
Hypoalbuminemia Is a Hepatocellular Carcinoma Independent Risk Factor for Tumor Progression in Low-Risk Bridge to Transplant Candidates

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Primary Outcome
2.3. Study Variables
2.4. Liver-Directed Therapy Sites and Treatment Protocols
2.5. Statistical Methods
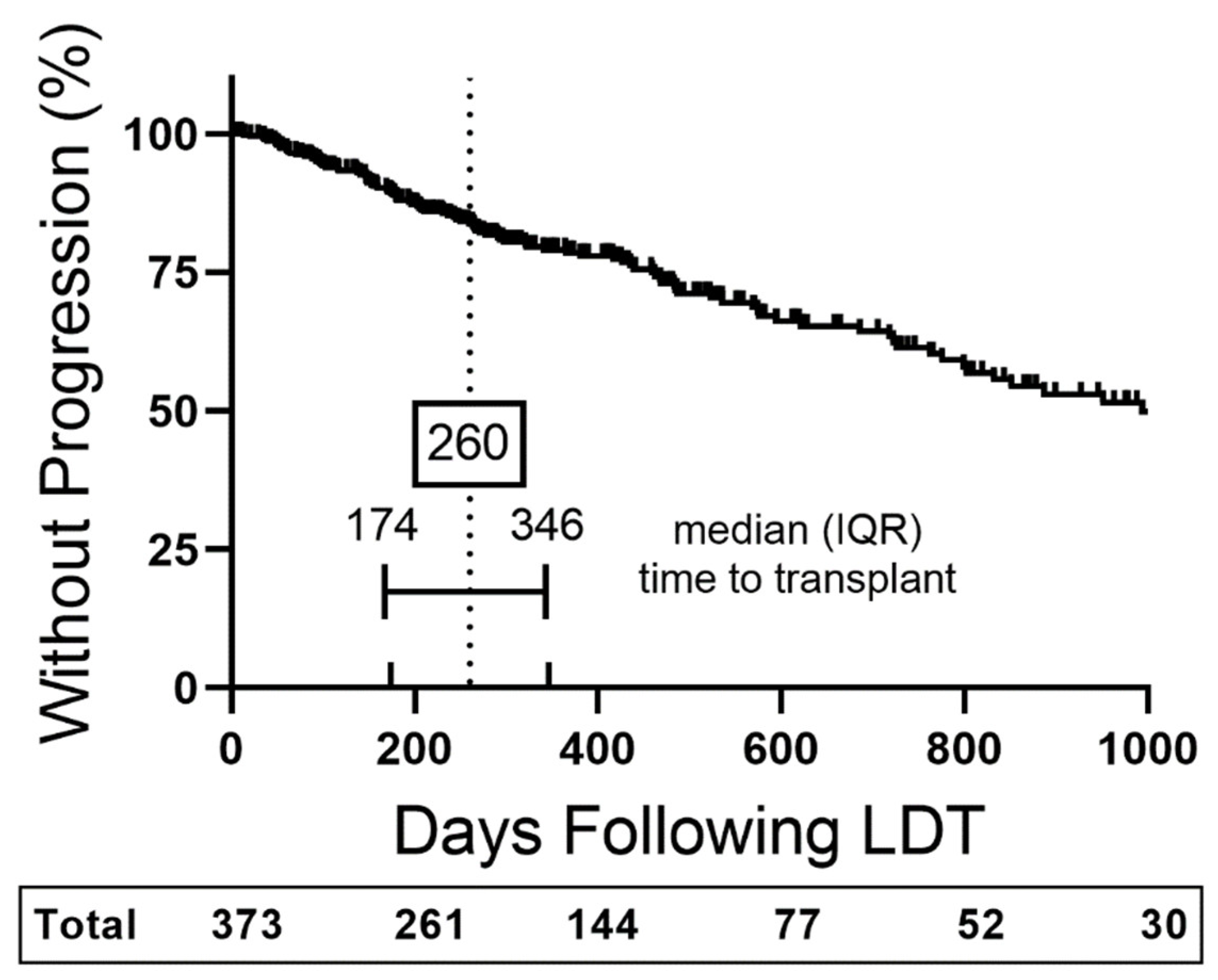
3. Results
3.1. Cohort Demographics
3.2. Liver-Directed Therapy Baseline Factors Associated with Time to Progression
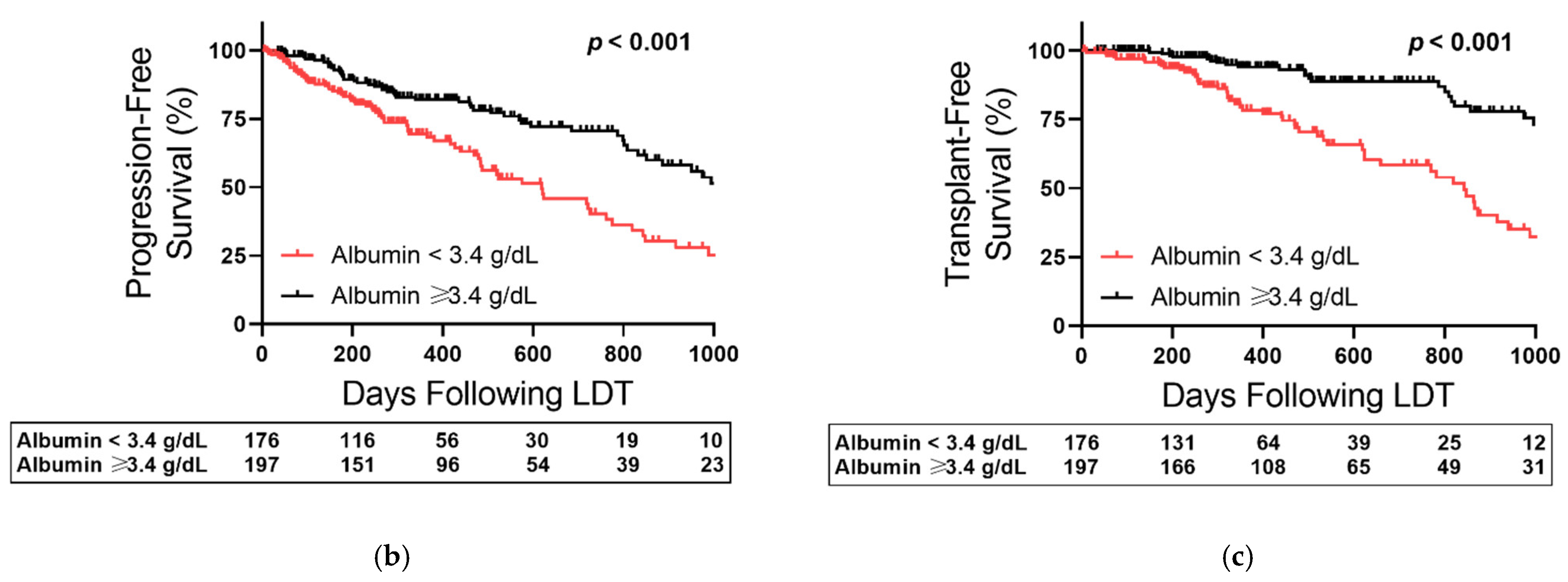
3.3. Albumin-Based Stratification of Early-Stage HCC Outcomes
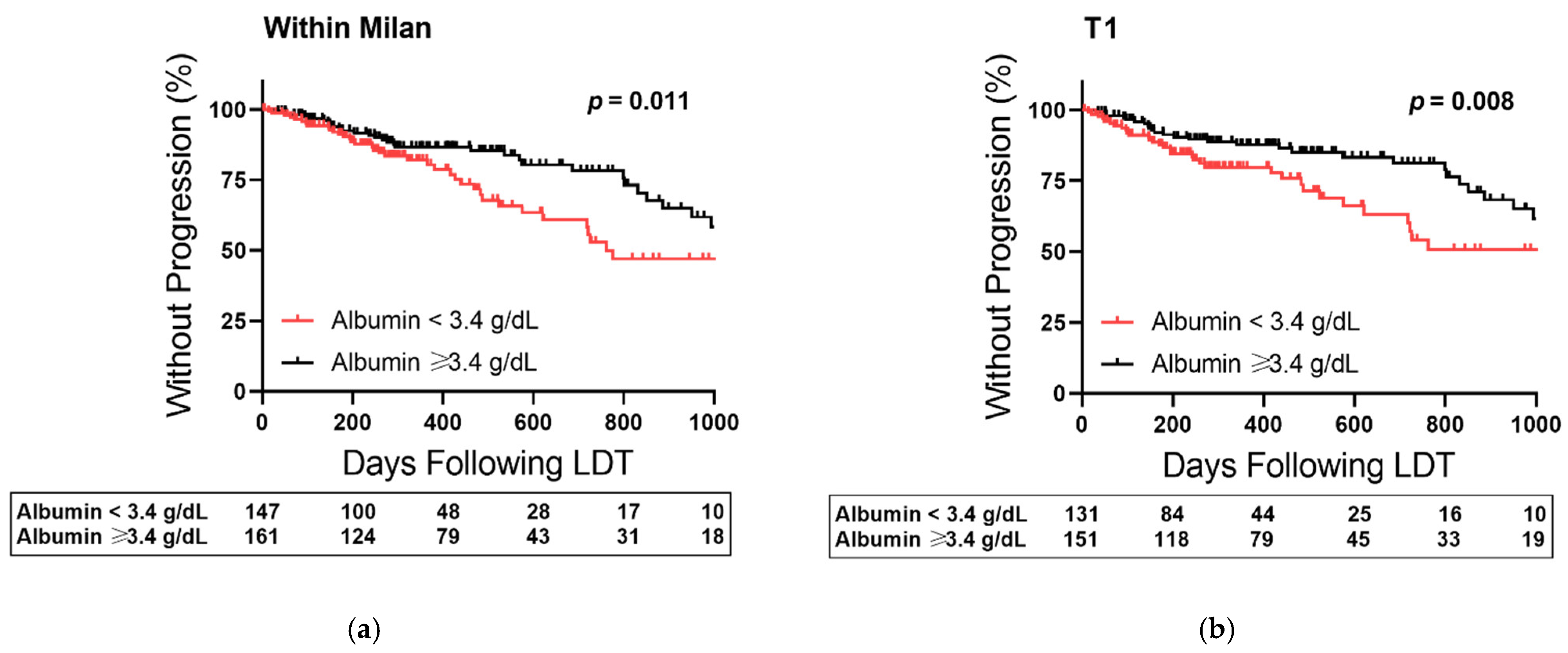
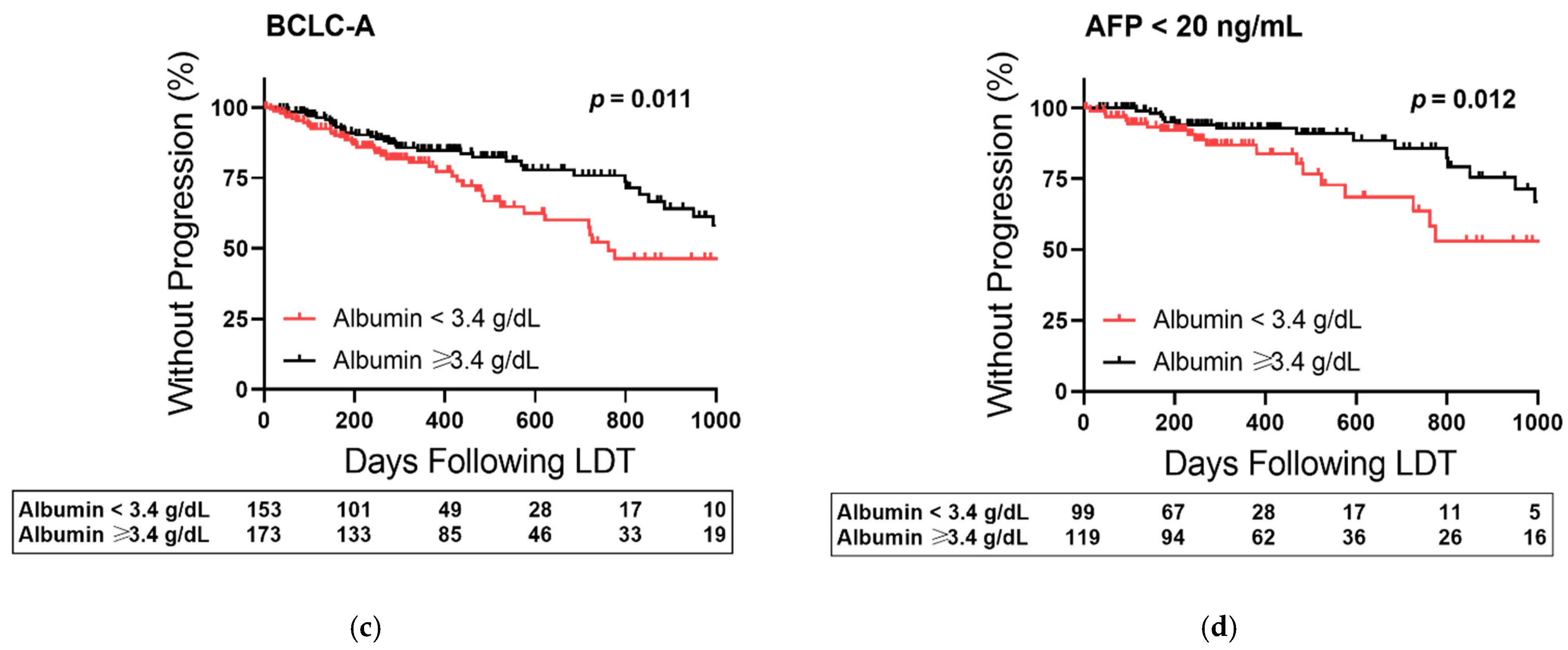
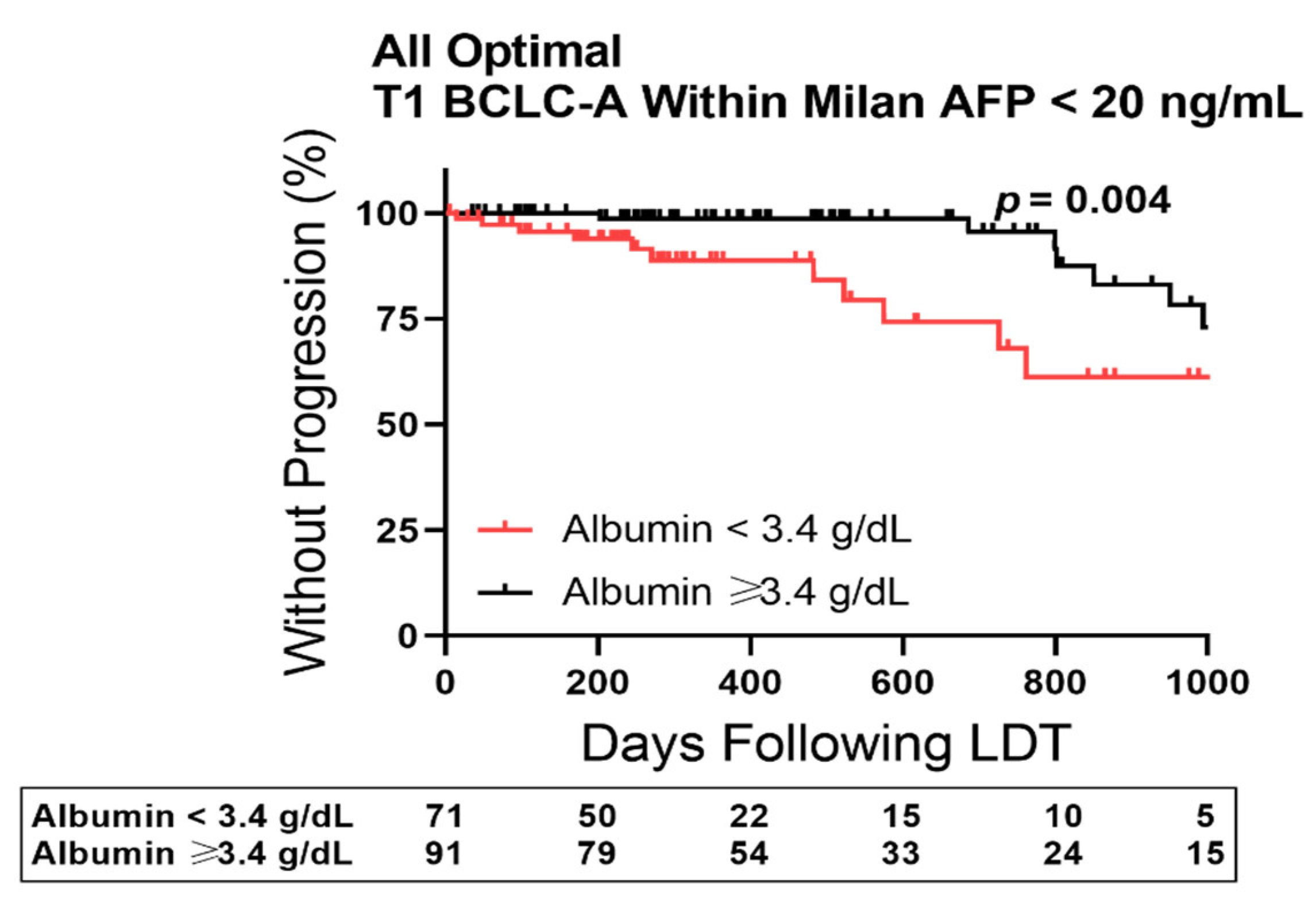
3.4. Albumin-Based Stratification of Outcomes in Low-Risk Early-Stage HCC
3.5. Role of First Cycle Treatment Modality in Albumin-Based Stratification
3.6. Difference in Baseline Factors Prior to First Cycle LDT after Albumin Stratification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bertuccio, P.; Turati, F.; Carioli, G.; Rodriguez, T.; La Vecchia, C.; Malvezzi, M.; Negri, E. Global trends and predictions in hepatocellular carcinoma mortality. J. Hepatol. 2017, 67, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, F.Y.; Bass, N.M.; Nikolai, B.; Merriman, R.; Davern, T.J.; Kerlan, R.; Ascher, N.L.; Roberts, J.P. A follow-up analysis of the pattern and predictors of dropout from the waiting list for liver transplantation in patients with hepatocellular carcinoma: Implications for the current organ allocation policy. Liver Transpl. 2003, 9, 684–692. [Google Scholar] [CrossRef]
- Kanwal, F.; Singal, A.G. Surveillance for Hepatocellular Carcinoma: Current Best Practice and Future Direction. Gastroenterology 2019, 157, 54–64. [Google Scholar] [CrossRef] [Green Version]
- Meller, R.; Galvan, L.; Lan, J.Q.; Han, E.; Bauer, J.; Morris, K.T. Programmed cell death in a patient with hepatocellular carcinoma treated with yttrium-90 and doxorubicin-loaded beads. J. Vasc. Interv. Radiol. 2013, 24, 1537–1542e2. [Google Scholar] [CrossRef]
