
Oncological and Peri-Operative Outcomes of Percutaneous Cryoablation of Renal Cell Carcinoma for Patients with Hereditary RCC Diseases—An Analysis of European Multi-Centre Prospective EuRECA Registry

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Characteristic of Included Patients
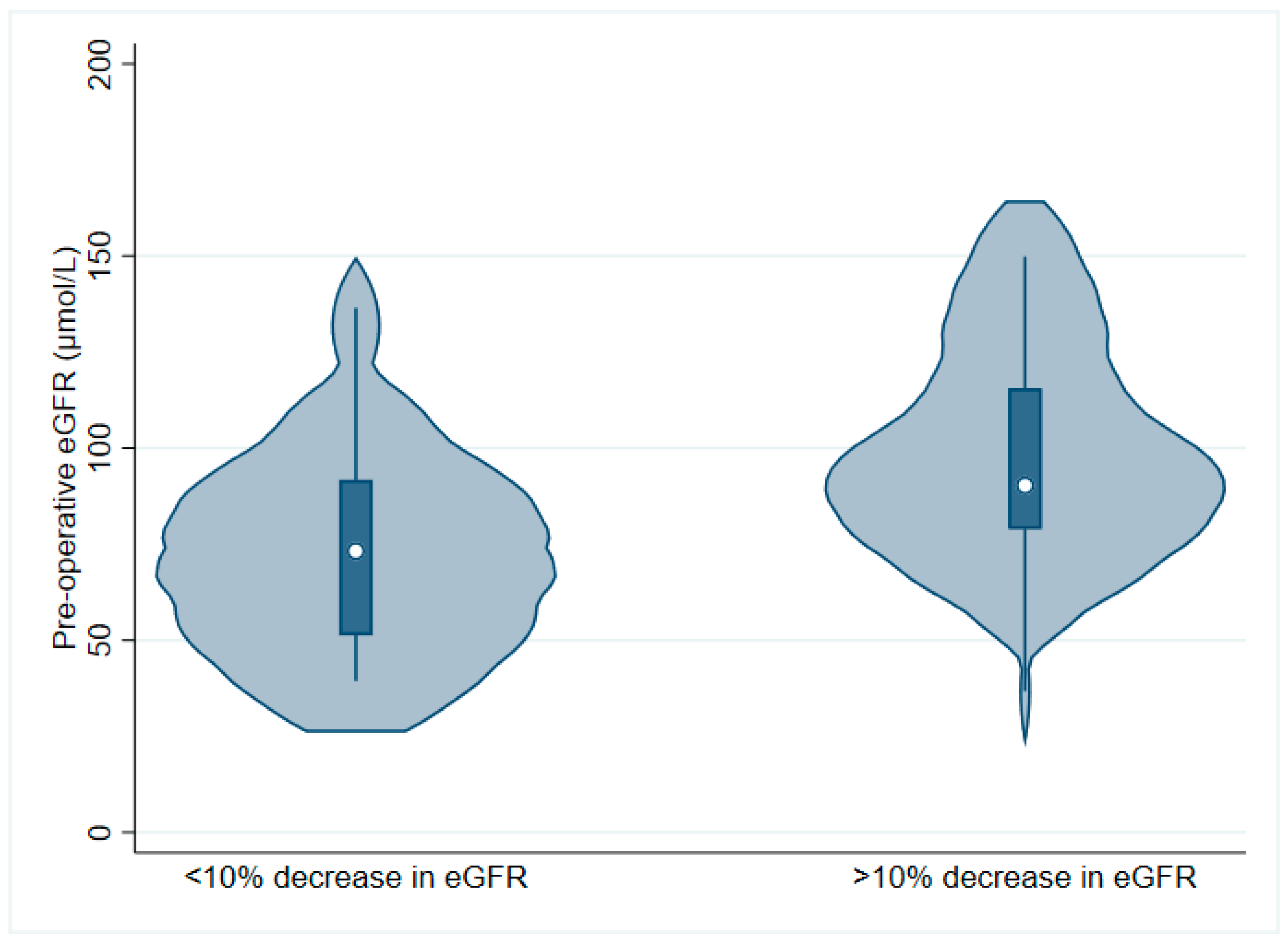
3.2. Treatment Efficacy, Peri-Operative Complications, and Change in eGFR
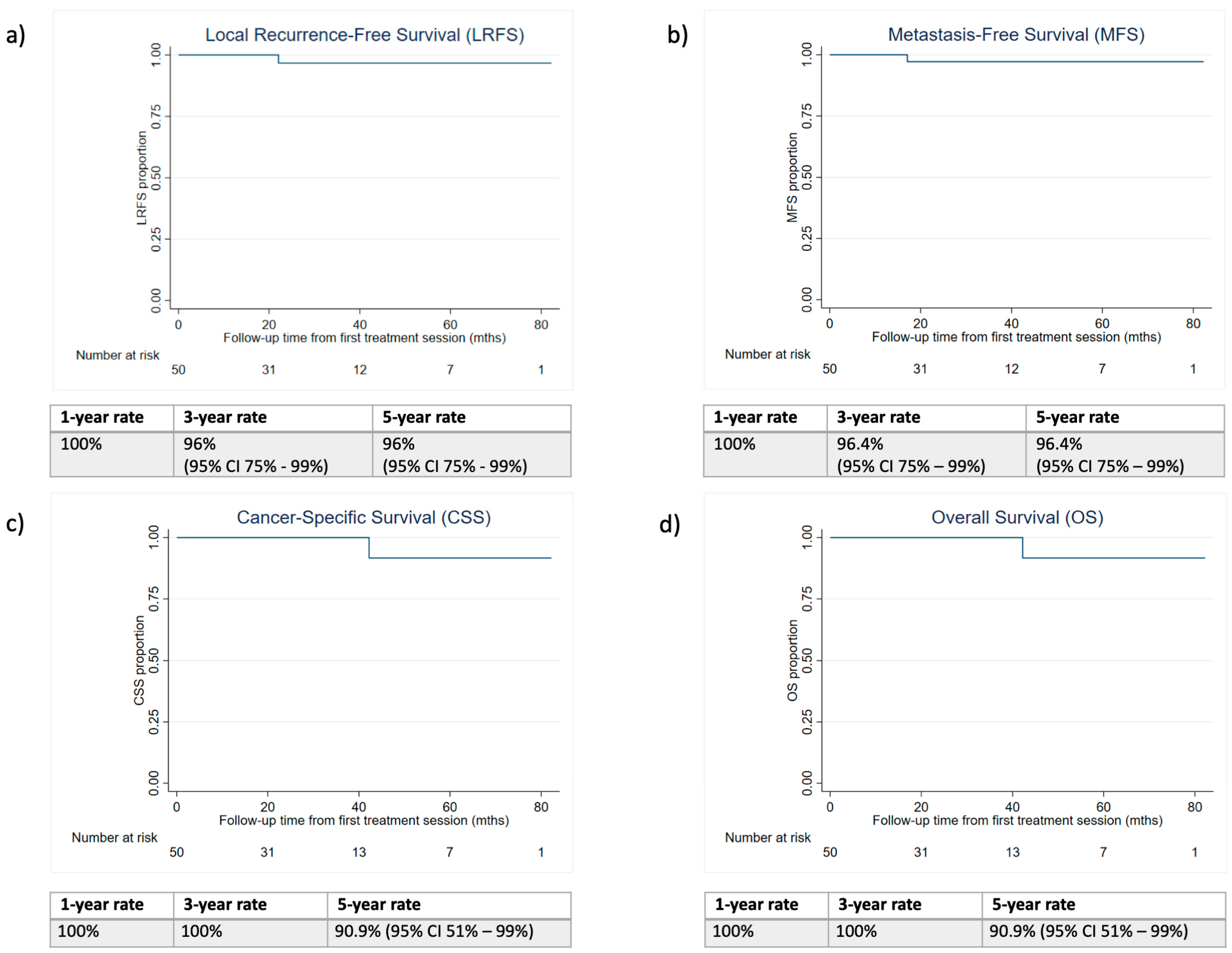
3.3. Oncological Durability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
| Hospital | Freq. | Percent |
|---|---|---|
| St James University Hospital, UK | 13 | 24.53 |
| University Hospital of Southampton, UK | 10 | 18.87 |
| Aarhus Universitetshospital, Denmark | 8 | 15.09 |
| Nouvel Hopital Civil, France | 6 | 11.32 |
| Gartnavel General Hospital, UK | 6 | 11.32 |
| Onze Lieve Vrouwe Gasthuis, Netherlands | 3 | 5.66 |
| Odense University Hospital | 3 | 5.66 |
| Southmead Hospital, UK | 2 | 3.77 |
| University College Hospital London, UK | 1 | 1.89 |
| Saint Louis Hospital, France | 1 | 1.89 |
| Total | 53 | 100 |
| Variable | >10% Reduction in eGFR | Mean | SD | p-Value (t-Test) | |
| Renal Nephrometry Score | Yes | 6.9 | 2.42 | 0.673 | |
| No | 7.24 | 1.68 | |||
| Age | Yes | 50.3 | 19.00 | 0.825 | |
| No | 51.59 | 11.05 | |||
| ASA score | Yes | 2 | 0.56 | 0.383 | |
| No | 2.24 | 0.82 | |||
| Pre-operative eGFR (μmol/L) | Yes | 93.89 | 31.82 | 0.074 | |
| No | 72.93 | 26.01 | |||
| Variable | Category | >10% reduction in eGFR | Frequency | Percentage | p-value (Chi-Square) |
| Sex | Male | Yes | 6 | 42.86 | 0.516 |
| No | 8 | 57.14 | |||
| Female | Yes | 4 | 30.77 | ||
| No | 9 | 69.23 | |||
| Inherited RCC syndromes | VHL | Yes | 4 | 22.22 | 0.065 |
| No | 14 | 77.78 | |||
| HLRCC | Yes | 1 | 100.00 | ||
| No | 0 | 0.00 | |||
| HPCC | Yes | 2 | 100.00 | ||
| No | 0 | 0.00 | |||
| BHD | Yes | 3 | 50.00 | ||
| No | 3 | 50.00 | |||
| Solitary kidney | Yes | Yes | 9 | 37.50 | 0.888 |
| No | 15 | 62.50 | |||
| No | Yes | 1 | 33.33 | ||
| No | 2 | 66.67 | |||
| Charlson Score | 0 | Yes | 2 | 28.57 | 0.590 |
