1. Introduction
Squamous cell carcinoma of the skin (cSCC) is the second-most-frequent skin cancer after basal cell carcinoma [
1]. Risk localisations of cSCC include the ear and lip, which display an increased risk of lymph node metastases (LNMs) compared to other tumour localisations. Alam et al. showed that the localisations of cSCC at the external ear (ECSCC) and lip (LSCC) with recurrence and metastasis rates of 8–25% are more aggressive than other localisations [
2]. Furthermore, the localisation in the lip area has an influence on the tumour aggressiveness, so that LSCC is more aggressive when oral mucosa is affected [
3]. However, the lymph node metastasis status (N+ or N−) is one of the most-important prognostic factors in cSCC of the head and neck [
2,
4,
5]. The distinction between N+ and N− patients is very important, as N+ patients have a worse prognosis and a lower 5-year survival rate. N− patient had a 5-year survival of 87–95%, and N+ had only survival rates of 25–50% [
6]. Especially patients with high-risk localisations LSCC and ECSCC benefit from risk prediction. In addition to the prognostic assessment, the risk evaluation of LNMs and the indication for neck dissection are controversial topics among different disciplines [
1].
In terms of individualised medicine, there is a particular need for research on predictive tumour markers. For example, a predictive model for LSCC has been created. A study by Wermker et al. showed that, with the help of tumour thickness and grading, a risk stratification and evaluation for LNMs could be made [
6]. In contrast to the histopathomorphological risk constellations, immunohistochemical markers could also be helpful in the prognostic evaluation of high-risk localisations of cSCC.
The insulin-like growth factor 2 mRNA-binding protein 3 (IGF2BP3, also named IMP3) could be a tumour marker with such a potential. IMP3 is an RNA-binding oncofetal protein [
7]. Different studies have shown that these proteins have important implications in cell function, polarisation, cell migration, morphology, cellular metabolism, proliferation, and differentiation [
7,
8,
9]. Gong et al. presented that IMP3 expression supports tumour cell proliferation, tumour cell adhesion, and tumour cell invasion [
10]. There is also evidence of a link between increased IMP3 expression and advanced tumour stage [
11]. In a meta-analysis in 2017, Chen et al. showed that the level of IMP3 expression correlates significantly with a decreased overall survival (OS) in different tumour entities. The authors evaluated 53 studies covering numerous tumour entities including renal cancer, lung cancer, oral cancer, and gastrointestinal cancer. There were positive correlations of high IMP3 expression with worse overall survival, disease-specific survival, and metastasis-free survival. To summarise, a high IMP3 expression is associated with a worse prognosis [
12].
In oral squamous cell carcinoma (oSCC), high IMP3 expression correlates with lymph node metastasis (N+) and decreased 5-year survival. If two patients had the same tumour stage, but different IMP3 expression levels, the patient with the higher IMP3 expression had a worse prognosis [
13].
The aim of our study was to analyse if the marker IMP3 can be used in a clinical setting to assess the aggressiveness of high-risk localisations of cSCC. The aggressiveness was determined with the overall survival rate, disease-specific survival, occurrence of local relapses, and progression-free survival. The key question was if the IMP3 analysis methods (IMP3 Analysis Category I (<25%, 25–50%, 50–75%, >75%), IMP3 Analysis Category II (0%, 1–20%, 21–60%, >60%), IMP3 Analysis Category III (>50%; <50%)) were usable for risk prediction for N+ cases (correlated with worse prognosis). It seems that one of the IMP3 analysis categories (IMP3 Analysis Category II) is particularly suitable in terms of outcome prediction.
2. Materials and Methods
2.1. Ethics Statement
This study was approved by the local ethics committee (Ethical Committee of the Westphalian Wilhelms University Muenster, Approval No. 2013-063-f-S) and was conducted in accordance with the Guidelines for Good Clinical Practice and in compliance with the Declaration of Helsinki. All patients gave their written informed consent for participating in this study.
2.2. Patients
All included patients were > 18 years old and had a histologically proven cSCC of the lip (LSCC) or ear (ECSCC). Included localisations for LSCC were the upper lip and lower lip. The following localisations were defined for the ECSCC: helix, cavum conchae/anthelix/tragus, retroauricular/posterior side, or a combination with more than one of these regions. All patients were resected R0 in the primary tumour.
