Japan. Neuroradiology 2018, 60, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.K.; Saini, J.; Sahoo, P.; Patir, R.; Ahlawat, S.; Beniwal, M.; Thennarasu, K.; Santosh, V.; Gupta, R.K. Role of Dynamic Contrast-Enhanced Perfusion Magnetic Resonance Imaging in Grading of Pediatric Brain Tumors on 3T. PNE 2017, 52, 298–305. [Google Scholar] [CrossRef]
- Wu, R.; Watanabe, Y.; Arisawa, A.; Takahashi, H.; Tanaka, H.; Fujimoto, Y.; Watabe, T.; Isohashi, K.; Hatazawa, J.; Tomiyama, N. Whole-Tumor Histogram Analysis of the Cerebral Blood Volume Map: Tumor Volume Defined by 11C-Methionine Positron Emission Tomography Image Improves the Diagnostic Accuracy of Cerebral Glioma Grading. Jpn. J. Radiol. 2017, 35, 613–621. [Google Scholar] [CrossRef]
- Ma, H.; Wang, Z.; Xu, K.; Shao, Z.; Yang, C.; Xu, P.; Liu, X.; Hu, C.; Lu, X.; Rong, Y. Three-Dimensional Arterial Spin Labeling Imaging and Dynamic Susceptibility Contrast Perfusion-Weighted Imaging Value in Diagnosing Glioma Grade Prior to Surgery. Exp. Ther. Med. 2017, 13, 2691–2698. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.S.; Ahn, S.S.; Lee, S.-K.; Chang, J.H.; Kang, S.-G.; Kim, S.H.; Zhou, J. Amide Proton Transfer Imaging to Discriminate between Low- and High-Grade Gliomas: Added Value to Apparent Diffusion Coefficient and Relative Cerebral Blood Volume. Eur. Radiol. 2017, 27, 3181–3189. [Google Scholar] [CrossRef]
- Ulyte, A.; Katsaros, V.K.; Liouta, E.; Stranjalis, G.; Boskos, C.; Papanikolaou, N.; Usinskiene, J.; Bisdas, S. Prognostic Value of Preoperative Dynamic Contrast-Enhanced MRI Perfusion Parameters for High-Grade Glioma Patients. Neuroradiology 2016, 58, 1197–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.; Li, J.; Diao, Q.; Lin, Y.; Zhang, J.; Li, L.; Yang, G.; Fang, X.; Li, X.; Chen, Y.; et al. Assessment of Glioma Response to Radiotherapy Using 3D Pulsed-Continuous Arterial Spin Labeling and 3D Segmented Volume. Eur. J. Radiol. 2016, 85, 1987–1992. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Zhao, B.; Wang, G.; Xiang, J.; Xu, S.; Liu, Y.; Zhao, P.; Pfeuffer, J.; Qian, T. Improving the Grading Accuracy of Astrocytic Neoplasms Noninvasively by Combining Timing Information with Cerebral Blood Flow: A Multi-TI Arterial Spin-Labeling MR Imaging Study. Am. J. Neuroradiol. 2016, 37, 2209–2216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, N.; Shaukat, A.; Rehan, A.; Rashid, S. Diagnostic Accuracy of Perfusion Computed Tomography in Cerebral Glioma Grading. J. Coll. Physicians Surg. Pak. 2016, 26, 562–565. [Google Scholar] [PubMed]
- Santarosa, C.; Castellano, A.; Conte, G.M.; Cadioli, M.; Iadanza, A.; Terreni, M.R.; Franzin, A.; Bello, L.; Caulo, M.; Falini, A.; et al. Dynamic Contrast-Enhanced and Dynamic Susceptibility Contrast Perfusion MR Imaging for Glioma Grading: Preliminary Comparison of Vessel Compartment and Permeability Parameters Using Hotspot and Histogram Analysis. Eur. J. Radiol. 2016, 85, 1147–1156. [Google Scholar] [CrossRef]
- Shen, N.; Zhao, L.; Jiang, J.; Jiang, R.; Su, C.; Zhang, S.; Tang, X.; Zhu, W. Intravoxel Incoherent Motion Diffusion-Weighted Imaging Analysis of Diffusion and Microperfusion in Grading Gliomas and Comparison with Arterial Spin Labeling for Evaluation of Tumor Perfusion. J. Magn. Reson. Imaging 2016, 44, 620–632. [Google Scholar] [CrossRef]
- Gao, F.; Guo, R.; Hu, X.-J.; Li, C.-J.; Li, M. Noninvasive Tumor Grading of Glioblastomas Before Surgery Using Arterial Spin Labeling. A Cohort Study. Available online: https://pubmed.ncbi.nlm.nih.gov/26860009/ (accessed on 2 February 2021).
