
Treatment of Neuropathic Pain Directly Due to Cancer: An Update


1
Palliative Care, Pain Therapy and Rehabilitation Unit, Fondazione IRCCS Istituto Nazionale dei Tumori, 20133 Milano, Italy
2
Institute of Clinical Medicine, University of Oslo, 0318 Oslo, Norway
3
Department of Clinical Sciences and Community Health, Università degli Studi di Milano, 20122 Milano, Italy
*
Author to whom correspondence should be addressed.
Cancers 2022, 14(8), 1992; https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14081992
Submission received: 28 February 2022
/
Revised: 10 April 2022
/
Accepted: 12 April 2022
/
Published: 14 April 2022
(This article belongs to the Special Issue Palliative and Supportive Care in Oncology: An Update)
Abstract
:Simple Summary
This review discusses treatment approaches for providing pain relief to oncological patients affected by pain caused by nerve damage due to the tumor, also known as neuropathic cancer pain. Although being encountered often and causing a relevant burden to these patients, neuropathic cancer pain remains still difficult to diagnose and treat. Strong evidence about the best drugs to be used remain limited, as do therapeutic choices.
Abstract
Neuropathic pain can be defined as pain related to abnormal somatosensory processing in either the peripheral or central nervous system. In this review article, with neuropathic cancer pain (NCP), we refer to pain due to nervous tissue lesions caused by the tumor or its metastases. Nervous tissue damage is the cause of cancer pain in approximately 40% of those experiencing cancer pain. Recognizing a neuropathic pathophysiology in these cases may be difficult and requires specific criteria that are not homogenously applied in clinical practice. The management of this type of pain can be challenging, requiring the use of specific non-opioid adjuvant drugs. The majority of the criteria for NCP diagnosis and management have been based mainly on results from the noncancer population, risking the failure of addressing the specific needs of this population of patients. In this review, we summarize current management options available for NCP and provide some insights on new promising treatments.
1. Introduction
Neuropathic pain is defined by the International Association for the Study of Pain (IASP) Special Interest Group on Neuropathic Pain (NeuPSIG) as “pain arising as a direct consequence of a lesion or disease affecting the somatosensory system” [1].
There are many causes of neuropathic pain, through peripheral nerve lesions or brain and spinal cord lesions. The most common pathophysiological characteristic of pain due to neurological lesions is that the lesion affects the somatosensory pathways specifically involving the nociceptive fibers and their peripheral and central connectivity. Neuropathic pain in oncological patients can be caused by either the nerve damage from the cancer mass-effect and/or treatments including chemotherapy, radiotherapy, and surgery. However, in this article we refer to neuropathic cancer pain (NCP) as pain caused by the primary tumor or its metastases damaging or injuring the peripheral or central nervous system [2]. While the prevalence of pain due to neurological lesions in patients with advanced cancer can reach 40%, the neuropathic pathophysiology contributing to the individual pain experience is often unclear or at least not homogenously assessed according to individual clinical practices [3]. The local tumor’s direct effects and associated inflammatory processes are however always producing significant nociceptive mechanisms, which are often accounted for by considering a mixed, both nociceptive and neuropathic, pathophysiology in most cases of NCP pain [4,5].
The evaluation of the presence of NCP is relevant, since both its clinical characteristics and management are considered to differ from purely nociceptive and chronic neuropathic non-cancer pain [6]. These differences are partly related to the fact that NCP is often accompanied by a relevant nociceptive component but also to the fragility of oncological patients and the effect size of antalgic drugs used [7]. Clinically, neuropathic pain may be characterized by the presence of positive or negative sensory phenomena. NCP management is considered complex and often does not respond to opioid monotherapy, commonly requiring the use of adjuvant drugs such as antidepressants and anticonvulsants [8]. Due to its complexity, poor outcomes, and limited treatment options, NCP can become a relevant burden for patients, considerably impacting their quality of life [9].
Overall, there is little good clinical trial data on the use of adjuvant drugs and treatment approaches for NCP. This is, in part, related to the unique characteristics of these patients. The complexity and heterogeneity of pain characteristics, including the different clinical presentations of disease progression and the need for concomitant antineoplastic treatments, all can contribute to the difficulties of performing trials under stable experimental conditions. Additionally, relevant ethical concerns related to characteristics such as frailty require an accuracy in choosing the most appropriate designs and methodologies that take into account these specific characteristics. Existing treatment guidelines are highly dependent on trials in patients without cancer [10], failing often to address important issues such as side effects and the altered kinetics of these drugs in oncological patients [7]. Additionally, choice of treatments is often guided also by the coexistence of additional symptoms [9].
Despite challenges, progress in the understanding of the pathophysiology of neuropathic pain is spurring the development of new diagnostic procedures and personalized interventions, which emphasize the need for a multidisciplinary approach to the management of NCP. In this review article, we provide the state of the art in NCP treatment and novel promising therapeutic approaches developed.
2. General Principles
Opioid therapy is the first-line approach for moderate or severe chronic pain due to advanced cancer [11]. In some cases, however, additional analgesic interventions are considered [12]. In particular, it has been observed that NCP is associated with poorer outcomes when treated with only opioid analgesics [13], and analgesia can be improved by combining opioids with the so-called adjuvant medications [14]. Adjuvant analgesics commonly prescribed for NCP are the same as those used for chronic neuropathic pain of other causes [15].
Appropriate pain assessment is a key component for providing appropriate pain management [16]. Considering its heterogeneous characteristics, NCP diagnosis is not straightforward in most cases, and, to date, there is no accepted standardized gold standard for its assessment [4]. A grading system has been proposed by the Neuropathic Pain Special Interest Group (NeuPSIG) of the International Association for the Study of Pain (IASP), which can help identify probable or definite neuropathic pain in general [17]. The grading system is based on four criteria, as follows:
- Criterion 1: neuroanatomical plausible pain distribution;
- Criterion 2: suggestive history of a relevant neurological lesion or disease;
- Criterion 3: negative or positive sensory signs within innervation territory of the lesion;
- Criterion 4: confirmation of the lesion by a diagnostic test.
A probable diagnosis of neuropathic pain can be made if criteria 1, 2, and 3 or criteria 1, 2, and 4 are present. A definite neuropathic pain diagnosis is based on the presence of all four criteria. Yet, these criteria were not developed and validated for oncological patients; this is why in 2014, these criteria were revised and adapted for these patients, leading to the proposal of the EAPC/IASP algorithm for diagnostic criteria of NCP, which still needs validation [18].
Based on the association between pain characteristics, signs, and symptoms of the underlying lesion, NCP can be subdivided into specific pain syndromes according to the type of neurological involvement, including plexopathy, radiculopathy, and peripheral neuropathies, among other categories [19] (Table 1). Peripheral neurological lesions caused by the tumor are relatively frequent, while it is rare that neurological lesions due to cancer to the CNS cause pain, albeit in some cases of spinal cord lesions. The correct identification of the presence of NCP and its specific etiology can guide therapeutic decision making. For example, pain syndromes associated with focal, local, or regional pain can benefit from the application of topical treatments.
The diagnosis of a neuropathic component in the pathophysiology of pain should be made when cancer is causing a neurological lesion, and the pain is referred to the area of the neurological lesion of interest. Neurological negative signs and loss of motor function can confirm the presence of a neurological dysfunction, and pain can or cannot be associated with positive neurological signs of hyperexcitability, such as allodynia and hyperalgesia, that are typical of neuropathic pain. Sometimes, other symptoms, such as dysesthesia, paresthesia, burning or lancinating pain episodes, are also present and considered characteristic of NCP.
However, not all these clinical findings have been valued for establishing a diagnosis of neuropathic pain, especially in patients with cancer. Some screening questionnaires such as the DN4 (Douleur Neuropathique 4 Questions) [20], LANSS [21] (Leeds assessment of neuropathic symptoms and signs), and painDETECT [22] have been developed to identify the clinical characteristics of neuropathic pain and can be applied also to patients with cancer [5], but a homogenous and standardized method to combine clinical diagnosis and questionnaires results is still lacking. As a conclusion, the presence of a neurological lesion with signs and symptoms characteristic of neuropathic pain should be required for diagnosing NCP [23].
