
The Role of Surgery in Spinal Intradural Metastases from Renal Cell Carcinoma: A Literature Review



Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
3. Results
3.1. Literature Review of Intradural Extramedullary (IDEM) Spinal Metastasis
3.2. Literature Review of Intramedullary Spinal Cord Metastasis (ISCMs)
3.3. Intradural Extramedullary and Intramedullary Spinal Cord Metastases from RCC at Mirror
4. Discussion
4.1. Intradural Extramedullary (IDEM) Spinal Metastases
4.2. Intramedullary Spinal Cord Metastases (ISCMs)
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Saad, A.M.; Gad, M.M.; Al-Husseini, M.J.; Ruhban, I.A.; Sonbol, M.B.; Ho, T.H. Trends in Renal-Cell Carcinoma Incidence and Mortality in the United States in the Last 2 Decades: A SEER-Based Study. Clin. Genitourin. Cancer 2019, 17, 46–57.e45. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Motzer, R.J. Systemic Therapy for Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2017, 376, 354–366. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.C.; Desai, K.; Zhang, T.; Ornstein, M.C. The Immunotherapy Landscape in Renal Cell Carcinoma. BioDrugs 2020, 34, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Dabestani, S.; Thorstenson, A.; Lindblad, P.; Harmenberg, U.; Ljungberg, B.; Lundstam, S. Renal cell carcinoma recurrences and metastases in primary non-metastatic patients: A population-based study. World J. Urol. 2016, 34, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, M.; Sun, M.; Jeldres, C.; Shariat, S.F.; Trinh, Q.D.; Briganti, A.; Tian, Z.; Schmitges, J.; Graefen, M.; Perrotte, P.; et al. Distribution of metastatic sites in renal cell carcinoma: A population-based analysis. Ann. Oncol. 2012, 23, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Mariniello, G.; Corvino, S.; Sgulò, F.; Guadagno, G.; Del Basso De Caro, M.; Maiuri, F. Intradural cauda equina metastases from renal cell carcinoma. Interdiscip. Neurosurg 2022, 27, 101397. [Google Scholar] [CrossRef]
- Takahashi, I.; Isu, T.; Iwasaki, Y.; Akino, M.; Takahashi, A.; Abe, H.; Kitagawa, M.; Kojima, H.; Inoue, K.; Saitoh, H. Metastatic Grawitz’s tumor to the cauda equina: Case report. No Shinkei Geka 1990, 18, 1157–1160. [Google Scholar]
- Maxwell, M.; Borges, L.F.; Zervas, N.T. Renal cell carcinoma: A rare source of cauda equina metastasis. Case report. J. Neurosurg. 1999, 90, 129–132. [Google Scholar] [CrossRef]
- Mak, K.H.; Kwok, J.C. Intradural spinal metastasis from renal cell carcinoma: A case report. J. Orthop. Surg. 2001, 9, 57–61. [Google Scholar] [CrossRef] [Green Version]
- Kubota, M.; Saeki, N.; Yamaura, A.; Iuchi, T.; Ohga, M.; Osato, K. A rare case of metastatic renal cell carcinoma resembling a nerve sheath tumor of the cauda equina. J. Clin. Neurosci. 2004, 11, 530–532. [Google Scholar] [CrossRef]
- Takada, T.; Doita, M.; Nishida, K.; Miura, J.; Yoshiya, S.; Kurosaka, M. Unusual metastasis to the cauda equina from renal cell carcinoma. Spine 2003, 28, E114–E117. [Google Scholar] [CrossRef]
- Gaetani, P.; Di Ieva, A.; Colombo, P.; Tancioni, F.; Aimar, E.; Debernardi, A.; Rodriguez, Y.; Baena, R. Intradural spinal metastasis of renal clear cell carcinoma causing cauda equina syndrome. Acta Neurochir. 2004, 146, 857–861. [Google Scholar] [CrossRef]
