
Dietary Fat Intake: Associations with Dietary Patterns and Postmenopausal Breast Cancer—A Case-Control Study

 ,
,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
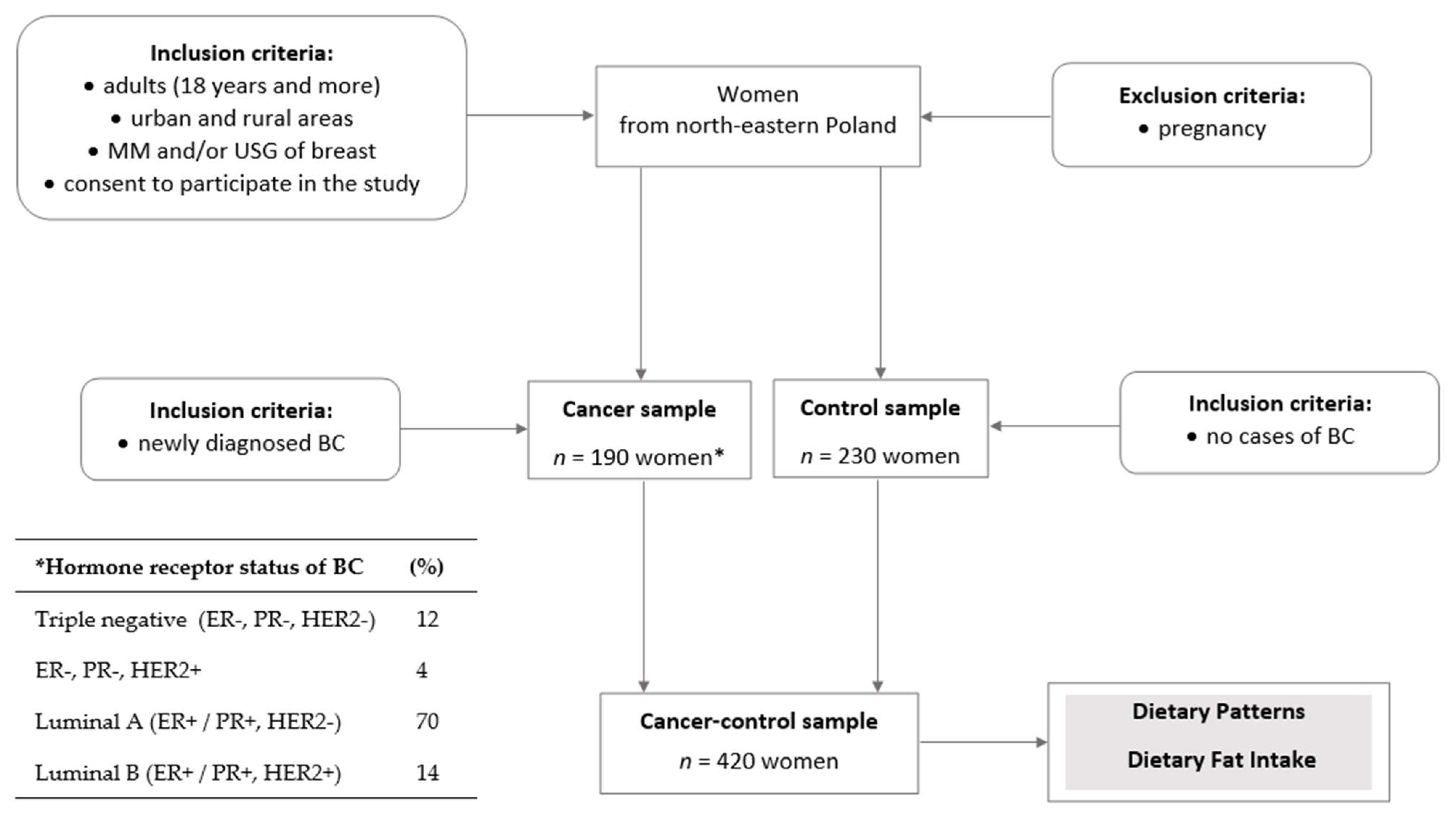
2.1. Study Design and Sample Collection
2.2. Dietary Patterns Identification
2.3. Dietary Fat Intake Assessment
(b11 ∗ salad dressings) + (b12 ∗ rice) + (b13 ∗ regular fat).