| No | 5 | 71.43 | |||
| >1 | Yes | 8 | 40.00 | ||
| No | 12 | 60.00 | |||
| Hypertension | Yes | Yes | 5 | 55.56 | 0.159 |
| No | 4 | 44.44 | |||
| No | Yes | 5 | 27.78 | ||
| No | 13 | 72.22 | |||
| Smoking | Yes | Yes | 5 | 62.50 | 0.075 |
| No | 1 | 37.50 | |||
| No | Yes | 5 | 26.32 | ||
| No | 14 | 73.68 | |||
| Obesity | BMI > 30 | Yes | 8 | 40.00 | 0.590 |
| No | 12 | 60.00 | |||
| BMI < 30 | Yes | 2 | 28.57 | ||
| No | 5 | 71.43 | |||
References
- Menko, F.H.; Maher, E.R. Diagnosis and Management of Hereditary Renal Cell Cancer. Recent Results Cancer Res. 2016, 205, 85–104. [Google Scholar]
- Barrisford, G.W.; Singer, E.A.; Rosner, I.L.; Linehan, W.M.; Bratslavsky, G. Familial Renal Cancer: Molecular Genetics and Surgical Management. Int. J. Surg. Oncol. 2011, 2011, 658767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haas, N.B.; Nathanson, K.L. Hereditary kidney cancer syndromes. Adv. Chronic Kidney Dis. 2014, 21, 81–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, V.W.; Abul, A.; Osman, F.H.; Ng, H.H.; Wang, K.; Yuan, Y.; Cartledge, J.; Wah, T.M. Ablative Therapies versus Partial Nephrectomy for Small Renal Masses–A systematic review and meta-analysis of observational studies. Int. J. Surg. 2021, 97, 106194. [Google Scholar] [CrossRef]
- Chan, V.W.-S.; Osman, F.H.; Cartledge, J.; Gregory, W.; Kimuli, M.; Vasudev, N.S.; Ralph, C.; Jagdev, S.; Bhattarai, S.; Smith, J.; et al. Long-term outcomes of image-guided ablation and laparoscopic partial nephrectomy for T1 renal cell carcinoma. Eur. Radiol. 2022, 32, 5811–5820. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.; Sudarshan, S.; Liu, J.; Linehan, W.M.; Pinto, P.A.; Bratslavsky, G. Feasibility and Outcomes of Repeat Partial Nephrectomy. J. Urol. 2008, 180, 89–93. [Google Scholar] [CrossRef] [Green Version]
