
Treating Primary Node-Positive Prostate Cancer: A Scoping Review of Available Treatment Options

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
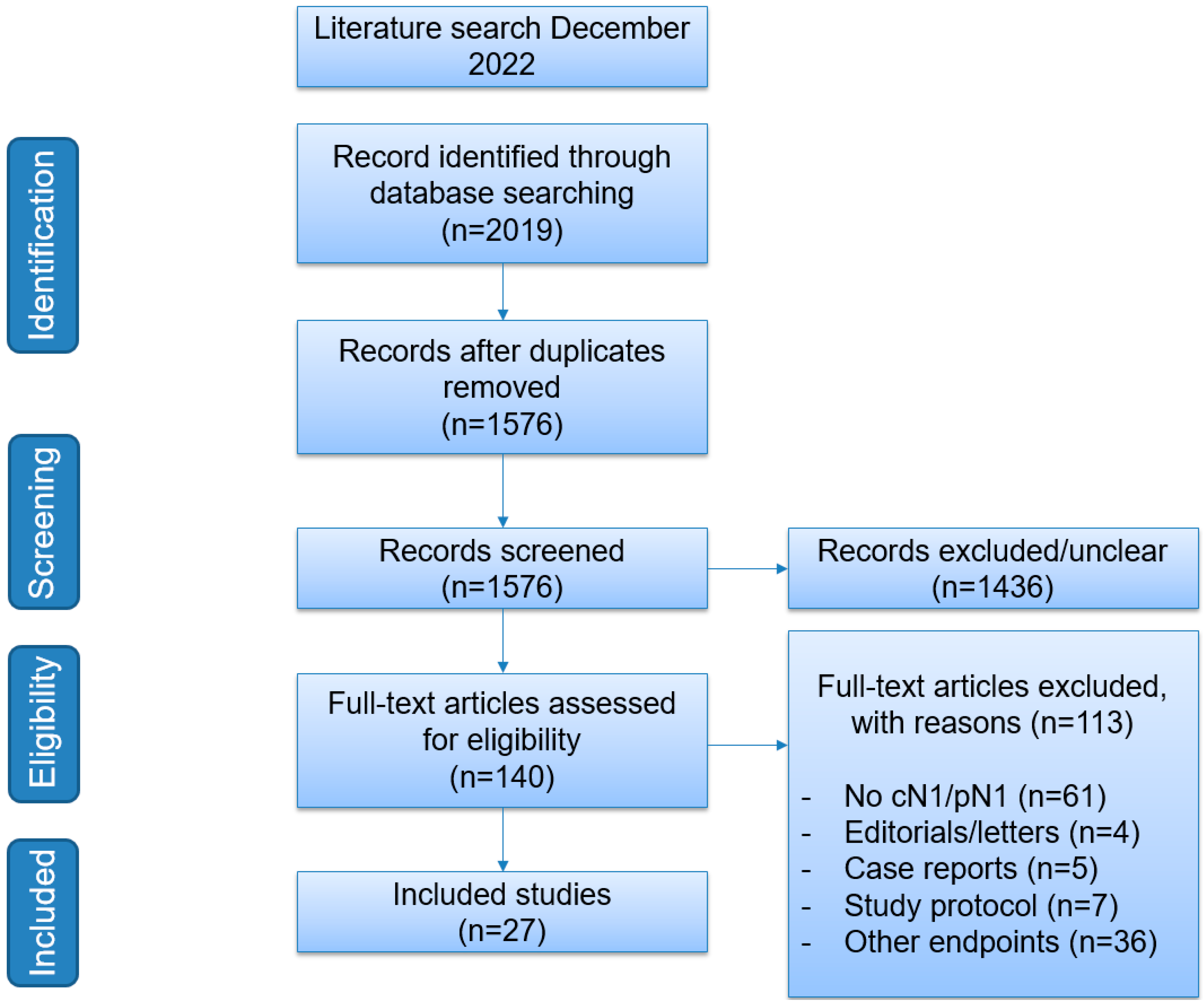
2. Materials and Methods
3. Results
3.1. Treatment of Patients with cN1M0 Disease
3.1.1. Treatment with ADT
3.1.2. Treatment with Local Therapy
3.1.3. Treatment with ADT ± Any Form of Local Therapy
3.1.4. Treatment with ADT ± Additional Systemic Therapy
3.2. Treatment of Patients with pN1M0 Disease
3.2.1. ADT as Adjuvant Treatment
3.2.2. ADT ± EBRT as Adjuvant Treatment
3.2.3. EBRT as Adjuvant Treatment
3.2.4. Chemotherapy as Adjuvant Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Bellmunt, J.; Bolla, M. EAU-ESTRO-SIOG Guidelines on prostate cancer. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Touijer, K.A.; Mazzola, C.R.; Sjoberg, D.D.; Scardino, P.T.; Eastham, J.A. Long-term outcomes of patients with lymph node metastasis treated with radical prostatectomy without adjuvant androgen-deprivation therapy. Eur. Urol. 2014, 65, 20–25. [Google Scholar] [CrossRef]
- Mandel, P.; Rosenbaum, C.; Pompe, R.S.; Steuber, T.; Salomon, G.; Chun, F.K.; Graefen, M.; Huland, H.; Tilki, D. Long-term oncological outcomes in patients with limited nodal disease undergoing radical prostatectomy and pelvic lymph node dissection without adjuvant treatment. World J. Urol. 2017, 35, 1833–1839. [Google Scholar] [CrossRef] [PubMed]
- Touijer, K.A.; Karnes, R.J.; Passoni, N.; Sjoberg, D.D.; Assel, M.; Fossati, N.; Gandaglia, G.; Eastham, J.A.; Scardino, P.T.; Vickers, A.; et al. Survival Outcomes of Men with Lymph Node-positive Prostate Cancer After Radical Prostatectomy: A Comparative Analysis of Different Postoperative Management Strategies. Eur. Urol. 2018, 73, 890–896. [Google Scholar] [CrossRef]
- Da Pozzo, L.F.; Cozzarini, C.; Briganti, A.; Suardi, N.; Salonia, A.; Bertini, R.; Gallina, A.; Bianchi, M.; Fantini, G.V.; Bolognesi, A.; et al. Long-Term Follow-up of Patients with Prostate Cancer and Nodal Metastases Treated by Pelvic Lymphadenectomy and Radical Prostatectomy: The Positive Impact of Adjuvant Radiotherapy. Eur. Urol. 2009, 55, 1003–1011. [Google Scholar] [CrossRef]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Attard, G.; Murphy, L.; Clarke, N.W.; Cross, W.; Jones, R.J.; Parker, C.C.; Gillessen, S.; Cook, A.; Brawley, C.; Amos, C.L.; et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet 2022, 399, 447–460. [Google Scholar] [CrossRef]
- Schaeffer, E.M.C.; An, Y.; Barocas, D.M.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; Victor, A.D.; Desai, N.; Dorff, T.; et al. NCCN Guidelines Version 1.2023 Prostate Cancer. 2022. Available online: https://www.nccn.org/home/ (accessed on 1 March 2023).
- Lieng, H.; Kneebone, A.; Hayden, A.J.; Christie, D.R.H.; Davis, B.J.; Eade, T.N.; Emmett, L.; Holt, T.; Hruby, G.; Pryor, D.; et al. Radiotherapy for node-positive prostate cancer: 2019 Recommendations of the Australian and New Zealand Radiation Oncology Genito-Urinary group. Radiother. Oncol. 2019, 140, 68–75. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Schröder, F.H.; Kurth, K.H.; Fossa, S.D.; Hoekstra, W.; Karthaus, P.P.; De Prijck, L.; Collette, L. Early Versus Delayed Endocrine Treatment of T2-T3 pN1-3 M0 Prostate Cancer Without Local Treatment of the Primary Tumour: Final Results of European Organisation for the Research and Treatment of Cancer Protocol 30846 After 13 Years of Follow-up (A Randomised Controlled Trial). Eur. Urol. 2009, 55, 14–22. [Google Scholar] [CrossRef]