- Lee, D.D.; Samoylova, M.; Mehta, N.; Musto, K.R.; Roberts, J.P.; Yao, F.Y.; Harnois, D.M. The mRECIST Classification Provides Insight into Tumor Biology for Patients with Hepatocellular Carcinoma Awaiting Liver Transplantation. Liver Transpl. 2019, 25, 228–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.; Chu, H.H.; Kim, J.H.; Kim, S.Y.; Alrashidi, I.; Gwon, D.I.; Yoon, H.K.; Kim, N. Clinical Significance of the Initial and Best Responses after Chemoembolization in the Treatment of Intermediate-Stage Hepatocellular Carcinoma with Preserved Liver Function. J. Vasc. Interv. Radiol. 2020, 31, 1998–2006.E1. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Lario, M.; Alvarez-Mon, M. Cirrhosis-associated immune dysfunction: Distinctive features and clinical relevance. J. Hepatol. 2014, 61, 1385–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soeters, P.B.; Wolfe, R.R.; Shenkin, A. Hypoalbuminemia: Pathogenesis and Clinical Significance. JPEN J. Parenter. Enteral. Nutr. 2019, 43, 181–193. [Google Scholar] [CrossRef] [Green Version]
- Bernardi, M.; Angeli, P.; Claria, J.; Moreau, R.; Gines, P.; Jalan, R.; Caraceni, P.; Fernandez, J.; Gerbes, A.L.; O’Brien, A.J.; et al. Albumin in decompensated cirrhosis: New concepts and perspectives. Gut 2020, 69, 1127–1138. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, A.J.; Fullerton, J.N.; Massey, K.A.; Auld, G.; Sewell, G.; James, S.; Newson, J.; Karra, E.; Winstanley, A.; Alazawi, W.; et al. Immunosuppression in acutely decompensated cirrhosis is mediated by prostaglandin E2. Nat. Med. 2014, 20, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Padia, S.A.; Lewandowski, R.J.; Johnson, G.E.; Sze, D.Y.; Ward, T.J.; Gaba, R.C.; Baerlocher, M.O.; Gates, V.L.; Riaz, A.; Brown, D.B.; et al. Radioembolization of Hepatic Malignancies: Background, Quality Improvement Guidelines, and Future Directions. J. Vasc. Interv. Radiol. 