- Bratslavsky, G.; Liu, J.J.; Johnson, A.D.; Sudarshan, S.; Choyke, P.L.; Linehan, W.M.; Pinto, P.A. Salvage partial nephrectomy for hereditary renal cancer: Feasibility and outcomes. J. Urol. 2008, 179, 67–70. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Bensalah, K.; Bex, A.; Giles, R.H.; Hora, M.; Kuczyk, M.A.; Lam, T.; Marconi, L.; Merseburger, A.S.; et al. EAU Guidelines on Renal Cell Carcinoma 2020; European Association of Urology Guidelines 2020 Edition; European Association of Urology Guidelines Office: Arnhem, The Netherlands, 2020. [Google Scholar]
- Chan, V.W.-S.; Lenton, J.; Smith, J.; Jagdev, S.; Ralph, C.; Vasudev, N.; Bhattarai, S.; Lewington, A.; Kimuli, M.; Cartledge, J.; et al. Multimodal image-guided ablation on management of renal cancer in Von-Hippel-Lindau syndrome patients from 2004 to 2021 at a specialist centre: A longitudinal observational study. Eur. J. Surg. Oncol. 2022, 48, 672–679. [Google Scholar] [CrossRef]
- Allasia, M.; Soria, F.; Battaglia, A.; Gazzera, C.; Calandri, M.; Caprino, M.P.; Lucatello, B.; Velrti, A.; Maccario, M.; Pasini, B.; et al. Radiofrequency Ablation for Renal Cancer in Von Hippel–Lindau Syndrome Patients: A Prospective Cohort Analysis. Clin. Genitourin. Cancer 2018, 16, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA A Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Joly, D.; Méjean, A.; Corréas, J.M.; Timsit, M.O.; Verkarre, V.; Deveaux, S.; Landais, P.; Grünfeld, J.P.; Richard, S. Progress in nephron sparing therapy for renal cell carcinoma and von Hippel-Lindau disease. J. Urol. 2011, 185, 2056–2060. [Google Scholar] [CrossRef]
- Andrews, J.R.; Atwell, T.; Schmit, G.; Lohse, C.M.; Kurup, A.N.; Weisbrod, A.; Callstrom, M.R.; Cheville, J.C.; Boorjian, S.A.; Leibovich, B.C.; et al. Oncologic Outcomes Following Partial Nephrectomy and Percutaneous Ablation for cT1 Renal Masses. Eur. Urol. 2019, 76, 244–251. [Google Scholar] [CrossRef]
- Psutka, S.P.; Feldman, A.S.; McDougal, W.S.; McGovern, F.J.; Mueller, P.; Gervais, D.A. Long-Term Oncologic Outcomes after Radiofrequency Ablation for T1 Renal Cell Carcinoma. Eur. Urol. 2013, 63, 486–492. [Google Scholar] [CrossRef]