2.4. Statistical Analysis
3. Results
3.1. Dietary Fat Intake and Dietary Patterns
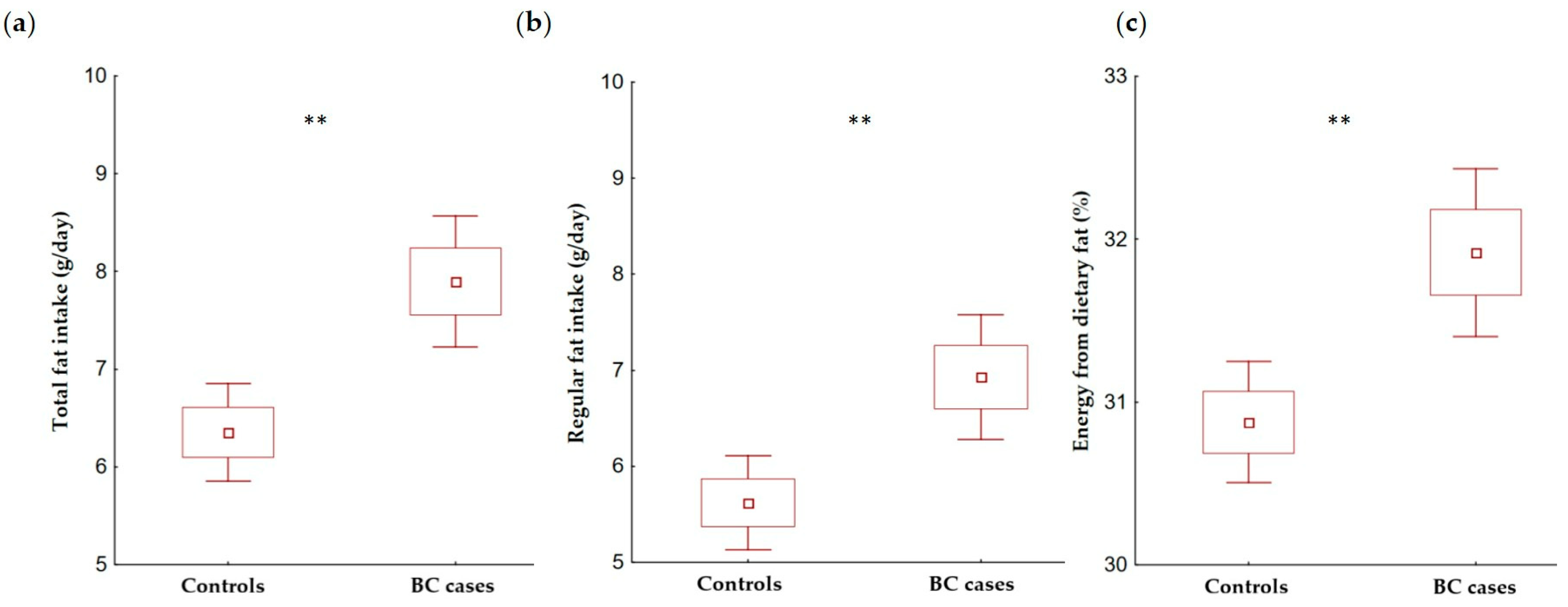
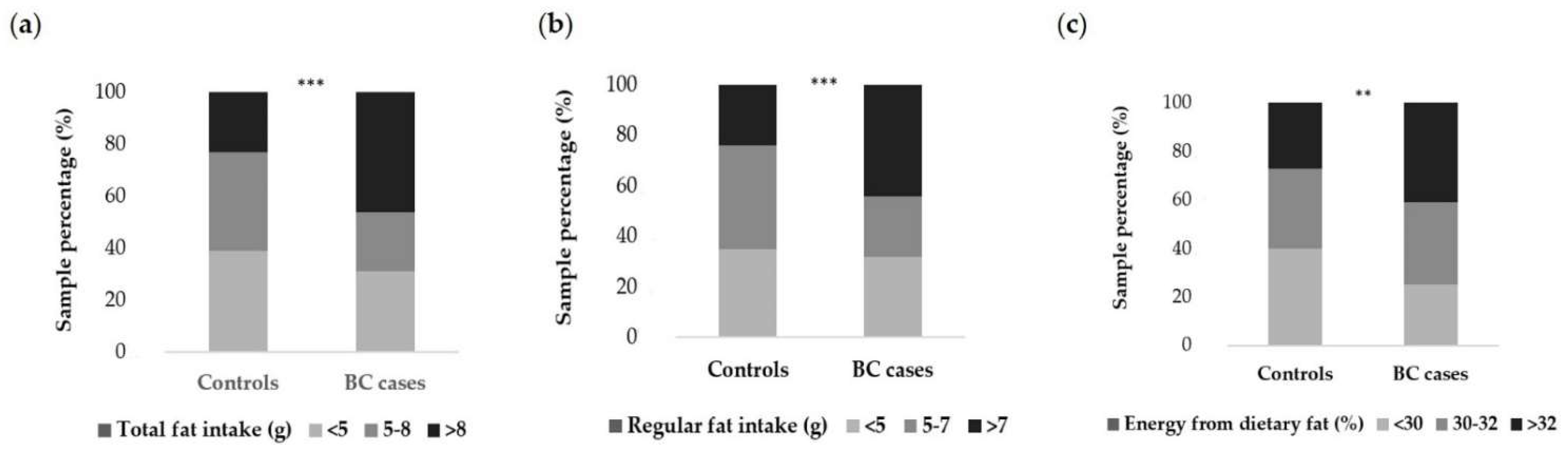
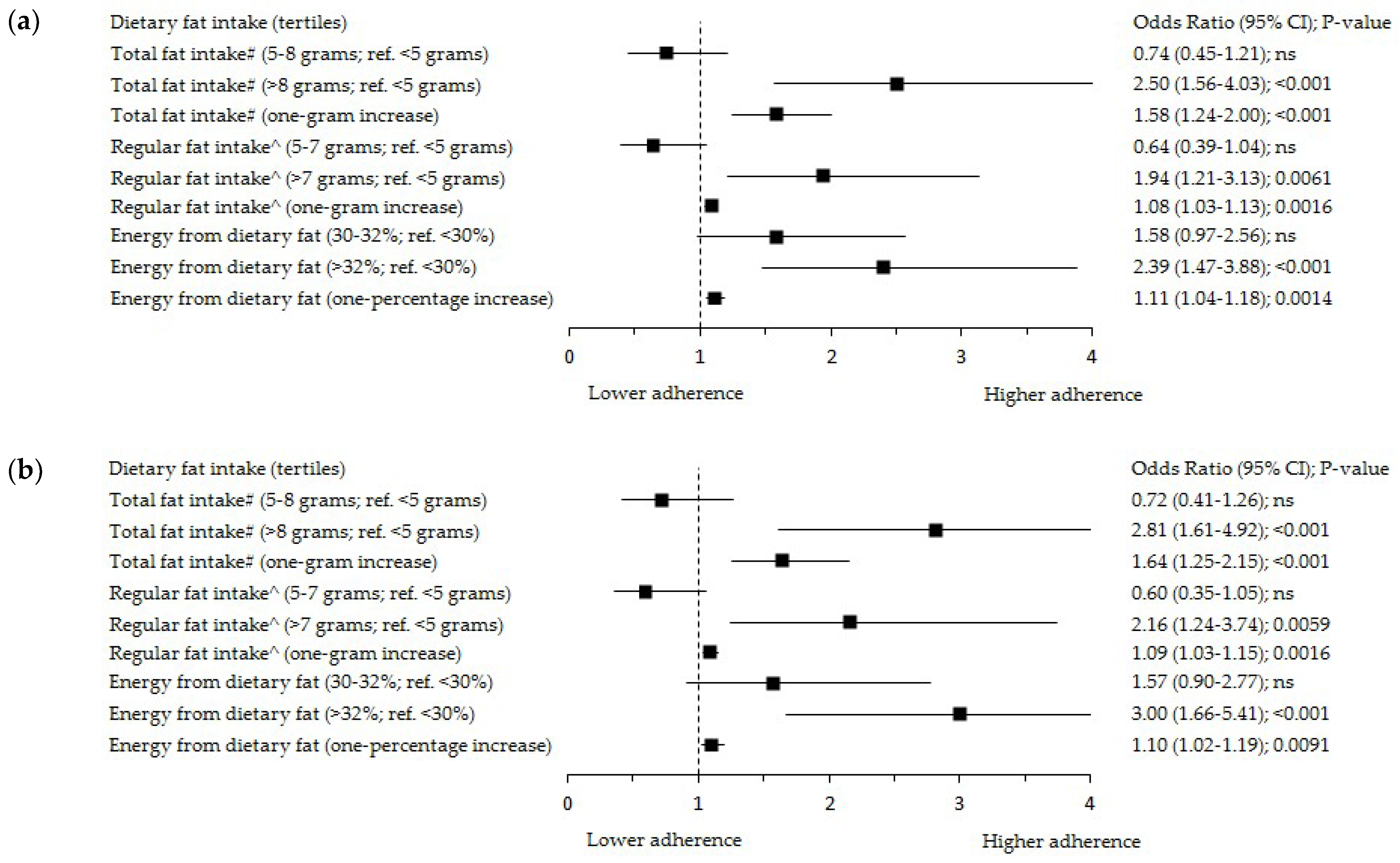
3.2. Dietary Fat Intake and Breast Cancer
4. Discussion
4.1. Dietary Fat Intake in Total Sample
4.2. Dietary Fat Intake and Breast Cancer