- Alfieri, A.; Mazzoleni, G.; Schwarz, A.; Campello, M.; Broger, M.; Vitale, M.; Vigl, E.E. Renal cell carcinoma and intradural spinal metastasis with cauda equina infiltration: Case report. Spine 2005, 30, 161–163. [Google Scholar] [CrossRef]
- Jost, G.; Zimmerer, S.; Frank, S.; Cordier, D.; Merlo, A. Intradural spinal metastasis of renal cell cancer. Report of a case and review of 26 published cases. Acta Neurochir. 2009, 151, 815–821, discussion 821. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.Y.; Lee, J.K.; Moon, S.J.; Kim, S.C.; Kim, C.S. Intradural spinal metastasis to the cauda equina in renal cell carcinoma: A case report and review of the literature. Spine 2009, 34, E892–E895. [Google Scholar] [CrossRef]
- Lin, T.K.; Chen, S.M.; Jung, S.M. Solitary intradural extramedullary metastasis of renal cell carcinoma to the conus medullaris. Kaohsiung J. Med. Sci. 2011, 27, 45–48. [Google Scholar] [CrossRef] [Green Version]
- Dobson, G.M.; Polvikoski, T.; Nissen, J.J.; Holliman, D. Cauda equina syndrome secondary to intradural renal cell carcinoma metastasis haemorrhage. Br. J. Neurosurg. 2013, 27, 249–250. [Google Scholar] [CrossRef]
- Ji, G.Y.; Oh, C.H.; Kim, S.H.; Shin, D.A.; Kim, K.N. Intradural cauda equina metastasis of renal cell carcinoma: A case report with literature review of 10 cases. Spine 2013, 38, E1171–E1174. [Google Scholar] [CrossRef]
- Strong, C.; Yanamadala, V.; Khanna, A.; Walcott, B.P.; Nahed, B.V.; Borges, L.F.; Coumans, J.V. Surgical treatment options and management strategies of metastatic renal cell carcinoma to the lumbar spinal nerve roots. J. Clin. Neurosci. 2013, 20, 1546–1549. [Google Scholar] [CrossRef] [Green Version]
- Srinivasan, A.; Dhandapani, S.; Chatterjee, D.; Simha, V. Renal small cell carcinoma presenting with solitary lumbar intradural metastasis. Neurol. India 2014, 62, 561–563. [Google Scholar] [CrossRef]
- Carminucci, A.; Hanft, S. Intradural extramedullary spinal metastasis of renal cell carcinoma: Illustrative case report and comprehensive review of the literature. Eur. Spine J. 2020, 29, 176–182. [Google Scholar] [CrossRef]
- Ali, S.; Qasim, A.; Salah, R.; Sarwar, M.R.; Usman, M.; Shams, S. Isolated late intradural cauda equina metastasis of renal cell carcinoma. Surg. Neurol. Int. 2021, 12, 481. [Google Scholar] [CrossRef]
- Capek, S.; Krauss, W.E.; Amrami, K.K.; Parisi, J.E.; Spinner, R.J. Perineural Spread of Renal Cell Carcinoma: A Case Illustration with a Proposed Anatomic Mechanism and a Review of the Literature. World Neurosurg. 2016, 89, 728.e11–728.e17. [Google Scholar] [CrossRef]
- Madhavan, A.A.; Eckel, L.J.; Carr, C.M.; Diehn, F.E.; Lehman, V.T. Subdural spinal metastases detected on CT myelography: A case report and brief review. Radiol. Case Rep. 2021, 16, 1499–1503. [Google Scholar] [CrossRef] [PubMed]
- Ateaque, A.; Martin, J.L.; O’Brien, C. Intramedullary spinal cord metastases from a hypernephroma 11 years following the diagnosis and treatment of the primary lesion. Br. J. Neurosurg. 2000, 14, 474–476. [Google Scholar] [CrossRef] [PubMed]
- Schijns, O.E.; Kurt, E.; Wessels, P.; Luijckx, G.J.; Beuls, E.A. Intramedullary spinal cord metastasis as a first manifestation of a renal cell carcinoma: Report of a case and review of the literature. Clin. Neurol. Neurosurg. 2000, 102, 249–254. [Google Scholar] [CrossRef]
- Fakih, M.; Schiff, D.; Erlich, R.; Logan, T.F. Intramedullary spinal cord metastasis (ISCM) in renal cell carcinoma: A series of six cases. Ann. Oncol. 2001, 12, 1173–1177. [Google Scholar] [CrossRef] [PubMed]
