
Systematic Review of Photodynamic Therapy in Gliomas

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
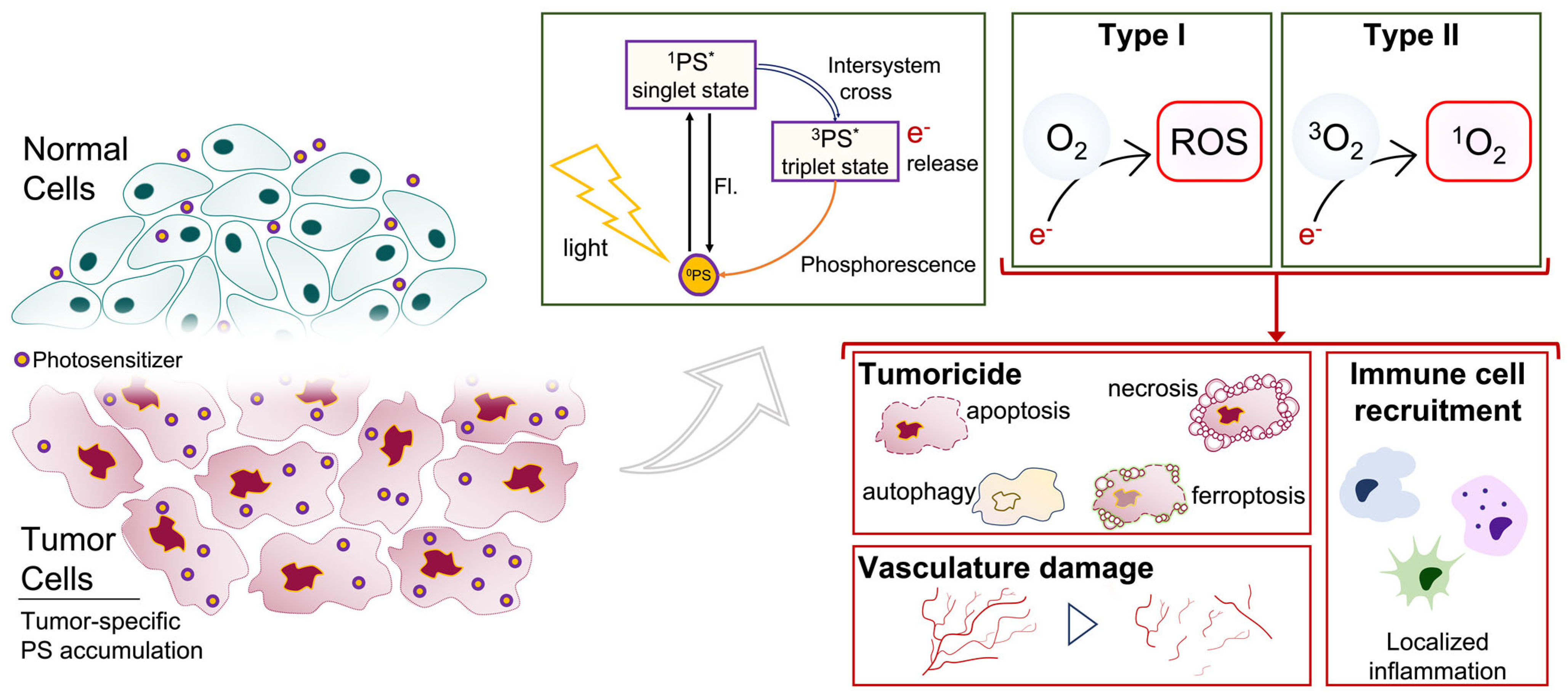
2. Photodynamic-Therapy-Mediated Tumoricidal Effect
2.1. PDT Induces Cell Death following PS Uptake, Accumulation, and Activation
2.2. PDT Controls Glioma Stem Cell (GSC) Processes
2.3. PDT Modulates Neurovasculature: Disruption of the Blood–Brain Barrier (BBB) and Destruction of Tumor Vasculature
2.4. PDT Stimlates Anti-Tumor Immunity
3. Photosensitizers
3.1. First Generation: Naturally Occurring Porphyrins
3.2. Second Generation: Increased Singlet Oxygen Potency
Combining Second-Generation PDT with Standard Therapies
3.3. Third-Generation PS: Increased Tumor Selectivity
4. Optimizing Light Delivery
5. PDT in Other CNS Tumors
6. Limitations
6.1. Limitations of PDT and Its Synergistic Agents
6.2. PDT Efficacy Negatively Influenced by the Harsh Glioma Microenvironment
6.3. Innate PDT Resistance
6.4. Peri-Tumor Edema Limits PDT Efficacy
6.5. PDT Drug Interactions and Synergistic Agents
7. Conclusions and Future Directions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Marsden, P.A. Angiogenesis in Glioblastoma. N. Engl. J. Med. 2013, 369, 1561–1563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.B.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of Radiotherapy with Concomitant and Adjuvant Temozolomide versus Radiotherapy Alone on Survival in Glioblastoma in a Randomised Phase III Study: 5-Year Analysis of the EORTC-NCIC Trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [Green Version]
- Majewska, P.; Ioannidis, S.; Raza, M.H.; Tanna, N.; Bulbeck, H.; Williams, M. Postprogression Survival in Patients with Glioblastoma Treated with Concurrent Chemoradiotherapy: A Routine Care Cohort Study. CNS Oncol. 2017, 6, 307–313. [Google Scholar] [CrossRef]
- Parker, N.R.; Khong, P.; Parkinson, J.F.; Howell, V.M.; Wheeler, H.R. Molecular Heterogeneity in Glioblastoma: Potential Clinical Implications. Front. Oncol. 2015, 5, 55. [Google Scholar] [CrossRef]
- DeCordova, S.; Shastri, A.; Tsolaki, A.G.; Yasmin, H.; Klein, L.; Singh, S.K.; Kishore, U. Molecular Heterogeneity and Immunosuppressive Microenvironment in Glioblastoma. Front. Immunol. 2020, 11, 1402. [Google Scholar] [CrossRef] [PubMed]
- Mallick, S.; Benson, R.; Hakim, A.; Rath, G.K. Management of Glioblastoma after Recurrence: A Changing Paradigm. J. Egypt. Natl. Cancer Inst. 2016, 28, 199–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallego, O. Nonsurgical Treatment of Recurrent Glioblastoma. Curr. Oncol. 2015, 22, 273–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weller, M.; Cloughesy, T.; Perry, J.R.; Wick, W. Standards of Care for Treatment of Recurrent Glioblastoma—Are We There Yet? Neuro. Oncol. 2013, 15, 4–27. [Google Scholar] [CrossRef] [Green Version]
- dos Santos, M.A.; Pignon, J.-P.; Blanchard, P.; Lefeuvre, D.; Levy, A.; Touat, M.; Louvel, G.; Dhermain, F.; Soria, J.-C.; Deutsch, E.; et al. Systematic Review and Meta-Analysis of Phase I/II Targeted Therapy Combined with Radiotherapy in Patients with Glioblastoma Multiforme: Quality of Report, Toxicity, and Survival. J. Neurooncol. 2015, 123, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Su, J.; Cai, M.; Li, W.; Hou, B.; He, H.; Ling, C.; Huang, T.; Liu, H.; Guo, Y. Molecularly Targeted Drugs Plus Radiotherapy and Temozolomide Treatment for Newly Diagnosed Glioblastoma: A Meta-Analysis and Systematic Review. Oncol. Res. Featur. Preclin. Clin. Cancer Ther. 2016, 24, 117–128. [Google Scholar] [CrossRef]
- Laws, E.R., Jr.; Cortese, D.A.; Kinsey, J.H.; Eagan, R.T.; Anderson, R.E. Photoradiation Therapy in the Treatment of Malignant Brain Tumors: A Phase I (feasibility) Study. Neurosurgery 1981, 9, 672–678. [Google Scholar] [CrossRef]
- Dougherty, T.J.; Kaufman, J.E.; Goldfarb, A.; Weishaupt, K.R.; Boyle, D.; Mittleman, A. Photoradiation Therapy for the Treatment of Malignant Tumors. Cancer Res. 1978, 38, 2628–2635. [Google Scholar]
- da Silva, B.A.; Nazarkovsky, M.; Padilla-Chavarría, H.I.; Mendivelso, E.A.C.; de Mello, H.L.; de Nogueira, C.S.C.; Carvalho, R.D.S.; Cremona, M.; Zaitsev, V.; Xing, Y.; et al. Novel Scintillating Nanoparticles for Potential Application in Photodynamic Cancer Therapy. Pharmaceutics 2022, 14, 2258. [Google Scholar] [CrossRef] [PubMed]
- Vedunova, M.; Turubanova, V.; Vershinina, O.; Savyuk, M.; Efimova, I.; Mishchenko, T.; Raedt, R.; Vral, A.; Vanhove, C.; Korsakova, D.; et al. DC Vaccines Loaded with Glioma Cells Killed by Photodynamic Therapy Induce Th17 Anti-Tumor Immunity and Provide a Four-Gene Signature for Glioma Prognosis. Cell Death Dis. 2022, 13, 1062. [Google Scholar] [CrossRef]
- Plaetzer, K.; Krammer, B.; Berlanda, J.; Berr, F.; Kiesslich, T. Photophysics and Photochemistry of Photodynamic Therapy: Fundamental Aspects. Lasers Med. Sci. 2009, 24, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Hirschberg, H.; Berg, K.; Peng, Q. Photodynamic Therapy Mediated Immune Therapy of Brain Tumors. Neuroimmunol. Neuroinflammation 2018, 5, 27. [Google Scholar] [CrossRef]
- Cramer, S.W.; Chen, C.C. Photodynamic Therapy for the Treatment of Glioblastoma. Front. Surg. 2019, 6, 81. [Google Scholar] [CrossRef] [Green Version]
- Castano, A.P.; Mroz, P.; Hamblin, M.R. Photodynamic Therapy and Anti-Tumour Immunity. Nat. Rev. Cancer 2006, 6, 535–545. [Google Scholar] [CrossRef] [Green Version]
- Dougherty, T.J.; Gomer, C.J.; Henderson, B.W.; Jori, G.; Kessel, D.; Korbelik, M.; Moan, J.; Peng, Q. Photodynamic Therapy. J. Natl. Cancer Inst. 1998, 90, 889–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostinis, P.; Berg, K.; Cengel, K.A.; Foster, T.H.; Girotti, A.W.; Gollnick, S.O.; Hahn, S.M.; Hamblin, M.R.; Juzeniene, A.; Kessel, D.; et al. Photodynamic Therapy of Cancer: An Update. CA Cancer J. Clin. 2011, 61, 250–281. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Lovell, J.F.; Yoon, J.; Chen, X. Clinical Development and Potential of Photothermal and Photodynamic Therapies for Cancer. Nat. Rev. Clin. Oncol. 2020, 17, 657–674. [Google Scholar] [CrossRef] [PubMed]
- Miki, Y.; Akimoto, J.; Moritake, K.; Hironaka, C.; Fujiwara, Y. Photodynamic Therapy Using Talaporfin Sodium Induces Concentration-Dependent Programmed Necroptosis in Human Glioblastoma T98G Cells. Lasers Med. Sci. 2015, 30, 1739–1745. [Google Scholar] [CrossRef]
- Castano, A.P.; Demidova, T.N.; Hamblin, M.R. Mechanisms in Photodynamic Therapy: Part One-Photosensitizers, Photochemistry and Cellular Localization. Photodiagnosis Photodyn. Ther. 2004, 1, 279–293. [Google Scholar] [CrossRef] [Green Version]
- Castano, A.P.; Demidova, T.N.; Hamblin, M.R. Mechanisms in Photodynamic Therapy: Part Two—Cellular Signaling, Cell Metabolism and Modes of Cell Death. Photodiagnosis Photodyn. Ther. 2005, 2, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Castano, A.P.; Demidova, T.N.; Hamblin, M.R. Mechanisms in Photodynamic Therapy: Part three—Photosensitizer Pharmacokinetics, Biodistribution, Tumor Localization and Modes of Tumor Destruction. Photodiagnosis Photodyn. Ther. 2005, 2, 91–106. [Google Scholar] [CrossRef] [Green Version]
- Mishchenko, T.; Balalaeva, I.; Gorokhova, A.; Vedunova, M.; Krysko, D.V. Which Cell Death Modality Wins the Contest for Photodynamic Therapy of Cancer? Cell Death Dis. 2022, 13, 455. [Google Scholar] [CrossRef]
- Stylli, S.S.; Kaye, A.H. Photodynamic Therapy of Cerebral Glioma—A Review Part I—A Biological Basis. J. Clin. Neurosci. 2006, 13, 615–625. [Google Scholar] [CrossRef]
- Miki, Y.; Akimoto, J.; Hiranuma, M.; Fujiwara, Y. Effect of Talaporfin Sodium-Mediated Photodynamic Therapy on Cell Death Modalities in Human Glioblastoma T98G Cells. J. Toxicol. Sci. 2014, 39, 821–827. [Google Scholar] [CrossRef] [Green Version]
- Shui, S.; Zhao, Z.; Wang, H.; Conrad, M.; Liu, G. Non-Enzymatic Lipid Peroxidation Initiated by Photodynamic Therapy Drives a Distinct Ferroptosis-like Cell Death Pathway. Redox Biol. 2021, 45, 102056. [Google Scholar] [CrossRef] [PubMed]
- Zhu, T.; Shi, L.; Yu, C.; Dong, Y.; Qiu, F.; Shen, L.; Qian, Q.; Zhou, G.; Zhu, X. Ferroptosis Promotes Photodynamic Therapy: Supramolecular Photosensitizer-Inducer Nanodrug for Enhanced Cancer Treatment. Theranostics 2019, 9, 3293–3307. [Google Scholar] [CrossRef]
- Schimanski, A.; Ebbert, L.; Sabel, M.C.; Finocchiaro, G.; Lamszus, K.; Ewelt, C.; Etminan, N.; Fischer, J.C.; Sorg, R.V. Human Glioblastoma Stem-like Cells Accumulate Protoporphyrin IX When Subjected to Exogenous 5-Aminolaevulinic Acid, Rendering Them Sensitive to Photodynamic Treatment. J. Photochem. Photobiol. B Biol. 2016, 163, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Fujishiro, T.; Nonoguchi, N.; Pavliukov, M.; Ohmura, N.; Kawabata, S.; Park, Y.; Kajimoto, Y.; Ishikawa, T.; Nakano, I.; Kuroiwa, T. 5-Aminolevulinic Acid-Mediated Photodynamic Therapy Can Target Human Glioma Stem-like Cells Refractory to Antineoplastic Agents. Photodiagnosis Photodyn. Ther. 2018, 24, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Auffinger, B.; Tobias, A.L.; Han, Y.; Lee, G.; Guo, D.; Dey, M.; Lesniak, M.S.; Ahmed, A.U. Conversion of Differentiated Cancer Cells into Cancer Stem-like Cells in a Glioblastoma Model after Primary Chemotherapy. Cell Death Differ. 2014, 21, 1119–1131. [Google Scholar] [CrossRef]
- Jackson, M.; Hassiotou, F.; Nowak, A. Glioblastoma Stem-like Cells: At the Root of Tumor Recurrence and a Therapeutic Target. Carcinogenesis 2015, 36, 177–185. [Google Scholar] [CrossRef]
- Fisher, C.; Obaid, G.; Niu, C.; Foltz, W.; Goldstein, A.; Hasan, T.; Lilge, L. Liposomal Lapatinib in Combination with Low-Dose Photodynamic Therapy for the Treatment of Glioma. J. Clin. Med. Res. 2019, 8, 2214. [Google Scholar] [CrossRef] [Green Version]