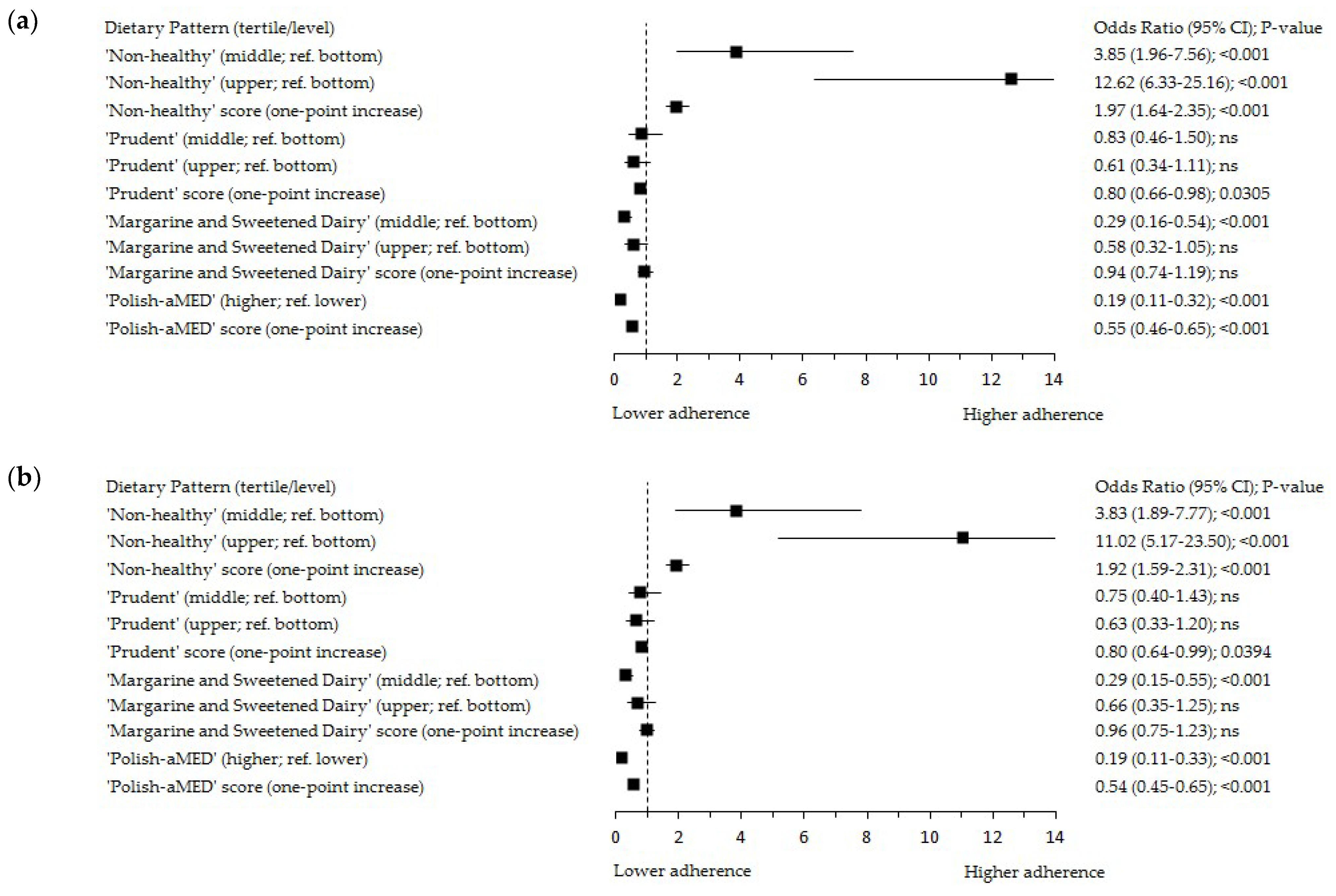
4.3. Dietary Fat Intake and Dietary Patterns in Associations with Breast Cancer
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. Ca Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization—Cancer Country Profiles. 2020. Available online: https://www.who.int/cancer/country-profiles (accessed on 5 November 2021).
