
Care Management and Survival of Patients Diagnosed with Synchronous Metastatic Colorectal Cancer: A High-Resolution Population-Based Study in Two French Areas

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Covariates
2.3. Statistical Analysis
2.4. Missing Data
3. Results
3.1. Overall Population
3.2. Group 1: Patients Receiving No Treatment or Only RT
3.3. Group 2: Patients Receiving CT (+/− RT)
3.4. Group 3: Patients Receiving PTR (+/− RT)
3.5. Group 4: Patients Receiving PTR + CT (+/− RT)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brouwer, N.P.M.; Bos, A.C.R.K.; Lemmens, V.E.P.P.; Tanis, P.J.; Hugen, N.; Nagtegaal, I.D.; de Wilt, J.H.W.; Verhoeven, R.H.A. An overview of 25 years of incidence, treatment and outcome of colorectal cancer patients. Int. J. Cancer 2018, 143, 2758–2766. [Google Scholar] [CrossRef] [PubMed]
- Goey, K.K.H.; ’t Lam-Boer, J.; de Wilt, J.H.W.; Punt, C.J.A.; van Oijen, M.G.H.; Koopman, M. Significant increase of synchronous disease in first-line metastatic colorectal cancer trials: Results of a systematic review. Eur. J. Cancer 2016, 69, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Cirocchi, R.; Trastulli, S.; Abraha, I.; Vettoretto, N.; Boselli, C.; Montedori, A.; Parisi, A.; Noya, G.; Platell, C. Non-resection versus resection for an asymptomatic primary tumour in patients with unresectable stage IV colorectal cancer. Cochrane Database Syst. Rev. 2012, 8, CD008997. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Xia, Z.; Jia, X.; Chen, K.; Li, D.; Dai, Y.; Tao, M.; Mao, Y. Primary Tumor Resection Is Associated with Improved Survival in Stage IV Colorectal Cancer: An Instrumental Variable Analysis. Sci. Rep. 2015, 5, 16516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poultsides, G.A.; Servais, E.L.; Saltz, L.; Patil, S.; Kemeny, N.E.; Guillem, J.G.; Weiser, M.; Temple, L.K.; Wong, W.D.; Paty, P.B. Outcome of primary tumor in patients with synchronous stage IV colorectal cancer receiving combination chemotherapy without surgery as initial treatment. J. Clin. Oncol. 2009, 27, 3379–3384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakedis, J.; Schmidt, C.R. Surgical Treatment of Metastatic Colorectal Cancer. Surg. Oncol. Clin. N. Am. 2018, 27, 377–399. [Google Scholar] [CrossRef] [PubMed]