- Semyachkina-Glushkovskaya, O.; Kurths, J.; Borisova, E.; Sokolovski, S.; Mantareva, V.; Angelov, I.; Shirokov, A.; Navolokin, N.; Shushunova, N.; Khorovodov, A.; et al. Photodynamic Opening of Blood-Brain Barrier. Biomed. Opt. Express 2017, 8, 5040–5048. [Google Scholar] [CrossRef]
- Madsen, S.J.; Gach, H.M.; Hong, S.J.; Uzal, F.A.; Peng, Q.; Hirschberg, H. Increased Nanoparticle-Loaded Exogenous Macrophage Migration into the Brain Following PDT-Induced Blood-Brain Barrier Disruption. Lasers Surg. Med. 2013, 45, 524–532. [Google Scholar] [CrossRef] [Green Version]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- Dolmans, D.E.J.G.J.; Fukumura, D.; Jain, R.K. Photodynamic Therapy for Cancer. Nat. Rev. Cancer 2003, 3, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Yi, W.; Xu, H.-T.; Tian, D.-F.; Wu, L.-Q.; Zhang, S.-Q.; Wang, L.; Ji, B.-W.; Zhu, X.-N.; Okechi, H.; Liu, G.; et al. Photodynamic Therapy Mediated by 5-Aminolevulinic Acid Suppresses Gliomas Growth by Decreasing the Microvessels. J. Huazhong Univ. Sci. Technolog. Med. Sci. 2015, 35, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.S.; Shin, H.; Han, J.; Na, K. Combination of Photodynamic Therapy (PDT) and Anti-Tumor Immunity in Cancer Therapy. J. Pharm. Investig. 2018, 48, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falk-Mahapatra, R.; Gollnick, S.O. Photodynamic Therapy and Immunity: An Update. Photochem. Photobiol. 2020, 96, 550–559. [Google Scholar] [CrossRef]
- Etminan, N.; Peters, C.; Ficnar, J.; Anlasik, S.; Bünemann, E.; Slotty, P.J.; Hänggi, D.; Steiger, H.-J.; Sorg, R.V.; Stummer, W. Modulation of Migratory Activity and Invasiveness of Human Glioma Spheroids Following 5-Aminolevulinic Acid-Based Photodynamic Treatment. Laboratory Investigation. J. Neurosurg. 2011, 115, 281–288. [Google Scholar] [CrossRef]
- Li, F.; Cheng, Y.; Lu, J.; Hu, R.; Wan, Q.; Feng, H. Photodynamic Therapy Boosts Anti-Glioma Immunity in Mice: A Dependence on the Activities of T Cells and Complement C3. J. Cell. Biochem. 2011, 112, 3035–3043. [Google Scholar] [CrossRef]
- Etminan, N.; Peters, C.; Lakbir, D.; Bünemann, E.; Börger, V.; Sabel, M.C.; Hänggi, D.; Steiger, H.-J.; Stummer, W.; Sorg, R.V. Heat-Shock Protein 70-Dependent Dendritic Cell Activation by 5-Aminolevulinic Acid-Mediated Photodynamic Treatment of Human Glioblastoma Spheroids in Vitro. Br. J. Cancer 2011, 105, 961–969. [Google Scholar] [CrossRef] [Green Version]
- Shibata, S.; Shinozaki, N.; Suganami, A.; Ikegami, S.; Kinoshita, Y.; Hasegawa, R.; Kentaro, H.; Okamoto, Y.; Aoki, I.; Tamura, Y.; et al. Photo-Immune Therapy with Liposomally Formulated Phospholipid-Conjugated Indocyanine Green Induces Specific Antitumor Responses with Heat Shock Protein-70 Expression in a Glioblastoma Model. Oncotarget 2019, 10, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Turubanova, V.D.; Balalaeva, I.V.; Mishchenko, T.A.; Catanzaro, E.; Alzeibak, R.; Peskova, N.N.; Efimova, I.; Bachert, C.; Mitroshina, E.V.; Krysko, O.; et al. Immunogenic Cell Death Induced by a New Photodynamic Therapy Based on Photosens and Photodithazine. J. Immunother. Cancer 2019, 7, 350. [Google Scholar] [CrossRef]
- Helbig, D.; Simon, J.C.; Paasch, U. Photodynamic Therapy and the Role of Heat Shock Protein 70. Int. J. Hyperth. 2011, 27, 802–810. [Google Scholar] [CrossRef]
- Zhou, F.; Xing, D.; Chen, W.R. Regulation of HSP70 on Activating Macrophages Using PDT-Induced Apoptotic Cells. Int. J. Cancer 2009, 125, 1380–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kammerer, R.; Buchner, A.; Palluch, P.; Pongratz, T.; Oboukhovskij, K.; Beyer, W.; Johansson, A.; Stepp, H.; Baumgartner, R.; Zimmermann, W. Induction of Immune Mediators in Glioma and Prostate Cancer Cells by Non-Lethal Photodynamic Therapy. PLoS ONE 2011, 6, e21834. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Zhu, S.; Yang, B.; Chen, C.; Chen, S.; Liu, Y.; Nie, X.; Hao, L.; Wang, Z.; Sun, J.; et al. The Destruction Of Laser-Induced Phase-Transition Nanoparticles Triggered By Low-Intensity Ultrasound: An Innovative Modality To Enhance The Immunological Treatment Of Ovarian Cancer Cells. Int. J. Nanomed. 2019, 14, 9377–9393. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.; Zhang, F.; Deng, H.; Lin, L.; Wang, S.; Kang, F.; Yu, G.; Lau, J.; Tian, R.; Zhang, M.; et al. Smart Nanovesicle-Mediated Immunogenic Cell Death through Tumor Microenvironment Modulation for Effective Photodynamic Immunotherapy. ACS Nano 2020, 14, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Ni, J.; Song, J.; Wang, B.; Hua, H.; Zhu, H.; Guo, X.; Xiong, S.; Zhao, Y. Dendritic Cell Vaccine for the Effective Immunotherapy of Breast Cancer. Biomed. Pharmacother. 2020, 126, 110046. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Liu, L.; Liang, R.; Zhou, H.; Pan, H.; Zhang, S.; Cai, L. Tumor-Targeted Nanoplatform for in Situ Oxygenation-Boosted Immunogenic Phototherapy of Colorectal Cancer. Acta Biomater. 2020, 104, 188–197. [Google Scholar] [CrossRef]
- Wang, H.; Wang, K.; He, L.; Liu, Y.; Dong, H.; Li, Y. Engineering Antigen as Photosensitiser Nanocarrier to Facilitate ROS Triggered Immune Cascade for Photodynamic Immunotherapy. Biomaterials 2020, 244, 119964. [Google Scholar] [CrossRef]
- Wang, T.; Zhang, H.; Han, Y.; Liu, H.; Ren, F.; Zeng, J.; Sun, Q.; Li, Z.; Gao, M. Light-Enhanced O2-Evolving Nanoparticles Boost Photodynamic Therapy To Elicit Antitumor Immunity. ACS Appl. Mater. Interfaces 2019, 11, 16367–16379. [Google Scholar] [CrossRef]
- Doix, B.; Trempolec, N.; Riant, O.; Feron, O. Low Photosensitizer Dose and Early Radiotherapy Enhance Antitumor Immune Response of Photodynamic Therapy-Based Dendritic Cell Vaccination. Front. Oncol. 2019, 9, 811. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Chen, B.; Mo, Y.; Wang, Z.; Qi, T.; Zhang, Q.; Wang, Y. Correction to Redox-Activated Porphyrin-Based Liposome Remote-Loaded with Indoleamine 2,3-Dioxygenase (IDO) Inhibitor for Synergistic Photoimmunotherapy through Induction of Immunogenic Cell Death and Blockage of IDO Pathway. Nano Lett. 2020, 20, 1476. [Google Scholar] [CrossRef] [Green Version]
- Olzowy, B.; Hundt, C.S.; Stocker, S.; Bise, K.; Reulen, H.J.; Stummer, W. Photoirradiation Therapy of Experimental Malignant Glioma with 5-Aminolevulinic Acid. J. Neurosurg. 2002, 97, 970–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kostron, H.; Obwegeser, A.; Jakober, R.; Zimmermann, A.; Rueck, A.C. Experimental and clinical results of mTHPC (Foscan)-mediated photodynamic therapy for malignant brain tumors. In Optical Methods for Tumor Treatment and Detections: Mechanisms and Techniques in Photodynamic Therapy VII; SPIE: Bellingham, WA, USA, 1998. [Google Scholar]
- Callahan, D.E.; Forte, T.M.; Afzal, S.M.; Deen, D.F.; Kahl, S.B.; Bjornstad, K.A.; Bauer, W.F.; Blakely, E.A. Boronated Protoporphyrin (BOPP): Localization in Lysosomes of the Human Glioma Cell Line SF-767 with Uptake Modulated by Lipoprotein Levels. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 761–771. [Google Scholar] [CrossRef] [PubMed]
- Aveline, B.; Hasan, T.; Redmond, R.W. Photophysical and Photosensitizing Properties of Benzoporphyrin Derivative Monoacid Ring A (BPD-MA). Photochem. Photobiol. 1994, 59, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.H.; Meyer, G.A.; Reichert, K.W.; Cheng, J.; Krouwer, H.G.; Ozker, K.; Whelan, H.T. Evaluation of Photodynamic Therapy near Functional Brain Tissue in Patients with Recurrent Brain Tumors. J. Neurooncol. 2004, 67, 201–207. [Google Scholar] [CrossRef]
- Fingar, V.H.; Kik, P.K.; Haydon, P.S.; Cerrito, P.B.; Tseng, M.; Abang, E.; Wieman, T.J. Analysis of Acute Vascular Damage after Photodynamic Therapy Using Benzoporphyrin Derivative (BPD). Br. J. Cancer 1999, 79, 1702–1708. [Google Scholar] [CrossRef] [Green Version]
- Fingar, V.H.; Wieman, T.J.; Haydon, P.S. The Effects of Thrombocytopenia on Vessel Stasis and Macromolecular Leakage after Photodynamic Therapy Using Photofrin. Photochem. Photobiol. 1997, 66, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Sharman, W.M.; Allen, C.M.; van Lier, J.E. Photodynamic Therapeutics: Basic Principles and Clinical Applications. Drug Discov. Today 1999, 4, 507–517. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.-G.; Wang, L.-D.; Feng, X.-S.; Qu, Z.-F.; Shan, T.-Y.; Xie, X.-H. Absorption and elimination of photofrin-II in human immortalization esophageal epithelial cell line SHEE and its malignant transformation cell line SHEEC. Ai Zheng 2009, 28, 1248–1254. [Google Scholar] [CrossRef]
- Schweitzer, V.G. Photodynamic Therapy for Treatment of Head and Neck Cancer. Otolaryngol. Head Neck Surg. 1990, 102, 225–232. [Google Scholar] [CrossRef]
- Kim, M.M.; Darafsheh, A. Light Sources and Dosimetry Techniques for Photodynamic Therapy. Photochem. Photobiol. 2020, 96, 280–294. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, K.; Nitta, M.; Komori, T.; Maruyama, T.; Yasuda, T.; Fujii, Y.; Masamune, K.; Kawamata, T.; Maehara, T.; Muragaki, Y. Intraoperative Photodynamic Diagnosis Using Talaporfin Sodium Simultaneously Applied for Photodynamic Therapy against Malignant Glioma: A Prospective Clinical Study. Front. Neurol. 2018, 9, 24. [Google Scholar] [CrossRef] [Green Version]
- Tetard, M.-C.; Vermandel, M.; Mordon, S.; Lejeune, J.-P.; Reyns, N. Experimental Use of Photodynamic Therapy in High Grade Gliomas: A Review Focused on 5-Aminolevulinic Acid. Photodiagnosis Photodyn. Ther. 2014, 11, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, K.; Garvey, K.L.; Bouras, A.; Cramer, G.; Stepp, H.; Jesu Raj, J.G.; Bozec, D.; Busch, T.M.; Hadjipanayis, C.G. 5-Aminolevulinic Acid Photodynamic Therapy for the Treatment of High-Grade Gliomas. J. Neurooncol. 2019, 141, 595–607. [Google Scholar] [CrossRef] [PubMed]
- Lipson, R.L.; Baldes, E.J.; Olsen, A.M. Hematoporphyrin derivative: A new aid for endoscopic detection of malignant disease. J. Thorac. Cardiovasc. Surg. 1961, 42, 623–629. [Google Scholar] [CrossRef]