- Poggi, M.M.; Patronas, N.; Buttman, J.A.; Hewitt, S.M.; Fuller, B. Intramedullary spinal cord metastasis from renal cell carcinoma: Detection by positron emission tomography. Clin. Nucl. Med. 2001, 26, 837–839. [Google Scholar] [CrossRef]
- Kaya, R.A.; Dalkiliç, T.; Ozer, F.; Aydin, Y. Intramedullary spinal cord metastasis: A rare and devastating complication of cancer—Two case reports. Neurol. Med. Chir 2003, 43, 612–615. [Google Scholar] [CrossRef] [Green Version]
- Altinoz, M.A.; Santaguida, C.; Guiot, M.C.; Del Maestro, R.F. Spinal hemangioblastoma containing metastatic renal cell carcinoma in von Hippel-Lindau disease. Case report and review of the literature. J. Neurosurg. Spine 2005, 3, 495–500. [Google Scholar] [CrossRef]
- Gómez de la Riva, A.; Isla, A.; Pérez-López, C.; Budke, M.; Gutiérrez, M.; Frutos, R. Intramedullary spinal cord metastasis as the first manifestation of a renal carcinoma. Neurocirugia 2005, 16, 359–364. [Google Scholar] [CrossRef] [Green Version]
- Donovan, D.J.; Freeman, J.H. Solitary intramedullary spinal cord tumor presenting as the initial manifestation of metastatic renal cell carcinoma: Case report. Spine 2006, 31, E460–E463. [Google Scholar] [CrossRef] [PubMed]
- Asadi, M.; Rokni-Yazdi, H.; Salehinia, F.; Allameh, F.S. Metastatic renal cell carcinoma initially presented with an intramedullary spinal cord lesion: A case report. Cases J. 2009, 2, 7805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parikh, S.; Heron, D.E. Fractionated radiosurgical management of intramedullary spinal cord metastasis: A case report and review of the literature. Clin. Neurol. Neurosurg. 2009, 111, 858–861. [Google Scholar] [CrossRef]
- Petrelli, F.; Cabiddu, M.; Carpo, M.; Ghilardi, M.; Barni, S. Progression of intramedullary metastasis during perioperative cessation of sunitinib. Nat. Rev. Urol. 2010, 7, 634–637. [Google Scholar] [CrossRef]
- Komura, S.; Myamoto, K.; Hosoe, H.; Iwata, A. Intramedullary spinal cord metastasis from renal cell carcinoma mimicking intramedullary hemangioblastoma. Eur. J. Orthop. Surg. Traumatol. 2011, 22, 597–599. [Google Scholar] [CrossRef]
- Zakaria, Z.; Fenton, E.; Jansen, M.; O’Brien, D. The occult nature of intramedullary spinal cord metastases from renal cell carcinoma. BMJ Case Rep. 2012, 2012, bcr2012007476. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Chung, S.W.; Kim, K.T.; Cho, D.C.; Hwang, J.H.; Sung, J.K.; Lee, D. Intramedullary spinal cord metastasis in renal cell carcinoma: A case report of the surgical experience. J. Korean Med. Sci. 2013, 28, 1253–1256. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Li, Y.; Yang, Z.; Wang, R. Intramedullary spinal cord metastasis of renal cell carcinoma 6 years following the nephrectomy. Turk. Neurosurg. 2014, 24, 294–296. [Google Scholar] [CrossRef]
- Nomoto, Y.; Tsukie, T.; Kurita, A.; Seki, K.; Suzuki, H.; Yamazaki, K. Metastatic renal cell carcinoma initially presented with a longitudinally extensive spinal cord lesion on MRI. Rinsho Shinkeigaku 2016, 56, 348–351. [Google Scholar] [CrossRef]
- Soga, H.; Imanishi, O. Case of intramedullary spinal cord metastasis of renal cell carcinoma. World J. Clin. Urol. 2016, 5, 72–74. [Google Scholar] [CrossRef]