- Krajowy Rejestr Nowotworów, Centrum Onkologii—Instytut im. Marii Skłodowskiej—Curie (Polish National Cancer Registry, Oncology Centre. Institute of M. Sklodowska-Curie). Available online: http://onkologia.org.pl/k/epidemiologia/ (accessed on 3 November 2021). (In Polish).
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. In Diet, Nutrition, Physical Activity, and Breast Cancer; American Institute for Cancer Research: Washington, DC, USA, 2018. [Google Scholar]
- Tao, Z.; Shi, A.; Lu, C.; Song, T.; Zhang, Z.; Zhao, J. Breast cancer: Epidemiology and etiology. Cell Biochem. Biophys. 2015, 72, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Loda, M.; Mucci, L.A.; Mittelstadt, M.L.; Van Hemelrijck, M.; Cotter, M.B. Pathology and Epidemiology of Cancer; Springer: Berlin/Heidelberg, Germany, 2017; pp. 156–166. [Google Scholar]
- Combet, E.; Gray, S.R. Nutrient-nutrient interactions: Competition, bioavailability, mechanism and function in health and diseases. Proc. Nutr. Soc. 2019, 78, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escrich, E.; Solanas, M.; Moral, R.; Escrich, R. Modulatory effects and molecular mechanisms of olive oil and other dietary lipids in breast cancer. Curr. Pharm. Des. 2011, 17, 813–830. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, Y.; Conroy, S.M.; Pagano, I.; Franke, A.A.; Stanczyk, F.Z.; Maskarinec, G. Influence of diet on nipple aspirate fluid production and estrogen levels. Food Funct. 2011, 2, 665–670. [Google Scholar] [CrossRef]
- Key, T.J.; Appleby, P.N.; Cairns, B.J.; Luben, R.; Dahm, C.C.; Akbaraly, T.; Brunner, E.J.; Burley, V.; Cade, J.E.; Greenwood, D.C.; et al. Dietary fat and breast cancer: Comparison of results from food diaries and food-frequency questionnaires in the UK Dietary Cohort Consortium. Am. J. Clin. Nutr. 2011, 94, 1043–1052. [Google Scholar] [CrossRef]
- Psaltopoulou, T.; Kosti, R.I.; Haidopoulos, D.; Dimopoulos, M.; Panagiotakos, D.B. Olive oil intake is inversely related to cancer prevalence: A systematic review and a meta-analysis of 13800 patients and 23340 controls in 19 observational studies. Lipids Health Dis. 2011, 10, 127. [Google Scholar] [CrossRef] [Green Version]
- Kruk, J.; Marchlewicz, M. Dietary Fat and Physical Activity in Relation to Breast Cancer among Polish Women. Asian Pac. J. Cancer Prev. 2013, 14, 2495–2502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xin, Y.; Li, X.-Y.; Sun, S.-R.; Wang, L.-X.; Huang, T. Vegetable Oil Intake and Breast Cancer Risk: A Meta-analysis. Asian Pac. J. Cancer Prev. 2015, 16, 5125–5135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Tan, Y.S.; Aupperlee, M.D.; Langohr, I.M.; Kirk, E.L.; Troester, M.A.; Schwartz, R.C.; Haslam, S.Z. Pubertal high fat diet: Effects on mammary cancer development. Breast Cancer Res. 2013, 15, R100. [Google Scholar] [CrossRef] [Green Version]
- Hauner, D.; Janni, W.; Rack, B.; Hauner, H. The effect of overweight and nutrition on prognosis in breast cancer. Dtsch. Arztebl. Int. 2011, 108, 795–801. [Google Scholar] [CrossRef]
- Cao, Y.; Hou, L.; Wang, W. Dietary total fat and fatty acids intake, serum fatty acids and risk of breast cancer: A meta-analysis of prospective cohort studies. Int. J. Cancer 2016, 138, 1894–1904. [Google Scholar] [CrossRef] [PubMed]
- Chlebowski, R.T.; Aragaki, A.K.; Anderson, G.L.; Pan, K.; Neuhouser, M.L.; Manson, J.E.; Thomson, C.A.; Mossavar-Rahmani, Y.; Lane, D.S.; Johnson, K.C.; et al. Dietary Modification and Breast Cancer Mortality: Long-Term Follow-Up of the Women’s Health Initiative Randomized Trial. J. Clin. Oncol. 2020, 38, 1419–1428. [Google Scholar] [CrossRef] [PubMed]