- Kanemitsu, Y.; Shitara, K.; Mizusawa, J.; Hamaguchi, T.; Shida, D.; Komori, K.; Ikeda, S.; Ojima, H.; Ike, H.; Shiomi, A.; et al. Primary Tumor Resection Plus Chemotherapy Versus Chemotherapy Alone for Colorectal Cancer Patients With Asymptomatic, Synchronous Unresectable Metastases (JCOG1007; iPACS): A Randomized Clinical Trial. J. Clin. Oncol. 2021, 39, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Cotte, E.; Villeneuve, L.; Passot, G.; Boschetti, G.; Bin-Dorel, S.; François, Y.; Glehen, O.; French Research Group of Rectal Cancer Surgery (GRECCAR). GRECCAR 8: Impact on survival of the primary tumor resection in rectal cancer with unresectable synchronous metastasis: A randomized multicentre study. BMC Cancer 2015, 15, 47. [Google Scholar] [CrossRef] [Green Version]
- ′t Lam-Boer, J.; Mol, L.; Verhoef, C.; De Haan, A.F.J.; Yilmaz, M.K.; Punt, C.J.A.; De Wilt, J.H.W.; Koopman, M. The CAIRO4 study: The role of surgery of the primary tumour with few or absent symptoms in patients with synchronous unresectable metastases of colorectal cancer--a randomized phase III study of the Dutch Colorectal Cancer Group (DCCG). BMC Cancer 2014, 14, 741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-C.; Ou, Y.-C.; Hu, W.-H.; Liu, C.-C.; Chen, H.-H. Meta-analysis of outcomes of patients with stage IV colorectal cancer managed with chemotherapy/radiochemotherapy with and without primary tumor resection. Onco Targets Ther. 2016, 9, 7059–7069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Hu, W.; Huang, C.; Liang, W.; Zhang, J.; Wu, D.; Lv, Z.; Li, Y.; Luo, Y.; Liang, Z.; et al. Survival outcome of palliative primary tumor resection for colorectal cancer patients with synchronous liver and/or lung metastases: A retrospective cohort study in the SEER database by propensity score matching analysis. Int. J. Surg. 2020, 80, 135–152. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Becerra, A.Z.; Fleming, F.J.; Aquina, C.T.; Dolan, J.G.; Monson, J.R.; Temple, L.K.; Jusko, T.A. Treatments for Stage IV Colon Cancer and Overall Survival. J. Surg. Res. 2019, 242, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Afshari, K.; Chabok, A.; Naredi, P.; Smedh, K.; Nikberg, M. Prognostic factors for survival in stage IV rectal cancer: A Swedish nationwide case-control study. Surg. Oncol. 2019, 29, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Ghiasloo, M.; Pavlenko, D.; Verhaeghe, M.; Van Langenhove, Z.; Uyttebroek, O.; Berardi, G.; Troisi, R.I.; Ceelen, W. Surgical treatment of stage IV colorectal cancer with synchronous liver metastases: A systematic review and network meta-analysis. Eur. J. Surg. Oncol. 