Each patient had a preoperative stay with a minimum diagnostic procedure of sonography of the head and neck, X-ray of the thorax, and abdominal sonography. All patients were presented in an interdisciplinary tumour board. After the therapy, all patients received a periodic recall. The exclusion criteria were: no written consent and condition according to neck dissection or different HNSCC than in the inclusion criteria. Further data included in the correlation analysis were: follow-up time, first diagnosis, tumour localisation, local recurrence, lymph node metastasis, distant metastasis, disease-specific death, and overall survival.
The electronic patient data were complete and had a follow-up of at least 24 months. The abuse of alcohol or tobacco was not part of the exclusion criteria.
All patients (n = 122) were divided into two main groups and subsequently into two subgroups. Allocation to the two main groups was based on the localisation: LSCC and ESCC. These were then further subdivided into cases of N+ or N−. In addition, subgroup division into LSCC and ECSCC and lymph node status was performed: LSCC N−, LSCC N+, ECSCC N−, ECSCC N+.
In addition, a subdivision was performed for nodal status with both cases: N+ (LSCC N+ and ECSCC N+) and N− (LSCC N− + ECSCC N−).
The matched pair approach was used, as it allows a certain homogeneity to be achieved. The following groups were compared: LSCC N− vs. LSCC N+ and ECSCC N− vs. ECSCC N+. Each patient from the respective group was contrasted with a patient from the other group and with clinically pathologically selected known risk factors with as few differences as possible.
Included parameters for matching were: age, gender, grading, T-stadium, primary tumour localisation, tumour infiltration depth, perineural growth, cartilage invasion (only for ECSCC), comorbidities, and immunosuppression (classification into none, weak, moderate, strong). Finally, IMP3 expression (different IMP3 expression ranges; see below) was correlated with clinical pathological data.
2.3. Immunohistochemistry Analysis of IMP3
The selection of suitable tumour samples was made on Haematoxylin-Eosin-stained slices. The tumour tissue (histologically proven LSCC and ECSCC) was fixed in 10% formaldehyde solution.
Incubation with a primary antibody against IMP3 (anti-IMP3 Clon 69.1, 1:50, Agilent/Dako (Glostrup, Denmark)) was performed in the Autostainer Plus (Dako REAL DETECTION SYSTEM K5005, Glostrup). The tissue slices were incubated with the secondary (Dako REAL Link Biotinylated secondary antibody (AB2), Glostrup) antibody (exposure time 15 min) and then with Dako Real Streptavidin Alkaline Phosphatase (AP) (Glostrup; exposure time 15 min). Afterwards the SCC tissue slices were exposed to chromogen (Dako RED Chromogen, Glostrup) for 8 min. Next, Haematoxylin (nucleus counterstain/eight-minute exposure time) was applied. Coverslip tape was used.
The cellular localisation of IMP3 staining was determined by the Olympus BX51 microscope (Hamburg, Germany).
Two investigators blinded to the patients’ prognostic data analysed each slice with a first overview and then divided each slice into 5 high-power fields (HPFs) with a magnification of 400× after randomisation.
In every HPF, the investigator counted 5 × 10 tumour cells, totalling 50 cells per HPF and 250 cells in each slice. All tumour cells with a positive dark brown colour in the cytoplasm were counted as positive. Tonsil tissue was used as the positive control. The expression analysis was according to the literature [
13,
14]. In the event of discrepancies between the investigators, the case was reevaluated in a shared discussion.
The study focused on three different analysis categories. The aim was to find which expression range is most suitable for prognostic use. The expression was analysed in % ranges of expression: IMP3 Analysis Category I (<25%, 25–50%, 50–75%, >75%), IMP3 Analysis Category II (0%, 1–20%, 21–60%, >60%), IMP3 Analysis Category III (>50%; <50%). These three categories are presented in the Results Section.
2.4. Statistical Analysis
All statistical analyses were performed by using the Statistical Package for Social Sciences (SPSS) Version 22.0 for Windows® (SPSS Inc., Chicago, IL, USA).