- Chlebowski, R.T.; Aragaki, A.K.; Anderson, G.L.; Thomson, C.A.; Manson, J.E.; Simon, M.S.; Howard, B.V.; Rohan, T.E.; Snetselar, L.; Lane, D.; et al. Low-Fat Dietary Pattern and Breast Cancer Mortality in the Women’s Health Initiative Randomized Controlled Trial. J. Clin. Oncol. 2017, 35, 2919–2926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beasley, J.M.; Newcomb, P.A.; Trentham-Dietz, A.; Hampton, J.M.; Bersch, A.J.; Passarelli, M.N.; Holick, C.N.; Titus-Ernstoff, L.; Egan, K.M.; Holmes, M.D.; et al. Post-diagnosis dietary factors and survival after invasive breast cancer. Breast Cancer Res. Treat. 2011, 128, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Sczaniecka, A.K.; Brasky, T.M.; Lampe, J.W.; Patterson, R.E.; White, E. Dietary intake of specific fatty acids and breast cancer risk among postmenopausal women in the VITAL cohort. Nutr. Cancer 2012, 64, 1131–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makarem, N.; Chandran, U.; Bandera, E.V.; Parekh, N. Dietary Fat in Breast Cancer Survival. Annu. Rev. Nutr. 2013, 33. [Google Scholar] [CrossRef] [Green Version]
- Boeke, C.E.; Eliassen, A.H.; Chen, W.Y.; Cho, E.; Holmes, M.D.; Rosner, B.; Willett, W.C.; Tamimi, R.M. Dietary fat intake in relation to lethal breast cancer in two large prospective cohort studies. Breast Cancer Res. Treat. 2014, 146, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Farvid, M.S.; Cho, E.; Chen, W.Y.; Eliassen, A.H.; Willett, W.C. Premenopausal dietary fat in relation to pre- and post-menopausal breast cancer. Breast Cancer Res. Treat. 2014, 145, 255–265. [Google Scholar] [CrossRef]
- Thomson, C.A.; Van Horn, L.; Caan, B.J.; Aragaki, A.K.; Chlebowski, R.T.; Manson, J.E.; Rohan, T.E.; Tinker, L.F.; Kuller, L.H.; Hou, L.; et al. Cancer Incidence and Mortality during the intervention and post intervention periods of the Women’s Health Initiative Dietary Modification Trial. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 2924–2935. [Google Scholar] [CrossRef] [Green Version]
- Bertrand, K.A.; Burian, R.A.; Eliassen, A.H.; Willett, W.C.; Tamimi, R.M. Adolescent intake of animal fat and red meat in relation to premenopausal mammographic density. Breast Cancer Res. Treat. 2016, 155, 385–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.L.; Cho, D.; Salner, A.L.; Dornelas, E. A Randomized Controlled Trial of Two Mail-based Lifestyle Interventions for Breast Cancer Survivors. Support Care Cancer 2016, 24, 3037–3046. [Google Scholar] [CrossRef] [Green Version]
- Jung, S.; Goloubeva, O.; Klifa, C.; LeBlanc, E.S.; Snetselaar, L.G.; Van Horn, L.; Dorgan, J.F. Dietary fat intake during adolescence and breast density among young women. Cancer Epidemiol. Biomarkers Prev. 2016, 25, 918–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Z.; Rundle, A.; Genkinger, J.M.; Cheung, Y.K.; Ergas, I.J.; Roh, J.M.; Kushi, L.H.; Kwan, M.L.; Greenlee, H. Distinct trajectories of fruits and vegetables, dietary fat, and alcohol intake following a breast cancer diagnosis: The Pathways Study. Breast Cancer Res. Treat. 2020, 179, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Prentice, R.L.; Aragaki, A.K.; Howard, B.V.; Chlebowski, R.Y.; Thomson, C.A.; Van Horn, L.; Tinker, L.F.; Manson, J.E.; Anderson, G.L.; Kuller, L.E.; et al. Low-Fat Dietary Pattern among Postmenopausal Women Influences Long-Term Cancer, Cardiovascular Disease, and Diabetes Outcomes. J. Nutr. 2019, 149, 1565–1574. [Google Scholar] [CrossRef] [PubMed]
- Prentice, R.L.; Howard, B.V.; Van Horn, L.; Neuhouser, M.L.; Anderson, G.L.; Tinker, L.F.; Lampe, J.W.; Raftery, D.; Pettinger, M.; Aragaki, A.K.; et al. Nutritional epidemiology and the Women’s Health Initiative: A review. Am. J. Clin. Nutr. 2021, 113, 1083–1092. [Google Scholar] [CrossRef]
- Chlebowski, R.T.; Aragaki, A.K.; Prentice, R.L. Association of Low-Fat Dietary Pattern With Breast Cancer Overall Survival. JAMA Oncol. 2019, 11, 580. [Google Scholar] [CrossRef]
- Cena, H.; Calder, P.C. Defining a Healthy Diet: Evidence for the Role of Contemporary Dietary Patterns in Health and Disease. Nutrients 2020, 12, 334. [Google Scholar] [CrossRef] [Green Version]
- World Cancer Research Fund International/American Institute for Cancer Research Continuous Update Project Report: Diet, Nutrition, Physical Activity, and Breast Cancer Survivors. 2018. Available online: www.wcrf.org/sites/default/files/Breast-Cancer-Survivors-2018-Report.pdf (accessed on 22 February 2022).