2020, 46, 1203–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engstrand, J.; Strömberg, C.; Nilsson, H.; Freedman, J.; Jonas, E. Synchronous and metachronous liver metastases in patients with colorectal cancer-towards a clinically relevant definition. World J. Surg. Oncol. 2019, 17, 228. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group 1 | Group 2 | Group 3 | Group 4 | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No Treatment or Only RT | CT [+/− RT] | PTR [+/− RT | PTR + CT [+/− RT] | |||||||
| N = 650 | % | N = 768 | % | N = 423 | % | N = 1159 | % | N = 3000 | % | |
| Sex | ||||||||||
| Men | 302 | 46.46 | 460 | 59.90 | 216 | 51.06 | 677 | 58.41 | 1655 | 55.17 |
| Women | 348 | 53.54 | 308 | 40.10 | 207 | 48.94 | 482 | 41.59 | 1345 | 44.83 |
| Age group | ||||||||||
| <60 | 19 | 2.92 | 194 | 25.26 | 18 | 4.26 | 327 | 28.21 | 558 | 18.60 |
| 60–69 | 87 | 13.38 | 248 | 32.29 | 39 | 9.22 | 367 | 31.67 | 741 | 24.70 |
| 70–79 | 140 | 21.54 | 210 | 27.34 | 98 | 23.17 | 359 | 30.97 | 807 | 26.90 |
| >=80 | 404 | 62.15 | 116 | 15.10 | 268 | 63.36 | 106 | 9.15 | 894 | 29.80 |
| Year of diagnosis | ||||||||||
| 2006–2008 | 123 | 18.92 | 162 | 21.09 | 124 | 29.31 | 322 | 27.78 | 731 | 24.37 |
| 2009–2012 | 247 | 38.00 | 268 | 34.90 | 163 | 38.53 | 414 | 35.72 | 1092 | 36.23 |
| 2013–2016 | 280 | 43.08 | 338 | 44.01 | 136 | 32.15 | 423 | 36.50 | 1177 | 39.05 |
| Department | ||||||||||
| Calvados | 252 | 38.77 | 332 | 43.23 | 190 | 44.92 | 441 | 38.05 | 1215 | 40.50 |
| Finistere | 398 | 61.23 | 436 | 56.77 | 233 | 55.08 | 718 | 61.95 | 1785 | 59.50 |
| Charlson index | ||||||||||
| 0 | 90 | 13.85 | 206 | 26.82 | 83 | 19.62 | 306 | 26.40 | 685 | 22.83 |
| 1 or 2 | 135 | 20.77 | 256 | 33.33 | 90 | 21.28 | 369 | 31.84 | 850 | 28.33 |
| >2 | 357 | 54.92 | 232 | 30.21 | 231 | 54.61 | 390 | 33.65 | 1210 | 40.33 |
| missing | 68 | 10.46 | 74 | 9.64 | 19 | 4.49 | 94 | 8.11 | 255 | 8.50 |
| Localisation of primary tumora | ||||||||||
| colon | 491 | 75.54 | 472 | 61.46 | 381 | 90.07 | 937 | 80.85 | 2281 | 76.03 |
| rectum | 159 | 24.46 | 296 | 38.54 | 42 | 9.93 | 222 | 19.15 | 719 | 23.97 |
| Number of metastatic disease | ||||||||||
| multiple | 270 | 41.54 | 334 | 43.49 | 125 | 29.55 | 340 | 29.34 | 1069 | 35.63 |
| unique | 380 | 58.46 | 434 | 56.51 | 298 | 70.45 | 819 | 70.66 | 1931 | 64.37 |