2017, 28, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver. Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semmler, G.; Meyer, E.L.; Kozbial, K.; Schwabl, P.; Hametner-Schreil, S.; Zanetto, A.; Bauer, D.; Chromy, D.; Simbrunner, B.; Scheiner, B.; et al. HCC risk stratification after cure of hepatitis C in patients with compensated advanced chronic liver disease. J. Hepatol. 2021, 76, 812–821. [Google Scholar] [CrossRef]
- Demirtas, C.O.; D’Alessio, A.; Rimassa, L.; Sharma, R.; Pinato, D.J. ALBI grade: Evidence for an improved model for liver functional estimation in patients with hepatocellular carcinoma. JHEP Rep. 2021, 3, 100347. [Google Scholar] [CrossRef] [PubMed]
- Feng, D.; Wang, M.; Hu, J.; Li, S.; Zhao, S.; Li, H.; Liu, L. Prognostic value of the albumin-bilirubin grade in patients with hepatocellular carcinoma and other liver diseases. Ann. Transl. Med. 2020, 8, 553. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Kudo, M. Newly Proposed ALBI Grade and ALBI-T Score as Tools for Assessment of Hepatic Function and Prognosis in Hepatocellular Carcinoma Patients. Liver Cancer 2019, 8, 312–325. [Google Scholar] [CrossRef]
- Yilma, M.; Saxena, V.; Mehta, N. Models to Predict Development or Recurence of Hepatocellular Carcinoma (HCC) in Patients with Advanced Hepatic Fibrosis. Curr. Gastroenterol. Rep. 2022, 24, 1–9. [Google Scholar] [CrossRef]
- Alcaraz-Quiles, J.; Casulleras, M.; Oettl, K.; Titos, E.; Flores-Costa, R.; Duran-Guell, M.; Lopez-Vicario, C.; Pavesi, M.; Stauber, R.E.; Arroyo, V.; et al. Oxidized Albumin Triggers a Cytokine Storm in Leukocytes Through P38 Mitogen-Activated Protein Kinase: Role in Systemic Inflammation in Decompensated Cirrhosis. Hepatology 2018, 68, 1937–1952. [Google Scholar] [CrossRef] [PubMed]
- Fu, X.; Yang, Y.; Zhang, D. Molecular mechanism of albumin in suppressing invasion and metastasis of hepatocellular carcinoma. Liver Int. 2021, 42, 696–709. [Google Scholar] [CrossRef]