- Previdelli, Á.N.; de Andrade, S.C.; Fisberg, R.M.; Marchioni, D.M. Using two different approaches to assess dietary patterns: Hypothesis-driven and data-driven analysis. Nutrients 2016, 8, 593. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Y.; Xia, J.; Li, L.; Ke, Y.; Cheng, J.; Xie, Y.; Chu, W.; Cheung, P.; Kim, J.H.; Colditz, G.H.; et al. Associations between dietary patterns and the risk of breast cancer: A systematic review and meta-analysis of observational studies. Breast Cancer Res. 2019, 21, 16. [Google Scholar] [CrossRef] [Green Version]
- Guinter, M.A.; McLain, A.C.; Merchant, A.T.; Sandler, D.P.; Steck, S.E. A dietary pattern based on estrogen metabolism is associated with breast cancer risk in a prospective cohort of postmenopausal women. Int. J. Cancer 2018, 143, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Dela Cruz, R.; Park, S.-Y.; Shvetsov, Y.B.; Boushey, C.J.; Monroe, K.R.; Le Marchand, L.; Maskarinec, G. Diet quality and breast cancer incidence in the Multiethnic Cohort. Eur. J. Clin. Nutr. 2020, 74, 1743–1747. [Google Scholar] [CrossRef] [PubMed]
- De Cicco, P.; Catani, M.V.; Gasperi, V.; Sibilano, M.; Quaglietta, M.; Savini, I. Nutrition and Breast Cancer: A Literature Review on Prevention, Treatment and Recurrence. Nutrients 2019, 11, 1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, T.M.; Vitolins, M.Z.; Cook, K.L. From the Table to the Tumor: The Role of Mediterranean and Western Dietary Patterns in Shifting Microbial-Mediated Signaling to Impact Breast Cancer Risk. Nutrients 2019, 11, 2565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pot, G.K.; Stephen, A.M.; Dahm, C.C.; Key, T.J.; Cairns, B.J.; Burley, V.J.; Cade, J.E.; Greenwood, D.C.; Keogh, R.H.; Bhaniani, A.; et al. Dietary patterns derived with multiple methods from food diaries and breast cancer risk in the UK Dietary Cohort Consortium. Eur. J. Clin. Nutr. 2014, 68, 1353–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirko, K.A.; Willett, W.C.; Hankinson, S.E.; Rosner, B.A.; Beck, A.H.; Tamimi, R.M.; Eliassen, A.H. Healthy dietary patterns and risk of breast cancer by molecular subtype. Breast Cancer Res. Treat. 2016, 155, 579–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mourouti, N.; Papavagelis, C.; Plytzanopoulou, P.; Kontogianni, M.; Vassilakou, T.; Malamos, N.; Linos, A.; Panagiotakos, D. Dietary patterns and breast cancer: A case-control study in women. Eur. J. Nutr. 2015, 54, 609–617. [Google Scholar] [CrossRef]
- Link, L.B.; Canchola, A.J.; Bernstein, L.; Clarke, C.A.; Stram, D.O.; Ursin, G.; Horn-Ross, P.L. Dietary patterns and breast cancer risk in the California Teachers Study cohort. Am. J. Clin. Nutr. 2013, 98, 1524–1532. [Google Scholar] [CrossRef] [Green Version]
- Sieri, S.; Agnoli, C.; Pala, V.; Mattiello, A.; Panico, S.; Masala, G.; Assedi, M.; Tumino, R.; Frasca, G.; Sacerdote, C.; et al. Dietary habits and cancer: The experience of EPIC-Italy. Epidemiol. Prev. 2015, 39, 333–338. [Google Scholar]
- Penniecook-Sawyers, J.A.; Jaceldo-Siegl, K.; Fan, J.; Beeson, L.; Knutsen, S.; Herring, P.; Fraser, G.E. Vegetarian dietary patterns and the risk of breast cancer in a low-risk population. Br. J. Nutr. 2016, 10, 1790–1797. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Huang, S.; Cao, L.; Ge, M.; Li, Y.; Shao, J. Vegetable-Fruit-Soybean Dietary Pattern and Breast Cancer: A Meta-Analysis of Observational Studies. J. Nutr. Sci. Vitaminol. 2019, 65, 375–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro-Quezada, I.; Román-Viñas, B.; Serra-Majem, L. The Mediterranean Diet and Nutritional Adequacy: A Review. Nutrients 2014, 6, 231–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: An updated systematic review and meta-analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health Benefits of the Mediterranean Diet: Metabolic and Molecular Mechanisms. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 318–326. [Google Scholar] [CrossRef] [Green Version]
- Van den Brandt, P.A.; Schulpen, M. Mediterranean diet adherence and risk of postmenopausal breast cancer: Results of a cohort study and meta-analysis. Int. J. Cancer 2017, 140, 2220–2231. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, M.A.; Martín-Calvo, N. Mediterranean diet and life expectancy; beyond olive oil, fruits and vegetables. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 401–407. [Google Scholar] [CrossRef]
- Mirabelli, M.; Chiefari, E.; Arcidiacono, B.; Corigliano, D.M.; Brunetti, F.S.; Maggisano, V.; Russo, D.; Foti, D.P.; Brunetti, A. Mediterranean Diet Nutrients to Turn the Tide against Insulin Resistance and Related Diseases. Nutrients 2020, 12, 1066. [Google Scholar] [CrossRef] [Green Version]
- Turati, F.; Carioli, G.; Bravi, F.; Ferraroni, M.; Serraino, D.; Montella, M.; Giacosa, A.; Toffolutti, F.; Negri, E.; Levi, F.; et al. Mediterranean diet and breast cancer risk. Nutrients 2018, 10, 326. [Google Scholar] [CrossRef] [Green Version]
- Black, M.H.; Watanabe, R.M.; Trigo, E.; Takayanagi, M.; Lawrence, J.M.; Buchanan, T.A.; Xiang, A.H. High-Fat Diet Is Associated with Obesity-Mediated Insulin Resistance and b-Cell Dysfunction in Mexican Americans. J. Nutr. 2013, 143, 479–485. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Nutrition Policy Review 2016–2017: Country Progress in Creating Enabling Policy Environments for Promoting Healthy Diets and Nutrition (DRAFT), 2018; World Health Organization, Department of Nutrition for Health and Develop-ment (NHD), Nutrition Policy and Scientific AdviceUnit (NPU): Geneva, Switzerland, 2018. [Google Scholar]
- European Food Safety Authority (EFSA). Dietary Reference Values for Nutrients; Summary Report, EFSA Supporting Publication 2017, e15121 (Update 2019); EFSA: Parma, Italy, 2017. [Google Scholar] [CrossRef] [Green Version]
- Waśkiewicz, A.; Szcześniewska, D.; Szostak-Węgierek, D.; Kwaśniewska, M.; Pająk, A.; Stepaniak, U.; Kozakiewicz, K.; Tykarski, A.; Zdrojewski, T.; Zujko, M.E.; et al. Are dietary habits of the Polish population consistent with the recommendations for prevention of cardiovascular disease?—WOBASZ II project. Kardiol. Pol. 2016, 74, 969–977. [Google Scholar] [CrossRef] [Green Version]
- Krusinska, B.; Wadolowska, L.; Slowinska, M.A.; Biernacki, M.; Drozdowski, M.; Chadzynski, T. Associations of dietary patterns and metabolic-hormone profiles with breast cancer risk: A case-control study. Nutrients 2018, 10, 2013. [Google Scholar] [CrossRef] [Green Version]
- Krusinska, B.; Hawrysz, I.; Wadolowska, L.; Slowinska, M.A.; Biernacki, M.; Czerwinska, A.; Golota, J.J. Associations of Mediterranean diet and a posteriori derived dietary patterns with breast and lung cancer risk: A case-control study. Nutrients 2018, 10, 470. [Google Scholar] [CrossRef] [Green Version]
- Niedzwiedzka, E.; Wadolowska, L.; Kowalkowska, J. Reproducibility of a non-quantitative Food Frequency Questionnaire (62-item FFQ-6) and PCA-driven dietary pattern identification in 13–21-year-old females. Nutrients 2019, 11, 2183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lidia Wadolowska Website. Available online: http://www.uwm.edu.pl/edu/lidiawadolowska/ (accessed on 20 July 2018).