- Islam, R. Renal Cell Carcinoma presented with An Intramedullary Spinal Cord Metastasis: A Case Report. Bangladesh Crit. Care J. 2016, 4, 51–53. [Google Scholar] [CrossRef] [Green Version]
- Weng, Y.; Zhan, R.; Shen, J.; Pan, J.; Jiang, H.; Huang, K.; Xu, K.; Huang, H. Intramedullary Spinal Cord Metastasis from Renal Cell Carcinoma: A Systematic Review of the Literature. Biomed. Res. Int 2018, 2018, 7485020. [Google Scholar] [CrossRef]
- Malik, M.T.; Kazmi, S.J.; Turner, S. Teaching NeuroImages: Intradural, intramedullary spinal cord metastasis from primary renal cell carcinoma. Neurology 2018, 90, e911–e912. [Google Scholar] [CrossRef] [Green Version]
- Strickland, B.A.; McCutcheon, I.E.; Chakrabarti, I.; Rhines, L.D.; Weinberg, J.S. The surgical treatment of metastatic spine tumors within the intramedullary compartment. J. Neurosurg. Spine 2018, 28, 79–87. [Google Scholar] [CrossRef]
- Barrie, U.; Elguindy, M.; Pernik, M.; Adeyemo, E.; Aoun, S.G.; Hall, K.; Reyes, V.P.; El Ahmadieh, T.Y.; Bagley, C.A. Intramedullary Spinal Metastatic Renal Cell Carcinoma: Systematic Review of Disease Presentation, Treatment, and Prognosis with Case Illustration. World Neurosurg. 2020, 134, 584–593. [Google Scholar] [CrossRef]
- Ponzo, G.; Umana, G.E.; Giuffrida, M.; Furnari, M.; Nicoletti, G.F.; Scalia, G. Intramedullary craniovertebral junction metastasis leading to the diagnosis of underlying renal cell carcinoma. Surg. Neurol. Int. 2020, 11, 152. [Google Scholar] [CrossRef]
- Kalimuthu, L.M.; Ora, M.; Gambhir, S. Recurrent Renal Carcinoma with Solitary Intramedullary Spinal Cord Metastasis. Indian J. Nucl. Med. 2020, 35, 358–359. [Google Scholar] [CrossRef]
- Mosdal, C.; Bang, F. Intradural spinal metastases. Acta Neurochir. 1981, 56, 107–110. [Google Scholar] [CrossRef]
- Westphal, M.; Mende, K.C.; Eicker, S.O. Refining the treatment of spinal cord lesions: Experience from 500 cases. Neurosurg. Focus 2021, 50, E22. [Google Scholar] [CrossRef]
- Cofano, F.; Giambra, C.; Costa, P.; Zeppa, P.; Bianconi, A.; Mammi, M.; Monticelli, M.; Di Perna, G.; Junemann, C.V.; Melcarne, A.; et al. Management of Extramedullary Intradural Spinal Tumors: The Impact of Clinical Status, Intraoperative Neurophysiological Monitoring and Surgical Approach on Outcomes in a 12-Year Double-Center Experience. Front. Neurol. 2020, 11, 598619. [Google Scholar] [CrossRef] [PubMed]
- Ahn, A.; Phan, K.; Cheung, Z.B.; White, S.J.W.; Kim, J.S.; Cho, S.K. Predictors of Discharge Disposition Following Laminectomy for Intradural Extramedullary Spinal Tumors. World Neurosurg. 2019, 123, e427–e432. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Msaouel, P.; Hara, K.; Choi, H.; Le, V.; Shah, A.Y.; Wang, J.; Jonasch, E.; Choi, S.; Nguyen, Q.N.; et al. Definitive radiotherapy in lieu of systemic therapy for oligometastatic renal cell carcinoma: A single-arm, single-centre, feasibility, phase 2 trial. Lancet Oncol. 2021, 22, 1732–1739. [Google Scholar] [CrossRef]
- Kjaer, M.; Frederiksen, P.L.; Engelholm, S.A. Postoperative radiotherapy in stage II and III renal adenocarcinoma. A randomized trial by the Copenhagen Renal Cancer Study Group. Int J. Radiat. Oncol. Biol. Phys. 1987, 13, 665–672. [Google Scholar] [CrossRef]
- Deschavanne, P.J.; Fertil, B. A review of human cell radiosensitivity in vitro. Int. J. Radiat. Oncol. Biol. Phys. 1996, 34, 251–266. [Google Scholar] [CrossRef]