- Pilepich, M.V.; Winter, K.; Lawton, C.A.; Krisch, R.E.; Wolkov, H.B.; Movsas, B.; Hug, E.B.; Asbell, S.O.; Grignon, D. Androgen suppression adjuvant to definitive radiotherapy in prostate carcinoma—Long-term results of phase III RTOG 85-31. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 1285–1290. [Google Scholar] [CrossRef]
- Tward, J.D.; Kokeny, K.E.; Shrieve, D.C. Radiation therapy for clinically node-positive prostate adenocarcinoma is correlated with improved overall and prostate cancer-specific survival. Pract. Radiat. Oncol. 2013, 3, 234–240. [Google Scholar] [CrossRef]
- Rusthoven, C.G.; Carlson, J.A.; Waxweiler, T.V.; Raben, D.; Dewitt, P.E.; Crawford, E.D.; Maroni, P.D.; Kavanagh, B.D. The impact of definitive local therapy for lymph node-positive prostate cancer: A population-based study. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 1064–1073. [Google Scholar] [CrossRef]
- Lin, C.C.; Gray, P.J.; Jemal, A.; Efstathiou, J.A. Androgen Deprivation with or Without Radiation Therapy for Clinically Node-Positive Prostate Cancer. J. Natl. Cancer Inst. 2015, 107, djv119. [Google Scholar] [CrossRef] [PubMed]
- James, N.D.; Spears, M.R.; Clarke, N.W.; Dearnaley, D.P.; Mason, M.D.; Parker, C.C.; Ritchie, A.W.S.; Russell, J.M.; Schiavone, F.; Attard, G.; et al. Failure-free survival and radiotherapy in patients with newly diagnosed nonmetastatic prostate cancer. JAMA Oncol. 2016, 2, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Seisen, T.; Vetterlein, M.W.; Karabon, P.; Jindal, T.; Sood, A.; Nocera, L.; Nguyen, P.L.; Choueiri, T.K.; Trinh, Q.D.; Menon, M.; et al. Efficacy of Local Treatment in Prostate Cancer Patients with Clinically Pelvic Lymph Node-positive Disease at Initial Diagnosis. Eur. Urol. 2018, 73, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Bryant, A.K.; Kader, A.K.; McKay, R.R.; Einck, J.P.; Mell, L.K.; Mundt, A.J.; Kane, C.J.; Efstathiou, J.A.; Murphy, J.D.; Rose, B.S. Definitive Radiation Therapy and Survival in Clinically Node-Positive Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1188–1193. [Google Scholar] [CrossRef]
- Vale, C.L.; Burdett, S.; Rydzewska, L.H.M.; Albiges, L.; Clarke, N.W.; Fisher, D.; Fizazi, K.; Gravis, G.; James, N.D.; Mason, M.D.; et al. Addition of docetaxel or bisphosphonates to standard of care in men with localised or metastatic, hormone-sensitive prostate cancer: A systematic review and meta-analyses of aggregate data. Lancet Oncol. 2016, 17, 243–256. [Google Scholar] [CrossRef]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.G.; et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef]
- Armstrong, A.J.; Szmulewitz, R.Z.; Petrylak, D.P.; Holzbeierlein, J.; Villers, A.; Azad, A.; Alcaraz, A.; Alekseev, B.; Iguchi, T.; Shore, N.D.; et al. Arches: A randomized, phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J. Clin. Oncol. 2019, 37, 2974–2986. [Google Scholar] [CrossRef]