- Sunwoo, L.; Choi, S.H.; Yoo, R.-E.; Kang, K.M.; Yun, T.J.; Kim, T.M.; Lee, S.-H.; Park, C.-K.; Kim, J.; Park, S.-W.; et al. Paradoxical Perfusion Metrics of High-Grade Gliomas with an Oligodendroglioma Component: Quantitative Analysis of Dynamic Susceptibility Contrast Perfusion MR Imaging. Neuroradiology 2015, 57, 1111–1120. [Google Scholar] [CrossRef]
- Smitha, K.A.; Gupta, A.K.; Jayasree, R.S. Relative Percentage Signal Intensity Recovery of Perfusion Metrics—an Efficient Tool for Differentiating Grades of Glioma. BJR 2015, 88, 20140784. [Google Scholar] [CrossRef] [Green Version]
- Xiao, H.-F.; Chen, Z.-Y.; Lou, X.; Wang, Y.-L.; Gui, Q.-P.; Wang, Y.; Shi, K.-N.; Zhou, Z.-Y.; Zheng, D.-D.; Wang, D.J.J.; et al. Astrocytic Tumour Grading: A Comparative Study of Three-Dimensional Pseudocontinuous Arterial Spin Labelling, Dynamic Susceptibility Contrast-Enhanced Perfusion-Weighted Imaging, and Diffusion-Weighted Imaging. Eur. Radiol. 2015, 25, 3423–3430. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Li, J.; Zhang, Z.; Xu, Q.; Zhou, Z.; Zhang, Z.; Zhang, Y.; Zhang, Z. Comparison of Intravoxel Incoherent Motion Diffusion-Weighted MR Imaging and Arterial Spin Labeling MR Imaging in Gliomas. Available online: https://www.hindawi.com/journals/bmri/2015/234245/ (accessed on 2 February 2021).
- Arevalo-Perez, J.; Peck, K.K.; Young, R.J.; Holodny, A.I.; Karimi, S.; Lyo, J.K. Dynamic Contrast-Enhanced Perfusion MRI and Diffusion-Weighted Imaging in Grading of Gliomas. J. Neuroimaging 2015, 25, 792–798. [Google Scholar] [CrossRef] [Green Version]
- Aprile, I.; Giovannelli, G.; Fiaschini, P.; Muti, M.; Kouleridou, A.; Caputo, N. High- and Low-Grade Glioma Differentiation: The Role of Percentage Signal Recovery Evaluation in MR Dynamic Susceptibility Contrast Imaging. Radiol. Med. 2015, 120, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Tietze, A.; Mouridsen, K.; Mikkelsen, I.K. The Impact of Reliable Prebolus T1 Measurements or a Fixed T1 Value in the Assessment of Glioma Patients with Dynamic Contrast Enhancing MRI. Neuroradiology 2015, 57, 561–572. [Google Scholar] [CrossRef] [PubMed]
- Tietze, A.; Boldsen, J.K.; Mouridsen, K.; Ribe, L.; Dyve, S.; Cortnum, S.; Østergaard, L.; Borghammer, P. Spatial Distribution of Malignant Tissue in Gliomas: Correlations of 11C-L-Methionine Positron Emission Tomography and Perfusion- and Diffusion-Weighted Magnetic Resonance Imaging. Acta Radiol. 2015, 56, 1135–1144. [Google Scholar] [CrossRef] [PubMed]
- Cebeci, H.; Aydin, O.; Ozturk-Isik, E.; Gumus, C.; Inecikli, F.; Bekar, A.; Kocaeli, H.; Hakyemez, B. Assesment of Perfusion in Glial Tumors with Arterial Spin Labeling; Comparison with Dynamic Susceptibility Contrast Method. Eur. J. Radiol. 2014, 83, 1914–1919. [Google Scholar] [CrossRef]
- Fudaba, H.; Shimomura, T.; Abe, T.; Matsuta, H.; Momii, Y.; Sugita, K.; Ooba, H.; Kamida, T.; Hikawa, T.; Fujiki, M. Comparison of Multiple Parameters Obtained on 3T Pulsed Arterial Spin-Labeling, Diffusion Tensor Imaging, and MRS and the Ki-67 Labeling Index in Evaluating Glioma Grading. Am. J. Neuroradiol. 2014, 35, 2091–2098. [Google Scholar] [CrossRef] [Green Version]