- Kim, W.R.; Mannalithara, A.; Heimbach, J.K.; Kamath, P.S.; Asrani, S.K.; Biggins, S.W.; Wood, N.L.; Gentry, S.E.; Kwong, A.J. MELD 3.0: The Model for End-Stage Liver Disease Updated for the Modern Era. Gastroenterology 2021, 161, 1887–1895.e4. [Google Scholar] [CrossRef] [PubMed]
- China, L.; Maini, A.; Skene, S.S.; Shabir, Z.; Sylvestre, Y.; Colas, R.A.; Ly, L.; Becares Salles, N.; Belloti, V.; Dalli, J.; et al. Albumin Counteracts Immune-Suppressive Effects of Lipid Mediators in Patients with Advanced Liver Disease. Clin. Gastroenterol. Hepatol. 2018, 16, 738–747.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maini, A.A.; Becares, N.; China, L.; Tittanegro, T.H.; Patel, A.; De Maeyer, R.P.H.; Zakeri, N.; Long, T.V.; Ly, L.; Gilroy, D.W.; et al. Monocyte dysfunction in decompensated cirrhosis is mediated by the prostaglandin E2-EP4 pathway. JHEP Rep. 2021, 3, 100332. [Google Scholar] [CrossRef] [PubMed]
- Fouad, M.; El Kassas, M.; Ahmed, E.; El Sheemy, R. Tumor characteristics of hepatocellular carcinoma after direct-acting antiviral treatment for hepatitis C: Comparative analysis with antiviral therapy-naive patients. World J. Hepatol. 2021, 13, 1743–1752. [Google Scholar] [CrossRef] [PubMed]
- Deterding, K.; Honer Zu Siederdissen, C.; Port, K.; Solbach, P.; Sollik, L.; Kirschner, J.; Mix, C.; Cornberg, J.; Worzala, D.; Mix, H.; et al. Improvement of liver function parameters in advanced HCV-associated liver cirrhosis by IFN-free antiviral therapies. Aliment. Pharmacol. Ther. 2015, 42, 889–901. [Google Scholar] [CrossRef]
- Kan, T.; Hashimoto, S.; Kawabe, N.; Nakano, T.; Nakaoka, K.; Yoshioka, K. Increase in Albumin by Daclatasvir/asunaprevir Therapy is Correlated with Decrease in Aspartate Transaminase. J. Transl. Int. Med. 2017, 5, 148–154. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Seki, T.; Wakabayashi, M.; Nakagawa, T.; Itho, T.; Shiro, T.; Kunieda, K.; Sato, M.; Uchiyama, S.; Inoue, K. Ultrasonically guided percutaneous microwave coagulation therapy for small hepatocellular carcinoma. Cancer 1994, 74, 817–825. [Google Scholar] [CrossRef]