- Chi, K.N.; Chowdhury, S.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, R.; Soto, A.J.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H.; et al. Apalutamide in Patients With Metastatic Castration-Sensitive Prostate Cancer: Final Survival Analysis of the Randomized, Double-Blind, Phase III TITAN Study. J. Clin. Oncol. 2021, 39, 2294–2303. [Google Scholar] [CrossRef] [PubMed]
- Buonerba, C.; Ferro, M.; Dolce, P.; Crocetto, F.; Verde, A.; Lucarelli, G.; Scafuri, L.; Facchini, S.; Vaia, A.; Marinelli, A.; et al. Predictors of efficacy of androgen-receptor-axis-targeted therapies in patients with metastatic castration-sensitive prostate cancer: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2020, 151, 102992. [Google Scholar] [CrossRef] [PubMed]
- James, N.D.; Ingleby, F.C.; Clarke, N.W.; Amos, C.L.; Attard, G.; Brawley, C.D.; Chowdhury, S.; Cross, W.; Dearnaley, D.P.; Gilbert, D.C.; et al. Docetaxel for Nonmetastatic Prostate Cancer: Long-Term Survival Outcomes in the STAMPEDE Randomized Controlled Trial. JNCI Cancer Spectr. 2022, 6, pkac043. [Google Scholar] [CrossRef] [PubMed]
- Messing, E.M.; Manola, J.; Yao, J.; Kiernan, M.; Crawford, D.; Wilding, G.; di’SantAgnese, P.A. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol. 2006, 7, 472–479. [Google Scholar] [CrossRef]
- Wong, A.T.; Schwartz, D.; Osborn, V.; Safdieh, J.; Weiner, J.; Schreiber, D. Adjuvant radiation with hormonal therapy is associated with improved survival in men with pathologically involved lymph nodes after radical surgery for prostate cancer. Urol. Oncol. Semin. Orig. Investig. 2016, 34, 529.e15–529.e20. [Google Scholar] [CrossRef]
- Gupta, M.; Patel, H.D.; Schwen, Z.R.; Tran, P.T.; Partin, A.W. Adjuvant radiation with androgen-deprivation therapy for men with lymph node metastases after radical prostatectomy: Identifying men who benefit. BJU Int. 2019, 123, 252–260. [Google Scholar] [CrossRef]
- Briganti, A.; Karnes, R.J.; Da Pozzo, L.F.; Cozzarini, C.; Capitanio, U.; Gallina, A.; Suardi, N.; Bianchi, M.; Tutolo, M.; Salonia, A.; et al. Combination of adjuvant hormonal and radiation therapy significantly prolongs survival of patients with pT2-4 pN+ prostate cancer: Results of a matched analysis. Eur. Urol. 2011, 59, 832–840. [Google Scholar] [CrossRef]
- Kaplan, J.R.; Kowalczyk, K.J.; Borza, T.; Gu, X.; Lipsitz, S.R.; Nguyen, P.L.; Friedlander, D.F.; Trinh, Q.D.; Hu, J.C. Patterns of care and outcomes of radiotherapy for lymph node positivity after radical prostatectomy. BJU Int. 2013, 111, 1208–1214. [Google Scholar] [CrossRef]
- Abdollah, F.; Karnes, R.J.; Suardi, N.; Cozzarini, C.; Gandaglia, G.; Fossati, N.; Vizziello, D.; Sun, M.; Karakiewicz, P.I.; Menon, M.; et al. Impact of adjuvant radiotherapy on survival of patients with node-positive prostate cancer. J. Clin. Oncol. 2014, 32, 3939–3947. [Google Scholar] [CrossRef]