- Stachowska, E.; Ryterska, K.; Maciejewska, D.; Banaszczak, M.; Milkiewicz, P.; Milkiewicz, M.; Gutowska, I.; Ossowski, P.; Kaczorowska, M.; Jamioł-Milc, D.; et al. Nutritional Strategies for the individualized treatment of Non-Alcoholic Fatty Liver Disease (NAFLD) based on the Nutrient-Induced Insulin Output Ratio (NIOR). Int. J. Mol. Sci. 2016, 17, 1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FAO. Dietary Assessment: A Resource Guide to Method Selection and Application in Low Resource Settings; FAO: Rome, Italy, 2018. [Google Scholar]
- Armitage, P.; Berry, G.; Matthews, J.N.S. Statistical Methods in Medical Research, 4th ed.; Blackwell Science: Oxford, UK, 2001. [Google Scholar]
- Leeming, E.R.; Louca, P.; Gibson, R.; Menni, C.; Spector, T.D.; Le Roy, C.I. The complexities of the diet-microbiome relationship: Advances and perspectives. Genome Med. 2021, 13, 10. [Google Scholar] [CrossRef]
- National Cancer Institute, Division of Cancer Control and Population Sciences—Percentage Energy from Fat Screener: Scoring Procedures. Available online: https://epi.grants.cancer.gov/diet/screeners/fat/scoring.html (accessed on 24 July 2020).
- U.S. Department of Agriculture, Agricultural Research Service. Data tables: Results from USDA’s 1994–96 Continuing Survey of Food Intakes by Individuals and 1994-96 Diet and Health Knowledge Survey. 1997. Available online: https://www.ars.usda.gov/ (accessed on 12 August 2021).
- Jarosz, M.; Taraszewska, A. Nadwaga i otyłosc oraz wybrane elementy stylu zycia jako czynniki ryzyka GERD. (Overweight and obesity and selected lifestyle elements as risk factors for GERD). Postepy Nauk Medycznych 2011, 9, 749–759. (In Polish) [Google Scholar]
- Wadolowska, L.; Stasiewicz, B. The manual for developing nutritional data from the KomPAN® questionnaire. In KomPAN® Dietary Habits and Nutrition Beliefs Questionnaire and the Manual for Developing Nutritional Data; Gawecki, J., Ed.; Chapter 3; The Committee of Human Nutrition, Polish Academy of Sciences: Olsztyn, Poland, 2020; pp. 35–56. Available online: http://www.knozc.pan.pl/ (accessed on 23 February 2022).
- Krusinska, B.; Wadolowska, L.; Biernacki, M.; Slowinska, M.A.; Drozdowski, M. Serum ‘Vitamin-Mineral’ Profiles: Associations with Postmenopausal Breast Cancer Risk Including Dietary Patterns and Supplementation. A Case-Control Study. Nutrients 2019, 11, 2244. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total Sample | Energy from Dietary Fat (Tertiles) | p-Value | ||
|---|---|---|---|---|---|
| Bottom (<30%) | Middle (30–32%) | Upper (>32%) | |||
| Sample size (number) | 420 | 139 | 141 | 140 | |
| Breast cancer cases (%) | 45.2 | 34.5 | 45.4 | 55.7 | 0.0018 |
| Age (years) # | 59.9 (8.6) | 60.4 (8.4) | 60.8 (8.2) | 58.6 (9.0) | 0.0437 |
| 40.0–49.9 | 15.5 | 12.9 | 12.1 | 21.4 | |
| 50.0–59.9 | 30.0 | 30.9 | 24.8 | 34.3 | 0.0319 |
| 60.0–69.9 | 42.6 | 41.0 | 51.8 | 35.0 | |
| 70.0–79.9 | 11.9 | 15.1 | 11.3 | 9.3 | |
| Menopausal status (%) | |||||
| Peri-menopausal | 14.8 | 10.1 | 12.8 | 21.4 | 0.0200 |
| Postmenopausal | 85.2 | 89.9 | 87.2 | 78.6 | |
| BMI (kg/m2) a# | 27.9 (5.0) | 27.8 (4.7) | 28.2 (5.1) | 27.8 (5.0) | 0.7735 |
| Underweight (<18.5) | 0.7 | 0.7 | 0.7 | 0.7 | |
| Normal weight (18.5–24.9) | 29.2 | 30.9 | 25.0 | 31.7 | 0.7914 |
| Overweight (25.0–29.9) | 39.0 | 35.3 | 44.3 | 37.4 | |
| Obesity (≥30.0) | 31.1 | 33.1 | 30.0 | 30.2 | |
| Waist circumference (cm) a# | 92.0 (13.2) | 90.2 (12.0) | 92.4 (12.6) | 93.3 (14.6) | 0.1852 |