3. Pharmacological Management of NCP
Tricyclic antidepressants (TCAs), serotonin and norepinephrine reuptake inhibitors (SNRIs), and anticonvulsant drugs are effective in the management of neuropathic pain in general [24], and though data regarding their efficacy in NCP are scarce, they remain some of the main drugs used in these patients [25,26]. These drugs are commonly used in combination with non-opioid and opioid analgesics for NCP [26]. Due to the heterogeneity of patients and pain presentations, high-quality evidence to support the use of specific drugs for NCP is lacking; however, below we provide a list of some of the main drugs used for the pharmacological management of NCP.
3.1. Antidepressants
TCAs and SNRIs are commonly used for the treatment of NCP [26,27,28]. TCAs include drugs such as amitriptyline, nortriptyline, and desipramine; while SNRIs, which are often used for NCP, include venlafaxine and duloxetine [29]. The analgesic effect of antidepressants is independent of the antidepressant effect, and they exert this effect by reinforcing the descending inhibitory pathways, increasing the release of norepinephrine and serotonin in the synaptic cleft at both supraspinal and spinal levels [30]. A systematic review and meta-analysis on the effectiveness of antidepressants for NCP indicated that various trials reported a better response of combination therapy with antidepressants compared with treatments without antidepressants [8]. The absolute risk benefit (ARB) of antidepressants estimated in a review article based on five RCTs, three of which studied amitriptyline, was 0.55, and the absolute risk harm was0.13 [31].
SNRIs, mainly duloxetine, have been mostly studied and recommended for the treatment of chemotherapy-induced peripheral neuropathies [32]. However, a few recent studies have demonstrated that adding duloxetine to opioid or opioid–pregabalin therapy might be beneficial in patients with refractory NCP [33,34]. Additionally, a recent multicenter, randomized placebo-controlled trial performed at 12 specialized palliative care services in Japan, suggested that adding duloxetine to opioid–pregabalin therapy might have clinical benefit in alleviating refractory NCP [35]. Further studies are needed to conclude the efficacy of duloxetine in these cases.
Antidepressants can be helpful also in managing depression and anxiety accompanying chronic cancer pain. Yet, the potential benefits and risks should be well weighed before prescription. Drug toxicity can be dose-limiting for TCA, in particular, due to the anticholinergic effects. Common side effects of SNRIs include somnolence, dry mouth, dizziness, and increased sweating.
3.2. Anticonvulsants
Neuronal hyperexcitability plays a relevant role in the pathophysiology of neuropathic pain. Gabapentinoids reduce pain transmission in the spinal pathways and also modulate the central descending inhibitory pathways and have, therefore, been widely used for the treatment of neuropathic pain [36]. In the systematic review of Jongen et al. [31], the ARB of the anticonvulsants was 0.57, and the ARH was 0.005. Gabapentin and pregabalin are two of the most frequently used drugs of this class for treating NCP. Both drugs have established efficacy for treating neuropathic pain and are also recommended as first line treatment for NCP [11,26]. In general, both gabapentin and pregabalin, can be effectively combined with opioids for this purpose. Somnolence and dizziness are the most frequent dose-limiting side effects. Although a few RCTs have shown the efficacy of these drugs when used for NCP [23,37,38], more data are needed on efficacy and safety outcomes in patients with NCP [39]. An open-label randomized study has investigated the use of pregabalin over fentanyl in patients with moderate-to-severe NCP, showing some benefit and suggesting that pregabalin monotherapy in NCP may lead to better control of the neuropathic component, with opioid-sparing effects [40]. Other antiepileptics include lamotrigine and second-generation anticonvulsants, carbamazepine and oxcarbazepine, which are however less commonly used for NCP [41,42,43,44].
3.3. Opioids
Since the publication of the World Health Organization (WHO) analgesic ladder in 1986 [45], opioids have remained the mainstay therapy in cancer patients experiencing moderate to severe pain [11]. Considering the particular nature of cancer pain, the presence of a nociceptive component is very common, also in patients with NCP, making it difficult to objectively determine the effect of the analgesics on the neuropathic component. [46]. For this reason, control of NCP usually requires the concurrent use of opioids and adjuvant analgesics specific for NCP [26,47]. A systematic review and meta-analysis on the combined use of opioids with antidepressants or anticonvulsants indicated a nonsignificant improvement of pain relief in patients with NCP compared with opioid monotherapy, but the heterogeneity of the pain conditions in the studies did not allow the formulation of firm conclusions [48]. A balance should always be made between the benefits in terms of pain intensity improvement and the increased risk of adverse effects due to the combination therapy in these patients.
Strong opioids, including drugs such as morphine, oxycodone, methadone, and fentanyl, are used in moderate or severe cancer pain but also NCP and neuropathic pain from other chronic nonmalignant conditions [49]. Methadone is a synthetic opioid-receptor agonist and N-methyl-D-aspartate (NMDA) inhibitor [50]. A recent prospective cohort pilot study on patients with NCP indicated that methadone could significantly improve neuropathic pain through a targeted effect on allodynia and the pressure/squeezing component [51]. Due to its unpredictable very long half-life and risk of accumulation and toxicity, its use should be reserved to experienced clinicians [11,26].
Regarding drugs used for moderate-intensity pain, tramadol deserves some attention, since it is a centrally acting drug, with both opioid activity and monoaminergic properties, and has been used in the treatment of neuropathic pain [52]. A double-blind placebo-controlled study on patients with NCP has shown that tramadol was significantly more effective than the placebo in improving pain intensity and quality of life, decreasing the use of antiepileptic analgesics [53]. However, to date, there is still only modest evidence about the effectiveness of tramadol in NCP [54]. Tapentadol is a dual-acting μ-opioid receptor agonist and noradrenaline reuptake inhibitor, and its use has been suggested also for NCP, especially for cases in which an immediate dose adjustment is required or in patients at high risk for adverse effects [55,56].
Sometimes, the type of opioid or the route of its administration needs to be changed, either due to the presence of significant side effects or lack of response. This may be the case also for patients affected with NCP. The substitution of one opioid with another is also known as opioid switching or rotation [57] and has been found to improve opioid responsiveness [58]. The existence of an incomplete cross-tolerance among opioid agonists, genetic polymorphisms, and interindividual variations can partly explain the clinical improvement obtained in these cases [59]. The achievement of satisfactory pain control and decrease in adverse effects intensity after opioid rotation has been reported in around 50–90% of patients [60]. Particularly, methadone has been shown to improve pain control and reduce opioid toxicity in cancer patients who are receiving treatment with high doses of other opioids and in cases of NCP presence [61]. Opioid switching requires, however, clinical experience and adequate monitoring, especially in patients receiving high dosages. Further research is needed to improve the knowledge about the conversion ratios in the different clinical situations.
3.4. Local Anesthetics
Topical lidocaine is a local anesthetic used also for cancer related pain. A topical lidocaine 5% patch has been shown to effectively treat postherpetic neuralgia and other localized neuropathic pain associated with the presence of allodynia [62,63,64,65]. A prospective nonrandomized open-label study of patients with pain post-thoracotomy and post-mastectomy or pain caused by chest wall tumors demonstrated that the addition of lidocaine 5% patches was effective in the short term for the treatment of neuropathic pain accompanied by allodynia, whether deriving from a painful scar or chest wall tumor [66]. However, these findings need to be confirmed by randomized controlled trials with larger samples and specific for NCP only. Additionally, it should be kept in mind that lidocaine is effective only for well localized pain, which is not common. Though systemic absorption of topical lidocaine is minimal, it should not be used in patients on class I antiarrhythmics [41].
3.5. NMDA Antagonists
NMDA is a receptor for the excitatory neurotransmitter glutamate, which is released with noxious peripheral stimuli. The activation of these receptors has been associated with hyperalgesia, neuropathic pain, and reduced functionality of opioid receptors [67]. Therefore, NMDA antagonists could play a role in the management of neuropathic pain. There are several NMDA receptor antagonists available, including ketamine and methadone. They each differ in their level of activity on the NMDA receptor. Ketamine is a strong NMDA antagonist, usually less tolerated than the other antagonists due to a higher incidence of side effects, in particular hallucinations and a dissociative mental state [68]. Although ketamine has been used as an adjuvant drug in challenging cancer pain [69], recent trials have failed to indicate any benefit from the use of the drug in treating NCP [70,71]. There are currently not enough data to recommend the use of ketamine for NCP, but it has been hypothesized that some subgroups of patients, such as those with central sensitization, could benefit from the use of this drug [71].