- Van Cauter, S.; De Keyzer, F.; Sima, D.M.; Croitor Sava, A.; D’Arco, F.; Veraart, J.; Peeters, R.R.; Leemans, A.; Van Gool, S.; Wilms, G.; et al. Integrating Diffusion Kurtosis Imaging, Dynamic Susceptibility-Weighted Contrast-Enhanced MRI, and Short Echo Time Chemical Shift Imaging for Grading Gliomas. Neuro-Oncology 2014, 16, 1010–1021. [Google Scholar] [CrossRef]
- Alexiou, G.A.; Zikou, A.; Tsiouris, S.; Goussia, A.; Kosta, P.; Papadopoulos, A.; Voulgaris, S.; Kyritsis, A.P.; Fotopoulos, A.D.; Argyropoulou, M.I. Correlation of Diffusion Tensor, Dynamic Susceptibility Contrast MRI and 99mTc-Tetrofosmin Brain SPECT with Tumour Grade and Ki-67 Immunohistochemistry in Glioma. Clin. Neurol. Neurosurg. 2014, 116, 41–45. [Google Scholar] [CrossRef]
- Yoon, J.H.; Kim, J.; Kang, W.J.; Sohn, C.-H.; Choi, S.H.; Yun, T.J.; Eun, Y.; Song, Y.S.; Chang, K.-H. Grading of Cerebral Glioma with Multiparametric MR Imaging and 18F-FDG-PET: Concordance and Accuracy. Eur. Radiol. 2014, 24, 380–389. [Google Scholar] [CrossRef]
- Kim, H.; Choi, S.H.; Kim, J.-H.; Ryoo, I.; Kim, S.C.; Yeom, J.A.; Shin, H.; Jung, S.C.; Lee, A.L.; Yun, T.J.; et al. Gliomas: Application of Cumulative Histogram Analysis of Normalized Cerebral Blood Volume on 3 T MRI to Tumor Grading. PLoS ONE 2013, 8, e63462. [Google Scholar] [CrossRef]
- Roy, B.; Awasthi, R.; Bindal, A.; Sahoo, P.; Kumar, R.; Behari, S.; Ojha, B.K.; Husain, N.; Pandey, C.M.; Rathore, R.K.S.; et al. Comparative Evaluation of 3-Dimensional Pseudocontinuous Arterial Spin Labeling With Dynamic Contrast-Enhanced Perfusion Magnetic Resonance Imaging in Grading of Human Glioma. J. Comput. Assist. Tomogr. 2013, 37, 321–326. [Google Scholar] [CrossRef]
- Awasthi, R.; Rathore, R.K.S.; Soni, P.; Sahoo, P.; Awasthi, A.; Husain, N.; Behari, S.; Singh, R.K.; Pandey, C.M.; Gupta, R.K. Discriminant Analysis to Classify Glioma Grading Using Dynamic Contrast-Enhanced MRI and Immunohistochemical Markers. Neuroradiology 2012, 54, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Emblem, K.E.; Scheie, D.; Due-Tonnessen, P.; Nedregaard, B.; Nome, T.; Hald, J.K.; Beiske, K.; Meling, T.R.; Bjornerud, A. Histogram Analysis of MR Imaging–Derived Cerebral Blood Volume Maps: Combined Glioma Grading and Identification of Low-Grade Oligodendroglial Subtypes. Am. J. Neuroradiol. 2008, 29, 1664–1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comte, F.; Bauchet, L.; Rigau, V.; Hauet, J.R.; Fabbro, M.; Coubes, P.; Chevalier, J.; Mariano-Goulart, D.; Rossi, M.; Zanca, M. Correlation of Preoperative Thallium SPECT with Histological Grading and Overall Survival in Adult Gliomas. Nucl. Med. Commun. 2006, 27, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Warmuth, C.; Günther, M.; Zimmer, C. Quantification of Blood Flow in Brain Tumors: Comparison of Arterial Spin Labeling and Dynamic Susceptibility-Weighted Contrast-Enhanced MR Imaging. Radiology 2003, 228, 523–532. [Google Scholar] [CrossRef] [Green Version]