- Kohla, M.A.; Abu Zeid, M.I.; Al-Warraky, M.; Taha, H.; Gish, R.G. Predictors of hepatic decompensation after TACE for hepatocellular carcinoma. BMJ Open Gastroenterol. 2015, 2, e000032. [Google Scholar] [CrossRef] [PubMed]
- Miksad, R.A.; Ogasawara, S.; Xia, F.; Fellous, M.; Piscaglia, F. Liver function changes after transarterial chemoembolization in US hepatocellular carcinoma patients: The LiverT study. BMC Cancer 2019, 19, 795. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Data | p-Value |
|---|---|---|
| Cohort, n | 373 | |
| Study period, date range | 21 April 2016–4 November 2021 | |
| General Demographics | ||
| Age, median (IQR) | 63 (60–67) | 0.815 |
| Legal sex, n male (%) | 286 (77) | 0.784 |
| Hepatology at Diagnosis | ||
| Cirrhosis etiology, n (%) | 0.950 | |
| HCV | 208 (56) | |
| NASH | 52 (14) | |
| HCV + ALD | 44 (12) | |
| ALD | 34 (9) | |
| Other | 35 (8) | |
| Child Pugh, n (%) | 0.122 | |
| A | 284 (76) | |
| B | 89 (24) | |
| History of decompensation, n (%) | 119 (32) | 0.980 |
| Sodium mM, median (IQR) | 139 (137–141) | 0.300 |
| Creatinine mg/dL, median (IQR) | 0.9 (0.8–1.2) | 0.026 |
| Creatinine quartiles, n (%) | 0.291 | |
| ≤0.8 mg/dL | 136 (36) | |
| 0.9 mg/dL | 74 (20) | |
| 1.0–1.1 mg/dL | 70 (19) | |
| >1.2 mg/dL | 93 (25) | |
| Bilirubin mg/dL, median (IQR) | 1.0 (0.6–1.6) | 0.154 |
| Albumin g/dL, median (IQR) | 3.4 (2.9–3.7) | 0.002 |
| Albumin quartiles, n (%) | 0.006 | |
| ≤2.9 g/dL | 95 (25) | |
| 3.0–≤3.4 g/dL | 107 (29) | |
| 3.5–≤3.7 g/dL | 84 (23) | |
| >3.7 g/dL | 87 (23) | |
| INR, median (IQR) | 1.1 (1.0–1.2) | 0.018 |
| INR quartiles, n (%) | 0.349 | |
| ≤1.0 | 111 (30) | |
| 1.1 | 116 (31) | |
| 1.2 | 76 (20) | |
| ≥1.3 | 70 (19) | |
| MELD-Na, median (IQR) | 9 (7–12) | 0.819 |
| HCC Baseline | ||
| Multifocal, n (%) | 91 (24) | < 0.001 |
| Index lesion cm, median (IQR) | 2.8 (2.2–3.7) | < 0.001 |