- Jegadeesh, N.; Liu, Y.; Zhang, C.; Zhong, J.; Cassidy, R.J.; Gillespie, T.; Kucuk, O.; Rossi, P.; Master, V.A.; Alemozaffar, M.; et al. The role of adjuvant radiotherapy in pathologically lymph node-positive prostate cancer. Cancer 2017, 123, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Van Hemelryk, A.; De Meerleer, G.; Ost, P.; Poelaert, F.; De Gersem, W.; Decaestecker, K.; De Visschere, P.; Fonteyne, V. The Outcome for Patients With Pathologic Node-Positive Prostate Cancer Treated With Intensity Modulated Radiation Therapy and Androgen Deprivation Therapy: A Case-Matched Analysis of pN1 and pN0 Patients. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Poelaert, F.; Fonteyne, V.; Ost, P.; De Troyer, B.; Decaestecker, K.; De Meerleer, G.; De Visschere, P.; Claeys, T.; Dhondt, B.; Lumen, N. Bestrahlung des gesamten Beckens beim nodal metastasierten Prostatakarzinom: Onkologisches Outcome und prognostische Faktoren. Strahlenther. Onkol. 2017, 193, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Fonteyne, V.; Van Praet, C.; Ost, P.; Van Bruwaene, S.; Liefhooghe, N.; Berghen, C.; De Meerleer, G.; Vanneste, B.; Verbaeys, C.; Verbeke, S.; et al. Evaluating the Impact of Prostate Only Versus Pelvic Radiotherapy for Pathological Node-positive Prostate Cancer: First Results from the Multicenter Phase 3 PROPER Trial. Eur. Urol. Focus 2022, 9, 317–324. [Google Scholar] [CrossRef]
- Tilki, D.; Chen, M.-H.; Wu, J.; Huland, H.; Graefen, M.; Wiegel, T.; Böhmer, D.; Mohamad, O.; Cowan, J.E.; Feng, F.Y.; et al. Adjuvant Versus Early Salvage Radiation Therapy for Men at High Risk for Recurrence Following Radical Prostatectomy for Prostate Cancer and the Risk of Death. J. Clin. Oncol. 2021, 39, 2284–2293. [Google Scholar] [CrossRef]
- Ahlgren, G.M.; Flodgren, P.; Tammela, T.L.J.; Kellokumpu-Lehtinen, P.; Borre, M.; Angelsen, A.; Iversen, J.R.; Sverrisdottir, A.; Jonsson, E.; Sengelov, L. Docetaxel Versus Surveillance After Radical Prostatectomy for High-risk Prostate Cancer: Results from the Prospective Randomised, Open-label Phase 3 Scandinavian Prostate Cancer Group 12 Trial. Eur. Urol. 2018, 73, 870–876. [Google Scholar] [CrossRef]
- Kishan, A.U.; Sun, Y.; Hartman, H.; Pisansky, T.M.; Bolla, M.; Neven, A.; Steigler, A.; Denham, J.W.; Feng, F.Y.; Zapatero, A.; et al. Androgen deprivation therapy use and duration with definitive radiotherapy for localised prostate cancer: An individual patient data meta-analysis. Lancet Oncol. 2022, 23, 304–316. [Google Scholar] [CrossRef]
- Parker, C.C.; James, N.D.; Brawley, C.D.; Clarke, N.W.; Hoyle, A.P.; Ali, A.; Ritchie, A.W.S.; Attard, G.; Chowdhury, S.; Cross, W.; et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomised controlled phase 3 trial. Lancet 2018, 392, 2353–2366. [Google Scholar] [CrossRef]
- Boevé, L.M.; Hulshof, M.C.; Vis, A.N.; Zwinderman, A.H.; Twisk, J.W.; Witjes, W.P.; Delaere, K.P.; van Moorselaar, R.J.A.; Verhagen, P.C.; van Andel, G. Effect on Survival of Androgen Deprivation Therapy Alone Compared to Androgen Deprivation Therapy Combined with Concurrent Radiation Therapy to the Prostate in Patients with Primary Bone Metastatic Prostate Cancer in a Prospective Randomised Clinical Tria. Eur. Urol. 2019, 75, 410–418. [Google Scholar] [CrossRef]
- Burdett, S.; Boevé, L.M.; Ingleby, F.C.; Fisher, D.J.; Rydzewska, L.H.; Vale, C.L.; van Andel, G.; Clarke, N.W.; Hulshof, M.C.; James, N.D.; et al. Prostate Radiotherapy for Metastatic Hormone-sensitive Prostate Cancer: A STOPCAP Systematic Review and Meta-analysis. Eur. Urol. 2019, 76, 115–124. [Google Scholar] [CrossRef]