- Dabestani, S.; Marconi, L.; Hofmann, F.; Stewart, F.; Lam, T.B.; Canfield, S.E.; Staehler, M.; Powles, T.; Ljungberg, B.; Bex, A. Local treatments for metastases of renal cell carcinoma: A systematic review. Lancet Oncol. 2014, 15, e549–e561. [Google Scholar] [CrossRef]
- Alt, A.L.; Boorjian, S.A.; Lohse, C.M.; Costello, B.A.; Leibovich, B.C.; Blute, M.L. Survival after complete surgical resection of multiple metastases from renal cell carcinoma. Cancer 2011, 117, 2873–2882. [Google Scholar] [CrossRef]
- Kwak, C.; Park, Y.H.; Jeong, C.W.; Lee, S.E.; Ku, J.H. Metastasectomy without systemic therapy in metastatic renal cell carcinoma: Comparison with conservative treatment. Urol. Int. 2007, 79, 145–151. [Google Scholar] [CrossRef]
- Ouzaid, I.; Capitanio, U.; Staehler, M.; Wood, C.G.; Leibovich, B.C.; Ljungberg, B.; Van Poppel, H.; Bensalah, K.; Young Academic Urologists Kidney Cancer Working Group of the European Association of Urology. Surgical Metastasectomy in Renal Cell Carcinoma: A Systematic Review. Eur. Urol. Oncol. 2019, 2, 141–149. [Google Scholar] [CrossRef]
- Khoo, V.S.; Pyle, L. Radiotherapy and Supportive Care; Eisen, T., Christmas, T., Eds.; Clinical Progress in Renal Cancer; Informa UK Ltd.: Oxford, UK, 2007. [Google Scholar]
- Maor, M.H.; Frias, A.E.; Oswald, M.J. Palliative radiotherapy for brain metastases in renal carcinoma. Cancer 1988, 62, 1912–1917. [Google Scholar] [CrossRef]
- Ljungberg, B.; Bensalah, K.; Canfield, S.; Dabestani, S.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; Lam, T.; Marconi, L.; Merseburger, A.S.; et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur. Urol. 2015, 67, 913–924. [Google Scholar] [CrossRef]
- Samartzis, D.; Gillis, C.C.; Shih, P.; O’Toole, J.E.; Fessler, R.G. Intramedullary Spinal Cord Tumors: Part I-Epidemiology, Pathophysiology, and Diagnosis. Global Spine J. 2015, 5, 425–435. [Google Scholar] [CrossRef]
- Payer, S.; Mende, K.C.; Westphal, M.; Eicker, S.O. Intramedullary spinal cord metastases: An increasingly common diagnosis. Neurosurg. Focus 2015, 39, E15. [Google Scholar] [CrossRef] [Green Version]
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef]


{kind=link}
| N of Cases | Author, Year | Sex, Age (Yrs) | Latency to Spinal Metastasis (Months) | Spinal Level | Symptoms | Systemic Metastases | Management of Spinal Metastases | Clinical Outcome | Survival (Months) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Takahashi et al. [7]. 1990 | M, 51 | Simultaneous | L4 | LBP, sciatica | n.s. | S, CHT, RT | Decreased L4 sensitivity | Dead at 1 |
| 2 | Maxwell et al. [8]. 1999 | M, 84 | 60 | L2-L3 | LBP, sciatica | Lung | S (snr) | Improved | n.s. |
| 3 | Mak et al. [9]. 2001 | M, 59 | 48 | L3-L4 | Weakness, urinary incontinence | Bone | S (pnr) | Improved | Alive at 20 |
| 4 | Kubota et al. [10]. 2003 | M, 68 | 84 | L3 | LBP | Lung | S (snr) | Improved | Alive at 24 |
| 5 | Takada et al. [11]. 2003 | M, 61 | 60 | L3 | LBP, sciatica, weakness, urinary incontinence | Lung | S (snr), IFN | Motor worsening | Alive at 12 |
| 6 | Gaetani et al. [12]. 2004 | F, 36 | 4 | L3-L4 | LBP, sciatica, weakness, urinary incontinence | lepto-meningeal | S, RT | Improved | Dead at 12 |
| 7 | Alfieri et al. [13]. 2005 | F, 67 | 24 | L3-L5 | LBP, weakness, urinary symptoms | No | S | Improved | n.s. |