3.6. Cannabis
The endocannabinoid system is involved in many physiological functions and homeostasis. Cannabinoid receptors are expressed in the peripheral and central nervous system and on immune cells, therefore being potential targets for the modulation of pain processing. Cannabis is, in general, seen as an alternative to conventional treatment when patients do not respond or have severe side effects. Some evidence suggests that medical cannabis has the potential to effectively manage pain in cancer pain patients, and preclinical data in NCP models have suggested a potential analgesic role for cannabinoids [72,73]. However, although there are some positive results in pain of cancer patients, the clinical evidence for cannabinoids as analgesics is not yet demonstrated, and their use can only be weakly recommended [74]. A recent systematic review and meta-analysis to analyze the effects on pain and adverse effects of cannabinoids compared with a placebo or other active agents for the treatment of cancer-related pain showed that the addition of cannabinoids to opioids did not reduce cancer pain [75]. The efficacy of cannabinoids remains to be elucidated [76].
3.7. Interventional Treatment Options
Uncontrolled NCP can sometimes require the use of interventional analgesic techniques. Neuraxial analgesia consists in the delivery of local anesthetics, opioids, or coanalgesics into the epidural or intrathecal (spinal) space [77]. Intrathecal administration of morphine and other drugs such as bupivacaine or clonidine may provide better pain relief [78,79]. Clonidine is an alpha2-adrenergic agonist and has been approved for interventional administration in the treatment of neuropathic cancer pain [80]. Intrathecal ziconotide, a neuron-specific calcium channel blocker, is also an approved analgesic, which has been shown to provide pain intensity reduction in RCTs in noncancer and cancer pain patients [81,82]. Yet, these techniques require specialized equipment and a pain specialist, and although generally safe, they can be accompanied by relevant side effects [77]. The role of nerve blocks and neurolytic procedure in NCP is poorly documented.
3.8. Proposed Treatment Algorithm
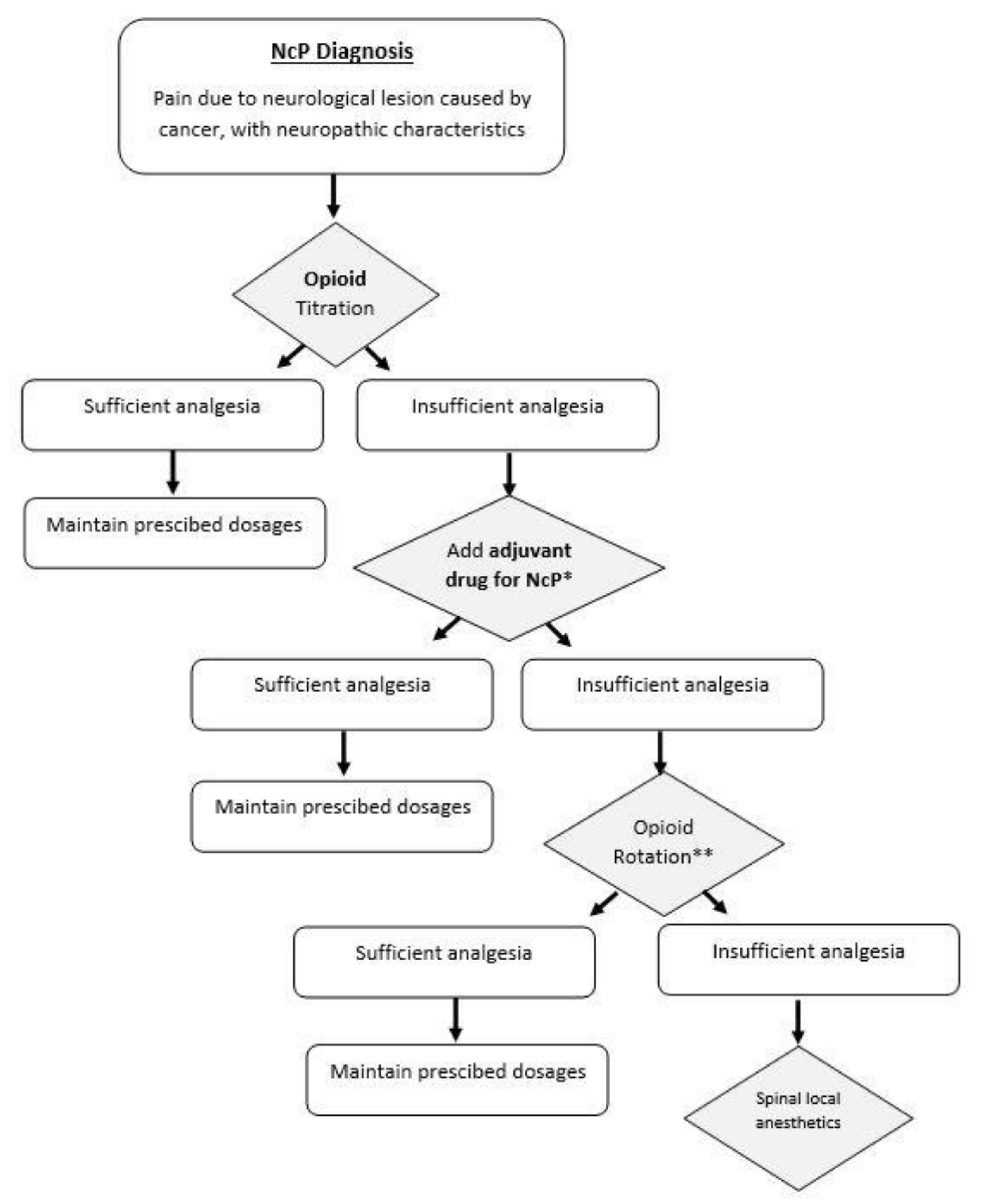
The pharmacological strategy for NCP treatment when analgesia is not satisfactory with the use of opioid medications is only weakly supported by clinical trials, and robust evidence is lacking. Most available studies have low quality of evidence often with unclear randomization procedures and heterogeneity, which make the pooling of the results not possible [83]. Based on the existing guidelines, but also on clinical experience, in our clinical practice the first step in for an appropriate management of NCP is the correct identification of this pain type, according to the pre-existing mentioned criteria [17]. After diagnosis of NCP, titration of monotherapy with opioids is attempted and maintained if it provides sufficient analgesia. In the case of insufficient analgesia and the coexistence of sensory symptoms, adjuvant drugs for NCP can be prescribed. Current evidence suggests benefits mainly using adjuvant drugs such as gabapentinoids, mainly gabapentin and pregabalin, and antidepressants such as amitriptyline [23,38]. The combination therapy is maintained if it provides adequate analgesia; otherwise, opioid rotation can be attempted. Methadone is usually the drug of choice although requiring cautions about its titration and dose conversion [60]. If pain persists, additional pain management approaches can be implemented, such as local spinal anesthetics. These steps have been summarized in Figure 1.
4. Novel Therapeutic Agents
Thanks to preclinical research studies, several advances have been made in better understanding the pathophysiology and neurobiology of pain in general. We provide here a summary of these findings and the drugs recently included in clinical practice or currently under investigation, for which positive effects in NCP treatment have been suggested either clinically or preclinically.