- Gravis, G.; Boher, J.; Chen, Y.; Liu, G.; Fizazi, K.; Carducci, A.; Oudard, S.; Joly, F.; Jarrard, D.M.; Soulie, M.; et al. Burden of Metastatic Castrate Naive Prostate Cancer Patients, to Identify Men More Likely to Benefit from Early Docetaxel: Further Analyses of CHAARTED and GETUG-AFU15 Studies. Eur. Urol. 2019, 73, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Roach, M.; Moughan, J.; Lawton, C.A.F.; Dicker, A.P.; Zeitzer, K.L.; Gore, E.M.; Kwok, Y.; Seider, M.J.; Hsu, I.C.; Hartford, A.C.; et al. Sequence of hormonal therapy and radiotherapy field size in unfavourable, localised prostate cancer (NRG/RTOG 9413): Long-term results of a randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1504–1515. [Google Scholar] [CrossRef] [PubMed]
- Pommier, P.; Chabaud, S.; Lagrange, J.L.; Richaud, P.; Le Prise, E.; Wagner, J.P.; Azria, D.; Beckendorf, V.; Suchaud, J.P.; Bernier, V.; et al. Is There a Role for Pelvic Irradiation in Localized Prostate Adenocarcinoma? Update of the Long-Term Survival Results of the GETUG-01 Randomized Study. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 759–769. [Google Scholar] [CrossRef]
- Murthy, V.; Maitre, P.; Kannan, S.; Panigrahi, G.; Krishnatry, R.; Bakshi, G.; Prakash, G.; Pal, M.; Menon, S.; Phurailatpam, R.; et al. Prostate-Only Versus Whole-Pelvic Radiation Therapy in High-Risk and Very High-Risk Prostate Cancer (POP-RT): Outcomes From Phase III Randomized Controlled Trial. J. Clin. Oncol. 2021, 39, 1234–1242. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.; Leliveld, A.M.; Decaestecker, K.; De Meerleer, G.; Berghen, C.; Briganti, A.; Vulsteke, C.; Murray, J.; Joniau, S.; Leliveld, A.M.; et al. Elective nodal radiotherapy in prostate cancer. Lancet Oncol. 2021, 22, e348–e357. [Google Scholar]
- Seiler, R.; Studer, U.E.; Tschan, K.; Bader, P.; Burkhard, F.C. Removal of limited nodal disease in patients undergoing radical prostatectomy: Long-term results confirm a chance for cure. J. Urol. 2014, 191, 1280–1285. [Google Scholar] [CrossRef]
- Parker, C.C.; Clarke, N.W.; Cook, A.D.; Kynaston, H.G.; Petersen, P.M.; Catton, C.; Cross, W.; Logue, J.; Parulekar, W.; Payne, H.; et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): A randomised, controlled phase 3 trial. Lancet 2020, 396, 1413–1421. [Google Scholar] [CrossRef]
- Vale, C.L.; Fisher, D.; Kneebone, A.; Parker, C.; Pearse, M.; Richaud, P.; Sargos, P.; Sydes, M.R.; Brawley, C.; Brihoum, M.; et al. Adjuvant or early salvage radiotherapy for the treatment of localised and locally advanced prostate cancer: A prospectively planned systematic review and meta-analysis of aggregate data. Lancet 2020, 396, 1422–1431. [Google Scholar] [CrossRef]
- Perera, M.; Papa, N.; Roberts, M.; Williams, M.; Udovicich, C.; Vela, I.; Christidis, D.; Bolton, D.; Hofman, M.S.; Lawrentschuk, N.; et al. Gallium-68 Prostate-specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer—Updated Diagnostic Utility, Sensitivity, Specificity, and Distribution of Prostate-specific Membrane Antigen-avid Lesions: A Systematic Review and Meta-. Eur. Urol. 2020, 77, 403–417. [Google Scholar] [CrossRef]