Categorical variables were analysed using the chi-squared test and Fisher’s exact test. For continuous variables, the Mann–Whitney U-test was used as a non-parametric test for abnormally distributed data, and an independent t-test was used to analyse normally distributed variables. Disease-specific survival (time from first diagnosis until tumour-dependent death; data on patients without tumour-dependent death were censored at the last follow-up time) and progression-free survival (time from first diagnosis until local recurrence or metastasising; data on patients without an event of progression were censored at the last follow-up time) were calculated using the Kaplan–Meier method, and group differences were analysed using the log-rank test.
3. Results
In the first part of the results, an overview of the patient cohort will be given, followed by the correlation of IMP3 expression with the nodal status groups in the second part. Finally, the evaluation methods of IMP3 expression (IMP3 Expression Categories I-III) are compared and correlated with clinical pathological outcome parameters.
3.1. Study Population
The patients’ age range was 42.7–97 years (mean 75.8 years, median 75.7 years, standard deviation 10.1 years). The patients’ subgroups were LSCC + ECSCC (n = 122, 100%, male n = 109, female n = 13). The subgroup data characteristics were: LSCC (n = 58, 47.5%, LSCC unilateral: n = 25; LSCC bilateral: n = 33) and ECSCC (n = 64, 52.5%).
The distribution of the classification of immunosuppression of the patients was as follows: none (n = 102), weak (n = 6), moderate (n = 13), strong (n = 1).
3.2. Clinical Pathology Data in the Study Cohort
Prognostic TNM data were collected: (all pT n = 122, 100%; pT1 n = 27, 22.5%; pT2 n = 31, 25.8%; pT3 n = 47, 37.5%; pT4 n = 17, 14.2%; all pN n = 120, 100%; pN0 n = 76, 63.3%; pN1 n = 26, 21.7%; pN 2a n = 14, 11.7%; pN 2b n = 3, 2.5%; pN 2c n = 1, 0.8%; all M n = 122, 100%; M0 n = 120, 98.4%; M1 n = 2, 1.6%). All patients showed an R0 status.
3.3. IMP3 Expression Distribution in the Study Cohort
As there were only marginal differences between the investigators, a shared decision was not necessary. The mean of IMP3 expression was 51.2%, and the median was 52.4% with a standard deviation of 19.5%. The range of IMP3 expression was between 0.0% and 88.4% IMP3 expression.
3.4. Higher IMP3 Expression Correlates with the Risk for Lymph Node Metastasis
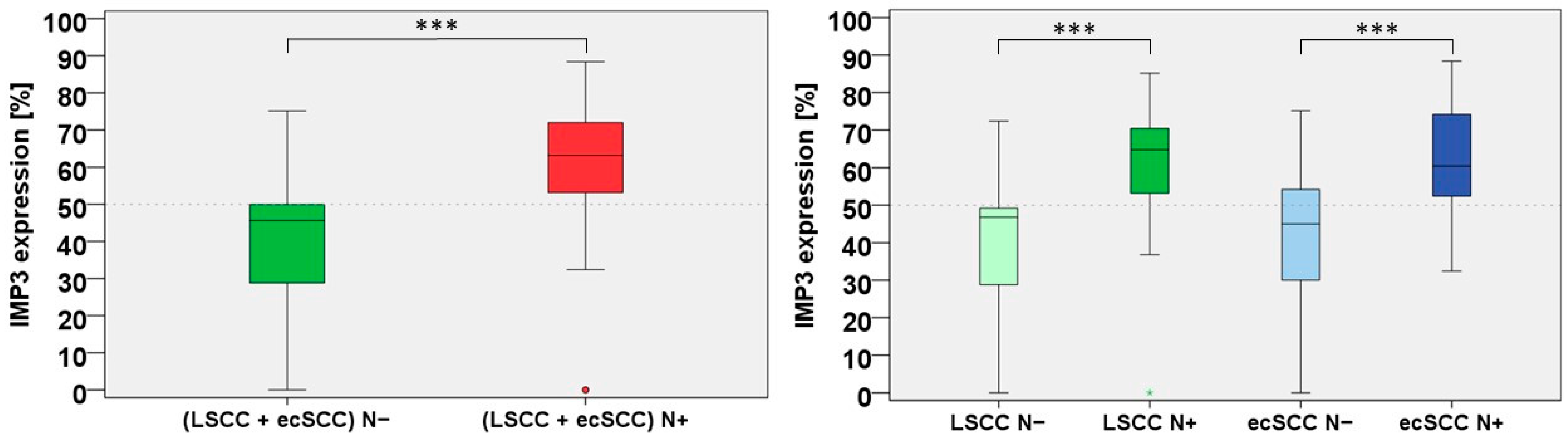
The comparison between the N+ and N− groups showed that IMP3 expression in all cases with N+ had a mean of 61.4%, a median of 63.2%, and a standard deviation of 14.9.