| 8 | Jost et al. [14]. 2009 | M, 82 | 6 | C6-C7 | Left hemiparesis | Brain | S (pnr), RT | Improved | Alive at 12 |
| 9 | Kim et al. [15]. 2009 | M, 41 | 12 | L2 | LBP, bilateral leg pain | Lung | S (snr), CHT | Improved | Alive at 12 |
| 10 | Lin et al. [16]. 2011 | M, 68 | 72 | T12-L1 | LBP, bilateral leg weakness and sciatica | No | S (pnr), RT, IFN | Improved | Alive at 36 |
| 11 | Dobson et al. [17]. 2013 | F, 81 | Simultaneous | L2 | LBP, bilateral sciatica, urinary incontinence | No | S (snr), RT | Improved | Alive at 36 |
| 12 | Ji et al. [18]. 2013 | M, 68 | 192 | T12-L1 | LBP, bilateral sciatica | Tibia | S (snr), RT | Improved | Alive at 24 |
| 13 | Strong et al. [19]. 2013 | F, 49 | 96 | L4 | Left leg weakness and hypoesthesia | No | S (pnr), RT | Improved | Alive at 24 |
| 14 | M, 72 | Simultaneous | L2 | asymptomatic | No | S (pnr), RT | Improved | Alive at 24 | |
| 15 | Srinivasan et al. [20]. 2014 | M, 40 | Simultaneous | L4-S1 | Sensory-motor deficits of both legs, urinary incontinence | No | S (pnr) | Improved | Dead during CHT |
| 16 | Capek et al. [23]. 2016 | F, 61 | 192 | T12 | LBP | No | S (snr), RT | Stable | Alive 108 |
| 17 | Ali et al. [22]. 2021 | F, 55 | 96 | L3-L4 | LBP | No | S (snr), CHT | Stable | n.s. |
| 18 | Madhavan et al. [24]. 2021 | M, 68 | Simultaneous | T11 | acute lower extremities weakness, urinary retention, severe back pain | Lung, lymph-node, bone | CHT (refused S) | Improved | n.s. |
| 19 | Mariniello et al. [6]. 2022 | M, 64 | 168 | L1-L2, L4-L5 | Sudden LBP and left sciatica | Lung | S (pnr), CHT, RT | Improved | Alive at 12 |
| Covariates | Ovearll Series IDEM Metastases | Ovearll Series ISC Metastases | Statistical Analysis p Value |
|---|---|---|---|
| Age (years) | Mean 61.84 ± 16.27 SD (range 36–84 yrs) | Mean 55.96 ± 10.89 SD (range 37–78 yrs) | |
| Sex | |||
| - Male | 13 (68%) | 25 (78%) | |
| - Female | 6 (32%) | 7 (22%) | |
| Interval between diagnoses of RCC and IDEM (months) | Mean 61.88 ± 65.65 SD (range 0–192 months) | Mean 28.76 ± 45.31 SD (range 0–180 months) | |
| - Metachronous | 14/19 (74%) | 23 (72%) | p = 0.889 |
| - Synchronous | 5/19 (26%) | 9 (28%) | |
| Spinal level of metastasis - Cervical - Thoracic - Lumbar - Thoraco-lumbar | 1/19 (5%) 2/19 (10%) 14/19 (75%) 2/19 (10%) | 14/32 (44%) 13/32 (41%) 3/32 (9%) 2/32 (6%) | p = 0.0035 p = 0.02 p < 0.00001 p = 0.58 |
| Presenting symptoms - Spinal pain - Radicular symptoms - Leg weakness - Urinary disfunction - Asymptomatic - Motility disturbance - Brown-Sequard syndrome | 13/19 (68%) 9/19 (47%) 7/19 (37%) 7/19 (37%) 1/19 (5%) --- --- | 8/32 (25%) --- 12/32 (37,5%) 6/32 (19%) --- 2/32 (6%) 2/32 (6%) | p = 0.002 p = 0.96 p = 0.15 |
| Systemic metastases - Lung - Brain - Bone - Leptomeninges - Lymph-nodes - Adrenal gland - Liver - IDEM alone - IM alone | 18 * 6/19 (32%) 1/19 (5%) 3/19 (16%) 1/19 (5%) 1/19 (5%) --- --- 8/19 (42%) --- | 30 * 15/30 (50%) 12/30 (40%) 6/30 (20%) --- 5/30 (17%) 3/30 (10%) 2/30 (7%) --- 5/30 (17%) | p = 0.2 p = 0.008 p = 1 p = 0.3 Single vs. Multiple p = 0.036 |
| Management - Surgery - Adjuvant radiotherapy - Adjuvant chemotherapy - Adjuvant IFN therapy - Adjuvant radio- and chemotherapy - Chemotherapy alone - Radiotherapy alone - Pharmacological alone | 18/19 (95%) 8/19 (42%) 2/19 (10%) 2/19 (10%) 2/19 (10%) 1/19 (5%) --- | 11/32 (35%) 10/32 (31%) 9/32 (28%) 2/32 (6%) | p < 0.0001 p = 0.68 |