- Lipson, R.L.; Baldes, E.J. The Photodynamic Properties of a Particular Hematoporphyrin Derivative. Arch. Dermatol. 1960, 82, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Kessel, D. Hematoporphyrin and HPD: Photophysics, Photochemistry and Phototherapy. Photochem. Photobiol. 1984, 39, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Tomio, L.; Zorat, P.L.; Jori, G.; Reddi, E.; Salvato, B.; Corti, L.; Calzavara, F. Elimination Pathway of Hematoporphyrin from Normal and Tumor-Bearing Rats. Tumori 1982, 68, 283–286. [Google Scholar] [CrossRef]
- Yuan, S.-X.; Li, J.-L.; Xu, X.-K.; Chen, W.; Chen, C.; Kuang, K.-Q.; Wang, F.-Y.; Wang, K.; Li, F.-C. Underlying Mechanism of the Photodynamic Activity of Hematoporphyrin-induced Apoptosis in U87 Glioma Cells. Int. J. Mol. Med. 2018, 41, 2288–2296. [Google Scholar] [CrossRef] [Green Version]
- Perria, C.; Capuzzo, T.; Cavagnaro, G.; Datti, R.; Francaviglia, N.; Rivano, C.; Tercero, V.E. Fast Attempts at the Photodynamic Treatment of Human Gliomas. J. Neurosurg. Sci. 1980, 24, 119–129. [Google Scholar]
- McCulloch, G.A.; Forbes, I.J.; See, K.L.; Cowled, P.A.; Jacka, F.J.; Ward, A.D. Phototherapy in Malignant Brain Tumors. Prog. Clin. Biol. Res. 1984, 170, 709–717. [Google Scholar]
- Kaye, A.H.; Morstyn, G.; Brownbill, D. Adjuvant High-Dose Photoradiation Therapy in the Treatment of Cerebral Glioma: A Phase 1–2 Study. J. Neurosurg. 1987, 67, 500–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, P.J.; Wilson, B.C. Photodynamic Therapy: Cavitary Photoillumination of Malignant Cerebral Tumours Using a Laser Coupled Inflatable Balloon. Can. J. Neurol. Sci. 1985, 12, 371–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kostron, H.; Weiser, G.; Fritsch, E.; Grunert, V. Photodynamic Therapy of Malignant Brain Tumors: Clinical and Neuropathological Results. Photochem. Photobiol. 1987, 46, 937–943. [Google Scholar] [CrossRef] [PubMed]
- Muller, P.J.; Wilson, B.C. Photodynamic Therapy of Malignant Primary Brain Tumours: Clinical Effects, Post-Operative ICP, and Light Penetration of the Brain. Photochem. Photobiol. 1987, 46, 929–935. [Google Scholar] [CrossRef]
- Kostron, H.; Fritsch, E.; Grunert, V. Photodynamic Therapy of Malignant Brain Tumours: A Phase I/II Trial. Br. J. Neurosurg. 1988, 2, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Kostron, H.; Plangger, C.; Fritsch, E.; Maier, H. Photodynamic Treatment of Malignant Brain Tumors. Wien. Klin. Wochenschr. 1990, 102, 531–535. [Google Scholar] [PubMed]
- Powers, S.K.; Cush, S.S.; Walstad, D.L.; Kwock, L. Stereotactic Intratumoral Photodynamic Therapy for Recurrent Malignant Brain Tumors. Neurosurgery 1991, 29, 688–695; discussion 695–696. [Google Scholar] [CrossRef]
- Muller, P.J.; Wilson, B.C. Photodynamic Therapy of Malignant Brain Tumours. Lasers Med. Sci. 1990, 5, 245–252. [Google Scholar] [CrossRef]
- Origitano, T.C.; Reichman, O.H. Photodynamic Therapy for Intracranial Neoplasms: Development of an Image-Based Computer-Assisted Protocol for Photodynamic Therapy of Intracranial Neoplasms. Neurosurgery 1993, 32, 587–595; discussion 595–596. [Google Scholar] [CrossRef]
- Muller, P.J.; Wilson, B.C. Photodynamic Therapy for Recurrent Supratentorial Gliomas. Semin. Surg. Oncol. 1995, 11, 346–354. [Google Scholar] [CrossRef]
- Popovic, E.A.; Kaye, A.H.; Hill, J.S. Photodynamic Therapy of Brain Tumors. Semin. Surg. Oncol. 1995, 11, 335–345. [Google Scholar] [CrossRef]
- Muller, P.J.; Wilson, B.C. Photodynamic Therapy of Supratentorial Gliomas. In Optical Methods for Tumor Treatment and Detection: Mechanisms and Techniques in Photodynamic Therapy VI; SPIE: Bellingham, WA, USA, 1997; Volume 2972, pp. 14–26. [Google Scholar]
- Muller, P.J.; Wilson, B.C.; Lilge, L.D.; Yang, V.X.; Hetzel, F.W.; Chen, Q.; Fullagar, T.; Fenstermaker, R.; Selker, R.; Abrams, J. Photofrin photodynamic therapy for malignant brain tumors. In Optical Methods for Tumor Treatment and Detection: Mechanisms and Techniques in Photodynamic Therapy X; SPIE: Bellingham, WA, USA, 2001. [Google Scholar]
- Stylli, S.S.; Howes, M.; MacGregor, L.; Rajendra, P.; Kaye, A.H. Photodynamic Therapy of Brain Tumours: Evaluation of Porphyrin Uptake versus Clinical Outcome. J. Clin. Neurosci. 2004, 11, 584–596. [Google Scholar] [CrossRef] [PubMed]
- Stylli, S.S.; Kaye, A.H.; MacGregor, L.; Howes, M.; Rajendra, P. Photodynamic Therapy of High Grade Glioma—Long Term Survival. J. Clin. Neurosci. 2005, 12, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Muller, P.J.; Wilson, B.C. Photodynamic Therapy of Brain Tumors--a Work in Progress. Lasers Surg. Med. 2006, 38, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, S. Recent Advances in PDD and PDT for Malignant Brain Tumors. Rev. Laser Eng. 2008, 36, 1351–1354. [Google Scholar] [CrossRef]
- Perria, C.; Carai, M.; Falzoi, A.; Orunesu, G.; Rocca, A.; Massarelli, G.; Francaviglia, N.; Jori, G. Photodynamic Therapy of Malignant Brain Tumors: Clinical Results Of, Difficulties With, Questions About, and Future Prospects for the Neurosurgical Applications. Neurosurgery 1988, 23, 557–563. [Google Scholar] [CrossRef]
- Forbes, I.J.; Cowled, P.A.; Leong, A.S.Y.; Ward, A.D.; Black, R.B.; Blake, A.J.; Jacka, F.J. Phototherapy of human tumours using haematoporphyrin derivative. Med. J. Aust. 1980, 2, 489–493. [Google Scholar] [CrossRef]
- Kostron, H.; Obwegeser, A.; Jakober, R. Photodynamic Therapy in Neurosurgery: A Review. J. Photochem. Photobiol. B 1996, 36, 157–168. [Google Scholar] [CrossRef]
- Quirk, B.J.; Brandal, G.; Donlon, S.; Vera, J.C.; Mang, T.S.; Foy, A.B.; Lew, S.M.; Girotti, A.W.; Jogal, S.; LaViolette, P.S.; et al. Photodynamic Therapy (PDT) for Malignant Brain Tumors—Where Do We Stand? Photodiagnosis Photodyn. Ther. 2015, 12, 530–544. [Google Scholar] [CrossRef] [Green Version]
- Kostron, H.; Hochleitner, B.W.; Obwegeser, A.; Seiwald, M. Clinical and experimental results of photodynamic therapy in neurosurgery. In Proceedings of the 5th International Photodynamic Association Biennial Meeting, Amelia Island, FL, USA, 21–24 September 1994; Cortese, D.A., Ed.; SPIE: Bellingham, WA, USA, 1995; Volume 2371, pp. 126–128. [Google Scholar]
- Gunaydin, G.; Gedik, M.E.; Ayan, S. Photodynamic Therapy for the Treatment and Diagnosis of Cancer-A Review of the Current Clinical Status. Front. Chem. 2021, 9, 686303. [Google Scholar] [CrossRef]
- Du, P.; Hu, S.; Cheng, Y.; Li, F.; Li, M.; Li, J.; Yi, L.; Feng, H. Photodynamic Therapy Leads to Death of C6 Glioma Cells Partly through AMPAR. Brain Res. 2012, 1433, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.-L.; Du, P.; Hu, R.; Li, F.; Feng, H. Imbalance of Ca2+ and K+ Fluxes in C6 Glioma Cells after PDT Measured with Scanning Ion-Selective Electrode Technique. Lasers Med. Sci. 2014, 29, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowski, J.M.; Arnaut, L.G. Photodynamic Therapy (PDT) of Cancer: From Local to Systemic Treatment. Photochem. Photobiol. Sci. 2015, 14, 1765–1780. [Google Scholar] [CrossRef] [PubMed]
- Tirapelli, L.F.; Morgueti, M.; da Cunha Tirapelli, D.P.; Bagnato, V.S.; Ferreira, J.; Neto, F.S.L.; Peria, F.M.; Oliveira, H.F.; Junior, C.G.C. Apoptosis in Glioma Cells Treated with PDT. Photomed. Laser Surg. 2011, 29, 305–309. [Google Scholar] [CrossRef]
- Park, J.; Lee, Y.-K.; Park, I.-K.; Hwang, S.R. Current Limitations and Recent Progress in Nanomedicine for Clinically Available Photodynamic Therapy. Biomedicines 2021, 9, 85. [Google Scholar] [CrossRef]
- Baskaran, R.; Lee, J.; Yang, S.-G. Clinical Development of Photodynamic Agents and Therapeutic Applications. Biomater. Res. 2018, 22, 25. [Google Scholar]
- Kostron, H.; Fiegele, T.; Akatuna, E. Combination of FOSCAN® Mediated Fluorescence Guided Resection and Photodynamic Treatment as New Therapeutic Concept for Malignant Brain Tumors. Med. Laser Appl. 2006, 21, 285–290. [Google Scholar] [CrossRef]
- Rosenthal, M.A.; Kavar, B.; Hill, J.S.; Morgan, D.J.; Nation, R.L.; Stylli, S.S.; Basser, R.L.; Uren, S.; Geldard, H.; Green, M.D.; et al. Phase I and Pharmacokinetic Study of Photodynamic Therapy for High-Grade Gliomas Using a Novel Boronated Porphyrin. J. Clin. Oncol. 2001, 19, 519–524. [Google Scholar] [CrossRef]
- Rosenthal, M.A.; Kavar, B.; Uren, S.; Kaye, A.H. Promising Survival in Patients with High-Grade Gliomas Following Therapy with a Novel Boronated Porphyrin. J. Clin. Neurosci. 2003, 10, 425–427. [Google Scholar] [CrossRef]
- Beck, T.J.; Kreth, F.W.; Beyer, W.; Mehrkens, J.H.; Obermeier, A.; Stepp, H.; Stummer, W.; Baumgartner, R. Interstitial Photodynamic Therapy of Nonresectable Malignant Glioma Recurrences Using 5-Aminolevulinic Acid Induced Protoporphyrin IX. Lasers Surg. Med. 2007, 39, 386–393. [Google Scholar] [CrossRef]
- Eljamel, M.S.; Goodman, C.; Moseley, H. ALA and Photofrin Fluorescence-Guided Resection and Repetitive PDT in Glioblastoma Multiforme: A Single Centre Phase III Randomised Controlled Trial. Lasers Med. Sci. 2008, 23, 361–367. [Google Scholar] [CrossRef]
- Stepp, H.G.; Beck, T.; Beyer, W.; Pongratz, T.; Sroka, R.; Baumgartner, R.; Stummer, W.; Olzowy, B.; Mehrkens, J.H.; Tonn, J.C.; et al. Fluorescence-guided resections and photodynamic therapy for malignant gliomas using 5-aminolevulinic acid. In Photonic Therapeutics and Diagnostics; SPIE: Bellingham, WA, USA, 2005; Volume 5686, pp. 547–557. [Google Scholar]
- Stepp, H.; Beck, T.; Pongratz, T.; Meinel, T.; Kreth, F.-W.; Tonn, J.C.; Stummer, W. ALA and Malignant Glioma: Fluorescence-Guided Resection and Photodynamic Treatment. J. Environ. Pathol. Toxicol. Oncol. 2007, 26, 157–164. [Google Scholar] [CrossRef]
- Akimoto, J.; Haraoka, J.; Aizawa, K. Preliminary Clinical Report on Safety and Efficacy of Photodynamic Therapy Using Talaporfin Sodium for Malignant Gliomas. Photodiagnosis Photodyn. Ther. 2012, 9, 91–99. [Google Scholar] [CrossRef]