- Meijer, D.; van Leeuwen, P.J.; Roberts, M.J.; Siriwardana, A.R.; Morton, A.; Yaxley, J.W.; Samaratunga, H.; Emmett, L.; van de Ven, P.M.; van der Poel, H.G.; et al. External Validation and Addition of Prostate-specific Membrane Antigen Positron Emission Tomography to the Most Frequently Used Nomograms for the Prediction of Pelvic Lymph-node Metastases: An International Multicenter Study. Eur. Urol. 2021, 80, 234–242. [Google Scholar] [CrossRef]


{kind=link}
| Guideline | cN1M0 | pN1M0 |
|---|---|---|
| EAU [2] |
|
|
| FROGG [10] |
|
|
| NCCN [9] |
|
|
| P | Population | Patients with clinically node-positive prostate cancer (cN1M0) |
| I | Intervention | Treatment A |
| C | Comparator | Treatment B |
| O | Outcome | Oncological outcome, survival |
| P | Population | Patients with pathologically node-positive prostate cancer (pN1M0) after primary lymph node dissection (RP + LND as treatment or with staging LND) |
| I | Intervention | Treatment A |
| C | Comparator | Treatment B |
| O | Outcome | Oncological outcome, survival |
| Study Design | Number of cN1M0 Patients | Treatment Groups | Study Period | Outcome | |
|---|---|---|---|---|---|
| ADT | |||||
| Schröder et al. (2009) [12] | RCT: EORTC 30846 | 234 | Arm I: immediate ADT ARM II: delayed ADT | 1986–1998 | No statistically significant differences Median OS 7.6 yr (95% CI, 6.3–8.3 yr) (immediate) vs. 6.1 yr (95% CI, 5.7–7.3 yr) (delayed) HR 1.22 for OS (95% CI 0.92–1.62); not statistically significant |
| Local therapy | |||||
| Pilepich et al. (2005) [13] | RCT: Phase III RTOG 85-31 | 263 | Arm I: EBRT + goserelin Arm II: RT alone | 1987–1992 | Favours EBRT + ADT, especially high GS. 10 yr absolute survival 49% (RT + ADT) vs. 39% (RT alone) (p = 0.002) |
| Tward et al. (2013) [14] | Observational, SEER database | 1100 | EBRT vs. no EBRT | 1988–2006 | Favours EBRT 10-yr CSS 50% vs. 63%; (HR 0.66, 95% CI 0.54–0.82, p < 0.01) 10-yr OS 29% vs. 44%; (HR 0.70, 95% CI 0.59–0.81, p < 0.01) |
| ADT ± any form of local therapy | |||||
| Rusthoven et al. (2014) [15] | Observational, SEER database | 796 | ADT vs. ADT + EBRT | 1995–2006 | Favours EBRT over no therapy 10 yr OS rate of 45% vs. 29% (p < 0.001) 10 yr PCSS rate 76% vs. 53% (p < 0.001) |
| Lin et al. (2015) [16] | Observational, NCDB | 3540 total—318 propensity scored matched | ADT vs. ADT + EBRT | 2004–2011 Sub-cohort 2004–2006 | Favours ADT + EBRT 50% reduction in 5-yr all-cause mortality (HR = 0.50, 95% CI 0.37–0.67, p < 0.001) |
| James et al. (2016) [17] | Observational, control arm of STAMPEDE | 177 | ADT vs. ADT + EBRT | 2005–2014 | Favours ADT + EBRT HR 0.48 (95% CI 0.29–0.79) 2 yr FFS of 81% (95% CI 0.71–0.85) (ADT + RT) vs. 53% (95% CI 0.40–0.65) (ADT) |
| Seisen et al. (2018) [18] | Observational, NCDB | 1987 | ADT vs. ADT + Local Therapy (LT) | 2003–2011 | Favours ADT + LT 5 yr OM-free survival was 78.8% (95% CI 74.1–83.9%) (ADT + LT) vs. 49.2% (95% CI 33.9–71.4) (ADT) |
| Bryant et al. (2018) [19] | Observational, Veterans Affair database | 648 | ADT vs. ADT + EBRT | 2000–2015 | Favours ADT + EBRT PSA < 26: ADT + RT improved PCSM (HR 0.50: 95%CI 0.28–0.88; p = 0.02) and ACM (HR 0.38; 95%CI 0.25–0.57; p < 0.001) |
| ADT ± Systemic treatment | |||||
| Vale et al. (2016) [20] | Systematic review: GETUG-12, RTOG 0521, STAMPEDE | 945 | ADT ± docetaxel | 2002–2013 | OS: No benefit adding docetaxel: HR 0.87, 95%CI 0.69–1.09; p = 0.218) |