| Clinical outcome - Improved - Stable - Worsened | 15/19 (80%) 2/19 (10%) 2/19 (10%) | 27 * 16/27 (59%) 9/27 (34%) 2/27 (7%) | p = 0.16 p = 0.09 p = 0.71 |
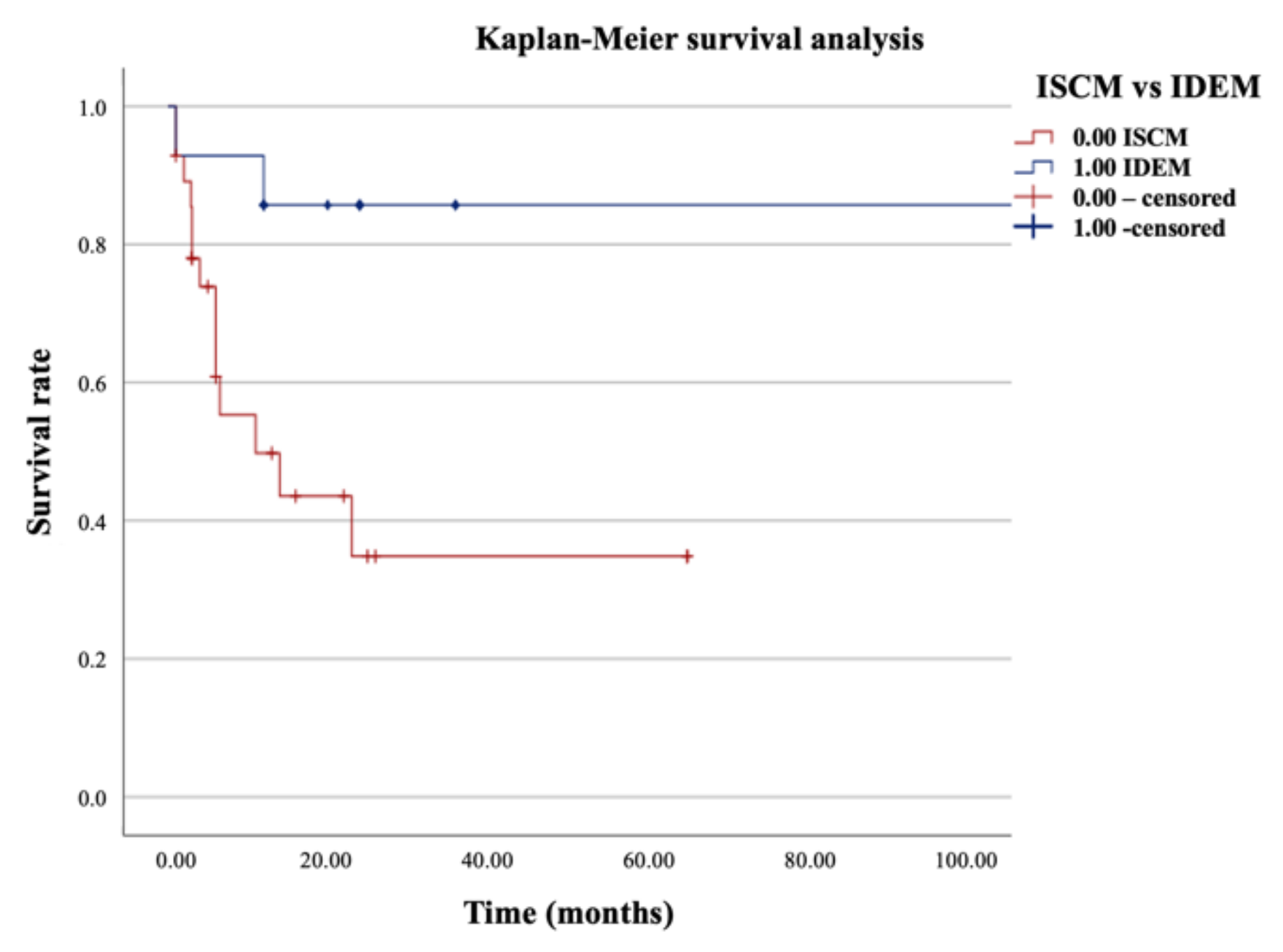
| Survival (months) - Alive at last follow-up - Dead at last follow-up | 15 * Mean 25.5 ± 25.6 SD (range 1–108 months) 12/15 (80%) 3/15 (20%) | 28 * Mean 13.15 ± 17.09 SD (range 1–65 months) 14/28 (50%) 14/28 (50%) | p = 0.011 |
| n of Cases | Author, Year | Sex, Age (yrs) | Latency to Spinal Metastasis (Months) | Spinal Level | Symptoms | Systemic Metastases | Management of Spinal Metastases | Clinical Outcome | Survival (Months) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Ateaque et al. [25]. 2000 | M, 63 | 132 | C2-C3 | Ataxia, tetraparesis | No | S | Stable | Dead at 1 |
| 2 | Schijns et al. [26]. 2000 | F, 70 | Simultaneous | C7 | Cervical-brachialgia, paraparesis | Liver | S | Improved | Alive at 13 |
| 3 | Fakih et al. [27]. 2001 | M, 56 | 0 | C4 | Lower extremities weakness, urinary incontinence | Brain, lung | Med, RT | Improved | Dead at 6 |
| 4 | M, 60 | 180 | T1-T2 | Lower extremity weakness | Brain, lung | S, RT | Improved | Alive at 5 | |
| 5 | F, 68 | 2 | T8-L2 | Lower extremities weakness | No | Med, RT | Improved | Dead at 11 | |
| 6 | F, 57 | Simultaneous | C7 | Brown-Sequard syndrome | Brain, lung | Med, RT | Improved | Dead at 6 | |
| 7 | M, 46 | 2 | T5 | Leg weakness, urinary disfunction | Brain, lung, lymph-nodes | RT, Med | Stable | Dead at 4 | |
| 8 | F, 37 | 25 | C2 | Bilateral cervical-brachialgia | Lung | S | Improved | Dead at 23 | |
| 9 | Poggi et al. [28]. 2001 | M, 37 | 2 | T12 | Dysesthesia right leg | Brain, bone, lymph-nodes | RT, Med | n.s. | n.s |
| 10 | Kaya et al. [29]. 2003 | M, 43 | 12 | L1 | LBP, urinary incontinence, lower extremities weakness | n.s. | S | Improved | Dead at 6 |
| 11 | Altinoz et al. [30]. 2005 | M, 43 | 26 | T6-T7 | Back pain, leg weakness | Brain, lung, adrenal gland | S | Stable | Alive at 25 |
| 12 | Gomez de la Riva et al. [31]. 2005 | M, 69 | Simultaneous | L1 | Lower extremities weakness | Lung | S | Improved | Alive at 16 |
| 13 | Donovan et al. [32]. 2006 | F, 41 | Simultaneous | C4 | Brown-Sequard syndrome | Lung, bone | S, RT | Worsened | Dead at 2 |
| 14 | Asadi et al. [33]. 2009 | F, 51 | Simultaneous | T12 | Back pain, paraparesis | Brain, bone | palliative | n.s. | n.s |
| 15 | Parikh et al. [34]. 2009 | M, 50 | 4 | C5 | Upper extremities paresthesiae | Brain, lymph-nodes | RT, SRS | Stable | Alive at 26 |
| 16 | Petrelli et al. [35]. 2010 | F, 57 | Simultaneous | T12-L1 | Paraparesis, paresthesia, hypoesthesia | Lung, bone, lymph-nodes | CHT, RT | Improved | Alive at 6 |
| 17 | Komura et al. [36]. 2011 | M, 57 | 60 | C4 | Bilateral shoulder pain, upper and lower extremities weakness | No | S | Improved | Alive at 22 |
| 18 | Zakaria et al. [37]. 2012 | M, 62 | 2 | C7 | Back pain, urinary incontinence, lower limb weakness | Lung, lymph-nodes | RT, S, Med | Improved | Dead at 3 |
| 19 | Park et al. [38]. 2013 | M, 44 | 6 | T12 | Paraparesis | Lung | RT, S | Improved | Alive at 6 |
| 20 | Gao et al. [39]. 2014 | M, 51 | 72 | T4-T5 | Lower extremities weakness, urinary incontinence | No | S | Improved | Alive at 3 |
| 21 | Nomoto et al. [40]. 2016 | M 48 | 5 | T8-T9 | Paraplegia | Lung | RT, S | n.s. | Alive at 3 |