- Lyons, M.; Phang, I.; Eljamel, S. The Effects of PDT in Primary Malignant Brain Tumours Could Be Improved by Intraoperative Radiotherapy. Photodiagnosis Photodyn. Ther. 2012, 9, 40–45. [Google Scholar] [CrossRef]
- Johansson, A.; Faber, F.; Kniebühler, G.; Stepp, H.; Sroka, R.; Egensperger, R.; Beyer, W.; Kreth, F.-W. Protoporphyrin IX Fluorescence and Photobleaching During Interstitial Photodynamic Therapy of Malignant Gliomas for Early Treatment Prognosis. Lasers Surg. Med. 2013, 45, 225–234. [Google Scholar] [CrossRef]
- Muragaki, Y.; Akimoto, J.; Maruyama, T.; Iseki, H.; Ikuta, S.; Nitta, M.; Maebayashi, K.; Saito, T.; Okada, Y.; Kaneko, S.; et al. Phase II Clinical Study on Intraoperative Photodynamic Therapy with Talaporfin Sodium and Semiconductor Laser in Patients with Malignant Brain Tumors. J. Neurosurg. 2013, 119, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, C.; Rühm, A.; Tonn, J.-C.; Kreth, S.; Kreth, F.-W. Surg-25interstitial photodynamic therapy of de-novo glioblastoma multiforme who IV. Neuro-Oncology 2015, 17, v219.5–v220. [Google Scholar] [CrossRef]
- Vanaclocha, V.; Sureda, M.; Azinovic, I.; Rebollo, J.; Cañón, R.; Sapena, N.S.; Cases, F.G.; Brugarolas, A. Photodynamic Therapy in the Treatment of Brain Tumours. A Feasibility Study. Photodiagnosis Photodyn. Ther. 2015, 12, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Nitta, M.; Muragaki, Y.; Maruyama, T.; Iseki, H.; Komori, T.; Ikuta, S.; Saito, T.; Yasuda, T.; Hosono, J.; Okamoto, S.; et al. Role of Photodynamic Therapy Using Talaporfin Sodium and a Semiconductor Laser in Patients with Newly Diagnosed Glioblastoma. J. Neurosurg. 2018, 131, 1361–1368. [Google Scholar] [CrossRef]
- Lietke, S.; Schmutzer, M.; Schwartz, C.; Weller, J.; Siller, S.; Aumiller, M.; Heckl, C.; Forbrig, R.; Niyazi, M.; Egensperger, R.; et al. Interstitial Photodynamic Therapy Using 5-ALA for Malignant Glioma Recurrences. Cancers 2021, 13, 1767. [Google Scholar] [CrossRef]
- Vermandel, M.; Dupont, C.; Lecomte, F.; Leroy, H.-A.; Tuleasca, C.; Mordon, S.; Hadjipanayis, C.G.; Reyns, N. Standardized Intraoperative 5-ALA Photodynamic Therapy for Newly Diagnosed Glioblastoma Patients: A Preliminary Analysis of the INDYGO Clinical Trial. J. Neurooncol. 2021, 152, 501–514. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Nitta, M.; Shimizu, K.; Saito, T.; Tsuzuki, S.; Fukui, A.; Koriyama, S.; Kuwano, A.; Komori, T.; Masui, K.; et al. Therapeutic Options for Recurrent Glioblastoma-Efficacy of Talaporfin Sodium Mediated Photodynamic Therapy. Pharmaceutics 2022, 14, 353. [Google Scholar] [CrossRef] [PubMed]
- Kozlikina, E.I.; Trifonov, I.S.; Sinkin, M.V.; Krylov, V.V.; Loschenov, V.B. The Combined Use of 5-ALA and Chlorin e6 Photosensitizers for Fluorescence-Guided Resection and Photodynamic Therapy under Neurophysiological Control for Recurrent Glioblastoma in the Functional Motor Area after Ineffective Use of 5-ALA: Preliminary Results. Bioengineering 2022, 9, 104. [Google Scholar] [CrossRef]
- Neagu, M.; Constantin, C.; Tampa, M.; Matei, C.; Lupu, A.; Manole, E.; Ion, R.-M.; Fenga, C.; Tsatsakis, A.M. Toxicological and Efficacy Assessment of Post-Transition Metal (Indium) Phthalocyanine for Photodynamic Therapy in Neuroblastoma. Oncotarget 2016, 7, 69718–69732. [Google Scholar] [CrossRef] [Green Version]
- Velazquez, F.N.; Miretti, M.; Baumgartner, M.T.; Caputto, B.L.; Tempesti, T.C.; Prucca, C.G. Effectiveness of ZnPc and of an Amine Derivative to Inactivate Glioblastoma Cells by Photodynamic Therapy: An in Vitro Comparative Study. Sci. Rep. 2019, 9, 3010. [Google Scholar] [CrossRef] [PubMed]
- Stylli, S.; Hill, J.; Sawyer, W.; Kaye, A. Aluminium Phthalocyanine Mediated Photodynamic Therapy in Experimental Malignant Glioma. J. Clin. Neurosci. 1995, 2, 146–151. [Google Scholar] [CrossRef]
- de Paula, L.B.; Primo, F.L.; Pinto, M.R.; Morais, P.C.; Tedesco, A.C. Evaluation of a Chloroaluminium Phthalocyanine-Loaded Magnetic Nanoemulsion as a Drug Delivery Device to Treat Glioblastoma Using Hyperthermia and Photodynamic Therapy. RSC Adv. 2017, 7, 9115–9122. [Google Scholar] [CrossRef] [Green Version]
- Hirschberg, H.; Sørensen, D.R.; Angell-Petersen, E.; Peng, Q.; Tromberg, B.; Sun, C.-H.; Spetalen, S.; Madsen, S. Repetitive Photodynamic Therapy of Malignant Brain Tumors. J. Environ. Pathol. Toxicol. Oncol. 2006, 25, 261–279. [Google Scholar] [CrossRef]
- Davies, N.; Wilson, B.C. Interstitial in Vivo ALA-PpIX Mediated Metronomic Photodynamic Therapy (mPDT) Using the CNS-1 Astrocytoma with Bioluminescence Monitoring. Photodiagnosis Photodyn. Ther. 2007, 4, 202–212. [Google Scholar] [CrossRef]
- Guo, H.-W.; Lin, L.-T.; Chen, P.-H.; Ho, M.-H.; Huang, W.-T.; Lee, Y.-J.; Chiou, S.-H.; Hsieh, Y.-S.; Dong, C.-Y.; Wang, H.-W. Low-Fluence Rate, Long Duration Photodynamic Therapy in Glioma Mouse Model Using Organic Light Emitting Diode (OLED). Photodiagnosis Photodyn. Ther. 2015, 12, 504–510. [Google Scholar] [CrossRef]
- Chelakkot, V.S.; Liu, K.; Yoshioka, E.; Saha, S.; Xu, D.; Licursi, M.; Dorward, A.; Hirasawa, K. MEK Reduces Cancer-Specific PpIX Accumulation through the RSK-ABCB1 and HIF-1α-FECH Axes. Sci. Rep. 2020, 10, 22124. [Google Scholar] [CrossRef]
- Hagiya, Y.; Endo, Y.; Yonemura, Y.; Takahashi, K.; Ishizuka, M.; Abe, F.; Tanaka, T.; Okura, I.; Nakajima, M.; Ishikawa, T.; et al. Pivotal Roles of Peptide Transporter PEPT1 and ATP-Binding Cassette (ABC) Transporter ABCG2 in 5-Aminolevulinic Acid (ALA)-Based Photocytotoxicity of Gastric Cancer Cells in Vitro. Photodiagnosis Photodyn. Ther. 2012, 9, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Kobuchi, H.; Moriya, K.; Ogino, T.; Fujita, H.; Inoue, K.; Shuin, T.; Yasuda, T.; Utsumi, K.; Utsumi, T. Mitochondrial Localization of ABC Transporter ABCG2 and Its Function in 5-Aminolevulinic Acid-Mediated Protoporphyrin IX Accumulation. PLoS ONE 2012, 7, e50082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishizuka, M.; Abe, F.; Sano, Y.; Takahashi, K.; Inoue, K.; Nakajima, M.; Kohda, T.; Komatsu, N.; Ogura, S.-I.; Tanaka, T. Novel Development of 5-Aminolevurinic Acid (ALA) in Cancer Diagnoses and Therapy. Int. Immunopharmacol. 2011, 11, 358–365. [Google Scholar] [CrossRef]
- Markwardt, N.A.; Haj-Hosseini, N.; Hollnburger, B.; Stepp, H.; Zelenkov, P.; Rühm, A. 405 Nm versus 633 Nm for Protoporphyrin IX Excitation in Fluorescence-Guided Stereotactic Biopsy of Brain Tumors. J. Biophotonics 2016, 9, 901–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akimoto, J.; Fukami, S.; Ichikawa, M.; Mohamed, A.; Kohno, M. Intraoperative Photodiagnosis for Malignant Glioma Using Photosensitizer Talaporfin Sodium. Front. Surg. 2019, 6, 12. [Google Scholar] [CrossRef]
- Tsutsumi, M.; Miki, Y.; Akimoto, J.; Haraoka, J.; Aizawa, K.; Hirano, K.; Beppu, M. Photodynamic Therapy with Talaporfin Sodium Induces Dose-Dependent Apoptotic Cell Death in Human Glioma Cell Lines. Photodiagnosis Photodyn. Ther. 2013, 10, 103–110. [Google Scholar] [CrossRef]
- Miki, Y.; Akimoto, J.; Yokoyama, S.; Homma, T.; Tsutsumi, M.; Haraoka, J.; Hirano, K.; Beppu, M. Photodynamic Therapy in Combination with Talaporfin Sodium Induces Mitochondrial Apoptotic Cell Death Accompanied with Necrosis in Glioma Cells. Biol. Pharm. Bull. 2013, 36, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Jia, Y.; Chen, L.; Chi, D.; Cong, D.; Zhou, P.; Jin, J.; Ji, H.; Liang, B.; Gao, S.; Hu, S. Photodynamic Therapy Combined with Temozolomide Inhibits C6 Glioma Migration and Invasion and Promotes Mitochondrial-Associated Apoptosis by Inhibiting Sodium-Hydrogen Exchanger Isoform 1. Photodiagnosis Photodyn. Ther. 2019, 26, 405–412. [Google Scholar] [CrossRef]
- Miki, Y.; Akimoto, J.; Omata, H.; Moritake, K.; Hiranuma, M.; Hironaka, C.; Fujiwara, Y.; Beppu, M. Concomitant Treatment with Temozolomide Enhances Apoptotic Cell Death in Glioma Cells Induced by Photodynamic Therapy with Talaporfin Sodium. Photodiagnosis Photodyn. Ther. 2014, 11, 556–564. [Google Scholar] [CrossRef]
- Cong, D.; Zhu, W.; Shi, Y.; Pointer, K.B.; Clark, P.A.; Shen, H.; Kuo, J.S.; Hu, S.; Sun, D. Upregulation of NHE1 Protein Expression Enables Glioblastoma Cells to Escape TMZ-Mediated Toxicity via Increased H+ Extrusion, Cell Migration and Survival. Carcinogenesis 2014, 35, 2014–2024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Guo, M.; Shen, L.; Hu, S. Combination of Photodynamic Therapy and Temozolomide on Glioma in a Rat C6 Glioma Model. Photodiagnosis Photodyn. Ther. 2014, 11, 603–612. [Google Scholar] [CrossRef]
- Tzerkovsky, D.A.; Osharin, V.V.; Istomin, Y.P.; Alexandrova, E.N.; Vozmitel, M.A. Fluorescent Diagnosis and Photodynamic Therapy for C6 Glioma in Combination with Antiangiogenic Therapy in Subcutaneous and Intracranial Tumor Models. Exp. Oncol. 2014, 36, 85–89. [Google Scholar]
- Ji, B.; Wei, M.; Yang, B. Recent Advances in Nanomedicines for Photodynamic Therapy (PDT)-Driven Cancer Immunotherapy. Theranostics 2022, 12, 434–458. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Yu, S.; Wang, X.; Qian, Y.; Wu, W.; Zhang, S.; Zheng, B.; Wei, G.; Gao, S.; Cao, Z.; et al. High Affinity of Chlorin e6 to Immunoglobulin G for Intraoperative Fluorescence Image-Guided Cancer Photodynamic and Checkpoint Blockade Therapy. ACS Nano 2019, 13, 10242–10260. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Pan, Y.; Cao, W.; Xia, F.; Liu, B.; Niu, J.; Alfranca, G.; Sun, X.; Ma, L.; de la Fuente, J.M.; et al. A Tumor Microenvironment Responsive Biodegradable CaCO3/MnO2- Based Nanoplatform for the Enhanced Photodynamic Therapy and Improved PD-L1 Immunotherapy. Theranostics 2019, 9, 6867–6884. [Google Scholar] [CrossRef]
- Liu, B.; Qiao, G.; Han, Y.; Shen, E.; Alfranca, G.; Tan, H.; Wang, L.; Pan, S.; Ma, L.; Xiong, W.; et al. Targeted Theranostics of Lung Cancer: PD-L1-Guided Delivery of Gold Nanoprisms with Chlorin e6 for Enhanced Imaging and Photothermal/photodynamic Therapy. Acta Biomater. 2020, 117, 361–373. [Google Scholar] [CrossRef]