- Boxerman, J.L.; Schmainda, K.M.; Weisskoff, R.M. Relative Cerebral Blood Volume Maps Corrected for Contrast Agent Extravasation Significantly Correlate with Glioma Tumor Grade, Whereas Uncorrected Maps Do Not. Am. J. Neuroradiol. 2006, 27, 859–867. [Google Scholar]
- Lucas, J.T., Jr.; Knapp, B.J.; Uh, J.; Hua, C.-H.; Merchant, T.E.; Hwang, S.N.; Patay, Z.; Broniscer, A. Posttreatment DSC-MRI Is Predictive of Early Treatment Failure in Children with Supratentorial High-Grade Glioma Treated with Erlotinib. Clin. Neuroradiol. 2018, 28, 393–400. [Google Scholar] [CrossRef]
- Tateishi, K.; Tateishi, U.; Sato, M.; Yamanaka, S.; Kanno, H.; Murata, H.; Inoue, T.; Kawahara, N. Application of 62Cu-Diacetyl-Bis (N4-Methylthiosemicarbazone) PET Imaging to Predict Highly Malignant Tumor Grades and Hypoxia-Inducible Factor-1α Expression in Patients with Glioma. Am. J. Neuroradiol. 2013, 34, 92–99. [Google Scholar] [CrossRef] [Green Version]
- Law, M.; Yang, S.; Wang, H.; Babb, J.S.; Johnson, G.; Cha, S.; Knopp, E.A.; Zagzag, D. Glioma Grading: Sensitivity, Specificity, and Predictive Values of Perfusion MR Imaging and Proton MR Spectroscopic Imaging Compared with Conventional MR Imaging. Am. J. Neuroradiol. 2003, 24, 1989–1998. [Google Scholar]
- Hong, E.K.; Choi, S.H.; Shin, D.J.; Jo, S.W.; Yoo, R.-E.; Kang, K.M.; Yun, T.J.; Kim, J.; Sohn, C.-H.; Park, S.-H.; et al. Comparison of Genetic Profiles and Prognosis of High-Grade Gliomas Using Quantitative and Qualitative MRI Features: A Focus on G3 Gliomas. Korean J. Radiol. 2021, 22, 233–242. [Google Scholar] [CrossRef]
- Shin, J.H.; Lee, H.K.; Kwun, B.D.; Kim, J.-S.; Kang, W.; Choi, C.G.; Suh, D.C. Using Relative Cerebral Blood Flow and Volume to Evaluate the Histopathologic Grade of Cerebral Gliomas: Preliminary Results. Am. J. Roentgenol. 2002, 179, 783–789. [Google Scholar] [CrossRef]
- Law, M.; Young, R.; Babb, J.; Pollack, E.; Johnson, G. Histogram Analysis versus Region of Interest Analysis of Dynamic Susceptibility Contrast Perfusion MR Imaging Data in the Grading of Cerebral Gliomas. Am. J. Neuroradiol. 2007, 28, 761–766. [Google Scholar] [PubMed]
- Spampinato, M.V.; Smith, J.K.; Kwock, L.; Ewend, M.; Grimme, J.D.; Camacho, D.L.A.; Castillo, M. Cerebral Blood Volume Measurements and Proton MR Spectroscopy in Grading of Oligodendroglial Tumors. Am. J. Roentgenol. 2007, 188, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Maia, A.C.M.; Malheiros, S.M.F.; da Rocha, A.J.; da Silva, C.J.; Gabbai, A.A.; Ferraz, F.A.P.; Stávale, J.N. MR Cerebral Blood Volume Maps Correlated with Vascular Endothelial Growth Factor Expression and Tumor Grade in Nonenhancing Gliomas. Am. J. Neuroradiol. 2005, 26, 777–783. [Google Scholar]