| Milan Criteria, n (%) | 308 (83) | < 0.001 |
| UCSF Criteria, n (%) | 40 (11) | |
| T-Stage, n (%) | < 0.001 | |
| T1 | 282 (76) | |
| T2 | 91 (24) | |
| BCLC Stage, n (%) | < 0.001 | |
| A | 326 (87) | |
| B | 47 (13) | |
| ECOG, n (%) | 0.118 | |
| 0 | 228 (61) | |
| 1 | 145 (39) | |
| AFP ng/mL, median (IQR) | 13 (5.2–75) | < 0.001 |
| AFP ≤ 20 ng/mL, n (%) | 215 (58) | < 0.001 |
| Index Liver-Directed Therapy | ||
| Modality, n (%) | 0.066 | |
| DEE-TACE | 155 (42) | |
| 90Y | 136 (36) | |
| MWA | 82 (22) | |
| Days from diagnosis to treatment, median (IQR) | 56 (39–82) | 0.556 |
| Variate | Milan Model | T-Stage Model | BCLC Model | |||
|---|---|---|---|---|---|---|
| Parameters | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) |
| Albumin quartiles | ||||||
| 3.0–≤3.4 g/dL vs. ≤2.9 g/dL | 0.006 | 2.1 (1.2–3.5) | 0.004 | 2.2 (1.3–3.7) | 0.006 | 2.1 (1.2–3.5) |
| 3.5–≤3.7 g/dL vs. 3.0–≤3.4 g/dL | 0.635 | 0.897 | 0.908 | |||
| >3.7 g/dL vs. 3.5–≤3.7 g/dL | 0.717 | 0.810 | 0.903 | |||
| Milan Criteria | ||||||
| Outside vs. Within | <0.001 | 2.5 (1.6–3.9) | ||||
| T-Stage | ||||||
| T1 vs. T2 | <0.001 | 2.3 (1.5–3.5) | ||||
| BCLC Stage | ||||||
| A vs. B | <0.001 | 2.5 (1.5–4.0) | ||||
| AFP | ||||||
| >20 ng/mL vs. ≤… | <0.001 | 2.7 (1.8–4.2) | <0.001 | 2.8 (1.8–4.3) | <0.001 | 2.8 (1.8–4.3) |
| Variate | Milan Model | T-Stage Model | BCLC Model | |||
|---|---|---|---|---|---|---|
| Parameters | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) |
| Albumin median split | ||||||
| <3.4 g/dL vs. ≥3.4 g/dL | 0.001 | 1.9 (1.3–3.0) | 0.005 | 1.8 (1.2–2.7) | 0.005 | 1.8 (1.2–2.7) |
| Milan Criteria | ||||||
| Outside vs. Within | <0.001 | 2.6 (1.6–4.0) | ||||
| T-Stage | ||||||
| T1 vs. T2 | <0.001 | 2.3 (1.5–3.4) | ||||
| BCLC Stage | ||||||
| A vs. B | <0.001 | 2.6 (1.5–4.1) | ||||
| AFP | ||||||
| >20 ng/mL vs. ≤… | <0.001 | 2.7 (1.8–4.1) | <0.001 | 2.8 (1.8–4.3) | <0.001 | 2.8 (1.8–4.3) |
| Variate | Milan Model | T-Stage Model | BCLC Model | |||