| Metastatic disease | ||||||||||
| intra-abdominal | 415 | 63.85 | 476 | 61.98 | 322 | 76.12 | 860 | 74.20 | 2073 | 69.10 |
| intra-thoracic | 36 | 5.54 | 35 | 4.56 | 26 | 6.15 | 63 | 5.44 | 160 | 5.33 |
| thoraco-abdominal | 180 | 27.69 | 234 | 30.47 | 60 | 14.18 | 214 | 18.46 | 688 | 22.93 |
| others b | 11 | 1.69 | 12 | 1.56 | 3 | 0.71 | 2 | 0.17 | 79 | 2.63 |
| Multidisciplinary consultation | ||||||||||
| yes | 326 | 50.15 | 711 | 92.58 | 299 | 70.69 | 1079 | 93.10 | 2415 | 80.50 |
| no | 163 | 25.08 | 25 | 3.26 | 61 | 14.42 | 22 | 1.90 | 271 | 9.03 |
| missing | 161 | 24.77 | 32 | 4.17 | 63 | 14.89 | 58 | 5.00 | 314 | 10.47 |
| Type of surgery | ||||||||||
| colectomy | 0 | 0.00 | 0 | 0.00 | 360 | 85.11 | 850 | 73.34 | 1210 | 40.33 |
| protectomy | 0 | 0.00 | 0 | 0.00 | 56 | 13.24 | 298 | 25.71 | 354 | 11.80 |
| internal by-pass | 21 | 3.23 | 13 | 1.69 | 0 | 0.00 | 0 | 0.00 | 34 | 1.13 |
| permanent stoma | 117 | 18.00 | 155 | 20.18 | 0 | 0.00 | 0 | 0.00 | 272 | 9.07 |
| exploratory laparotomy | 32 | 4.92 | 80 | 10.42 | 0 | 0.00 | 0 | 0.00 | 112 | 3.73 |
| metastasectomy | 1 | 0.15 | 6 | 0.78 | 0 | 0.00 | 0 | 0.00 | 7 | 0.23 |
| others resections | 0 | 0.00 | 0 | 0.00 | 4 | 0.95 | 11 | 0.95 | 15 | 0.50 |
| no surgery | 479 | 73.69 | 514 | 66.93 | 0 | 0.00 | 0 | 0.00 | 993 | 33.10 |
| unknown | 0 | 0.00 | 0 | 0.00 | 3 | 0.71 | 0 | 0.00 | 3 | 0.10 |
| Complicated primary tumor | ||||||||||
| yes | 97 | 14.92 | 69 | 8.98 | 132 | 31.21 | 200 | 17.26 | 498 | 13.90 |
| no | 553 | 85.08 | 699 | 91.02 | 291 | 68.79 | 959 | 82.74 | 2502 | 86.10 |
| EDI quintile group | ||||||||||
| 1-2 | 298 | 45.85 | 369 | 48.05 | 163 | 38.53 | 573 | 49.44 | 1403 | 46.77 |
| 3-4-5 | 346 | 53.23 | 395 | 51.43 | 259 | 61.23 | 582 | 50.22 | 1582 | 52.73 |
| missing | 6 | 0.92 | 4 | 0.52 | 1 | 0.24 | 4 | 0.35 | 15 | 0.50 |
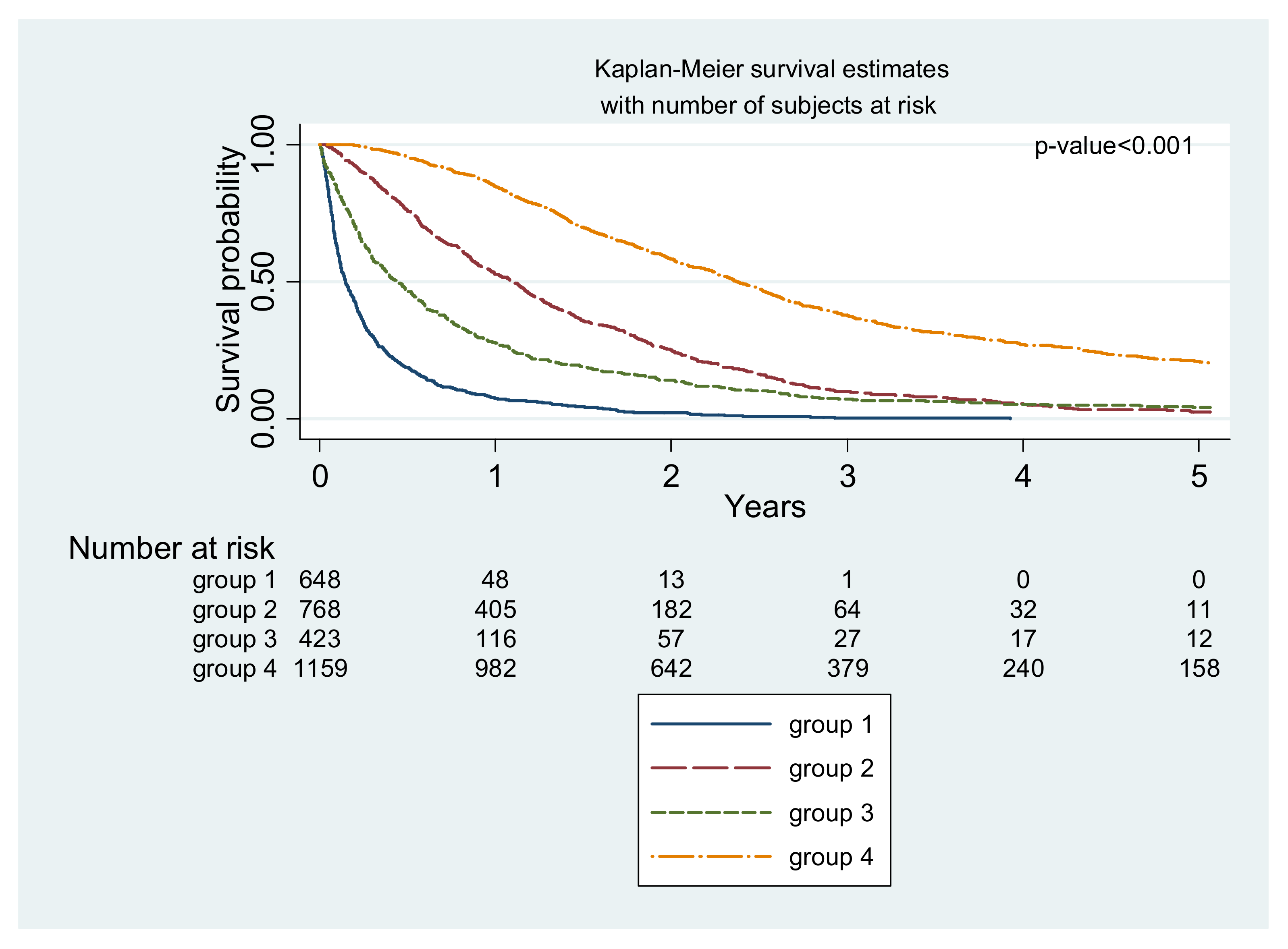
| Survival (95% CI) | ||||||||||
| 1-year | 7.41 (5.60 to 9.60) | 52.83 (49.23 to 56.29) | 27.55 (23.37 to 31.87) | 84.83 (82.53 to 86.68) | 51.80 (50.00 to 53.60) | |||||
| 5-year | -c | 2.42 (1.37 to 3.96) | 4.12 (2.41 to 6.51) | 21.01 (18.50 to 23.65) | 9.40 (8.30 to 10.60) | |||||
| M0 | M1 | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Treatment first | ||||||
| PTR | 1 | Ref | 0.50 | 1 | Ref | 0.55 |
| CT | 0.95 | 0.80 to 1.11 | 1.05 | 0.88 to 1.24 | ||
| Sex | ||||||
| Men | 1 | Ref | 0.36 | |||
| Women | 1.07 | 0.93 to 1.22 | ||||