- Tong, Q.; Xu, J.; Wu, A.; Zhang, C.; Yang, A.; Zhang, S.; Lin, H.; Lu, W. Pheophorbide A-Mediated Photodynamic Therapy Potentiates Checkpoint Blockade Therapy of Tumor with Low PD-L1 Expression. Pharmaceutics 2022, 14, 2513. [Google Scholar] [CrossRef]
- Yuan, Z.; Fan, G.; Wu, H.; Liu, C.; Zhan, Y.; Qiu, Y.; Shou, C.; Gao, F.; Zhang, J.; Yin, P.; et al. Photodynamic Therapy Synergizes with PD-L1 Checkpoint Blockade for Immunotherapy of CRC by Multifunctional Nanoparticles. Mol. Ther. 2021, 29, 2931–2948. [Google Scholar] [CrossRef]
- Zhang, R.; Zhu, Z.; Lv, H.; Li, F.; Sun, S.; Li, J.; Lee, C.-S. Immune Checkpoint Blockade Mediated by a Small-Molecule Nanoinhibitor Targeting the PD-1/PD-L1 Pathway Synergizes with Photodynamic Therapy to Elicit Antitumor Immunity and Antimetastatic Effects on Breast Cancer. Small 2019, 15, e1903881. [Google Scholar] [CrossRef]
- Su, Z.; Xiao, Z.; Huang, J.; Wang, Y.; An, Y.; Xiao, H.; Peng, Y.; Pang, P.; Han, S.; Zhu, K.; et al. Dual-Sensitive PEG-Sheddable Nanodrug Hierarchically Incorporating PD-L1 Antibody and Zinc Phthalocyanine for Improved Immuno-Photodynamic Therapy. ACS Appl. Mater. Interfaces 2021, 13, 12845–12856. [Google Scholar] [CrossRef]
- O’Shaughnessy, M.J.; Murray, K.S.; La Rosa, S.P.; Budhu, S.; Merghoub, T.; Somma, A.; Monette, S.; Kim, K.; Corradi, R.B.; Scherz, A.; et al. Systemic Antitumor Immunity by PD-1/PD-L1 Inhibition Is Potentiated by Vascular-Targeted Photodynamic Therapy of Primary Tumors. Clin. Cancer Res. 2018, 24, 592–599. [Google Scholar] [CrossRef] [Green Version]
- Tumangelova-Yuzeir, K.; Minkin, K.; Angelov, I.; Ivanova-Todorova, E.; Kurteva, E.; Vasilev, G.; Arabadjiev, J.; Karazapryanov, P.; Gabrovski, K.; Zaharieva, L.; et al. Alteration of Mesenchymal Stem Cells Isolated from Glioblastoma Multiforme under the Influence of Photodynamic Treatment. Curr. Issues Mol. Biol. 2023, 45, 2580–2596. [Google Scholar] [CrossRef] [PubMed]
- Josefsen, L.B.; Boyle, R.W. Photodynamic Therapy: Novel Third-Generation Photosensitizers One Step Closer? Br. J. Pharmacol. 2008, 154, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Luiza Andreazza, N.; Vevert-Bizet, C.; Bourg-Heckly, G.; Sureau, F.; José Salvador, M.; Bonneau, S. Berberine as a Photosensitizing Agent for Antitumoral Photodynamic Therapy: Insights into Its Association to Low Density Lipoproteins. Int. J. Pharm. 2016, 510, 240–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, X.; Zhou, H.; Liu, Y.; Wen, Y.; Wei, C.; Yu, Q.; Liu, J. Transferrin/aptamer Conjugated Mesoporous Ruthenium Nanosystem for Redox-Controlled and Targeted Chemo-Photodynamic Therapy of Glioma. Acta Biomater. 2018, 82, 143–157. [Google Scholar] [CrossRef]
- Sudheesh, K.V.; Jayaram, P.S.; Samanta, A.; Bejoymohandas, K.S.; Jayasree, R.S.; Ajayaghosh, A. A Cyclometalated Ir Complex as a Lysosome-Targeted Photodynamic Therapeutic Agent for Integrated Imaging and Therapy in Cancer Cells. Chemistry 2018, 24, 10999–11007. [Google Scholar] [CrossRef]
- Ibarra, L.E.; Porcal, G.V.; Macor, L.P.; Ponzio, R.A.; Spada, R.M.; Lorente, C.; Chesta, C.A.; Rivarola, V.A.; Palacios, R.E. Metallated Porphyrin-Doped Conjugated Polymer Nanoparticles for Efficient Photodynamic Therapy of Brain and Colorectal Tumor Cells. Nanomedicine 2018, 13, 605–624. [Google Scholar] [CrossRef]
- Boreham, E.M.; Jones, L.; Swinburne, A.N.; Blanchard-Desce, M.; Hugues, V.; Terryn, C.; Miomandre, F.; Lemercier, G.; Natrajan, L.S. A Cyclometallated Fluorenyl Ir(iii) Complex as a Potential Sensitiser for Two-Photon Excited Photodynamic Therapy (2PE-PDT). Dalton Trans. 2015, 44, 16127–16135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, X.-L.; Jing, F.; Lin, B.-L.; Cui, S.; Yu, R.-T.; Shen, X.-D.; Wang, T.-W. pH-Responsive Magnetic Mesoporous Silica-Based Nanoplatform for Synergistic Photodynamic Therapy/Chemotherapy. ACS Appl. Mater. Interfaces 2018, 10, 15001–15011. [Google Scholar] [CrossRef]
- Jamali, Z.; Khoobi, M.; Hejazi, S.M.; Eivazi, N.; Abdolahpour, S.; Imanparast, F.; Moradi-Sardareh, H.; Paknejad, M. Evaluation of Targeted Curcumin (CUR) Loaded PLGA Nanoparticles for in Vitro Photodynamic Therapy on Human Glioblastoma Cell Line. Photodiagnosis Photodyn. Ther. 2018, 23, 190–201. [Google Scholar] [CrossRef]
- Wang, Q.; Li, J.-M.; Yu, H.; Deng, K.; Zhou, W.; Wang, C.-X.; Zhang, Y.; Li, K.-H.; Zhuo, R.-X.; Huang, S.-W. Fluorinated Polymeric Micelles to Overcome Hypoxia and Enhance Photodynamic Cancer Therapy. Biomater. Sci. 2018, 6, 3096–3107. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Zhao, X.; Fu, T.; Li, K.; He, Y.; Luo, Z.; Dai, L.; Zeng, R.; Cai, K. An iRGD-Conjugated Prodrug Micelle with Blood-Brain-Barrier Penetrability for Anti-Glioma Therapy. Biomaterials 2020, 230, 119666. [Google Scholar] [CrossRef] [PubMed]
- de Paula, L.B.; Primo, F.L.; Tedesco, A.C. Nanomedicine Associated with Photodynamic Therapy for Glioblastoma Treatment. Biophys. Rev. 2017, 9, 761–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellosi, D.S.; Paula, L.B.; de Melo, M.T.; Tedesco, A.C. Targeted and Synergic Glioblastoma Treatment: Multifunctional Nanoparticles Delivering Verteporfin as Adjuvant Therapy for Temozolomide Chemotherapy. Mol. Pharm. 2019, 16, 1009–1024. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Luo, L.; Amirshaghaghi, A.; Miller, J.; Meng, C.; You, T.; Busch, T.M.; Tsourkas, A.; Cheng, Z. Dextran-Benzoporphyrin Derivative (BPD) Coated Superparamagnetic Iron Oxide Nanoparticle (SPION) Micelles for T2-Weighted Magnetic Resonance Imaging and Photodynamic Therapy. Bioconjugate Chem. 2019, 30, 2974–2981. [Google Scholar] [CrossRef]
- Bœuf-Muraille, G.; Rigaux, G.; Callewaert, M.; Zambrano, N.; Van Gulick, L.; Roullin, V.G.; Terryn, C.; Andry, M.-C.; Chuburu, F.; Dukic, S.; et al. Evaluation of mTHPC-Loaded PLGA Nanoparticles for in Vitro Photodynamic Therapy on C6 Glioma Cell Line. Photodiagnosis Photodyn. Ther. 2019, 25, 448–455. [Google Scholar] [CrossRef]
- Castilho-Fernandes, A.; Lopes, T.G.; Primo, F.L.; Pinto, M.R.; Tedesco, A.C. Photodynamic Process Induced by Chloro-Aluminum Phthalocyanine Nanoemulsion in Glioblastoma. Photodiagnosis Photodyn. Ther. 2017, 19, 221–228. [Google Scholar] [CrossRef]
- Davanzo, N.N.; Pellosi, D.S.; Franchi, L.P.; Tedesco, A.C. Light Source Is Critical to Induce Glioblastoma Cell Death by Photodynamic Therapy Using Chloro-Aluminiumphtalocyanine Albumin-Based Nanoparticles. Photodiagnosis Photodyn. Ther. 2017, 19, 181–183. [Google Scholar] [CrossRef]
- Lv, Z.; Cao, Y.; Xue, D.; Zhang, H.; Zhou, S.; Yin, N.; Li, W.; Jin, L.; Wang, Y.; Zhang, H. A Multiphoton Transition Activated Iron Based Metal Organic Framework for Synergistic Therapy of Photodynamic Therapy/chemodynamic Therapy/chemotherapy for Orthotopic Gliomas. J. Mater. Chem. B Mater. Biol. Med. 2023, 11, 1100–1107. [Google Scholar] [CrossRef]
- Tsai, Y.-C.; Vijayaraghavan, P.; Chiang, W.-H.; Chen, H.-H.; Liu, T.-I.; Shen, M.-Y.; Omoto, A.; Kamimura, M.; Soga, K.; Chiu, H.-C. Targeted Delivery of Functionalized Upconversion Nanoparticles for Externally Triggered Photothermal/Photodynamic Therapies of Brain Glioblastoma. Theranostics 2018, 8, 1435–1448. [Google Scholar] [CrossRef]
- Chen, G.; Qiu, H.; Prasad, P.N.; Chen, X. Upconversion Nanoparticles: Design, Nanochemistry, and Applications in Theranostics. Chem. Rev. 2014, 114, 5161–5214. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.-L.; Wu, J.; Lin, B.-L.; Cui, S.; Liu, H.-M.; Yu, R.-T.; Shen, X.-D.; Wang, T.-W.; Xia, W. Near-Infrared Light-Activated Red-Emitting Upconverting Nanoplatform for T-Weighted Magnetic Resonance Imaging and Photodynamic Therapy. Acta Biomater. 2018, 74, 360–373. [Google Scholar] [CrossRef]
- Wang, L.-X.; Li, J.-W.; Huang, J.-Y.; Li, J.-H.; Zhang, L.-J.; O’Shea, D.; Chen, Z.-L. Antitumor Activity of Photodynamic Therapy with a Chlorin Derivative in Vitro and in Vivo. Tumour Biol. 2015, 36, 6839–6847. [Google Scholar] [CrossRef]
- Hiramatsu, R.; Kawabata, S.; Tanaka, H.; Sakurai, Y.; Suzuki, M.; Ono, K.; Miyatake, S.-I.; Kuroiwa, T.; Hao, E.; Vicente, M.G.H. Tetrakis(p-Carboranylthio-Tetrafluorophenyl)chlorin (TPFC): Application for Photodynamic Therapy and Boron Neutron Capture Therapy. J. Pharm. Sci. 2015, 104, 962–970. [Google Scholar] [CrossRef]
- Song, R.; Hu, D.; Chung, H.Y.; Sheng, Z.; Yao, S. Lipid-Polymer Bilaminar Oxygen Nanobubbles for Enhanced Photodynamic Therapy of Cancer. ACS Appl. Mater. Interfaces 2018, 10, 36805–36813. [Google Scholar] [CrossRef]
- Wang, X.; Tian, Y.; Liao, X.; Tang, Y.; Ni, Q.; Sun, J.; Zhao, Y.; Zhang, J.; Teng, Z.; Lu, G. Enhancing Selective Photosensitizer Accumulation and Oxygen Supply for High-Efficacy Photodynamic Therapy toward Glioma by 5-Aminolevulinic Acid Loaded Nanoplatform. J. Colloid Interface Sci. 2020, 565, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Wu, J.; He, M.; Hou, X.; Wang, Y.; Cai, X.; Xin, H.; Gao, F.; Chen, Y. Combined Cancer Chemo-Photodynamic and Photothermal Therapy Based on ICG/PDA/TPZ-Loaded Nanoparticles. Mol. Pharm. 2019, 16, 2172–2183. [Google Scholar] [CrossRef]
- Kaneko, K.; Acharya, C.R.; Nagata, H.; Yang, X.; Hartman, Z.C.; Hobeika, A.; Hughes, P.F.; Haystead, T.A.J.; Morse, M.A.; Lyerly, H.K.; et al. Combination of a Novel Heat Shock Protein 90-Targeted Photodynamic Therapy with PD-1/PD-L1 Blockade Induces Potent Systemic Antitumor Efficacy and Abscopal Effect against Breast Cancers. J. Immunother. Cancer 2022, 10. [Google Scholar] [CrossRef]
- Dupont, C.; Mordon, S.; Deleporte, P.; Reyns, N.; Vermandel, M. A Novel Device for Intraoperative Photodynamic Therapy Dedicated to Glioblastoma Treatment. Future Oncol. 2017, 13, 2441–2454. [Google Scholar] [CrossRef] [Green Version]