Interestingly, IMP3 expression of all cases with N− showed a mean of 41.1%, a median of 45.6%, and a standard deviation of 18.4. Thus, a higher IMP 3 expression was correlated with pN+ in high-risk localisation of cSCC (
p < 0.001).
Figure 1 (left side) shows the correlation of the nodal status and IMP3 expression in the boxplot.
In addition to the correlation of the total collective (including both LSCC and ECSCC) with N+, the analysis of the subgroups LSCC and ECSCC followed. Interestingly, both subgroups showed a higher expression of IMP3 in the N+ group.
Figure 1 (right side) displays the risk for LNMs and the expression of IMP3 in the subgroups of LSCC N+/N− and ECSCC N+/N− and IMP3 expression.
LSCC N+ patients presented with a mean IMP3 expression of 60.3%, a range of 0.0–85.2%, and a standard deviation of 16.2. For LSCC N−, we found a mean of 40.3%, a range of 0.0–72.4%, and a standard deviation of 17.9. Interestingly, the difference of LSCC N+ vs. LSCC N− was significant in the Mann–Whitney U-test in the subgroup analysis (p < 0.001), proving that higher IMP3 expression is correlated with the risk for LNMs in LSCC. This was also revealed in the analysis of the ECSCC N+ subgroup. These patients presented with a mean IMP3 expression of 62.3%, a median of 60.4%, a range of 32.4–88.4%, and a standard deviation of 13.8, whereas the ECSCC N− subgroup showed a mean of 41.8%, a median of 45.0%, a range of 0.0–75.2%, and a standard deviation of 19.1. The difference of ECSCC N+ v. ECSCC N− was also significant (p < 0.001) in the Mann–Whitney U-test. Taken together, IMP3 could be a reliable marker for metastasis risk assessment as it consistently correlated with the LNM rates.
3.5. IMP3 Correlates with Disease Progression and Local Relapse
In addition to the prediction of N+ cases by the IMP3 expression rates, other prognostically significant outcome parameters were also analysed: A higher IMP3 expression significantly correlated with disease progression (p < 0.001) and local relapse (p = 0.014). However, IMP3 expression did not correlate with disease-specific death (p = 0.090) and distant metastasis (p = 0.090).
3.6. IMP3 Analysis Categories I–III
After proving the prognostic potential of IMP3 expression analysis for pN+, a simple clinically applicable semiquantitative IMP3 expression analysis needed to be established. For this purpose, we analysed the IMP3 expression using three different approaches (Analysis Categories I–III) to identify the most-reliable and -application-oriented method for the prognostic evaluation of IMP3 expression in LSCC and ECSCC. In addition, it should be investigated whether the correlation between increased IMP3 expression and the increased occurrence of LNMs also applies to IMP3 Analysis Categories I–III.
3.7. IMP3 Analysis Category I (<25%, 25–50%, 50–75%, >75% IMP3 Expression)
For the first screening of IMP3 expression ranges, a quarter-step classification (IMP3 Analysis Category I; <25%, 25–50%, 50–75%, >75% IMP3 expression) was performed.
In IMP3 Category I, the age at first diagnosis was as follows: <25% IMP3 expression: mean 76.1 years, median 73.6, 64.7–93.9 years; 25–50% IMP3 expression: mean 76.6 years, median 77.9 years, 42.7–94.8 years; 50–75% IMP3 expression: mean 74.9, median 75.2 years, 44.3–97.0 years; >75% IMP3 expression: mean 76.8 years, median 76.1 years, 65.2–91.7 years. The correlation was not significant in the Pearson chi-squared test (p = 0.346).