- McCullough, B.J.; Ader, V.; Aguedan, B.; Feng, X.; Susanto, D.; Benkers, T.L.; Henson, J.W.; Mayberg, M.; Cobbs, C.S.; Gwinn, R.P.; et al. Preoperative Relative Cerebral Blood Volume Analysis in Gliomas Predicts Survival and Mitigates Risk of Biopsy Sampling Error. J. Neurooncol. 2018, 136, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Lefranc, M.; Monet, P.; Desenclos, C.; Peltier, J.; Fichten, A.; Toussaint, P.; Sevestre, H.; Deramond, H.; Gars, D.L. Perfusion MRI as a Neurosurgical Tool for Improved Targeting in Stereotactic Tumor Biopsies. SFN 2012, 90, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Luan, J.; Wu, M.; Wang, X.; Qiao, L.; Guo, G.; Zhang, C. The Diagnostic Value of Quantitative Analysis of ASL, DSC-MRI and DKI in the Grading of Cerebral Gliomas: A Meta-Analysis. Radiat. Oncol. 2020, 15, 204. [Google Scholar] [CrossRef] [PubMed]
- Delgado, A.F.; Delgado, A.F. Discrimination between Glioma Grades II and III Using Dynamic Susceptibility Perfusion MRI: A Meta-Analysis. Am. J. Neuroradiol. 2017, 38, 1348–1355. [Google Scholar] [CrossRef] [Green Version]
- Abrigo, J.M.; Fountain, D.M.; Provenzale, J.M.; Law, E.K.; Kwong, J.S.; Hart, M.G.; Tam, W.W.S. Magnetic Resonance Perfusion for Differentiating Low-Grade from High-Grade Gliomas at First Presentation. Cochrane Database Syst. Rev. 2018, 1, CD011551. [Google Scholar] [CrossRef]
- Pauliah, M.; Saxena, V.; Haris, M.; Husain, N.; Rathore, R.K.S.; Gupta, R.K. Improved T1-Weighted Dynamic Contrast-Enhanced MRI to Probe Microvascularity and Heterogeneity of Human Glioma. Magn. Reson. Imaging 2007, 25, 1292–1299. [Google Scholar] [CrossRef]
- Brendle, C.; Hempel, J.-M.; Schittenhelm, J.; Skardelly, M.; Tabatabai, G.; Bender, B.; Ernemann, U.; Klose, U. Glioma Grading and Determination of IDH Mutation Status and ATRX Loss by DCE and ASL Perfusion. Clin. Neuroradiol. 2018, 28, 421–428. [Google Scholar] [CrossRef]
- Li, X.; Zhu, Y.; Kang, H.; Zhang, Y.; Liang, H.; Wang, S.; Zhang, W. Glioma Grading by Microvascular Permeability Parameters Derived from Dynamic Contrast-Enhanced MRI and Intratumoral Susceptibility Signal on Susceptibility Weighted Imaging. Cancer Imaging 2015, 15, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, K.E.; Ahn, K.J.; Choi, H.S.; Jung, S.L.; Kim, B.S.; Jeon, S.S.; Hong, Y.G. DCE and DSC MR Perfusion Imaging in the Differentiation of Recurrent Tumour from Treatment-Related Changes in Patients with Glioma. Clin. Radiol. 2014, 69, e264–e272. [Google Scholar] [CrossRef] [PubMed]
- Haris, M.; Husain, N.; Singh, A.; Husain, M.; Srivastava, S.; Srivastava, C.; Behari, S.; Rathore, R.K.S.; Saksena, S.; Gupta, R.K. Dynamic Contrast-Enhanced Derived Cerebral Blood Volume Correlates Better With Leak Correction Than With No Correction for Vascular Endothelial Growth Factor, Microvascular Density, and Grading of Astrocytoma. J. Comput. Assist. Tomogr. 2008, 32, 955–965. [Google Scholar] [CrossRef] [PubMed]
- Mills, S.J.; Patankar, T.A.; Haroon, H.A.; Balériaux, D.; Swindell, R.; Jackson, A. Do Cerebral Blood Volume and Contrast Transfer Coefficient Predict Prognosis in Human Glioma? Am. J. Neuroradiol. 2006, 27, 853–858. [Google Scholar]
- Trinh, A.; Wintermark, M.; Iv, M. Clinical Review of Computed Tomography and MR Perfusion Imaging in Neuro-Oncology. Radiol. Clin. N. Am. 2021, 59, 323–334. [Google Scholar] [CrossRef]