- Wah, T.M.; Irving, H.C.; Gregory, W.; Cartledge, J.; Joyce, A.D.; Selby, P.J. Radiofrequency ablation (RFA) of renal cell carcinoma (RCC): Experience in 200 tumours. BJU Int. 2014, 113, 416–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsui, Y.; Hiraki, T.; Gobara, H.; Iguchi, T.; Tomita, K.; Uka, M.; Araki, M.; Nasu, Y.; Furuya, M.; Kanazawa, S. Percutaneous thermal ablation for renal cell carcinoma in patients with Birt–Hogg–Dubé syndrome. Diagn. Interv. Imaging 2019, 100, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Shingleton, W.B.; Sewell, P.E., Jr. Percutaneous renal cryoablation of renal tumors in patients with von Hippel-Lindau disease. J. Urol. 2002, 167, 1268–1270. [Google Scholar] [CrossRef]
- Buy, X.; Lang, H.; Garnon, J.; Sauleau, E.; Roy, C.; Gangi, A. Percutaneous Renal Cryoablation: Prospective Experience Treating 120 Consecutive Tumors. Am. J. Roentgenol. 2013, 201, 1353–1361. [Google Scholar] [CrossRef] [PubMed]
- Weisbrod, A.J.; Atwell, T.D.; Frank, I.; Callstrom, M.R.; Farrell, M.A.; Mandrekar, J.N.; Charboneau, J.W. Percutaneous Cryoablation of Masses in a Solitary Kidney. Am. J. Roentgenol. 2010, 194, 1620–1625. [Google Scholar] [CrossRef]
- Breen, D.J.; King, A.J.; Patel, N.; Lockyer, R.; Hayes, M. Image-guided Cryoablation for Sporadic Renal Cell Carcinoma: Three- and 5-year Outcomes in 220 Patients with Biopsy-proven Renal Cell Carcinoma. Radiology 2018, 289, 554–561. [Google Scholar] [CrossRef]
- Greco, F.; Cirimele, V.; Mallio, C.; Zobel, B.; Grasso, R. Increased visceral adipose tissue in male patients with clear cell renal cell carcinoma. Clin. Cancer Investig. J. 2018, 7, 132–136. [Google Scholar] [CrossRef]
- Sorce, G.; Hoeh, B.; Hohenhorst, L.; Panunzio, A.; Tappero, S.; Tian, Z.; Kokorovic, A.; Larcher, A.; Capitanio, U.; Tilki, D.; et al. Cancer-specific Mortality after Cryoablation vs Heat-based Thermal Ablation in T1a Renal Cell Carcinoma. J. Urol. 2023, 209, 81–88. [Google Scholar] [CrossRef] [PubMed]

| No. of Patients (n = 53) | ||
|---|---|---|
| Variable | Frequency | % |
| Age (years) | ||
| <30 | 1 | 1.9 |
| 30–39 | 15 | 28.3 |
| 40–49 | 14 | 26.4 |
| 50–59 | 10 | 18.9 |
| 60–69 | 9 | 17.0 |
| 70–79 | 3 | 5.7 |