4.1. Tetrodotoxin
Tetrodotoxin (TTX) is a potent neurotoxin found mainly in puffer fish and other animals. It blocks voltage-gated sodium channels playing a key role in pain signaling [84]. During pathological pain conditions, such as neuropathic pain, upregulation of some TTX-sensitive voltage-gated sodium channels contribute to painful hypersensitization [85]. TTX displays a prominent analgesic effect in several models of neuropathic pain in rodents but is almost unexplored in preclinical models of pain induced by cancer, with only one article evaluating the role of TTX in bone cancer pain [86]. Using an in vivo behavioral test, they found that blockade of the dorsal root ganglion (DRG) neuron activity by intrathecal injection of TTX (10 μg/kg, once a day) inhibited the tumor-evoked mechanical allodynia and thermal hyperalgesia in bone cancer in rats. TTX has been tested in several clinical trials, including phase II and phase III trials. These studies have indicated promising results in terms of both the safety and efficacy of TTX in relieving pain associated with cancer [87]. A Phase IIa open-label study found that the 30 μg b.i.d. dose of TTX administered intramuscularly for 4 days appeared to be safe and efficacious in cancer patients whose pain was not relieved with standard therapy [88]. The role of TTX in cancer-related pain has been subsequently assessed in a larger Phase II randomized, multicenter, double-blind, placebo-controlled trial, which showed a statistically nonsignificant trend toward more responders in the active treatment arm based on pain intensity difference. A recent multicenter, randomized, double-blind, placebo-controlled, parallel-design trial on TTX (30 μg) given subcutaneously twice daily for four days, suggested a favorable benefit-risk profile and clinically important analgesic effect (Number Needed to Treat about 4–6) in the treatment of uncontrolled moderate to severe cancer-related pain [89]. However, this trial was underpowered, and more studies are needed to replicate and confirm the previous findings.
4.2. Botulinum Toxin Type A (BoNT-A)
BoNT-A is a potent neurotoxin produced by Clostridium botulinum, which mainly acts at the muscular level by inhibiting the release of acetylcholine at presynaptic levels, blocking the action potential in the neuromuscular junction [90]. In recent years, many experiments have been carried out in animal models but also on humans, investigating the role of BoNT-A in as an analgesic drug in both nociceptive and neuropathic cancer pain. Although its mechanism is not yet fully understood, evidence has shown that BoNT-A inhibits the secretion of pain mediators from the nerve endings and dorsal root ganglion, impacting directly on the nociceptive transmission through the anterolateral and trigeminothalamic systems [24,91].
4.3. TRPM8 Activator Menthol
Findings from basic science studies have shown upregulation of receptors for cooling in neuropathic pain models, indicating a role of cooling-induced analgesia as novel target for intervention [92,93]. Indeed, preclinical evidence has shown that the activation of the transient receptor potential melastatin 8 (TRPM8) ion channel, by topical agents, produces significant analgesia [94]. Clinical evidence also suggests that topical menthol, a TRPM8 activator, has potential as a novel analgesic therapy for localized cancer-related neuropathic pain, improving patient-rated measures [95].
4.4. Growth Factors Inhibitors
Growth factors, such as nerve growth factor, brain-derived neurotrophic factor, platelet-derived growth factor, insulin-like growth factor 1, and their respective receptors, have been identified as targets in the treatment of neuropathic pain [96]. Preliminary data have shown that Tanezumab, a monoclonal antibody against nerve growth factor can improve metastatic cancer-related bone pain [97,98]. However, its role in the management of NCP remains still to be elucidated. Recently, the epidermal growth factor receptor (EGFR) has also been identified as a potential therapeutic target. EGFR plays an important role in controlling functions such as growth, proliferation, metabolism, and survival, and, as such, its multifunctioning can drive tumorigenesis and tumor progression [99]. Anticancer drugs, which target EGFR, have been developed and are used for cancer treatment. However, recent studies and description of clinical cases have indicated that EGFR might be involved in pain and NCP pain treatment [100,101,102,103]. A recent proof-of-concept evaluation of an EGFR inhibitor used for neuropathic pain treatment did not provide statistical evidence of efficacy, although it demonstrated substantial reduction in pain [104]. These findings indicate that there might be a beneficial role of these drugs for NCP, which warrants further investigation.
4.5. Lemairamin
Lemairamin, isolated from the pericarps of the Zanthoxylum plants, is an agonist of α7 nicotinic acetylcholine receptors (α7nAChRs), which can reduce neuroinflammation in Alzheimer’s disease [105]. A recent study has evaluated its antinociceptive effects in pain hypersensitivity and explored the underlying mechanisms, showing that lemairamin could produce antinociception in pain hypersensitivity through the spinal IL-10/β-endorphin pathway following α7nAChR activation [106].
Other additional promising compounds can be found, which have shown some efficacy in pre-clinical studies and warrant further research. We might mention here drugs such as thalidomide targeting the IL-10/β-endorphin signaling pathway [107] or protopanaxadiol targeting the spinal microglial dynorphin A expression following glucocorticoid receptor activation [108].
5. Future Directions
There remain many challenges in the topic of NCP management, which open numerous opportunities for future clinical and preclinical research. Current guidelines on NCP are based on scarce evidence, which is often contradictory. It is clear that, in the future, more robust RCT are needed in order to obtain stronger evidence on existing recommendation. Good research is, however, largely based on good clinical practice and appropriate pain assessment; this is why, the identification of a gold standard for NCP diagnosis is imperative. Preclinical studies on the discovery of novel mechanisms and drugs are also needed. The very complex nature of cancer pain indicates that better insights are needed both regarding the neurobiology of pain in these patients and also on mechanisms and targeted therapies.
Author Contributions