- Madsen, S.J.; Sun, C.H.; Tromberg, B.J.; Hirschberg, H. Development of a Novel Indwelling Balloon Applicator for Optimizing Light Delivery in Photodynamic Therapy. Lasers Surg. Med. 2001, 29, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Jamali, Z.; Hejazi, S.M.; Ebrahimi, S.M.; Moradi-Sardareh, H.; Paknejad, M. Effects of LED-Based Photodynamic Therapy Using Red and Blue Lights, with Natural Hydrophobic Photosensitizers on Human Glioma Cell Line. Photodiagnosis Photodyn. Ther. 2018, 21, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Whelan, H.T. High-Grade Glioma/glioblastoma Multiforme: Is There a Role for Photodynamic Therapy? J. Natl. Compr. Canc. Netw. 2012, 10 (Suppl. S2), S31–S34. [Google Scholar] [CrossRef] [PubMed]
- Curnow, A.; Bown, S.G. The Role of Reperfusion Injury in Photodynamic Therapy with 5-Aminolaevulinic Acid—A Study on Normal Rat Colon. Br. J. Cancer 2002, 86, 989–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tetard, M.-C.; Vermandel, M.; Leroy, H.-A.; Leroux, B.; Maurage, C.-A.; Lejeune, J.-P.; Mordon, S.; Reyns, N. Interstitial 5-ALA Photodynamic Therapy and Glioblastoma: Preclinical Model Development and Preliminary Results. Photodiagnosis Photodyn. Ther. 2016, 13, 218–224. [Google Scholar] [CrossRef] [Green Version]
- Vermandel, M.; Quidet, M.; Vignion-Dewalle, A.-S.; Leroy, H.-A.; Leroux, B.; Mordon, S.; Reyns, N. Comparison of Different Treatment Schemes in 5-ALA Interstitial Photodynamic Therapy for High-Grade Glioma in a Preclinical Model: An MRI Study. Photodiagnosis Photodyn. Ther. 2019, 25, 166–176. [Google Scholar] [CrossRef] [Green Version]
- Leroy, H.-A.; Vermandel, M.; Leroux, B.; Duhamel, A.; Lejeune, J.-P.; Mordon, S.; Reyns, N. MRI Assessment of Treatment Delivery for Interstitial Photodynamic Therapy of High-Grade Glioma in a Preclinical Model. Lasers Surg. Med. 2018, 50, 460–468. [Google Scholar] [CrossRef]
- Leroy, H.-A.; Vermandel, M.; Vignion-Dewalle, A.-S.; Leroux, B.; Maurage, C.-A.; Duhamel, A.; Mordon, S.; Reyns, N. Interstitial Photodynamic Therapy and Glioblastoma: Light Fractionation in a Preclinical Model. Lasers Surg. Med. 2017, 49, 506–515. [Google Scholar] [CrossRef]
- van Zaane, F.; Subbaiyan, D.; van der Ploeg-van den Heuvel, A.; de Bruijn, H.S.; Balbas, E.M.; Pandraud, G.; Sterenborg, H.J.C.M.; French, P.J.; Robinson, D.J. A Telemetric Light Delivery System for Metronomic Photodynamic Therapy (mPDT) in Rats. J. Biophotonics 2010, 3, 347–355. [Google Scholar] [CrossRef]
- Plattner, M.; Bernwick, W.; Kostron, H. Hematoporphyrin-derivative photodynamic in-vitro sensitivity testing for brain tumors. In Proceedings of the International Conference on Photodynamic Therapy and Laser Medicine, Beijing, China, 15–17 October 1991; SPIE: Bellingham, WA, USA, 1993; Volume 1616, pp. 182–185. [Google Scholar]
- Chen, Z.-Q.; Wu, S.-E.; Zhu, S.-G. Adjuvant photodynamic therapy in surgical management of cerebral tumors. In Proceedings of the International Conference on Photodynamic Therapy and Laser Medicine, Beijing, China, 15–17 October 1991; SPIE: Bellingham, WA, USA, 1993; Volume 1616, pp. 94–97. [Google Scholar]
- Marks, P.V.; Furneaux, C.; Shivvakumar, R. An in Vitro Study of the Effect of Photodynamic Therapy on Human Meningiomas. Br. J. Neurosurg. 1992, 6, 327–332. [Google Scholar] [CrossRef]
- Neurosurgery. Available online: https://0-academic-oup-com.brum.beds.ac.uk/neurosurgery/article-abstract/32/3/357/2755000 (accessed on 18 January 2023).
- Malham, G.M.; Thomsen, R.J.; Finlay, G.J.; Baguley, B.C. Subcellular Distribution and Photocytotoxicity of Aluminium Phthalocyanines and Haematoporphyrin Derivative in Cultured Human Meningioma Cells. Br. J. Neurosurg. 1996, 10, 51–57. [Google Scholar] [CrossRef]
- Tsai, J.C.; Hsiao, Y.Y.; Teng, L.J.; Chen, C.T.; Kao, M.C. Comparative Study on the ALA Photodynamic Effects of Human Glioma and Meningioma Cells. Lasers Surg. Med. 1999, 24, 296–305. [Google Scholar] [CrossRef]
- Sam Eljamel, M. Which intracranial lesions would be suitable for fluoresce guided resection? A prospective review of 110 consecutive lesions. In Proceedings of the Photodynamic Therapy: Back to the Future, Seattle, WA, USA, 11–15 June 2009; SPIE: Bellingham, WA, USA, 2009; Volume 7380, pp. 112–125. [Google Scholar]
- El-Khatib, M.; Tepe, C.; Senger, B.; Dibué-Adjei, M.; Riemenschneider, M.J.; Stummer, W.; Steiger, H.J.; Cornelius, J.F. Aminolevulinic Acid-Mediated Photodynamic Therapy of Human Meningioma: An in Vitro Study on Primary Cell Lines. Int. J. Mol. Sci. 2015, 16, 9936–9948. [Google Scholar] [CrossRef] [Green Version]
- Hefti, M.; Holenstein, F.; Albert, I.; Looser, H.; Luginbuehl, V. Susceptibility to 5-Aminolevulinic Acid Based Photodynamic Therapy in WHO I Meningioma Cells Corresponds to Ferrochelatase Activity. Photochem. Photobiol. 2011, 87, 235–241. [Google Scholar] [CrossRef]
- Sun, W.; Kajimoto, Y.; Inoue, H.; Miyatake, S.-I.; Ishikawa, T.; Kuroiwa, T. Gefitinib Enhances the Efficacy of Photodynamic Therapy Using 5-Aminolevulinic Acid in Malignant Brain Tumor Cells. Photodiagnosis Photodyn. Ther. 2013, 10, 42–50. [Google Scholar] [CrossRef]
- Cornelius, J.F.; Slotty, P.J.; El Khatib, M.; Giannakis, A.; Senger, B.; Steiger, H.J. Enhancing the Effect of 5-Aminolevulinic Acid Based Photodynamic Therapy in Human Meningioma Cells. Photodiagnosis Photodyn. Ther. 2014, 11, 1–6. [Google Scholar] [CrossRef]
- Ichikawa, M.; Akimoto, J.; Miki, Y.; Maeda, J.; Takahashi, T.; Fujiwara, Y.; Kohno, M. Photodynamic Therapy with Talaporfin Sodium Induces Dose- and Time-Dependent Apoptotic Cell Death in Malignant Meningioma HKBMM Cells. Photodiagnosis Photodyn. Ther. 2019, 25, 29–34. [Google Scholar] [CrossRef]
- Takahashi, T.; Suzuki, S.; Misawa, S.; Akimoto, J.; Shinoda, Y.; Fujiwara, Y. Photodynamic Therapy Using Talaporfin Sodium Induces Heme Oxygenase-1 Expression in Rat Malignant Meningioma KMY-J Cells. J. Toxicol. Sci. 2018, 43, 353–358. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, T.; Misawa, S.; Suzuki, S.; Saeki, N.; Shinoda, Y.; Tsuneoka, Y.; Akimoto, J.; Fujiwara, Y. Possible Mechanism of Heme Oxygenase-1 Expression in Rat Malignant Meningioma KMY-J Cells Subjected to Talaporfin Sodium-Mediated Photodynamic Therapy. Photodiagnosis Photodyn. Ther. 2020, 32, 102009. [Google Scholar] [CrossRef]
- Kirollos, R.W.; Marks, P.V.; Igbaseimokumo, U.; Chakrabarty, A. A Preliminary Experimental in Vivo Study of the Effect of Photodynamic Therapy on Human Pituitary Adenoma Implanted in Mice. Br. J. Neurosurg. 1998, 12, 140–145. [Google Scholar] [CrossRef]
- Marks, P.V.; Buxton, T.; Furneaux, C.E. In Vitro Study of the Effect of Photodynamic Therapy on Pituitary Adenomas. Br. J. Neurosurg. 1993, 7, 401–406. [Google Scholar] [CrossRef]
- Igbaseimokumo, U. Quantification of in Vivo Photofrin Uptake by Human Pituitary Adenoma Tissue. J. Neurosurg. 2004, 101, 272–277. [Google Scholar] [CrossRef]
- Marks, P.V.; Belchetz, P.E.; Saxena, A.; Igbaseimokumo, U.; Thomson, S.; Nelson, M.; Stringer, M.R.; Holroyd, J.A.; Brown, S.B. Effect of Photodynamic Therapy on Recurrent Pituitary Adenomas: Clinical Phase I/II Trial--an Early Report. Br. J. Neurosurg. 2000, 14, 317–325. [Google Scholar] [CrossRef]
- Nemes, A.; Fortmann, T.; Poeschke, S.; Greve, B.; Prevedello, D.; Santacroce, A.; Stummer, W.; Senner, V.; Ewelt, C. 5-ALA Fluorescence in Native Pituitary Adenoma Cell Lines: Resection Control and Basis for Photodynamic Therapy (PDT)? PLoS ONE 2016, 11, e0161364. [Google Scholar] [CrossRef]
- Neumann, L.M.; Beseoglu, K.; Slotty, P.J.; Senger, B.; Kamp, M.A.; Hänggi, D.; Steiger, H.J.; Cornelius, J.F. Efficacy of 5-Aminolevulinic Acid Based Photodynamic Therapy in Pituitary Adenomas-Experimental Study on Rat and Human Cell Cultures. Photodiagnosis Photodyn. Ther. 2016, 14, 77–83. [Google Scholar] [CrossRef]
- Cornelius, J.F.; Eismann, L.; Ebbert, L.; Senger, B.; Petridis, A.K.; Kamp, M.A.; Sorg, R.V.; Steiger, H.J. 5-Aminolevulinic Acid-Based Photodynamic Therapy of Chordoma: In Vitro Experiments on a Human Tumor Cell Line. Photodiagnosis Photodyn. Ther. 2017, 20, 111–115. [Google Scholar] [CrossRef]
- Gull, H.H.; Karadag, C.; Senger, B.; Sorg, R.V.; Möller, P.; Mellert, K.; Steiger, H.-J.; Hänggi, D.; Cornelius, J.F. Ciprofloxacin Enhances Phototoxicity of 5-Aminolevulinic Acid Mediated Photodynamic Treatment for Chordoma Cell Lines. Photodiagnosis Photodyn. Ther. 2021, 35, 102346. [Google Scholar] [CrossRef]
- Briel-Pump, A.; Beez, T.; Ebbert, L.; Remke, M.; Weinhold, S.; Sabel, M.C.; Sorg, R.V. Accumulation of Protoporphyrin IX in Medulloblastoma Cell Lines and Sensitivity to Subsequent Photodynamic Treatment. J. Photochem. Photobiol. B 2018, 189, 298–305. [Google Scholar] [CrossRef]
- Schwake, M.; Nemes, A.; Dondrop, J.; Schroeteler, J.; Schipmann, S.; Senner, V.; Stummer, W.; Ewelt, C. In-Vitro Use of 5-ALA for Photodynamic Therapy in Pediatric Brain Tumors. Neurosurgery 2018, 83, 1328–1337. [Google Scholar] [CrossRef]
- Kast, R.E.; Michael, A.P.; Sardi, I.; Burns, T.C.; Heiland, T.; Karpel-Massler, G.; Kamar, F.G.; Halatsch, M.-E. A New Treatment Opportunity for DIPG and Diffuse Midline Gliomas: 5-ALA Augmented Irradiation, the 5aai Regimen. Brain Sci. 2020, 10, 51. [Google Scholar] [CrossRef] [Green Version]
- Chiba, K.; Aihara, Y.; Oda, Y.; Fukui, A.; Tsuduki, S.; Saito, T.; Nitta, M.; Muragaki, Y.; Kawamata, T. Photodynamic Therapy for Malignant Brain Tumors in Children and Young Adolescents. Front. Oncol. 2022, 12, 957267. [Google Scholar] [CrossRef]
- Stepp, H.; Stummer, W. 5-ALA in the Management of Malignant Glioma. Lasers Surg. Med. 2018, 50, 399–419. [Google Scholar] [CrossRef] [Green Version]