|---|---|---|---|---|---|---|
| Parameters | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) |
| ALBI Grade | ||||||
| Grade 1 vs. Grade 2 | 0.144 | 0.225 | 0.127 | |||
| Grade 2 vs. Grade 3 | 0.037 | 1.9 (1.4–6.3) | 0.031 | 1.9 (1.3–6.0) | 0.061 | |
| Milan Criteria | ||||||
| Outside vs. Within | 0.001 | 2.2 (1.4–3.3) | ||||
| T-Stage | ||||||
| T1 vs. T2 | 0.001 | 2.1 (1.4–3.2) | ||||
| BCLC Stage | ||||||
| A vs. B | 0.002 | 2.3 (1.4–3.6) | ||||
| AFP | ||||||
| >20 ng/mL vs. ≤… | <0.001 | 2.8 (1.8–4.4) | <0.001 | 2.8 (1.9–4.4) | <0.001 | 2.9 (1.9–4.5) |
| Parameters | <3.4 g/dL | ≥3.4 g/dL | p-Value |
|---|---|---|---|
| Cohort, n | 176 | 197 | |
| Study period, date range | |||
| General Demographics | |||
| Age, median (IQR) | 62 (59–66) | 64 (61–67) | 0.003 |
| Legal sex, n male (%) | 122 (69) | 164 (83) | 0.002 |
| Hepatology at Diagnosis | |||
| Cirrhosis etiology, n (%) | 0.735 | ||
| HCV | 95 (54) | 113 (57) | |
| NASH | 27 (15) | 25 (13) | |
| HCV + ALD | 20 (11) | 24 (12) | |
| ALD | 19 (11) | 15 (8) | |
| Other | 15 (9) | 20 (10) | |
| Child Pugh, n (%) | <0.001 | ||
| A | 94 (53) | 190 (96) | |
| B | 82 (47) | 7 (4) | |
| History of decompensation, n (%) | 87 (49) | 32 (16) | <0.001 |
| Sodium mM, median (IQR) | 138 (136–140) | 140 (138–141) | <0.001 |
| Creatinine mg/dL, median (IQR) | 0.9 (0.8–1.2) | 0.9 (0.8–1.1) | 0.430 |
| Bilirubin mg/dL, median (IQR) | 1.4 (0.9–2.1) | 0.8 (0.5–1.2) | <0.001 |
| INR, median (IQR) | 1.2 (1.1–1.3) | 1.1 (1.0–1.1) | <0.001 |
| ALBI Grade, n (%) | <0.001 | ||
| Grade 1 | 0 (0) | 67 (34) | |
| Grade 2 | 122 (69) | 130 (66) | |
| Grade 3 | 54 (31) | 0 (0) | |
| MELD-Na, median (IQR) | 11 (8–14) | 8 (7–10) | <0.001 |
| HCC Baseline | |||
| Multifocal, n (%) | 44 (25) | 46 (23) | 0.717 |
| Index lesion cm, median (IQR) | 2.8 (2.2–3.8) | 2.8 (2.2–3.7) | 0.897 |
| Milan Criteria, n (%) | 147 (84) | 161 (82) | 0.683 |
| T-Stage, n (%) | 0.631 | ||
| T1 | 131 (74) | 151 (77) | |
| T2 | 45 (26) | 46 (23) | |