- Law, M.; Young, R.; Babb, J.; Rad, M.; Sasaki, T.; Zagzag, D.; Johnson, G. Comparing Perfusion Metrics Obtained from a Single Compartment Versus Pharmacokinetic Modeling Methods Using Dynamic Susceptibility Contrast-Enhanced Perfusion MR Imaging with Glioma Grade. Am. J. Neuroradiol. 2006, 27, 1975–1982. [Google Scholar]
- Nguyen, T.B.; Cron, G.O.; Mercier, J.F.; Foottit, C.; Torres, C.H.; Chakraborty, S.; Woulfe, J.; Jansen, G.H.; Caudrelier, J.M.; Sinclair, J.; et al. Preoperative Prognostic Value of Dynamic Contrast-Enhanced MRI–Derived Contrast Transfer Coefficient and Plasma Volume in Patients with Cerebral Gliomas. Am. J. Neuroradiol. 2015, 36, 63–69. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Wei, L.; Wang, J.; Li, N.; Gao, Y.; Ma, H.; Qu, X.; Zhang, M. Evaluation of Perfusion MRI Value for Tumor Progression Assessment after Glioma Radiotherapy: A Systematic Review and Meta-Analysis. Medicine 2020, 99, e23766. [Google Scholar] [CrossRef]
- Kong, L.; Chen, H.; Yang, Y.; Chen, L. A Meta-Analysis of Arterial Spin Labelling Perfusion Values for the Prediction of Glioma Grade. Clin. Radiol. 2017, 72, 255–261. [Google Scholar] [CrossRef]
- Falk Delgado, A.; De Luca, F.; van Westen, D.; Falk Delgado, A. Arterial Spin Labeling MR Imaging for Differentiation between High- and Low-Grade Glioma—A Meta-Analysis. Neuro-Oncology 2018, 20, 1450–1461. [Google Scholar] [CrossRef]
- Alsaedi, A.; Doniselli, F.; Jäger, H.R.; Panovska-Griffiths, J.; Rojas-Garcia, A.; Golay, X.; Bisdas, S. The Value of Arterial Spin Labelling in Adults Glioma Grading: Systematic Review and Meta-Analysis. Oncotarget 2019, 10, 1589–1601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellika, S.K.; Jain, R.; Patel, S.C.; Scarpace, L.; Schultz, L.R.; Rock, J.P.; Mikkelsen, T. Role of Perfusion CT in Glioma Grading and Comparison with Conventional MR Imaging Features. Am. J. Neuroradiol. 2007, 28, 1981–1987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, B.; Ling, H.W.; Chen, K.M.; Jiang, H.; Zhu, Y.B. Comparison of Cerebral Blood Volume and Permeability in Preoperative Grading of Intracranial Glioma Using CT Perfusion Imaging. Neuroradiology 2006, 48, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Boxerman, J.L.; Quarles, C.C.; Hu, L.S.; Erickson, B.J.; Gerstner, E.R.; Smits, M.; Kaufmann, T.J.; Barboriak, D.P.; Huang, R.H.; Wick, W.; et al. Consensus Recommendations for a Dynamic Susceptibility Contrast MRI Protocol for Use in High-Grade Gliomas. Neuro Oncol. 2020, 22, 1262–1275. [Google Scholar] [CrossRef] [PubMed]
- Ellingson, B.M.; Bendszus, M.; Boxerman, J.; Barboriak, D.; Erickson, B.J.; Smits, M.; Nelson, S.J.; Gerstner, E.; Alexander, B.; Goldmacher, G.; et al. Consensus Recommendations for a Standardized Brain Tumor Imaging Protocol in Clinical Trials. Neuro. Oncol. 2015, 17, 1188–1198. [Google Scholar] [CrossRef] [Green Version]
- Welker, K.; Boxerman, J.; Kalnin, A.; Kaufmann, T.; Shiroishi, M.; Wintermark, M.; American Society of Functional Neuroradiology MR Perfusion Standards and Practice Subcommittee of the ASFNR Clinical Practice Committee. ASFNR Recommendations for Clinical Performance of MR Dynamic Susceptibility Contrast Perfusion Imaging of the Brain. Am. J. Neuroradiol. 2015, 36, E41–E51. [Google Scholar] [CrossRef] [Green Version]