- Kawai, N.; Hirohashi, Y.; Ebihara, Y.; Saito, T.; Murai, A.; Saito, T.; Shirosaki, T.; Kubo, T.; Nakatsugawa, M.; Kanaseki, T.; et al. ABCG2 Expression Is Related to Low 5-ALA Photodynamic Diagnosis (PDD) Efficacy and Cancer Stem Cell Phenotype, and Suppression of ABCG2 Improves the Efficacy of PDD. PLoS ONE 2019, 14, e0216503. [Google Scholar] [CrossRef] [Green Version]
- Blake, E.; Curnow, A. The Hydroxypyridinone Iron Chelator CP94 Can Enhance PpIX-Induced PDT of Cultured Human Glioma Cells. Photochem. Photobiol. 2010, 86, 1154–1160. [Google Scholar] [CrossRef]
- Chen, X.; Wang, C.; Teng, L.; Liu, Y.; Chen, X.; Yang, G.; Wang, L.; Liu, H.; Liu, Z.; Zhang, D.; et al. Calcitriol Enhances 5-Aminolevulinic Acid-Induced Fluorescence and the Effect of Photodynamic Therapy in Human Glioma. Acta Oncol. 2014, 53, 405–413. [Google Scholar] [CrossRef]
- Wang, C.; Chen, X.; Wu, J.; Liu, H.; Ji, Z.; Shi, H.; Gao, C.; Han, D.; Wang, L.; Liu, Y.; et al. Low-Dose Arsenic Trioxide Enhances 5-Aminolevulinic Acid-Induced PpIX Accumulation and Efficacy of Photodynamic Therapy in Human Glioma. J. Photochem. Photobiol. B 2013, 127, 61–67. [Google Scholar] [CrossRef]
- Coupienne, I.; Bontems, S.; Dewaele, M.; Rubio, N.; Habraken, Y.; Fulda, S.; Agostinis, P.; Piette, J. NF-kappaB Inhibition Improves the Sensitivity of Human Glioblastoma Cells to 5-Aminolevulinic Acid-Based Photodynamic Therapy. Biochem. Pharmacol. 2011, 81, 606–616. [Google Scholar] [CrossRef] [Green Version]
- Albert, I.; Hefti, M.; Luginbuehl, V. Physiological Oxygen Concentration Alters Glioma Cell Malignancy and Responsiveness to Photodynamic Therapy in Vitro. Neurol. Res. 2014, 36, 1001–1010. [Google Scholar] [CrossRef]
- Dereski, M.O.; Madigan, L.; Chopp, M. The Effect of Hypothermia and Hyperthermia on Photodynamic Therapy of Normal Brain. Neurosurgery 1995, 36, 141–146. [Google Scholar] [CrossRef]
- Fisher, C.J.; Niu, C.; Foltz, W.; Chen, Y.; Sidorova-Darmos, E.; Eubanks, J.H.; Lilge, L. ALA-PpIX Mediated Photodynamic Therapy of Malignant Gliomas Augmented by Hypothermia. PLoS ONE 2017, 12, e0181654. [Google Scholar] [CrossRef] [Green Version]
- Christie, C.; Molina, S.; Gonzales, J.; Berg, K.; Nair, R.K.; Huynh, K.; Madsen, S.J.; Hirschberg, H. Synergistic Chemotherapy by Combined Moderate Hyperthermia and Photochemical Internalization. Biomed. Opt. Express 2016, 7, 1240–1250. [Google Scholar] [CrossRef] [Green Version]
- Fisher, C.J.; Niu, C.J.; Lai, B.; Chen, Y.; Kuta, V.; Lilge, L.D. Modulation of PPIX Synthesis and Accumulation in Various Normal and Glioma Cell Lines by Modification of the Cellular Signaling and Temperature. Lasers Surg. Med. 2013, 45, 460–468. [Google Scholar] [CrossRef]
- Ghogare, A.A.; Rizvi, I.; Hasan, T.; Greer, A. “Pointsource” Delivery of a Photosensitizer Drug and Singlet Oxygen: Eradication of Glioma Cells in Vitro. Photochem. Photobiol. 2014, 90, 1119–1125. [Google Scholar] [CrossRef] [Green Version]
- Girotti, A.W. Upregulation of Nitric Oxide in Tumor Cells as a Negative Adaptation to Photodynamic Therapy. Lasers Surg. Med. 2018, 50, 590–598. [Google Scholar] [CrossRef]
- Girotti, A.W.; Fahey, J.M.; Korytowski, W. Nitric Oxide-Elicited Resistance to Anti-Glioblastoma Photodynamic Therapy. Cancer Drug Resist 2020, 3, 401–414. [Google Scholar] [CrossRef]
- Fahey, J.M.; Emmer, J.V.; Korytowski, W.; Hogg, N.; Girotti, A.W. Antagonistic Effects of Endogenous Nitric Oxide in a Glioblastoma Photodynamic Therapy Model. Photochem. Photobiol. 2016, 92, 842–853. [Google Scholar] [CrossRef] [Green Version]
- Fahey, J.M.; Stancill, J.S.; Smith, B.C.; Girotti, A.W. Nitric Oxide Antagonism to Glioblastoma Photodynamic Therapy and Mitigation Thereof by BET Bromodomain Inhibitor JQ1. J. Biol. Chem. 2018, 293, 5345–5359. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y.; Luk, S.K.; Chuang, C.P.; Yip, S.P.; To, S.S.T.; Yung, Y.M.B. TP53 Regulates Human AlkB Homologue 2 Expression in Glioma Resistance to Photofrin-Mediated Photodynamic Therapy. Br. J. Cancer 2010, 103, 362–369. [Google Scholar] [CrossRef] [Green Version]
- Li, B.O.; Meng, C.; Zhang, X.; Cong, D.; Gao, X.; Gao, W.; Ju, D.; Hu, S. Effect of Photodynamic Therapy Combined with Torasemide on the Expression of Matrix Metalloproteinase 2 and Sodium-Potassium-Chloride Cotransporter 1 in Rat Peritumoral Edema and Glioma. Oncol. Lett. 2016, 11, 2084–2090. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Cong, D.; Shen, D.; Gao, X.; Chen, L.; Hu, S. The Effect of Bumetanide on Photodynamic Therapy-Induced Peri-Tumor Edema of C6 Glioma Xenografts. Lasers Surg. Med. 2014, 46, 422–430. [Google Scholar] [CrossRef]
- Gupta, S.; Dwarakanath, B.S.; Muralidhar, K.; Koru-Sengul, T.; Jain, V. Non-Monotonic Changes in Clonogenic Cell Survival Induced by Disulphonated Aluminum Phthalocyanine Photodynamic Treatment in a Human Glioma Cell Line. J. Transl. Med. 2010, 8, 43. [Google Scholar] [CrossRef] [Green Version]
- Hefti, M.; Albert, I.; Luginbuehl, V. Phenytoin Reduces 5-Aminolevulinic Acid-Induced Protoporphyrin IX Accumulation in Malignant Glioma Cells. J. Neurooncol. 2012, 108, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Misuth, M.; Horvath, D.; Miskovsky, P.; Huntosova, V. Synergism between PKCδ Regulators Hypericin and Rottlerin Enhances Apoptosis in U87 MG Glioma Cells after Light Stimulation. Photodiagnosis Photodyn. Ther. 2017, 18, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Chopp, M.; Lu, Y.; Jiang, J.; Zhao, D.; Ding, C.; Yang, H.; Zhang, L.; Jiang, F. Atorvastatin Reduces Functional Deficits Caused by Photodynamic Therapy in Rats. Int. J. Oncol. 2011, 39, 1133–1141. [Google Scholar] [PubMed]
- Pridham, K.J.; Shah, F.; Hutchings, K.R.; Sheng, K.L.; Guo, S.; Liu, M.; Kanabur, P.; Lamouille, S.; Lewis, G.; Morales, M.; et al. Connexin 43 Confers Chemoresistance through Activating PI3K. Oncogenesis 2022, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.-P.; Bai, L.-R.; Lv, Y.-F.; Zhou, Y.; Ding, C.-H.; Yang, S.-M.; Zhang, F.; Huang, J.-L. A Novel Role of Cx43-Composed GJIC in PDT Phototoxicity: An Implication of Cx43 for the Enhancement of PDT Efficacy. Int. J. Biol. Sci. 2019, 15, 598–609. [Google Scholar] [CrossRef]


{kind=link}
| Photosensitizer | Intracellular Localization | Excitation Wavelength (nm) | Treatment Window a | Clearance Time | Tumor: Normal Fluorescence Ratio b | Administration | Side Effects | |
|---|---|---|---|---|---|---|---|---|
| First Generation | Porfimer Sodium | Inner mitochondrial membrane | 630 | 48–150 h | 4–8 weeks | 2.5–4:1 | Systemic | Skin sensitization, thrombocytopenia |
| Hematoporphyrin derivative [HpD] | 408, 510, 630 c | 24–48 h | 4–6 weeks | Systemic | ||||
| Dihematoporphyrin ether [DHE] | 395, 630 c | 24–72 h | 4–6 weeks | Systemic | ||||
| Second Generation | 5-Aminolevulinic Acid (Levulin®, Gliolan®) | Early: mitochondria Late: plasma membrane, lysosomes | 410, 510, 635 c | 4–8 h | 2 days | 10–20:1 | Oral | Skin sensitization, nausea, elevated liver enzymes, anemia |
| Talaporfin sodium (Laserphyrin, AptocineTM, LS11, PhotoIon®) | Lysosomes | 664 | 12–26 h | 15 days | ND | Systemic | Skin sensitization | |
| Temoporfin [m-THPC; m-tetrahydroxyphenylchlorin] (Foscan®, liquid formulation; Foslip®, liposomal formulation) | Strong: Golgi apparatus, Endoplasmic reticulum Weak: mitochondria, lysosomes | 652 | 48–110 h | 15 days | 150:1 | Systemic | Skin sensitization | |
| Boronated protoporphyrin [BOPP] | Lysosomes | 630 | 24 h | 4–6 weeks | 400:1 | Systemic | Skin sensitization, thrombocytopenia | |
| Benzoporphyrin derivative [BPD] | Lysosomes | 680–690 | 15–30 min. | 1–5 days | ND | Systemic | Vascular damage |
| Study Group a (n, Number of GBM Patients in Study) | Mean Age | PS b | Dose c | Route d | Time Prior to Photoillumination | Photoillumination Method e | Laser/Light Wavelength f (nm) | Photoillumination Energy (ED unless Otherwise Specified) | Reported Survival g | Survival Statistics | Adverse Events | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Perria et al. (1980) | GBM | 2 | n/a | HpD | 5 mg/kg | IV | n/a | n/a | 628 | 720–2400 J/cm2 | MS | GBM | 6.9 mo | n/a |
| Laws et al. (1981) | rMG | 5 | 14–75 | HpD | 5 mg/kg | IV | 48–72 h | Interstitial | 630 | 30–60 mW/cm2 § | TTP | rMG | 1–6 mo | Increased skin photosenstivity |
| McCulloch et al. (1984) | GBM | 9 | n/a | HpD | 5 mg/kg | IV | n/a | n/a | 627.8 (>1 laser) | n/a | OS | GBM (n = 3) | 17–42 mo | Increase in P/O cerebral edema |
| Muller and Wilson (1985) h | GBM rGBM | 1 2 | 53 32, 44 | HpD | 2.5 mg/kg 2 mg/kg | IV | 24 h | Cavitary (balloon) | 630 | 8–68 J/cm2 | n/a | None | ||
| Kaye et al. (1987) i | GBM rGBM | 13 6 | 45 *** 40 *** | HpD | 5 mg/kg | IV | 24 h | Interstitial | AI (9) GMVL (14) | 70–120 J/cm2 120–230 J/cm2 | PFS | GBM rGBM | 3–13 mo 12–16 wk | No AEs |
| Kostron et al. (1987) j | GBM | 6 | 63.3 | HpD | 1.0 mg/cm3 | IV IA Direct tumor | 3 d | LED (n = 9) Cavitary (n = 5) | 620–640 632 | 422 J/cm2 § <1600 J/cm2 § | MS/OS | GBM | 12 mo | IA/Direct tolerated without skin phototoxicity |
| rGBM (1x) | 5 | 50.8 | rGBM (1x) | 2–7 mo | ||||||||||
| rGBM (mult) | 3 | 57.0 | rGBM (mult) | 5 mo | ||||||||||
| Muller and Wilson (1987) h | [HpD] GBM | 1 | 52 | HpD (8) DHE (24) | 2.14 mg/kg 2.08 mg/kg | IV | 18–24 h | Cavitary | 630 | HpD: 32 J/cm2 DHE: 23 J/cm2 | MS | [HpD] GBM | 2.9 mo | Skin photosensitivity (n = 3) |
| [HpD] rGBM | 1 | 32 | [HpD] rGBM | 5.8 mo | ||||||||||
| [DHE] GBM | 7 | 58.3 | Total dose | 150 mg | [DHE] GBM | 1.1–13.6 mo | ||||||||
| [DHE] rGBM | 7 | 39.4 | [DHE] rGBM | 0.2–10.7 mo | ||||||||||
| Kostron et al. (1988) j | GBM | 8 | 55 ** | HpD | 1 mg/cm3 | IV, IA and/or Direct | 3 d | LED Cavitary | 590–750 632 | 422 J/cm2 § 60–200 J/cm2 | OS | GBM rGBM (1x) rGBM (mult) | 0.5–19 m 3–14 mo 1–6 mo | Skin phototoxicity (IA/IV only) |
| rGBM (1x) | 9 | |||||||||||||
| rGBM (mult) | 3 | |||||||||||||
| HPD only (n = 9), [HPD+single dose radiation of 4 Gy fast electrons] (n=10), [HPD+single dose radiation+conventional radiotherapy] (n = 4); 3 cases of recurrence and subsequent re-treatment. | ||||||||||||||