A distribution of IMP3 expression for the AJCC was also shown: <25% IMP3 expression: Stage I (n = 5), Stage II (n = 3), Stage III (n = 1), Stage IV (n = 3); 25–50% IMP3 expression: Stage I (n = 10), Stage II (n = 8), Stage III (n = 19), Stage IV (n = 9); 50–75% IMP3 expression: Stage I (n = 7), Stage II (n = 8), Stage III (n = 24), Stage IV (n = 14); >75% IMP3 expression: Stage I (n = 1), Stage II (n = 0), Stage III (n = 7), Stage IV (n = 3). The correlation failed to reach significance in the Pearson chi-squared test (p = 0.179).
In addition, IMP3 Analysis Category I is presented with the degree of differentiation (grading): <25% IMP3 expression: G1 (n = 4), G2 (n = 6), G 3 (n = 2); 25–50% IMP3 expression: G1 (n = 10), G2 (n = 27), G 3 (n = 9); 50–75% IMP3 expression: G1 (n = 11), G2 (n = 32), G 3 (n = 10); >75% IMP3 expression: G1 (n = 1), G2 (n = 8), G 3 (n = 3). The correlation was not significant in the Pearson chi-squared test (p = 0.905).
The distribution of the strength of immunosuppression could also be shown as dependent on the IMP3 expression: <25% IMP3 expression: none (n = 11), weak (n = 1), moderate (n = 0), strong (n = 0); 25–50% IMP3 expression: none (n = 38), weak (n = 4), moderate (n = 4), strong (n = 0); 50–75% IMP3 expression: none (n = 42), weak (n = 1), moderate (n = 9), strong n = 1); >75% IMP3 expression: no patient with immunosuppression. The correlation failed to reach significance in the Pearson chi-squared test (p = 0.381).
There were more cases in the N+ (LSCC N+ and ECSCC N+) group with an IMP3 expression range of 50–75% (63.9%) and an IMP3 expression range >75% (16.4%) as compared to the respective N− groups.
In line with this, the quartiles with lower IMP3 expression ranges showed fewer cases in the N+ (LSCC N+ and ECSCC N+) group (IMP3 expression range <25% (1.6%) and IMP3 expression range of 25–50% (18.0%)).
As expected, there were significantly more cases in the N− (LSCC N− + ECSCC N−) group with an IMP3 expression range <25% (18.0%) or IMP3 expression range of 25–50% (57.4%) and fewer cases for the high expression ranges (IMP3 expression range of 50–75% (23.0%) and IMP3 expression range >75% (1.6%)).
The cross-tabulation showed significance (p < 0.001) for IMP3 Analysis Category I with nodal status in the Pearson chi-squared test.
We then analysed this in further detail by comparing the individual subgroups (LSCC N−, LSCC N+, ECSCC N−, ECSCC N+) and found that, generally, the lower quartiles were more frequent in the N− subgroups, whereas in the N+ subgroups, the higher quartiles were prevalent: LSCC N−: IMP3 expression <25% (17.2%), IMP3 expression of 25–50% (65.5%), IMP3 expression of 50–75% (17.2%), IMP3 expression >75% (0%); LSCC N+: IMP3 expression <25% (3.4%), IMP3 expression of 25–50% (13.8%), IMP3 expression of 50–75% (75.9%), IMP3 expression >75% (6.9%); ECSCC N−: IMP3 expression <25% (18.8%), IMP3 expression of 25–50% (50.0%), IMP3 expression of 50–75% (28.1%), IMP3 expression >75% (3.1%); ECSCC N+: IMP3 expression <25% (0%), IMP3 expression of 25–50% (21.9%), IMP3 expression of 50–75% (53.1%), IMP3 expression >75% (25.0%).
After subgroup analysis, the correlations of IMP3 Analysis Category I with different clinical pathological outcome parameters were examined for all patients.
A significant correlation between IMP3 expression and N+ (p < 0.001) was demonstrated for IMP3 Analysis Category I.
There was no significant correlation (p = 0.370) of IMP3 Analysis Category I and disease-specific death in the Pearson chi-squared test. In contrast, there was a correlation in IMP3 Analysis Category I and disease progression (p < 0.001). In addition, trends could be shown for IMP3 Analysis Category I and distant metastasis (p = 0.093) and IMP3 Analysis Category I and local relapse (p = 0.058).