| 22 | Soga et al. [41]. 2016 | M 69 | 3 | T12 | Paraplegia, urinary retention | Lung | Refused S, Med | Worsened | Dead at 3 |
| 23 | Islam et al. [42]. 2016 | M 62 | Simultaneous | T12 | Spastic paraparesis | Bone | Refused S, RT | Improved | Alive at 1 |
| 24 | Weng et al. [43]. 2018 | M 58 | 34 | T12 | Lower extremities numbness, paraparesis | Lung | S, RT | Improved | Alive at 6 |
| 25 | Malik et al. [44]. 2018 | M 75 | Simultaneous | T11-T12 | Lower extremity weakness | n.s. | S, RT | n.s. | n.s. |
| 26 | Strickland et al. [45]. 2018 | M 50 | 64 | C1 | n.s. | Brain | S | Stable | Dead at 6.5 |
| 27 | M 50 | 92 | C5 | n.s. | Brain | S, RT | Stable | Dead at 2.9 | |
| 28 | M 66 | 97 | T11 | n.s. | Bone | S, RT | Stable | Alive at 65 | |
| 29 | M 59 | 32 | C3 | n.s. | Brain | S | Stable | Alive at 65 | |
| 30 | Barrie et al. [46]. 2019 | M 56 | 5 | C2-C3 | Left facial weakness, diplopia, left upper and lower extremity weakness | Brain, adrenal gland, lung, liver, mediastinum | RT, CHT, Med, S | Stable | Dead at 1 |
| 31 | Ponzo et al. [47]. 2020 | M, 78 | Simultaneous | C1-C2 | Cervicalgia, hemiplegia | Muscle, adrenal gland | S | Improved | Dead at 14 |
| 32 | Kalimuthu et al. [48]. 2020 | M, 65 | 6 | L1-L2 | LBP | No | RT | n.s. | n.s. |
| Treatment | Clinical Outcome | Overall Survival | |||||
|---|---|---|---|---|---|---|---|
| Stable | Improved | Worsened | n.s. | Alive (Months) | Dead | n.s. | |
| Surgery alone (5/19) | 0 | 5 | 0 | 0 | 2 (20–24 mo.) (Mean 22 ± 2.8 SD mo.) | 1 (Mean 22 ± 2.8 SD mo.) | 2 |
| Adjuvant radiotherapy (8/19) | 1 | 7 | 0 | 0 | 7 (12–108 mo.) (Mean 32 ± 37.7 SD mo.) | 1 (12 mo.) | 0 |
| Adjuvant chemotherapy (2/19) | 1 | 1 | 0 | 0 | 1 (12 mo.) | 0 | 1 |
| Adjuvant IFN therapy (2/19) | 0 | 1 | 1 | 0 | 2 (12–36 mo.) (Mean 24 ± 16.9 SD mo.) | 0 | 0 |
| Adjuvant radio and chemotherapy (2/19) | 0 | 1 | 1 | 0 | 1 (12 mo.) | 1 (1 mo.) | 0 |
| Chemotherapy alone (1/19) | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| Treatment | Clinical Outcome | Overall Survival | |||||
|---|---|---|---|---|---|---|---|
| Stable | Improved | Worsened | n.s. | Alive | Dead | n.s. | |
| Surgery alone (11/32) | 4 | 7 | 0 | 0 | 6 (3–65 mo.) (Mean 24 ± 21.5 SD mo.) | 5 (1–23 mo.) (Mean 11 ± 9.6 SD mo.) | 0 |
| Radiotherapy alone (9/32) | 2 | 5 | 0 | 2 | 3 (1–26 mo.) (Mean 11 ± 13.22 SD mo.) | 4 (4–11 mo.) (Mean 6.75 ± 2.98 SD mo.) | 2 |
| Surgery + Radiotherapy (10/32) | 3 | 4 | 1 | 2 | 5 (3–65 mo.) (Mean 17 ± 26.8 SD mo.) | 4 (1–3 mo.) (Mean 2 ± 1 SD mo.) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corvino, S.; Mariniello, G.; Solari, D.; Berardinelli, J.; Maiuri, F. The Role of Surgery in Spinal Intradural Metastases from Renal Cell Carcinoma: A Literature Review. Cancers 2022, 14, 1595. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061595
Corvino S, Mariniello G, Solari D, Berardinelli J, Maiuri F. The Role of Surgery in Spinal Intradural Metastases from Renal Cell Carcinoma: A Literature Review. Cancers. 2022; 14(6):1595. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061595
Chicago/Turabian StyleCorvino, Sergio, Giuseppe Mariniello, Domenico Solari, Jacopo Berardinelli, and Francesco Maiuri. 2022. "The Role of Surgery in Spinal Intradural Metastases from Renal Cell Carcinoma: A Literature Review" Cancers 14, no. 6: 1595. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061595