| BCLC Stage, n (%) | 0.876 | ||
| A | 153 (87) | 173 (88) | |
| B | 23 (13) | 24 (12) | |
| ECOG, n (%) | 0.001 | ||
| 0 | 92 (52) | 136 (69) | |
| 1 | 84 (48) | 61 (31) | |
| AFP ng/mL, median (IQR) | 16 (6–73) | 10 (5–79) | 0.142 |
| AFP ≤ 20 ng/mL, n (%) | 98 (56) | 117 (60) | 0.461 |
| Index Liver-Directed Therapy | |||
| Modality, n (%) | 0.002 | ||
| DEE-TACE | 89 (51) | 66 (34) | |
| 90Y | 50 (28) | 86 (44) | |
| MWA | 37 (21) | 45 (23) | |
| Days from diagnosis to treatment, median (IQR) | 58 (36–84) | 55 (34–81) | 0.398 |
| Objective Response Rate, n (%) | 0.131 | ||
| CR/PR | 108 (61) | 140 (71) | |
| SD/DP | 53 (30) | 46 (23) | |
| NA | 15 (9) | 11 (6) | |
| Primary Endpoint | 117 (66) | 99 (50) | 0.514 |
| Liver transplantation, n (%) | 63 (54) | 54 (55) | |
| Tumor progression, n (%) | 54 (46) | 45 (45) | |
| Source of Tumor Progression | 0.778 | ||
| Index progression, n (%) | 33 (61) | 25 (56) | |
| New disease, n (%) | 21 (39) | 20 (44) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Núñez, K.G.; Sandow, T.; Patel, J.; Hibino, M.; Fort, D.; Cohen, A.J.; Thevenot, P. Hypoalbuminemia Is a Hepatocellular Carcinoma Independent Risk Factor for Tumor Progression in Low-Risk Bridge to Transplant Candidates. Cancers 2022, 14, 1684. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14071684
Núñez KG, Sandow T, Patel J, Hibino M, Fort D, Cohen AJ, Thevenot P. Hypoalbuminemia Is a Hepatocellular Carcinoma Independent Risk Factor for Tumor Progression in Low-Risk Bridge to Transplant Candidates. Cancers. 2022; 14(7):1684. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14071684
Chicago/Turabian StyleNúñez, Kelley G., Tyler Sandow, Jai Patel, Mina Hibino, Daniel Fort, Ari J. Cohen, and Paul Thevenot. 2022. "Hypoalbuminemia Is a Hepatocellular Carcinoma Independent Risk Factor for Tumor Progression in Low-Risk Bridge to Transplant Candidates" Cancers 14, no. 7: 1684. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14071684