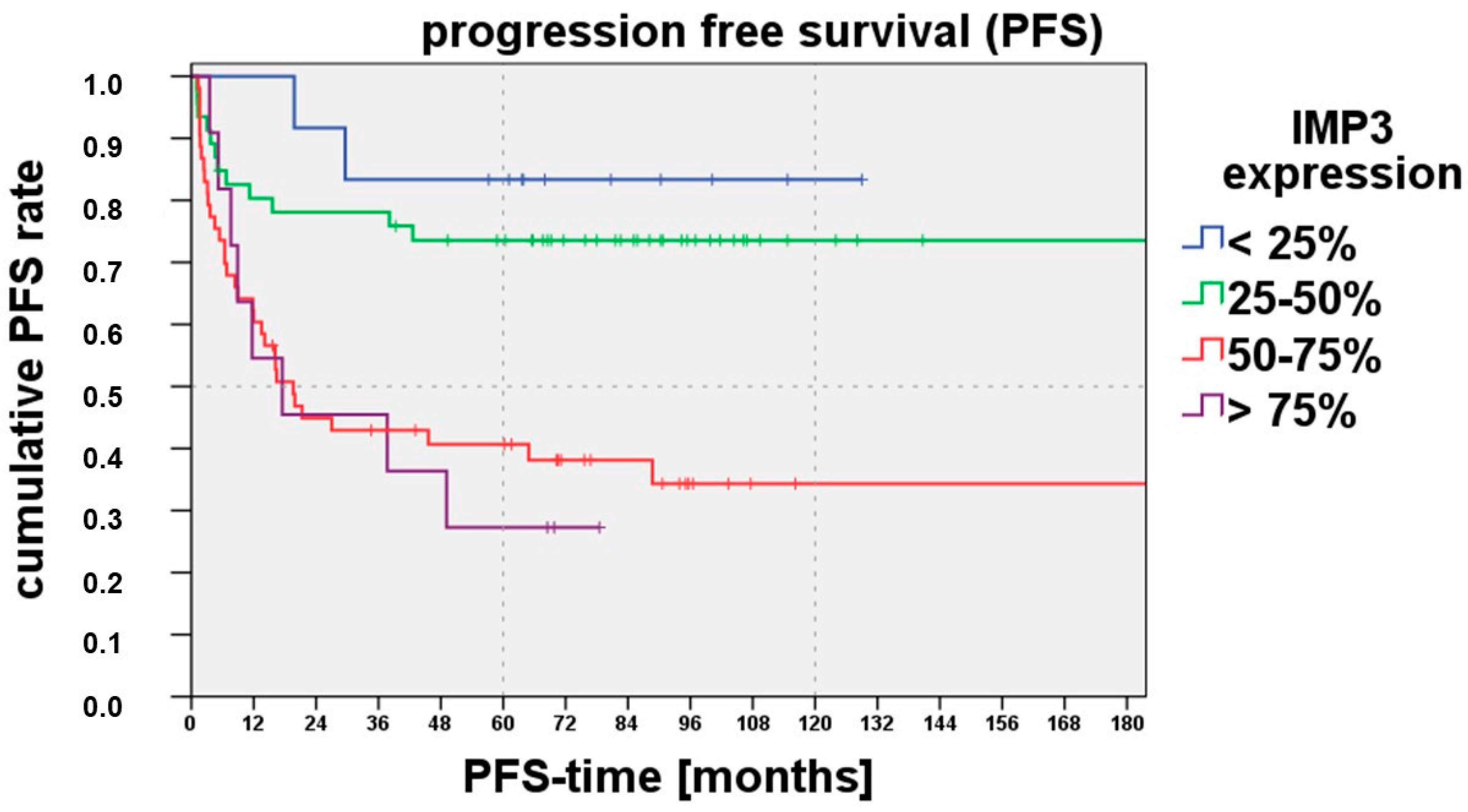
As we saw before that IMP3 expression correlates with disease-free progression, we also performed a Kaplan–Meyer analysis for progression-free survival for IMP3 Analysis Category I:
Figure 2 shows that progression-free survival was reduced for an IMP3 expression range > 50%. The log-rank test (comparison with the <25% IMP3 expression range) showed a significant difference with the 50–75% IMP3 expression range (
p = 0.007) and >75% IMP3 expression range (
p = 0.004). For the 25–50% IMP expression range, no significant difference could be shown.