| >80 | 1 | 1.9 |
| Sex | ||
| Male | 30 | 56.5 |
| Female | 23 | 43.4 |
| Race | ||
| Caucasian | 52 | 98.1 |
| Asian | 1 | 1.9 |
| Type of hereditary disease | ||
| VHL | 41 | 77.4 |
| HLRCC | 1 | 1.9 |
| HPRC | 2 | 3.8 |
| BHD | 9 | 17.0 |
| Family history of renal cancer | ||
| Unknown | 26 | 49.0 |
| Yes | 18 | 34.0 |
| No | 9 | 17.0 |
| Solitary kidney | ||
| No | 44 | 83 |
| Yes | 9 | 17 |
| Mean | SD | |
| No. of tumours per patient | 1.6 | 1.0 |
| Charlson Comorbidity Index | 2.0 | 1.9 |
| Baseline eGFR (mL/min/1.73 m2) | 88.4 | 44.7 |
| Follow-up duration (months) | 30.4 | 22.0 |
| No. of tumours (n = 85) | ||
| Frequency | % | |
| Laterality | ||
| Right | 42 | 49.4 |
| Left | 43 | 50.6 |
| Mean | SD | |
| Size of tumour (cm) | 2.46 | 1.0 |
| R.E.N.A.L. nephrometry score | 6.9 | 1.9 |
| Previous Treatment for RCCs on Same Kidney (n = 26) | Previous Treatment for RCCs on Contralateral Kidney (n = 29) | ||
|---|---|---|---|
| Treatment | No. of Patients, n | Treatment | No. of Patients, n |
| PN only | 8 | PN only | 6 |
| PN + PCA | 5 | PN + PCA | 2 |
| PN + RFA | 1 | PN + RFA | 1 |
| PN + RFA + PCA | 1 | PN + IRE | 1 |
| PCA only | 6 | PCA only | 7 |
| PCA + RFA | 2 | PCA + RFA | 2 |
| RFA only | 3 | PCA + IRE | 1 |
| RN only | 8 | ||
| Unknown | 1 | ||
| Variable | >25% Reduction in eGFR | Mean | SD | p-Value (t-Test) | |
| Renal Nephrometry Score | Yes | 9.5 | 0.5 | 0.071 | |
| No | 6.92 | 0.38 | |||
| Age (years) | Yes | 54.5 | 24.5 | 0.732 | |
| No | 50.84 | 2.58 | |||
| ASA score | Yes | 2.5 | 0.71 | 0.446 | |
| No | 2.12 | 0.67 | |||
| Pre-operative eGFR (mL/min/1.73 m2) | Yes | 143.78 | 6.04 | 0.001 | |
| No | 75.65 | 4.84 | |||
| Variable | Category | >25% reduction in eGFR | Frequency | Percentage | p-value (Chi-Square) |
| Sex | Male | Yes | 0 | 0 | 0.127 |
| No | 14 | 100 | |||
| Female | Yes | 2 | 15.38 | ||
| No | 11 | 84.62 | |||
| Inherited RCC syndromes | VHL | Yes | 1 | 5.56 | 0.115 |
| No | 17 | 94.44 | |||
| HLRCC | Yes | 0 | 0 | ||
| No | 1 | 100 | |||
| HPCC | Yes | 1 | 50.00 | ||
| No | 1 | 50.00 | |||