| Kostron et al. (1990) j | GBM rGBM | 9 18 | n/a | HpD | n/a | IV, IA and/or Direct | n/a | Interstitial | 630 | 40–220 J/cm2 | OS | GBM rGBM | 0.5–29 mo 4–13 mo | Increased phototoxicity of the skin |
| Muller and Wilson (1990) h | GBM rGBM | 9 14 | 48 | HpD DHE | 5 mg/kg 2 mg/kg | IV | 18–24 h | Cavitary | 630 | 24 J/cm2 | MS | GBM + rGBM | 6.3 mo | Increased skin photosensitivity |
| Powers et al. (1991) | rGBM rMG | 1 5 | 42–61 | HPE | 2.0 mg/kg | IV | 24 h | Interstitial | 630 | 1000 J §§ | TTP | rGBM rMG | 2–27 wk 6–45 wk | Edema, increased intracranial pressure and skin photosensitivity |
| Origitano et al. (1993) | rGBM | 8 | 42.2 | PNa | 2.0 mg/kg | IV | 48–72 h | Cavitary Interstitial + post-resection cavitary | 630 630 | 50 J/cm2 100 J/cm per fiber | TTP | rGBM | 5–22 mo | Increased skin photosensitivity |
| Muller and Wilson (1995) h | rGBM | 32 | 41 ** | HpD PNa HPE | 5 mg/kg 2 mg/kg 2 mg/kg | IV IV IV | 12–36 h | Cavitary | 630 | 38 J/cm2 | MS | [Stratify by light dose] Energy: >1700 J <1700 J | 28 wk 29 wk | Edema, increased skin photosensitivity |
| Popovic et al. (1995) i | GBM rGBM | 38 40 | n/a | HpD | 2.0–2.5 mg/kg | IV | 24 h | Cavitary | AI: 1986–1987 GMVL: 1987–1994 | 240–260 J/cm2 (initial pts: 70) | MS | GBM rGBM | 24 mo 9 mo | n/a |
| Muller and Wilson (1997) h | GBM rGBM | 11 32 | 40 58 | PNa | 2 mg/kg | IV | 12–36 h | Cavitary | 630 | GBM: 30 J/cm2 * rGBM: 43 J/cm2 * | MS | GBM rGBM | 37 wk 30 wk | Increased P/O cerebral edema |
| Muller et al. (2001) [Phase II] h | rGBM (ED ≤ 50) (ED ≥ 50) | 37 (22) (15) | 41 ** | PNa | 2 mg/kg | IV | 12–36 h | Cavitary | 630 | 8–110 J/cm2 | MS | rGBM (ED ≤ 50) (ED ≥ 50) | avg 29 wk (29 wk) (34 wk) | Increased P/O cerebral edema |
| Muller et al. (2001) [Phase III] h | GBM High light | 20 | 54 | PNa | 2 mg/kg | IV | 12–36 h | Cavitary | 630 | 30–50 J/cm2 (low) 110–130 J/cm2 (high) | MS | GBM High | 92 wk | n/a |
| rGBM Low light High light | 26 26 | 48 52 | rGBM Low High | 29 wk 51 wk | ||||||||||
| Schmidt et al. (2004) | Recurrent brain tumors (include GBM) | NS | n/a | PNa | 0.75 mg/kg 1.20 mg/kg 1.60 mg/kg 2.00 mg/kg | IV | 18–24 h | Laser/LED + Cavitary balloon | Laser: 630 LED: 20–25 | 100 J/cm2 | Not specified | No neurotoxicity | ||
| Stylli et al. (2004) i | GBM rGBM | 31 27 | 44 *** | HpD | 5 mg/kg | IV | 24 h | Cavitary | AI: 1986–1987 GMVL: 1987–1994 KTP: 1994–2000 | 240 J/cm2 §§ | MS | GBM/rGBM | 24 mo | n/a |
| Stylli et al. (2005) i | GBM rGBM | 31 55 | 47 * 42 * | HpD | 5 mg/kg | IV | 24 h | Cavitary | AI: 1986–1987 GMVL: 1987–1994 KTP: 1994–2000 | 240 J/cm2 §§ | MS | GBM rGBM | 14.3 mo 13.5 mo | Increased cerebral edema (n = 3) |
| Muller et al. (2006) h | GBM rGBM | 12 37 | 59 41 | PNa | 2 mg/kg | IV | 12–36 h | Cavitary (balloon/cont. filling with Intralipid) +/− interstitial | AI KTP | 58 J/cm2 §§§ | MS | GBM rGBM | 33 wk 29 wk | Skin photosensitivity |
| Kaneko (2008) | GBM | 26 | n/a | HPE | 3 mg/kg | IV | 2 d | Interstitial | 640 | 180 J/cm | n/a | n/a | ||
| Study Group a (n, Number of Patients with Disease and Treatment) | Mean Age | PS b | Dose c | Route d | Time Prior to Photoillumination | Photoillumination Method e | Laser/Light Wavelength f (nm) | Photoillumination Energy g (ED unless otherwise specified) | Reported Survival h | Survival Statistics | Adverse Events | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kostron et al. (1998) | GBM rGBM | 2 8 | 61–72 34–72 | mTHPC x | 0.15 mg/kg | IV | 4 d | Interstitial I/O cavitary | KTP 652 | 300 mW/cm2 § 20 J/cm2 | TTP MS | rGBM rGBM | 4 mo 6 mo | Phototoxicity |
| Rosenthall et al. (2001/2003) i | GBM rGBM | 7 9 | 51 * | BOPP | 0.25–8.0 mg/kg | IV | 24 h | I/O fiber diffuser for focused surface irradiation | 630 | 25 J/cm2 | MS | GBM rGBM | 5 mo 11 mo | n/a |
| Schmidt et al. (2004) | Recurrent brain tumors (including GBM) | NS | n/a | BPD | 0.25 mg/kg | IV | 3–6 h | Laser fiber optic catheter/balloon LED balloon | 680 | 1,800 J §§ (at 100 J/cm2) | Not specified | No cytotoxic effects | ||
| Kostron et al. (2006) | GBM | 26 | n/a | mTHPC x | 0.15 mg/kg | IV | 4 d | I/O cavitary I/O fiber diffuser | KTP 652 | 300 mW/cm2 § 20 J/cm2 | MS | GBM | 15 mo | Increased skin sensitivity |
| Beck et al. (2007) | rGBM | 10 | 51.7 | 5-ALA | 20 mg/kg | Oral | 1 h | I/O fiber diffuser for focused surface irradiation | 633 | 100 J/cm2 | MS | 15 m | n/a | |
| Elijamel et al. (2007) | GBM, PDT(+) GBM, PDT(−) | 13 14 | 59.6 60.1 | 5-ALA -- | 20 mg/kg -- | Oral -- | 3 h -- | P/O cavitary balloon | 630 | 100 J/cm2 | PFS MS | GBM | 8.6 mo 52.8 wk | Deep venous thrombosis (n = 2) |
| Stepp et al. (2005) | GBM | 5 | n/a | 5-ALA | 20 mg/kg | Oral | 3 h | I/O fiber diffuser for focused surface irradiation | 633 | 100–200 J/cm2 | n/a | n/a | ||
| Stepp et al. (2007) | GBM (a) GBM (b) GBM (c) | 5 8 7 | n/a | 5-ALA | 20 mg/kg | Oral | 3 h | I/O fiber diffuser for focused surface irradiation | 633 | (a) 100 J/cm2 (b) 150 J/cm2 (c) 200 J/cm2 | n/a | No AEs | ||
| Akimoto et al. (2012) | GBM rGBM | 6 8 | 49–82 41–61 | TS | 40 mg/m2 | IV | 24 h | I/O fiber diffuser for focused surface irradiation (1.0 cm diameter) | 664 | 27 J/cm2 | PFS | GBM | 24.8 mo | Increased photosensivity |
| Lyons et al. (2012) | Total (GBM) PDT(+) PDT(−) PDT(+): [a], [b] PDT(-): [c], [d] | 73 30 43 17, 13 18, 25 | 59 ** | 5-ALA | 20 mg/kg | Oral | 3 h | [a] IORT, I/O cavitary, MSR [b] I/O cavitary, MSR [c] IORT, MSR [d] MSR only | 630 | 100 J/cm2 | PFS MS | [a] [b] PDT+ PDT- | 79 wk 39.7 wk 62.9 wk 20.6 wk | n/a |
| Johansson et al. (2013) | GBM rGBM | 1 4 | 42 56 | 5-ALA | 20–30 mg/kg | Oral | 5–8 h | Interstitial | 635 | 720 J/cm2 | TTP | 3–36 mo | n/a | |
| Muragaki et al. (2013) | GBM | 13 | 47.1 ** | TS | 40 mg/m2 | IV | 22–27 h | I/O fiber diffuser for focused surface irradiation (1.5 cm diameter) | 664 | 27 J/cm2 | PFS MS | 12 mo 27.9 mo | Increased photosensitivity | |
| Schwartz et al. (2015) | GBM | 15 | n/a | 5-ALA | 20 mg/kg 30 mg/kg | Oral | n/a | Interstitial | 633 | 12.96 J §§ | PFS MS | 16 m 34 m | Transient aphasia, pulmonary embolism | |
| Vanaclocha et al. (2015) | GBM | 20 | 49 *** | DHE mTHPC x | 2 mg/kg 0.15 mg/kg | IV | 48 h 96 h | I/O cavitary | 630 652 | 75 J/cm2 20 J/cm2 | PFS MS MS (from 1st diagnosis) | 10 mo 9 mo 17 mo | Skin photosensitivity dermatitis | |
| Nitta et al. (2018) | GBM | 11 | 54 | TS | 40 mg/m2 | IV | 22–26 h | I/O fiber diffuser for focused surface irradiation (1.5 cm diameter) | 664 | 27 J/cm2 | PFS MS | 19.6 mo27.5 mo | Asymptomatic transient peripheral edema | |
| Shimizu et al. (2018) | GBM rGBM | 7 7 | 45–74 40–69 | TS | 40 mg/m2 | IV | 22–26 h | I/O fiber diffuser for focused surface irradiation (1.5 cm diameter) | 664 | 100 J/cm2 | n/a | Pulmonary embolism (if vessels are not shielded) | ||
| Lietke et al. (2021) | rGBM | 37 | 49.4 * | 5-ALA | 20 mg/kg | Oral | 3–5 h | Interstitial | 635 | 8883 J §§ | TTP MS (from 1st diagnosis) | Study combines GBM and AA | 7.1 mo 39.7 mo | Transient worsening of pre-existing neurological deficits |
| Vermandel et al. (2021) | GBM | 10 | 57.1 * | 5-ALA | 20 mg/kg | Oral | 6 h | I/O cavitary | 635 | 200 J/cm2 | PFS MS | 17.1 mo 23.1 mo | No AEs | |
| Kobayashi et al. (2022) | GBM | 43 | 46.7 ** | TS | 40 mg/m2 | IV | 22–26 h | I/O fiber diffuser for surface irradiation (1.5 cm diameter) | 664 | 27 J/cm2 | PFS MS | 6.3 mo 15.4 mo | No AEs | |
| Kozlikina et al. (2022) | GBM | CR | 29 | 5-ALA + Ce6 | 20 mg/kg 1 mg/kg | Oral IV | 4–4.5 h 3–3.5 h | I/O fiber | 660 | 60 J/cm2 §§§ | n/a | n/a | ||
| Study Name | Trial Phase (Study ID) | Type of Cancer | Drug | Principal Investigator |
|---|---|---|---|---|
| Photodynamic Therapy (PDT) for malignant brain tumor in children | Phase I/II (UMIN000030883) | Brain Tumor (Pediatric) | TS (Leserphyrin) | Kawamata Takakazu (Tokyo Women’s Medical University) |
| Clinical Safety Study on 5-Aminolevulinic Acid (5-ALA) in Children and Adolescents With Supratentorial Brain Tumors | Phase II (NCT04738162) | Brain Tumor (Pediatric) | 5-ALA (Gliolan) | Walter Stummer (Univ. Hospital, Münster) |
| Stereotactical Photodynamic Therapy With 5-aminolevulinic Acid (Gliolan®) in Recurrent Glioblastoma | Phase II (NCT04469699) | GBM | 5-ALA (Gliolan) | Walter Stummer (Univ. Hospital, Münster) |
| PD L 506 for Stereotactic Interstitial Photodynamic Therapy of Newly Diagnosed Supratentorial IDH Wild-type Glioblastoma | Phase II (NCT03897491) | GBM | 5-ALA (PD L 506) | Niklas Thon (Univ. Hospital, Munich) |
| Dose Finding for Intraoperative Photodynamic Therapy of Glioblastoma | Phase II (NCT04391062) | GBM | 5-ALA (Gliolan) | Nicholas Reyns (Univ. Hospital, Lille) |
| Study to Evaluate 5-ALA Combined With CV01 Delivery of Ultrasound in Recurrent High Grade Glioma | Phase I (NCT05362409) | High Grade Glioma | 5-ALA (Gliolan) | Alpheus Medical (Wash. Univ. St. Louis, Dent Institute, Northwell Health) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsia, T.; Small, J.L.; Yekula, A.; Batool, S.M.; Escobedo, A.K.; Ekanayake, E.; You, D.G.; Lee, H.; Carter, B.S.; Balaj, L. Systematic Review of Photodynamic Therapy in Gliomas. Cancers 2023, 15, 3918. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15153918
Hsia T, Small JL, Yekula A, Batool SM, Escobedo AK, Ekanayake E, You DG, Lee H, Carter BS, Balaj L. Systematic Review of Photodynamic Therapy in Gliomas. Cancers. 2023; 15(15):3918. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15153918
Chicago/Turabian StyleHsia, Tiffaney, Julia L. Small, Anudeep Yekula, Syeda M. Batool, Ana K. Escobedo, Emil Ekanayake, Dong Gil You, Hakho Lee, Bob S. Carter, and Leonora Balaj. 2023. "Systematic Review of Photodynamic Therapy in Gliomas" Cancers 15, no. 15: 3918. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15153918