Conceptualization, A.C. and M.S.; writing—original draft preparation, A.C. and M.S.; writing—review and editing, A.C. and M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received partial funding by the PAIN-Net project part of the EU Research Framework Programme H2020/Marie Skłodowska-Curie Actions, grant agreement number 721841.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jensen, T.S.; Baron, R.; Haanpaa, M.; Kalso, E.; Loeser, J.D.; Rice, A.S.C.; Treede, R.D. A New Definition of Neuropathic Pain. Pain 2011, 152, 2204–2205. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.I.; Kaasa, S.; Barke, A.; Korwisi, B.; Rief, W.; Treede, R.D.; IASP Taskforce for the Classification of Chronic Pain. The IASP Classification of Chronic Pain for ICD-11: Chronic Cancer-Related Pain. Pain 2019, 160, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.I.; Rayment, C.; Hjermstad, M.; Aass, N.; Caraceni, A.; Kaasa, S. Prevalence and Aetiology of Neuropathic Pain in Cancer Patients: A Systematic Review. Pain 2012, 153, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Shkodra, M.; Brunelli, C.; Zecca, E.; Formaglio, F.; Bracchi, P.; Lo Dico, S.; Caputo, M.; Kaasa, S.; Caraceni, A. Neuropathic Pain: Clinical Classification and Assessment in Patients with Pain due to Cancer. Pain 2021, 162, 866–874. [Google Scholar] [CrossRef] [PubMed]
- Mulvey, M.R.; Boland, E.G.; Bouhassira, D.; Freynhagen, R.; Hardy, J.; Hjermstad, M.J.; Mercadante, S.; Perez, C.; Bennett, M.I. Neuropathic Pain in Cancer: Systematic Review, Performance of Screening Tools and Analysis of Symptom Profiles. Br. J. Anaesth. 2017, 119, 765–774. [Google Scholar] [CrossRef] [Green Version]
- Fallon, M. Neuropathic Pain in Cancer. Br. J. Anaesth. 2013, 111, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Piano, V.; Verhagen, S.; Schalkwijk, A.; Hekster, Y.; Kress, H.; Lanteri-Minet, M.; Burgers, J.; Treede, R.; Engels, Y.; Vissers, K. Treatment for Neuropathic Pain in Patients with Cancer: Comparative Analysis of Recommendations in National Clinical Practice Guidelines from E Uropean Countries. Pain Pract. 2014, 14, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Guan, J.; Tanaka, S.; Kawakami, K. Anticonvulsants or Antidepressants in Combination Pharmacotherapy for Treatment of Neuropathic Pain in Cancer Patients: A Systematic Review and Meta-Analysis. Clin. J. Pain 2016, 32, 719–725. [Google Scholar] [CrossRef]
- Smith, B.H.; Torrance, N.; Bennett, M.I.; Lee, A.J. Health and Quality of Life Associated with Chronic Pain of Predominantly Neuropathic Origin in the Community. Clin. J. Pain 2007, 23, 143–149. [Google Scholar] [CrossRef]
- Davis, M.P. Cancer-Related Neuropathic Pain: Review and Selective Topics. Hematol./Oncol. Clin. 2018, 32, 417–431. [Google Scholar] [CrossRef]
- Caraceni, A.; Hanks, G.; Kaasa, S.; Bennett, M.I.; Brunelli, C.; Cherny, N.; Dale, O.; De Conno, F.; Fallon, M.; Hanna, M. Use of Opioid Analgesics in the Treatment of Cancer Pain: Evidence-Based Recommendations from the EAPC. Lancet Oncol. 2012, 13, e58–e68. [Google Scholar] [CrossRef]
- Lussier, D.; Huskey, A.G.; Portenoy, R.K. Adjuvant Analgesics in Cancer Pain Management. Oncologist 2004, 9, 571–591. [Google Scholar] [CrossRef]
- Cherny, N.I.; Thaler, H.T.; Friedlander-Klar, H.; Lapin, J.; Foley, K.M.; Houde, R.; Portenoy, R.K. Opioid Responsiveness of Cancer Pain Syndromes Caused by Neuropathic or Nociceptive Mechanisms: A Combined Analysis of Controlled, Single-Dose Studies. Neurology 1994, 44, 857–861. [Google Scholar] [CrossRef]
- Laird, B.; Colvin, L.; Fallon, M. Management of Cancer Pain: Basic Principles and Neuropathic Cancer Pain. Eur. J. Cancer 2008, 44, 1078–1082. [Google Scholar] [CrossRef]
- Swarm, R.; Paice, J.; Anghelescu, D.; Are, M.; Yang Bruce, J.; Buga, S.; Chwistek, M.; Cleeland, C.; Craig, D.; Gafford, E. NCCN Clinical Practice Guidelines in Oncology: Adult Cancer Pain (Version3. 2019). JNCCN 2019, 11, 992–1034. [Google Scholar] [CrossRef] [Green Version]
- Caraceni, A.; Shkodra, M. Cancer Pain Assessment and Classification. Cancers 2019, 11, 510. [Google Scholar] [CrossRef] [Green Version]
- Treede, R.D.; Jensen, T.S.; Campbell, J.N.; Cruccu, G.; Dostrovsky, J.O.; Griffin, J.W.; Hansson, P.; Hughes, R.; Nurmikko, T.; Serra, J. Neuropathic Pain: Redefinition and a Grading System for Clinical and Research Purposes. Neurology 2008, 70, 1630–1635. [Google Scholar] [CrossRef]
- Brunelli, C.; Bennett, M.I.; Kaasa, S.; Fainsinger, R.; Sjøgren, P.; Mercadante, S.; Løhre, E.T.; Caraceni, A.; European Association for Palliative Care (EAPC) Research Network. Classification of Neuropathic Pain in Cancer Patients: A Delphi Expert Survey Report and EAPC/IASP Proposal of an Algorithm for Diagnostic Criteria. Pain 2014, 155, 2707–2713. [Google Scholar] [CrossRef]
- Caraceni, A.; Portenoy, R.K. An International Survey of Cancer Pain Characteristics and Syndromes. Pain 1999, 82, 263–274. [Google Scholar] [CrossRef]
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brochet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A. Comparison of Pain Syndromes Associated with Nervous or Somatic Lesions and Development of a New Neuropathic Pain Diagnostic Questionnaire (DN4). Pain 2005, 114, 29–36. [Google Scholar] [CrossRef]
- Bennett, M. The LANSS Pain Scale: The Leeds Assessment of Neuropathic Symptoms and Signs. Pain 2001, 92, 147–157. [Google Scholar] [CrossRef]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tölle, T.R. Pain DETECT: A New Screening Questionnaire to Identify Neuropathic Components in Patients with Back Pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Caraceni, A.; Zecca, E.; Bonezzi, C.; Arcuri, E.; Tur, R.Y.; Maltoni, M.; Visentin, M.; Gorni, G.; Martini, C.; Tirelli, W. Gabapentin for Neuropathic Cancer Pain: A Randomized Controlled Trial from the Gabapentin Cancer Pain Study Group. J. Clin. Oncol. 2004, 22, 2909–2917. [Google Scholar] [CrossRef] [PubMed]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S. Pharmacotherapy for Neuropathic Pain in Adults: A Systematic Review and Meta-Analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Chapman, E.J.; Edwards, Z.; Boland, J.W.; Maddocks, M.; Fettes, L.; Malia, C.; Mulvey, M.R.; Bennett, M.I. Practice Review: Evidence-Based and Effective Management of Pain in Patients with Advanced Cancer. Palliat. Med. 2020, 34, 444–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallon, M.; Giusti, R.; Aielli, F.; Hoskin, P.; Rolke, R.; Sharma, M.; Ripamonti, C. Management of Cancer Pain in Adult Patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29, iv166–iv191. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.Y.; Oh, J. Neuropathic Cancer Pain: Prevalence, Pathophysiology, and Management. Korean J. Intern. Med. 2018, 33, 1058. [Google Scholar] [CrossRef]
- Attal, N.; Cruccu, G.; Baron, R.a.; Haanpää, M.; Hansson, P.; Jensen, T.; Nurmikko, T. EFNS Guidelines on the Pharmacological Treatment of Neuropathic Pain: 2010 Revision. Eur. J. Neurol. 2010, 17, 1113.e88. [Google Scholar] [CrossRef]
- Esin, E.; Yalcin, S. Neuropathic Cancer Pain: What we are Dealing with? how to Manage it? Onco Targets Ther. 2014, 7, 599–618. [Google Scholar]
- Dharmshaktu, P.; Tayal, V.; Kalra, B.S. Efficacy of Antidepressants as Analgesics: A Review. J. Clin. Pharmacol. 2012, 52, 6–17. [Google Scholar] [CrossRef]