| Attard et al. (2022) [8] | RCT 1: abiraterone trial RCT 2: abiraterone + enzalutamide trial STAMPEDE protocol | 774 | 1: ADT (control) vs. ADT + abiraterone and prednisolone (combi-therapy group) 2: ADT + (control) vs. ADT + abiraterone + prednisolone + enzalutamide (combi-therapy group) | 2011–2016 | Favours ADT + abiraterone + prednisolone 6 yr metastasis-free survival 82% (95%CI 79–85) (combination therapy) vs. 69% (95% CI 66–72) (control); HR 0.53, 95% CI 0.44–0.64, p < 0.0001) |
| Study Design | Number of pN1M0 Patients | Treatment Groups | Study Period | Outcome | |
|---|---|---|---|---|---|
| ADT as adjuvant treatment | |||||
| Messing et al. (2006) [26] | RCT ECOG 3886 | 98 | Immediate ADT vs. deferred ADT | 1988–1993 | Favour immediate ADT:Superior OS for immediate adjuvant ADT (HR 1.84, 95% CI 1.01–3.35, p = 0.04). Superior PCSS for immediate ADT (HR 4.09 (95%CI 1.76–9.49), p = 0.0004) |
| Wong et al. (2016) [27] | Retrospective, NCDB | 7225 | No adjuvant therapy ADT alone EBRT alone ADT + EBRT | 2004–2011 | Favours adjuvant EBRT + ADT: 5-yr OS rate, 85.2% (no therapy), 82.9% (ADT), 88.3% (EBRT), 88.8% (ADT + EBRT) (p ≤ 0.001) |
| Touijer et al. (2018) [5] | Retrospective, three institutions | 1338 | Observation vs. ADT alone vs. ADT + EBRT | 1988–2010 | CSS: Favours ADT compared to observation (HR: 0.64, 95% CI: 0.43–0.95, p = 0.027). OS: similar between ADT and observation, due to ADT increased risk of other-cause mortality (HR: 3.05, 95% CI: 1.45–6.40, p = 0.003) |
| Gupta et al. (2019) [28] | Retrospective | 8074 | Observation vs. ADT vs. ADT + EBRT | 2004–2013 | No difference in OS between ADT vs. observation (HR 1.01, 95%CI 0.87–1.18, p = 0.88) |
| ADT ± RT as adjuvant treatment | |||||
| Da Pozzo et al. (2009) [6] | Retrospective, single institution | 250 | ADT vs. ADT + EBRT | 1988–2002 | Favours adjuvant EBRT: 10 yr BCR-free survival 51% (ADT + EBRT) vs. 42% (ADT) (p = 0.11) 10 yr CSS rate 70% (ADT + EBRT) vs. 72% (ADT) (p = 0.22) |
| Briganti et al. (2011) [29] | Retrospective, two institutions | 364 | ADT vs. ADT + EBRT (matched analysis) | 1986–2002 | Favours adjuvant EBRT: 10 yr CSS 86% (ADT + EBRT) vs. 70% (ADT) p = 0.004 10 yr OS 74% (ADT + EBRT) vs. 55% (ADT) p < 0.001 |
| Kaplan et al. (2013) [30] | Retrospective, SEER | 577 | EBRT vs. no EBRT (both groups received ADT evenly) | 1995–2007 | No benefit of adjuvant EBRT: OM 5.35 (EBRT) vs. 3.77 (no EBRT) events per 100 person-years, p = 0.193 PCSM 2.39 (EBRT) vs. 1.30 (no EBRT), p = 0.354 |
| Abdollah et al. (2014) [31] | Retrospective, two institutions | 1107 | ADT vs. ADT + EBRT | 1988–2010 | Favours ADT with adjuvant EBRT 8 yr OM-free survival of 88% (ADT + EBRT) vs. 75% (ADT) (p < 0.01) 8-yr CSM-free survival 86% (ADT + EBRT) vs. 92%(ADT) (p = 0.08) |
| Rusthoven et al. (2014) [15] | Observational, SEER database | 2991 (pN1 after staging LND) | Local therapy (RP, EBRT or both) vs. no local therapy | 1995–2006 | Favours local therapy over no local therapy 10 yr OS rate 65% vs. 42% (p < 0.001) 10 yr PCSS 78% vs. 56% (p < 0.001) |
| Wong et al. (2016) [27] | Retrospective, NCDB | 7225 | No adjuvant therapy vs. ADT alone EBRT alone ADT + EBRT | 2004–2011 | Favours adjuvant EBRT + ADT 5-yr OS rate, 85.2% (no therapy), 82.9% (ADT), 88.3% (EBRT), 88.8% (ADT + EBRT) (p ≤ 0.001) |