3.8. IMP3 Analysis Category II (0%, 1–20%, 21–60%, >60% IMP3 Expression)
After the analysis of the IMP3 Analysis Category I (<25%, 25–50%, 50–75%, >75% IMP3 expression), the IMP3 expression was subdivided into thirds (IMP3 Analysis Category II; 0%, 1–20%, 21–60%, >60% IMP3 expression).
In IMP3 Category II, the age at first diagnosis was as follows: 0% IMP3 expression: mean 69.5 years, median 71.6 years, 64.7–72.1 years; 1–20% IMP3 expression: mean 78.8 years, median 77.4 years, 69.5–93.9 years; 21–60% IMP3 expression: mean 75.8 years, median 76.5 years, 42.7–97.0 years; >60% IMP3 expression: mean 75.8 years, median 76.0 years, 44.3–97.0 years. The correlation was not significant in the Pearson chi-squared test (p = 0.223).
In addition, a distribution of IMP3 Analysis Category II could be shown for the AJCC: 0% IMP3 expression: Stage I (n = 2), Stage II (n = 1), Stage III (n = 0), Stage IV (n = 0); 1–20% IMP3 expression: Stage I (n = 2), Stage II (n = 2), Stage III (n = 1), Stage IV (n = 3); 21–60% IMP3 expression: Stage I (n = 13), Stage II (n = 15), Stage III (n = 29), Stage IV (n = 14); >60% IMP3 expression: Stage I (n = 6), Stage II (n = 1), Stage III (n = 21), Stage IV (n = 12). The correlation was significant in the Pearson chi-squared test (p = 0.042).
In addition, the IMP3 Analysis Category I is presented with the degree of differentiation (grading): 0% IMP3 expression: G1 (n = 2), G2 (n = 1), G 3 (n = 0); 1–20% IMP3 expression: G1 (n = 2), G2 (n = 4), G 3 (n = 2); 21–60% IMP3 expression: G1 (n = 16), G2 (n = 42), G 3 (n = 13); >60% IMP3 expression: G1 (n = 6), G2 (n = 26), G 3 (n = 8). The correlation was not significant in the Pearson chi-squared test (p = 0.522).
The distribution of the strength of immunosuppression could also be shown as a dependent on the IMP3 expression: 0% IMP3 expression: no immunosuppression (n = 3); 1–20% IMP3 expression: none (n = 7), weak (n = 1), moderate (n = 0), strong (n = 0); 21–60% IMP3 expression: none (n = 58), weak (n = 4), moderate (n = 8), strong (n = 1); >60% IMP3 expression: none (n = 34), weak (n = 1), moderate (n = 5), strong (n = 0). The correlation failed to reach significance in the Pearson chi-squared test (p = 0.922).
In the N+ group (LSCC N+ + ECSCC N+), most patients (54.1%) were in the >60% IMP3 expression range and 44.3% in the 21–60% IMP3 expression range. In the 0% IMP3 expression range, there were 1.6% of the cases, and in the 1–20% IMP3 expression range, no patients (0%).
The distribution in the N− group (LSCC N− + ECSCC N−) was different. Here, in the IMP3 expression range group 0%, 3.3% of the cases, in the IMP3 expression range 1–20%, 13.1% of the cases, in the IMP3 expression range 21–60%, 72.1% of the cases, and in the IMP3 expression range >60%, 11.5% of the cases fell.