- Jongen, J.L.; Huijsman, M.L.; Jessurun, J.; Ogenio, K.; Schipper, D.; Verkouteren, D.R.; Moorman, P.W.; van der Rijt, C.C.D.; Vissers, K.C. The Evidence for Pharmacologic Treatment of Neuropathic Cancer Pain: Beneficial and Adverse Effects. J. Pain Symptom Manag. 2013, 46, 581–590.e1. [Google Scholar] [CrossRef]
- Hershman, D.L.; Lacchetti, C.; Dworkin, R.H.; Lavoie Smith, E.M.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Gavin, P.; Lavino, A.; Lustberg, M.B. Prevention and Management of Chemotherapy-Induced Peripheral Neuropathy in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2014, 32, 1941–1967. [Google Scholar] [CrossRef] [Green Version]
- Curry, Z.A.; Dang, M.C.; Sima, A.P.; Abdullaziz, S.; Del Fabbro, E.G. Combination Therapy with Methadone and Duloxetine for Cancer-Related Pain: A Retrospective Study. Ann. Palliat. Med. 2021, 10, 2505–2511. [Google Scholar] [CrossRef]
- Matsuoka, H.; Makimura, C.; Koyama, A.; Otsuka, M.; Okamoto, W.; Fujisaka, Y.; Kaneda, H.; Tsurutani, J.; Nakagawa, K. Pilot Study of Duloxetine for Cancer Patients with Neuropathic Pain Non-Responsive to Pregabalin. Anticancer Res. 2012, 32, 1805–1809. [Google Scholar]
- Matsuoka, H.; Iwase, S.; Miyaji, T.; Kawaguchi, T.; Ariyoshi, K.; Oyamada, S.; Satomi, E.; Ishiki, H.; Hasuo, H.; Sakuma, H. Additive Duloxetine for Cancer-Related Neuropathic Pain Nonresponsive or Intolerant to Opioid-Pregabalin Therapy: A Randomized Controlled Trial (JORTC-PAL08). J. Pain Symptom Manag. 2019, 58, 645–653. [Google Scholar] [CrossRef] [Green Version]
- Jordan, R.I.; Mulvey, M.R.; Bennett, M.I. A Critical Appraisal of Gabapentinoids for Pain in Cancer Patients. Curr. Opin. Supportive Palliat. Care 2018, 12, 108–117. [Google Scholar] [CrossRef]
- Keskinbora, K.; Pekel, A.F.; Aydinli, I. Gabapentin and an Opioid Combination Versus Opioid Alone for the Management of Neuropathic Cancer Pain: A Randomized Open Trial. J. Pain Symptom Manag. 2007, 34, 183–189. [Google Scholar] [CrossRef]
- Mishra, S.; Bhatnagar, S.; Goyal, G.N.; Rana, S.P.S.; Upadhya, S.P. A Comparative Efficacy of Amitriptyline, Gabapentin, and Pregabalin in Neuropathic Cancer Pain: A Prospective Randomized Double-Blind Placebo-Controlled Study. Am. J. Hosp. Palliat. Med. 2012, 29, 177–182. [Google Scholar] [CrossRef]
- Bennett, M.I.; Laird, B.; van Litsenburg, C.; Nimour, M. Pregabalin for the Management of Neuropathic Pain in Adults with Cancer: A Systematic Review of the Literature. Pain Med. 2013, 14, 1681–1688. [Google Scholar] [CrossRef] [Green Version]
- Raptis, E.; Vadalouca, A.; Stavropoulou, E.; Argyra, E.; Melemeni, A.; Siafaka, I. Pregabalin vs. Opioids for the Treatment of Neuropathic Cancer Pain: A Prospective, Head-to-head, Randomized, Open-label Study. Pain Pract. 2014, 14, 32–42. [Google Scholar] [CrossRef]
- Glasser, M.; Chen, J.; Alzarah, M.; Wallace, M. Non-opioid Analgesics and Emerging Therapies. In Fundamentals of Cancer Pain Management; Anonymous, Ed.; Springer: Berlin/Heidelberg, Germany, 2021; pp. 125–142. [Google Scholar]
- Vecht, C.J.; Hoff, A.M.; Kansen, P.J.; De Boer, M.F.; Andries Bosch, D. Types and Causes of Pain in Cancer of the Head and Neck. Cancer 1992, 70, 178–184. [Google Scholar] [CrossRef] [Green Version]
- Wiffen, P.J.; Derry, S.; Moore, R.A.; McQuay, H.J. Carbamazepine for Acute and Chronic Pain in Adults. Cochrane Database Syst. Rev. 2011, 1, CD005451. [Google Scholar] [CrossRef] [Green Version]
- Wiffen, P.J.; Derry, S.; Moore, R.A. Lamotrigine for Chronic Neuropathic Pain and Fibromyalgia in Adults. Cochrane Database Syst. Rev. 2013, 2013, CD006044. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Staff; World Health Organization. Cancer Pain Relief: With a Guide to Opioid Availability; World Health Organization: Geneva, Switzerland, 1996. [Google Scholar]
- Bechakra, M.; Moerdijk, F.; van Rosmalen, J.; Koch, B.C.; van der Rijt, C.C.D.; Smitt, P.A.S.; Jongen, J.L. Opioid Responsiveness of Nociceptive Versus Mixed Pain in Clinical Cancer Patients. Eur. J. Cancer 2018, 105, 79–87. [Google Scholar] [CrossRef]
- Madden, K.; Haider, A.; Rozman De Moraes, A.; Naqvi, S.M.; Enriquez, P.A.; Wu, J.; Williams, J.; Liu, D.; Bruera, E. Frequency of Concomitant use of Gabapentinoids and Opioids among Patients with Cancer-Related Pain at an Outpatient Palliative Care Clinic. J. Palliat. Med. 2021, 24, 91–96. [Google Scholar] [CrossRef]
- Kane, C.M.; Mulvey, M.R.; Wright, S.; Craigs, C.; Wright, J.M.; Bennett, M.I. Opioids Combined with Antidepressants or Antiepileptic Drugs for Cancer Pain: Systematic Review and Meta-Analysis. Palliat. Med. 2018, 32, 276–286. [Google Scholar] [CrossRef] [Green Version]
- Gilron, I.; Bailey, J.M.; Tu, D.; Holden, R.R.; Weaver, D.F.; Houlden, R.L. Morphine, Gabapentin, Or their Combination for Neuropathic Pain. N. Engl. J. Med. 2005, 352, 1324–1334. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, Y.; Okayama, S. Oral Methadone for Patients with Neuropathic Pain due to Neoplastic Brachial Plexopathy. J. Palliat. Care 2021, 08258597211016564. [Google Scholar] [CrossRef]
- Fawoubo, A.; Perceau-Chambard, É.; Ruer, M.; Filbet, M.; Tricou, C.; Economos, G. Methadone and Neuropathic Cancer Pain Subcomponents: A Prospective Cohort Pilot Study. BMJ Supportive Palliat. Care 2021. [Google Scholar] [CrossRef]
- Barakat, A. Revisiting Tramadol: A Multi-Modal Agent for Pain Management. CNS Drugs 2019, 33, 481–501. [Google Scholar] [CrossRef]
- Arbaiza, D.; Vidal, O. Tramadol in the Treatment of Neuropathic Cancer Pain. Clin. Drug Investig. 2007, 27, 75–83. [Google Scholar] [CrossRef]
- Duehmke, R.M.; Derry, S.; Wiffen, P.J.; Bell, R.F.; Aldington, D.; Moore, R.A. Tramadol for Neuropathic Pain in Adults. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Sazuka, S.; Koitabashi, T. Tapentadol is Effective in the Management of Moderate-to-Severe Cancer-Related Pain in Opioid-Naive and Opioid-Tolerant Patients: A Retrospective Study. J. Anesth. 2020, 34, 834–840. [Google Scholar] [CrossRef]
- Takemura, M.; Niki, K.; Okamoto, Y.; Matsuda, Y.; Omae, T.; Takagi, T.; Ueda, M. Tapentadol in Cancer Patients with Neuropathic Pain: A Comparison of Methadone, Oxycodone, Fentanyl, and Hydromorphone. Biol. Pharm. Bull. 2021, 44, 1286–1293. [Google Scholar] [CrossRef]
- Mercadante, S. Opioid Rotation for Cancer Pain: Rationale and Clinical Aspects. Cancer Interdiscip. Int. J. Am. Cancer Soc. 1999, 86, 1856–1866. [Google Scholar] [CrossRef]
- Cherny, N.; Ripamonti, C.; Pereira, J.; Davis, C.; Fallon, M.; McQuay, H.; Mercadante, S.; Pasternak, G.; Ventafridda, V.; Expert Working Group of the European Association of Palliative Care Network. Strategies to Manage the Adverse Effects of Oral Morphine: An Evidence-Based Report. J. Clin. Oncol. 2001, 19, 2542–2554. [Google Scholar] [CrossRef] [Green Version]
- McLean, S.; Twomey, F. Methods of Rotation from another Strong Opioid to Methadone for the Management of Cancer Pain: A Systematic Review of the Available Evidence. J. Pain Symptom Manag. 2015, 50, 248–259.e1. [Google Scholar] [CrossRef]