| Waist-to-height ratio a# | 0.57 (0.08) | 0.56 (0.08) | 0.57 (0.08) | 0.58 (0.09) | 0.2945 |
| Place of residence (%) | |||||
| Village | 28.1 | 25.9 | 26.2 | 32.1 | |
| Town (<20,000 inhabitants) | 15.2 | 12.2 | 14.2 | 19.3 | 0.0652 |
| Town (20–100,000 inhabitants) | 20.5 | 25.2 | 15.6 | 20.7 | |
| City (>100,000 inhabitants) | 36.2 | 36.7 | 44.0 | 27.9 | |
| Education level (%) | |||||
| Primary | 13.6 | 12.2 | 13.5 | 15.0 | |
| Secondary | 58.3 | 48.9 | 60.3 | 65.7 | 0.0084 |
| Higher | 28.1 | 38.8 | 26.2 | 19.3 | |
| Economic situation (%) | |||||
| Below average | 16.0 | 14.4 | 13.5 | 20.0 | |
| Average | 71.2 | 68.3 | 73.8 | 71.4 | 0.1595 |
| Above average | 12.9 | 17.3 | 12.8 | 8.6 | |
| Situation of household (%) | |||||
| We live poorly | 0.2 | 0.0 | 0.7 | 0.0 | |
| We live very thriftily | 16.9 | 15.8 | 14.2 | 20.7 | |
| We live thriftily | 56.0 | 59.7 | 56.0 | 52.1 | 0.6788 |
| We live well | 24.8 | 23.0 | 27.0 | 24.3 | |
| We live very well | 2.1 | 1.4 | 2.1 | 2.9 | |
| Socioeconomic index (points) b# | 9.9 (2.1) | 10.1 (2.1) | 10.0 (2.2) | 9.5 (2.0) | 0.0081 |
| Socioeconomic status (%) b | |||||
| Low | 41.0 | 34.5 | 34.0 | 54.3 | |
| Average | 36.7 | 38.8 | 42.6 | 28.6 | 0.0030 |
| High | 22.4 | 26.6 | 23.4 | 17.1 | |
| Physical activity at work (%) c | |||||
| Low | 54.0 | 60.4 | 61.7 | 40.0 | |
| Moderate | 32.6 | 27.3 | 29.8 | 40.7 | 0.0011 |
| High | 13.3 | 12.2 | 8.5 | 19.3 | |
| Physical activity in leisure time (%) d | |||||
| Low | 22.6 | 17.3 | 26.2 | 24.3 | |
| Moderate | 64.3 | 64.0 | 62.4 | 66.4 | 0.0862 |
| High | 13.1 | 18.7 | 11.3 | 9.3 | |
| Overall physical activity (%) e | |||||
| Low | 52.9 | 53.2 | 61.0 | 44.3 | |
| Moderate | 44.0 | 43.9 | 36.9 | 51.4 | 0.0852 |
| High | 3.1 | 2.9 | 2.1 | 4.3 | |
| Smokers (%) f | 53.1 | 46.8 | 51.1 | 61.4 | 0.0413 |
| Abuse of alcohol (%) g | 4.0 | 2.2 | 4.3 | 5.7 | 0.3175 |
| Age at menarche (years) | |||||
| <12 | 12.1 | 8.6 | 12.1 | 15.7 | |
| 12–14.9 | 63.3 | 64.0 | 65.2 | 60.7 | 0.4311 |
| ≥15 | 24.5 | 27.3 | 22.7 | 23.6 | |
| Number of full-term pregnancies (%) | |||||
| 0 | 12.1 | 12.9 | 13.5 | 10.0 | |
| 1–2 | 61.7 | 66.2 | 63.8 | 55.0 | 0.0691 |
| ≥3 | 26.2 | 20.9 | 22.7 | 35.0 | |
| Oral contraceptive use (%) h | 20.2 | 25.2 | 19.1 | 16.4 | 0.1768 |
| Hormone-replacement therapy use (%) h | 16.7 | 25.2 | 12.1 | 12.9 | 0.0044 |
| Vitamin/mineral supplements use (%) i | 38.6 | 42.4 | 35.5 | 37.9 | 0.4755 |
| Family history of BC (%) j | 19.3 | 27.3 | 19.1 | 11.4 | 0.0104 |
| Diagnosed chronic diseases (%) | 56.9 | 61.2 | 57.4 | 52.1 | 0.3114 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stasiewicz, B.; Wadolowska, L.; Biernacki, M.; Slowinska, M.A.; Stachowska, E. Dietary Fat Intake: Associations with Dietary Patterns and Postmenopausal Breast Cancer—A Case-Control Study. Cancers 2022, 14, 1724. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14071724
Stasiewicz B, Wadolowska L, Biernacki M, Slowinska MA, Stachowska E. Dietary Fat Intake: Associations with Dietary Patterns and Postmenopausal Breast Cancer—A Case-Control Study. Cancers. 2022; 14(7):1724. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14071724
Chicago/Turabian StyleStasiewicz, Beata, Lidia Wadolowska, Maciej Biernacki, Malgorzata Anna Slowinska, and Ewa Stachowska. 2022. "Dietary Fat Intake: Associations with Dietary Patterns and Postmenopausal Breast Cancer—A Case-Control Study" Cancers 14, no. 7: 1724. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14071724