| Age (years) | ||||||
| <60 | 1 | Ref | 0.001 | 1 | Ref | 0.001 |
| 60–69 | 1.12 | 0.93 to 1.34 | 1.09 | 0.91 to 1.32 | ||
| 70–79 | 1.66 | 1.39 to 1.98 | 1.47 | 1.21 to 1.79 | ||
| >=80 | 2.37 | 1.86 to 3.00 | 2.05 | 1.58 to 2.66 | ||
| Year of diagnosis | ||||||
| 2006–2008 | 1 | Ref | 0.03 | 1 | Ref | 0.09 |
| 2009–2012 | 0.85 | 0.73 to 1.00 | 0.88 | 0.75 to 1.03 | ||
| 2013–2016 | 0.81 | 0.68 to 0.96 | 0.83 | 0.70 to 0.99 | ||
| Departement | ||||||
| Calvados | 1 | Ref | 0.28 | |||
| Finistere | 1.08 | 0.94 to 1.24 | ||||
| Charlson comorbidity index | ||||||
| 0 | 1 | Ref | 0.001 | 1 | Ref | 0.01 |
| 1 ou 2 | 0.99 | 0.83 to 1.18 | 1.03 | 0.86 to 1.15 | ||
| >2 | 1.56 | 1.32 to 1.85 | 1.30 | 1.08 to 1.57 | ||
| Localisation of primary tumor | ||||||
| colic | 1 | Ref | 0.48 | |||
| rectal | 0.94 | 0.79 to 1.11 | ||||
| Localisation of metastatic disease | ||||||
| intra-abdominal | 1 | Ref | 0.001 | 1 | Ref | 0.001 |
| intra-thoracic | 0.99 | 0.73 to 1.33 | 0.90 | 0.67 to 1.22 | ||
| thoraco-abdominal | 1.56 | 1.32 to 1.84 | 1.53 | 1.30 to 1.80 | ||
| Number of metastatic site | ||||||
| unique | 1 | Ref | 0.01 | |||
| multiple | 0.51 | 0.45 to 0.59 | ||||
| EDI quintile | ||||||
| 1, 2 | 1 | Ref | 0.92 | |||
| 3, 4, 5 | 1.00 | 0.88 to 1.15 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mulliri, A.; Gardy, J.; Cariou, M.; Launoy, G.; Robaszkiewicz, M.; Alves, A.; Bouvier, V.; Dejardin, O. Care Management and Survival of Patients Diagnosed with Synchronous Metastatic Colorectal Cancer: A High-Resolution Population-Based Study in Two French Areas. Cancers 2022, 14, 1777. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14071777
Mulliri A, Gardy J, Cariou M, Launoy G, Robaszkiewicz M, Alves A, Bouvier V, Dejardin O. Care Management and Survival of Patients Diagnosed with Synchronous Metastatic Colorectal Cancer: A High-Resolution Population-Based Study in Two French Areas. Cancers. 2022; 14(7):1777. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14071777
Chicago/Turabian StyleMulliri, Andrea, Joséphine Gardy, Mélanie Cariou, Guy Launoy, Michel Robaszkiewicz, Arnaud Alves, Véronique Bouvier, and Olivier Dejardin. 2022. "Care Management and Survival of Patients Diagnosed with Synchronous Metastatic Colorectal Cancer: A High-Resolution Population-Based Study in Two French Areas" Cancers 14, no. 7: 1777. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14071777