- Mercadante, S.; Bruera, E. Opioid Switching in Cancer Pain: From the Beginning to Nowadays. Crit. Rev. Oncol. 2016, 99, 241–248. [Google Scholar] [CrossRef]
- Mercadante, S.; Casuccio, A.; Fulfaro, F.; Groff, L.; Boffi, R.; Villari, P.; Gebbia, V.; Ripamonti, C. Switching from Morphine to Methadone to Improve Analgesia and Tolerability in Cancer Patients: A Prospective Study. J. Clin. Oncol. 2001, 19, 2898–2904. [Google Scholar] [CrossRef]
- Fleming, J.A.; O’Connor, B.D. Use of Lidocaine Patches for Neuropathic Pain in a Comprehensive Cancer Centre. Pain Res. Manag. 2009, 14, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Meier, T.; Wasner, G.; Faust, M.; Kuntzer, T.; Ochsner, F.; Hueppe, M.; Bogousslavsky, J.; Baron, R. Efficacy of Lidocaine Patch 5% in the Treatment of Focal Peripheral Neuropathic Pain Syndromes: A Randomized, Double-Blind, Placebo-Controlled Study. Pain 2003, 106, 151–158. [Google Scholar] [CrossRef]
- Rowbotham, M.C.; Davies, P.S.; Verkempinck, C.; Galer, B.S. Lidocaine Patch: Double-Blind Controlled Study of a New Treatment Method for Post-Herpetic Neuralgia. Pain 1996, 65, 39–44. [Google Scholar] [CrossRef]
- López Ramírez, E. Treatment of Acute and Chronic Focal Neuropathic Pain in Cancer Patients with Lidocaine 5% Patches. A Radiation and Oncology Department Experience. Supportive Care Cancer 2013, 21, 1329–1334. [Google Scholar] [CrossRef] [PubMed]
- Garzón-Rodríguez, C.; Casals Merchan, M.; Calsina-Berna, A.; López-Rómboli, E.; Porta-Sales, J. Lidocaine 5% Patches as an Effective Short-Term Co-Analgesic in Cancer Pain. Preliminary Results. Supportive Care Cancer 2013, 21, 3153–3158. [Google Scholar] [CrossRef]
- Jamero, D.; Borghol, A.; Vo, N.; Hawawini, F. The Emerging Role of NMDA Antagonists in Pain Management. US Pharm. 2011, 36, HS4–HS8. [Google Scholar]
- Chizh, B.; Headley, P. NMDA Antagonists and Neuropathic Pain-Multiple Drug Targets and Multiple Uses. Curr. Pharm. Des. 2005, 11, 2977–2994. [Google Scholar] [CrossRef]
- Mercadante, S.; Arcuri, E.; Tirelli, W.; Casuccio, A. Analgesic Effect of Intravenous Ketamine in Cancer Patients on Morphine Therapy: A Randomized, Controlled, Double-Blind, Crossover, Double-Dose Study. J. Pain Symptom Manag. 2000, 20, 246–252. [Google Scholar] [CrossRef]
- Hardy, J.; Quinn, S.; Fazekas, B.; Plummer, J.; Eckermann, S.; Agar, M.; Spruyt, O.; Rowett, D.; Currow, D.C. Randomized, Double-Blind, Placebo-Controlled Study to Assess the Efficacy and Toxicity of Subcutaneous Ketamine in the Management of Cancer Pain. J. Clin. Oncol. 2012, 30, 3611–3617. [Google Scholar] [CrossRef] [Green Version]
- Fallon, M.T.; Wilcock, A.; Kelly, C.A.; Paul, J.; Lewsley, L.; Norrie, J.; Laird, B.J. Oral Ketamine Vs Placebo in Patients with Cancer-Related Neuropathic Pain: A Randomized Clinical Trial. JAMA Oncol. 2018, 4, 870–872. [Google Scholar] [CrossRef] [Green Version]
- Blake, A.; Wan, B.A.; Malek, L.; DeAngelis, C.; Diaz, P.; Lao, N.; Chow, E.; O’Hearn, S. A Selective Review of Medical Cannabis in Cancer Pain Management. Ann. Palliat. Med. 2017, 6, S215–S222. [Google Scholar] [CrossRef] [Green Version]
- Lichtman, A.H.; Lux, E.A.; McQuade, R.; Rossetti, S.; Sanchez, R.; Sun, W.; Wright, S.; Kornyeyeva, E.; Fallon, M.T. Results of a Double-Blind, Randomized, Placebo-Controlled Study of Nabiximols Oromucosal Spray as an Adjunctive Therapy in Advanced Cancer Patients with Chronic Uncontrolled Pain. J. Pain Symptom Manag. 2018, 55, 179–188.e1. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.R.; Farquhar-Smith, W.P. Cannabinoids and Cancer Pain: A New Hope or a False Dawn? Eur. J. Intern. Med. 2018, 49, 30–36. [Google Scholar] [CrossRef]
- Boland, E.G.; Bennett, M.I.; Allgar, V.; Boland, J.W. Cannabinoids for Adult Cancer-Related Pain: Systematic Review and Meta-Analysis. BMJ Supportive Palliat. Care 2020, 10, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Pergolizzi, J.V., Jr.; LeQuang, J.A.; Taylor, R., Jr.; Raffa, R.B.; Colucci, D. The Role of Cannabinoids in Pain Control: The Good, the Bad, and the Ugly. Minerva Anestesiol. 2018, 84, 955–969. [Google Scholar] [CrossRef]
- Vayne-Bossert, P.; Afsharimani, B.; Good, P.; Gray, P.; Hardy, J. Interventional Options for the Management of Refractory Cancer Pain—what is the Evidence? Supportive Care Cancer 2016, 24, 1429–1438. [Google Scholar] [CrossRef]
- Sjöberg, M.; Nitescu, P.; Appelgren, L.; Curelaru, I. Long-Term Intrathecal Morphine and Bupivacaine in Patients with Refractory Cancer Pain. Results from a Morphine: Bupivacaine Dose Regimen of 0.5:4.75 mg/ml. Anesthesiology 1994, 80, 284–297. [Google Scholar] [CrossRef]
- Eisenach, J.C.; DuPen, S.; Dubois, M.; Miguel, R.; Allin, D.; Epidural Clonidine Study Group. Epidural Clonidine Analgesia for Intractable Cancer Pain. Pain 1995, 61, 391–399. [Google Scholar] [CrossRef]
- Eisenach, J.C.; Hood, D.D.; Curry, R. Intrathecal, but Not Intravenous, Clonidine Reduces Experimental Thermal or Capsaicin-Induced Pain and Hyperalgesia in Normal Volunteers. Anesth. Analg. 1998, 87, 591–596. [Google Scholar] [CrossRef]
- Banik, R.K.; Engle, M.P. Ziconotide for Management of Cancer Pain Refractory to Pharmacotherapy: An Update. Pain Med. 2020, 21, 3253–3259. [Google Scholar] [CrossRef]
- Staats, P.S.; Yearwood, T.; Charapata, S.G.; Presley, R.W.; Wallace, M.S.; Byas-Smith, M.; Fisher, R.; Bryce, D.A.; Mangieri, E.A.; Luther, R.R. Intrathecal Ziconotide in the Treatment of Refractory Pain in Patients with Cancer or AIDS: A Randomized Controlled Trial. JAMA 2004, 291, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Van den Beuken-van Everdingen, M.H.J.; de Graeff, A.; Jongen, J.L.; Dijkstra, D.; Mostovaya, I.; Vissers, K.C.; National Guideline Working Group “Diagnosis Treatment of Cancer Pain”. Pharmacological Treatment of Pain in Cancer Patients: The Role of Adjuvant Analgesics, a Systematic Review. Pain Pract. 2017, 17, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Nieto, F.R.; Cobos, E.J.; Tejada, M.Á.; Sánchez-Fernández, C.; González-Cano, R.; Cendán, C.M. Tetrodotoxin (TTX) as a Therapeutic Agent for Pain. Mar. Drugs 2012, 10, 281–305. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.L.; Clark, A.J.; Huang, J.; Waxman, S.G.; Dib-Hajj, S.D. The Role of Voltage-Gated Sodium Channels in Pain Signaling. Physiol. Rev. 2019, 99, 1079–1151. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Fang, D.; Cai, J.; Wan, Y.; Han, J.; Xing, G. Enhanced Excitability of Small Dorsal Root Ganglion Neurons in Rats with Bone Cancer Pain. Mol. Pain 2012, 8, 1744–8069. [Google Scholar] [CrossRef] [Green Version]
- González-Cano, R.; Ruiz-Cantero, M.C.; Santos-Caballero, M.; Gómez-Navas, C.; Tejada, M.Á.; Nieto, F.R. Tetrodotoxin, a Potential Drug for Neuropathic and Cancer Pain Relief? Toxins 2021, 13, 483. [Google Scholar] [CrossRef]
- Hagen, N.A.; Fisher, K.M.; Lapointe, B.; du Souich, P.; Chary, S.; Moulin, D.; Sellers, E.; Ngoc, A.H.; Canadian Tetrodotoxin Study Group. An Open-Label, Multi-Dose Efficacy and Safety Study of Intramuscular Tetrodotoxin in Patients with Severe Cancer-Related Pain. J. Pain Symptom Manag. 2007, 34, 171–182. [Google Scholar] [CrossRef]