| BHD | Yes | 0 | 0 | ||
| No | 6 | 100 | |||
| Solitary kidney | Yes | Yes | 0 | 0 | 0.603 |
| No | 3 | 100 | |||
| No | Yes | 2 | 8.33 | ||
| No | 22 | 91.67 | |||
| Charlson Score | 0 | Yes | 1 | 14.29 | 0.419 |
| No | 6 | 85.71 | |||
| >1 | Yes | 1 | 5.00 | ||
| No | 19 | 95.00 | |||
| Hypertension | Yes | Yes | 2 | 22.22 | 0.038 |
| No | 7 | 77.78 | |||
| No | Yes | 0 | 0.00 | ||
| No | 18 | 100.00 | |||
| Smoking | Yes | Yes | 1 | 12.50 | 0.512 |
| No | 7 | 87.50 | |||
| No | Yes | 1 | 5.26 | ||
| No | 18 | 94.74 | |||
| Obesity | BMI > 30 | Yes | 0 | 0.00 | 0.385 |
| No | 7 | 100.00 | |||
| BMI < 30 | Yes | 2 | 10.00 | ||
| No | 18 | 90.00 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osman, F.H.; Chan, V.W.-S.; Breen, D.J.; King, A.; Nielsen, T.K.; Garnon, J.; Alcorn, D.; Lagerveld, B.; Graumann, O.; Keeley, F.X., Jr.; et al. Oncological and Peri-Operative Outcomes of Percutaneous Cryoablation of Renal Cell Carcinoma for Patients with Hereditary RCC Diseases—An Analysis of European Multi-Centre Prospective EuRECA Registry. Cancers 2023, 15, 3322. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15133322
Osman FH, Chan VW-S, Breen DJ, King A, Nielsen TK, Garnon J, Alcorn D, Lagerveld B, Graumann O, Keeley FX Jr., et al. Oncological and Peri-Operative Outcomes of Percutaneous Cryoablation of Renal Cell Carcinoma for Patients with Hereditary RCC Diseases—An Analysis of European Multi-Centre Prospective EuRECA Registry. Cancers. 2023; 15(13):3322. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15133322
Chicago/Turabian StyleOsman, Filzah Hanis, Vinson Wai-Shun Chan, David J. Breen, Alexander King, Tommy Kjærgaard Nielsen, Julien Garnon, Des Alcorn, Brunolf Lagerveld, Ole Graumann, Francis Xavier Keeley, Jr., and et al. 2023. "Oncological and Peri-Operative Outcomes of Percutaneous Cryoablation of Renal Cell Carcinoma for Patients with Hereditary RCC Diseases—An Analysis of European Multi-Centre Prospective EuRECA Registry" Cancers 15, no. 13: 3322. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15133322