| Jegadeesh et al. (2016) [32] | Retrospective, NCDB | 826 | ADT + EBRT ADT alone | 2003–2011 | Results favour ADT + EBRT Improved OS (HR 0.67, 95% CI 0.55–0.83, p < 0.001) |
| Van Hemelryk et al. (2016) [33] | Retrospective, case-matched | 69 | Case-matching of pN1 and pN0 after EBRT + ADT | 2006–? | 5-yr bRFS 65% (pN1) vs. 79% pN0 (p = 0.08) 5-yr cRFS 70% (pN1) vs. 83% (pN0) (p = 0.04) 5-yr PCSS 92% (pN1) vs. 93% (pN0) (p = 0.66) 5-yr OS 82% (pN1) vs. 80% (pN0) (p = 0.58) |
| Poelaert et al. (2016) [34] | Retrospective | 154 | ADT + whole pelvis EBRT | 2000–2016 | 5-year CSS 96% (±2%) 5-yr bRFS 67% (±5%) 5-yr cRFS 71% (±5%) 5-yr OS 89% (±3%) |
| Touijer et al. (2018) [5] | Retrospective, three institutions | 1338 | Observation vs. ADT alone vs. ADT + EBRT | 1988–2010 | Favours adjuvant ADT + EBRT over ADT HR 0.46 for OS (95% CI 0.32–0.66, p < 0.0001) Favours adjuvant ADT + EBRT over observation HR 0.41 for OS (95%CI 0.27–0.64, p < 0.0001) |
| Gupta et al. (2019) [28] | Retrospective | 8074 | Observation ADT ADT + EBRT | 2004–2013 | Results favour adjuvant ADT+ EBRT over ADT HR 0.76 for OS (95%CI 0.63–0.93, p = 0.007) Results favour adjuvant ADT+ EBRT over observation HR 0.77 for OS (95%CI 0.64–0.94, p = 0.008) |
| EBRT as adjuvant treatment | |||||
| Fonteyne et al. (2022) [35] | RCT PROPER trial | 69 | Prostate-only radiotherapy (arm A) vs. whole-pelvis radiotherapy (arm B) | 2016–2021 | Favours WPRT 3 yr 88% (PORT) vs. 92% (WPRT) (p = 0.31) 3-yr bRFS 79% (PORT) vs. 92% (WPRT) (p = 0.08) 3-yr OS 92% (PORT) vs. 93% (WPRT) (p = 0.61) |
| Tilki et al. (2021) [36] | Retrospective, five institutions | 1491 | Adjuvant vs. early salvage radiation therapy | 1989–2016 | Favours adjuvant EBRT in case of pN1 (HR 0.66, 95%CI 0.44–0.99; p = 0.04) |
| Chemotherapy as adjuvant treatment | |||||
| Ahlgren et al. (2018) [37] | RCT SPCG-12 trial | 55/459 (27 arm A and 28 arm B) | Arm A: docetaxel Arm B: surveillance | 2005–2010 | No difference in time to BCR > 0.5 ng/mL (p = 0.06) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zuur, L.G.; de Barros, H.A.; van der Mijn, K.J.C.; Vis, A.N.; Bergman, A.M.; Pos, F.J.; van Moorselaar, J.A.; van der Poel, H.G.; Vogel, W.V.; van Leeuwen, P.J. Treating Primary Node-Positive Prostate Cancer: A Scoping Review of Available Treatment Options. Cancers 2023, 15, 2962. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15112962
Zuur LG, de Barros HA, van der Mijn KJC, Vis AN, Bergman AM, Pos FJ, van Moorselaar JA, van der Poel HG, Vogel WV, van Leeuwen PJ. Treating Primary Node-Positive Prostate Cancer: A Scoping Review of Available Treatment Options. Cancers. 2023; 15(11):2962. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15112962
Chicago/Turabian StyleZuur, Lotte G., Hilda A. de Barros, Koen J. C. van der Mijn, André N. Vis, Andries M. Bergman, Floris J. Pos, Jeroen A. van Moorselaar, Henk G. van der Poel, Wouter V. Vogel, and Pim J. van Leeuwen. 2023. "Treating Primary Node-Positive Prostate Cancer: A Scoping Review of Available Treatment Options" Cancers 15, no. 11: 2962. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15112962