- Alsop, D.C.; Detre, J.A.; Golay, X.; Günther, M.; Hendrikse, J.; Hernandez-Garcia, L.; Lu, H.; MacIntosh, B.J.; Parkes, L.M.; Smits, M.; et al. Recommended Implementation of Arterial Spin-Labeled Perfusion MRI for Clinical Applications: A Consensus of the ISMRM Perfusion Study Group and the European Consortium for ASL in Dementia. Magn. Reson. Med. 2015, 73, 102–116. [Google Scholar] [CrossRef] [Green Version]
- Mutsaerts, H.J.M.M.; Petr, J.; Groot, P.; Vandemaele, P.; Ingala, S.; Robertson, A.D.; Václavů, L.; Groote, I.; Kuijf, H.; Zelaya, F.; et al. ExploreASL: An Image Processing Pipeline for Multi-Center ASL Perfusion MRI Studies. NeuroImage 2020, 219, 117031. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| DSC-MRI | DCE-MRI | ASL-MRI | BOLD-CVR | PCT | PET | SPECT | |
|---|---|---|---|---|---|---|---|
| Contrast agent | GBCA | GBCA | - | - | IBCA | 15-O2, H2150, C15O2 | 133Xe, 99mTc-HMPAO, 99mTc-ECD, 123i-IMP |
| Radiation exposure | - | - | - | - | +++ | + | - |
| Data model analysis | Meier–Zierler [39] | Meier-Zierler [39]; Tissue-homogeneity model, modified Tofts model, three-parameter models, two-parameter models, on-parameter models [47] | Kety–Schmidt [40] | Fürst et al. [61] | Meier–Zierler [39] | Kety–Schmidt [40] | Kety–Schmidt [40] |
| Assessed parameters * | CBV, CBF, MTT | Ktrans, Ve, Vp, Kep (CBV, CBF, MTT) | CBF | CVR | CBV, CBF, MTT, Ktrans, Ve, Vp, Kep | CBF, CBV, OEF | CBF |
| Strenghts | Lack of radiation exposure and use of iodinated CA; Combination with standard MRI sequences for a more comprehensive assessment of brain tumors | Lack of radiation exposure and use of iodinated CA; Combination with standard MRI sequences for a more comprehensive assessment of brain tumors; Higher spatial resolution than DSC | Non-invasive No need of GBCA | Non-invasive No need of GBCA | Linear relationship of tissue signal intensity with tissue contrast agent, allows measurement of permeability parameters | Accurate quantitative measurements Repeatibility due to short half of radiotracers | Low costs, Feasibility in emergency settings |
| Limitations | Indirect detection of the injected CA; Competing T1 contrast effect due to CA leakage through BBB **; Challenging measurement of AIF | Indirect detection of the injected CA; Choice of the most appropriate analysis models among the different existing ones; High temporal resolution required; Dependency from the CA extraction fraction Challenging measurement of AIF | Poor labeling efficiency, blood transport through vessels and tissue, proton water diffusion through the BBB, low SNR, high sensitivity from patient motion and magnetization transfer effects. Challenging measurement of AIF | Possible light patient discomfort due to carbon dioxide stimulus | Reduced anatomic coverage | High costs, impossibility to use in the emergency clinical settings | Poor spatial resolution |