- Hagen, N.A.; Cantin, L.; Constant, J.; Haller, T.; Blaise, G.; Ong-Lam, M.; du Souich, P.; Korz, W.; Lapointe, B. Tetrodotoxin for Moderate to Severe Cancer-Related Pain: A Multicentre, Randomized, Double-Blind, Placebo-Controlled, Parallel-Design Trial. Pain Res. Manag. 2017, 2017, 7212713. [Google Scholar] [CrossRef]
- Egeo, G.; Fofi, L.; Barbanti, P. Botulinum Neurotoxin for the Treatment of Neuropathic Pain. Front. Neurol. 2020, 11, 716. [Google Scholar] [CrossRef]
- Reyes-Long, S.; Alfaro-Rodríguez, A.; Cortes-Altamirano, J.L.; Lara-Padilla, E.; Herrera-Maria, E.; Romero-Morelos, P.; Salcedo, M.; Bandala, C. The Mechanisms of Action of Botulinum Toxin Type A in Nociceptive and Neuropathic Pathways in Cancer Pain. Curr. Med. Chem. 2021, 28, 2996–3009. [Google Scholar] [CrossRef]
- Eid, S.; Cortright, D. Transient Receptor Potential Channels on Sensory Nerves. Sens. Nerves 2009, 194, 261–281. [Google Scholar]
- Liu, Y.; Qin, N. TRPM8 in Health and Disease: Cold Sensing and Beyond. Transient Recept. Potential Channels 2011, 704, 185–208. [Google Scholar]
- Proudfoot, C.J.; Garry, E.M.; Cottrell, D.F.; Rosie, R.; Anderson, H.; Robertson, D.C.; Fleetwood-Walker, S.M.; Mitchell, R. Analgesia Mediated by the TRPM8 Cold Receptor in Chronic Neuropathic Pain. Curr. Biol. 2006, 16, 1591–1605. [Google Scholar] [CrossRef] [Green Version]
- Fallon, M.; Storey, D.; Krishan, A.; Weir, C.; Mitchell, R.; Fleetwood-Walker, S.; Scott, A.; Colvin, L. Cancer Treatment-Related Neuropathic Pain: Proof of Concept Study with Menthol—A TRPM8 Agonist. Supportive Care Cancer 2015, 23, 2769–2777. [Google Scholar] [CrossRef] [Green Version]
- Borges, J.P.; Mekhail, K.; Fairn, G.D.; Antonescu, C.N.; Steinberg, B.E. Modulation of Pathological Pain by Epidermal Growth Factor Receptor. Front. Pharmacol. 2021, 12, 642820. [Google Scholar] [CrossRef]
- Sopata, M.; Katz, N.; Carey, W.; Smith, M.D.; Keller, D.; Verburg, K.M.; West, C.R.; Wolfram, G.; Brown, M.T. Efficacy and Safety of Tanezumab in the Treatment of Pain from Bone Metastases. Pain 2015, 156, 1703–1713. [Google Scholar] [CrossRef]
- Fallon, M.; Sopata, M.; Dragon, E.; Brown, M.; Viktrup, L.; West, C.; Hamlett, K.; Bao, W.; Agyemang, A. LBA62 Efficacy and Safety of Tanezumab in Subjects with Cancer Pain Predominantly due to Bone Metastasis Receiving Background Opioid Therapy. Ann. Oncol. 2021, 32, S1339. [Google Scholar] [CrossRef]
- Sigismund, S.; Avanzato, D.; Lanzetti, L. Emerging Functions of the EGFR in Cancer. Mol. Oncol. 2018, 12, 3–20. [Google Scholar] [CrossRef]
- Kersten, C.; Cameron, M.G. Cetuximab Alleviates Neuropathic Pain Despite Tumour Progression. Case Rep. 2012, 2012, bcr1220115374. [Google Scholar] [CrossRef] [Green Version]
- Kersten, C.; Cameron, M.G.; Mjåland, S. Epithelial Growth Factor Receptor (EGFR)-Inhibition for Relief of Neuropathic pain–A Case Series. Scand. J. Pain 2013, 4, 3–7. [Google Scholar] [CrossRef]
- Kersten, C.; Cameron, M.; Laird, B.; Mjåland, S. Epidermal Growth Factor receptor–inhibition (EGFR-I) in the Treatment of Neuropathic Pain. Br. J. Anaesth. 2015, 115, 761–767. [Google Scholar] [CrossRef] [Green Version]
- Lananna, B.V.; Musiek, E.S. The Wrinkling of Time: Aging, Inflammation, Oxidative Stress, and the Circadian Clock in Neurodegeneration. Neurobiol. Dis. 2020, 139, 104832. [Google Scholar] [CrossRef] [PubMed]
- Kersten, C.; Cameron, M.G.; Bailey, A.G.; Fallon, M.T.; Laird, B.J.; Paterson, V.; Mitchell, R.; Fleetwood-Walker, S.M.; Daly, F.; Mjåland, S. Relief of Neuropathic Pain through Epidermal Growth Factor Receptor Inhibition: A Randomized Proof-of-Concept Trial. Pain Med. 2019, 20, 2495–2505. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Liang, D.; Bao, M.; Xie, Y.; Xu, W.; Wang, L.; Wang, Z.; Qiao, Z. Gx-50 Inhibits Neuroinflammation Via A7 nAChR Activation of the JAK2/STAT3 and PI3K/AKT Pathways. J. Alzheimer’s Dis. 2016, 50, 859–871. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Han, Q.; Deng, M.; Zhao, M.; Apryani, E.; Shoaib, R.M.; Wei, D.; Wang, Y. Lemairamin, Isolated from the Zanthoxylum Plants, Alleviates Pain Hypersensitivity Via Spinal A7 Nicotinic Acetylcholine Receptors. Biochem. Biophys. Res. Commun. 2020, 525, 1087–1094. [Google Scholar] [CrossRef] [PubMed]
- Deng, M.; Ahmad, K.A.; Han, Q.; Wang, Z.; Shoaib, R.M.; Li, X.; Wang, Y. Thalidomide Alleviates Neuropathic Pain through Microglial IL-10/β-Endorphin Signaling Pathway. Biochem. Pharmacol. 2021, 192, 114727. [Google Scholar] [CrossRef]
- Shoaib, R.M.; Ahmad, K.A.; Wang, Y. Protopanaxadiol Alleviates Neuropathic Pain by Spinal Microglial Dynorphin a Expression Following Glucocorticoid Receptor Activation. Br. J. Pharmacol. 2021, 178, 2976–2997. [Google Scholar] [CrossRef]
Figure 1.
Neuropathic Cancer Pain (NcP) treatment algorithm based on clinical experience. * There is some evidence suggesting the benefit of adjuvant drugs such as gabapentinoids (gabapentin and pregabalin) and antidepressants such as amitriptyline. ** most commonly methadone is used, although requiring caution regarding its titration and dose conversion.
Figure 1.
Neuropathic Cancer Pain (NcP) treatment algorithm based on clinical experience. * There is some evidence suggesting the benefit of adjuvant drugs such as gabapentinoids (gabapentin and pregabalin) and antidepressants such as amitriptyline. ** most commonly methadone is used, although requiring caution regarding its titration and dose conversion.


{kind=link}
Table 1.
Pain syndromes due to nervous tissue lesions.
| 1. Peripheral nerve syndrome | a. due to paraspinal mass b. due to chest wall mass c. due to retroperitoneal mass other than paraspinal d. due to other soft-tissue or bony tumor e. peripheral polyneuropathy |
| 2. Radiculopathy or cauda equina syndrome | a. due to vertebral lesion b. due to leptomeningeal metastases c. due to other intraspinal neoplasm |
| 3. Plexopathy | a. cervical plexopathy b. brachial plexopathy c. lumbosacral plexopathy d. sacral plexopathy |
| 4. Cranial neuropathy | a. due to base of the skull tumor b. due to leptomeningeal metastases c. due to other soft-tissue or bony cranial tumor |
| 5. Pain due to central nervous system lesion | a. due to myelopathy b. intracerebral lesion |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Shkodra, M.; Caraceni, A. Treatment of Neuropathic Pain Directly Due to Cancer: An Update. Cancers 2022, 14, 1992. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14081992
AMA Style
Shkodra M, Caraceni A. Treatment of Neuropathic Pain Directly Due to Cancer: An Update. Cancers. 2022; 14(8):1992. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14081992
Chicago/Turabian StyleShkodra, Morena, and Augusto Caraceni. 2022. "Treatment of Neuropathic Pain Directly Due to Cancer: An Update" Cancers 14, no. 8: 1992. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14081992
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.