| Suggested readings | Shiroishi et al. [62] and Quarles et al. [45] | Sourbron and Buckley [47] | Buxton et al. [63] and Calamante et al. [37] | Buxton et al. [64] Fisher et al. [65,66] | Jain et al. [51] | Zhang et al. [67] | Zhang et al. [67] |
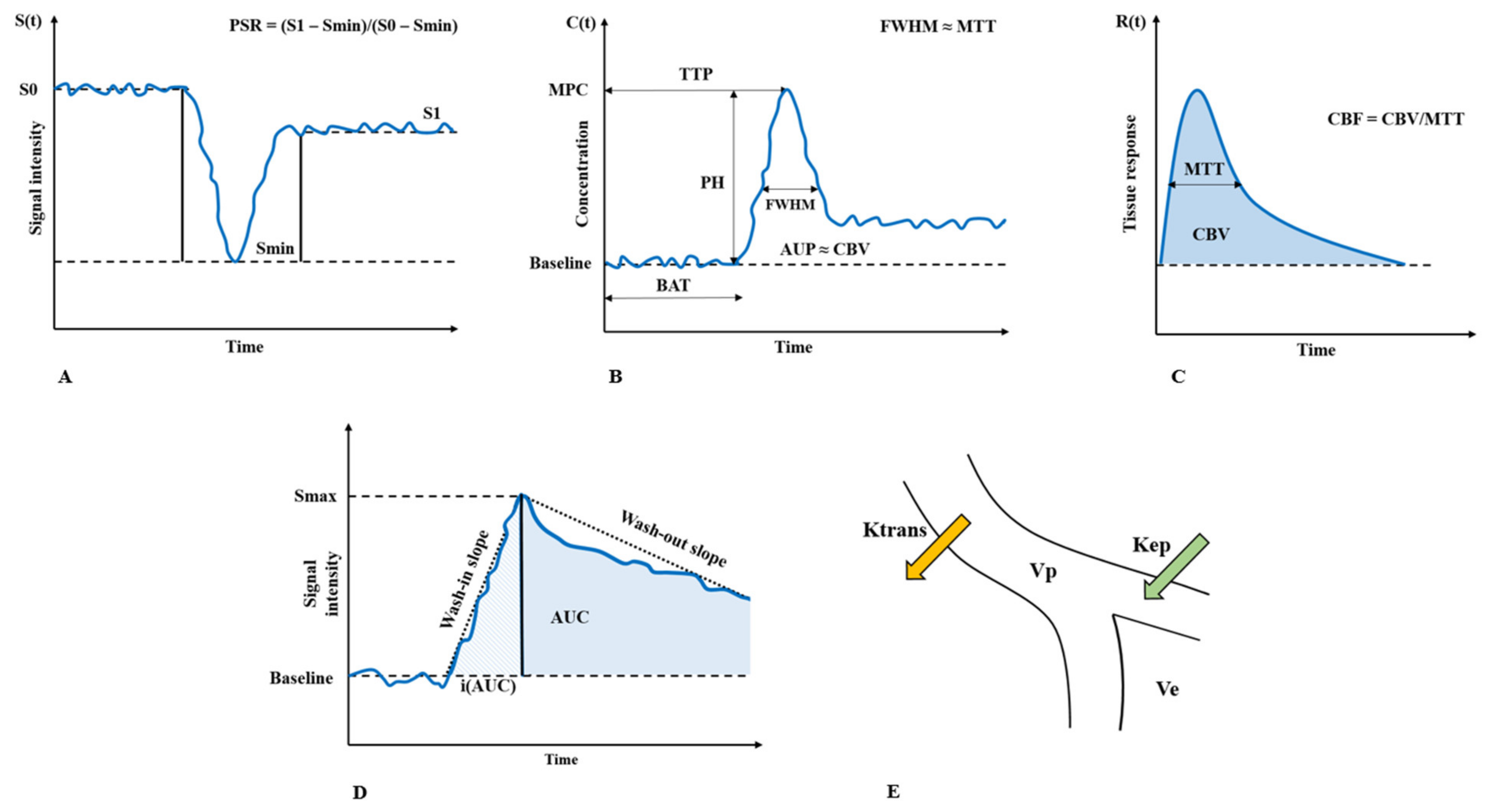
| Parameter | Interpretation | Explanation | Units |
|---|---|---|---|
| CBV | Cerebral blood volume | Quantity of blood in a given amount of brain tissue. It is considered a surrogate of microvascular density. | mL of blood/100 g tissue |
| CBF | Cerebral blood flow | Rate of delivery of arterial blood to a capillary bed in tissue. | mL of blood/100 g of tissue/min |
| MTT | Mean transit time | Average time that red blood cells spend within a determinate volume of capillary circulation. It is calculated as CBV/CBF. | s |
| Ktrans | Volume transfer constant between blood plasma and extravascular extracellular space | Measure of capillary permeability, is considered a good indicator of BBB leakiness. It should be noted that in situation of high permeability (disrupted BBB) this parameter is more reflective of CBF. | 1/min |
| Ve | Extravascular extracellular volume fraction | Quantification of cellularity and necrosis in extravascular extracellular space | mL/100 mL |
| Vp | Blood plasma fractional volume | Quantification of the volume of blood plasma | mL/100 mL |
| Kep | Rate constant from extravascular extracellular space into blood plasma | Flux rate constant between the EES and blood plasma. It can be derived as Ktrans/Ve. | 1/min |
| TTP * | Time to peak | Time at which contrast concentration reaches its maximum. | s |
| BAT * | Bolus arrival time | Time from CA bolus injection to measured concentration changes in the observed ROI | s |
| MPC * | Maximum peak-concentration | Maximal CA concentration in the observed ROI | mL/100 mL |
| FMWH * | Full-width at half-maximum concentration | Measure of the width at half the maximum value of peaked concentration–time curve | s |
| AUP * | Area under the peak | Area under the peaked concentration–time curve | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guida, L.; Stumpo, V.; Bellomo, J.; van Niftrik, C.H.B.; Sebök, M.; Berhouma, M.; Bink, A.; Weller, M.; Kulcsar, Z.; Regli, L.; et al. Hemodynamic Imaging in Cerebral Diffuse Glioma—Part A: Concept, Differential Diagnosis and Tumor Grading. Cancers 2022, 14, 1432. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061432
Guida L, Stumpo V, Bellomo J, van Niftrik CHB, Sebök M, Berhouma M, Bink A, Weller M, Kulcsar Z, Regli L, et al. Hemodynamic Imaging in Cerebral Diffuse Glioma—Part A: Concept, Differential Diagnosis and Tumor Grading. Cancers. 2022; 14(6):1432. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061432
Chicago/Turabian StyleGuida, Lelio, Vittorio Stumpo, Jacopo Bellomo, Christiaan Hendrik Bas van Niftrik, Martina Sebök, Moncef Berhouma, Andrea Bink, Michael Weller, Zsolt Kulcsar, Luca Regli, and et al. 2022. "Hemodynamic Imaging in Cerebral Diffuse Glioma—Part A: Concept, Differential Diagnosis and Tumor Grading" Cancers 14, no. 6: 1432. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061432