IMP3 expression in the subgroups (LSCC N−, LSCC N+, ECSCC N−, ECSCC N+) was also examined:
LSCC N−: IMP3 expression range of 0%: 3.4%, IMP3 expression range of 1–20%: 10.3%, IMP3 expression range of 21–60%: 79.3%, IMP3 expression range >60%: 6.9%; LSCC N+: IMP3 expression range of 0%: 3.4%, IMP3 expression range of 1–20%: 0%, IMP3 expression range of 21–60%: 37.9%, IMP3 expression range >60%: 58.6%; ECSCC N−: IMP3 expression range of 0%: 3.1%, IMP3 expression range of 1–20%: 15.6%, IMP3 expression range of 21–60%: 65.6%, IMP3 expression range >60%: 15.6%, ECSCC N+: IMP3 expression range of 0%: 0%, IMP3 expression range of 1–20%: 0%, IMP3 expression range of 21–60%: 50.0%, IMP3 expression range >60%: 50.0%.
No correlation was found between IMP3 Analysis Category II and the risk of disease- related death and local relapse.
In contrast, the Pearson chi-squared test showed a positive correlation of IMP3 Analysis Category II with disease progression (p = 0.001), distant metastasis (p = 0.014), and LNM (p = 0.008).
3.9. IMP3 Analysis Category III (<50%, >50% IMP3 Expression)
A quick and clinically easy way to implement IMP3 analysis is the classification into the >50% and <50% IMP3 expression ranges (IMP3 Analysis Category III).
In IMP3 Category III, the age at first diagnosis was as follows: >50% IMP3 expression: mean 75.3 years, median 75.7 years, 44.3–97.0 years; <50% IMP3 expression: mean 76.5 years, median 76.1 years, 42.7–94.8 years. The correlation was not significant in the Pearson chi-squared test (p = 0.397).
A distribution of IMP3 expression for the AJCC was also shown: >50% IMP3 expression: Stage I (n = 8), Stage II (n = 9), Stage III (n = 33), Stage IV (n = 18); <50% IMP3 expression: Stage I (n = 15), Stage II (n = 10), Stage III (n = 18), Stage IV (n = 11). The correlation failed to reach significance in the Pearson chi-squared test (p = 0.80).
In addition, the IMP3 Analysis Category I is presented with the degree of differentiation (grading): >50% IMP3 expression: G1 (n = 12) G2 (n = 43) G 3 (n = 13); <50% IMP3 expression: G1 (n = 14) G2 (n = 30) G 3 (n = 10). The correlation was not significant in the Pearson chi-squared test (p = 0.530).
The distribution of the strength of immunosuppression could also be shown as dependent on the IMP3 expression: >50% IMP3 expression: none (n = 57), weak (n = 1) moderate (n = 9) strong (n = 1); <50% IMP3 expression: none (n = 45), weak (n = 5) moderate (n = 4) strong (n = 0). The correlation failed to reach significance in the Pearson chi-squared test (p = 0.141).
The >50% IMP3 expression range was positively correlated with the presence of LNMs at all sites (LSCC N+ + ECSCC N+): 83.6% of these cases showed an LNM and 27.9% no LNM. In contrast, 72.1% of patients in the <50% IMP 3 expression range group did not have an LNM (LSCC N− + ECSCC N−), and 16.4% had an LNM. Thus, a higher IMP3 expression of >50% was significantly (p < 0.001) correlated with the occurrence of an LNM.
We next analysed the localisation subgroups and also found significant correlations with IMP3 Expression Category III. In the LSCC group and IMP3 expression >50%, 82.8% of patients had an LNM and only 24.1% had no LNM. In the LSCC group and IMP3 expression <50%, 75.9% of patient cases showed no LNM and only 17.2% had LNM.
Comparable results were also found in the ECSCC group. In the ECSCC group and an IMP3 expression of >50%, 84.4% of patients had an LNM and 31.3% had no LNM. In line with this, in the ESCC group and an IMP3 expression of <50%, 68.8% of the patients had no LNM and 15.6% had an LNM. IMP3 Expression Category III (<50%, >50% IMP3 expression) was significantly correlated (p < 0.001) with the risk for LNMs in the subgroups.
Although we were able to show the significant correlation of >50% IMP3 expression and LNMs, we could unfortunately not demonstrate a significant correlation for IMP3 expression and distant metastasis in this category. Furthermore, there was a correlation between IMP3 Analysis Category III and disease progression (p < 0.001).
In addition, it was investigated whether IMP3 Analysis Category III correlated with the risk of local recurrence. There was a correlation (p = 0.012) for IMP3 Analysis Category III and local recurrence in the Pearson chi-squared test.
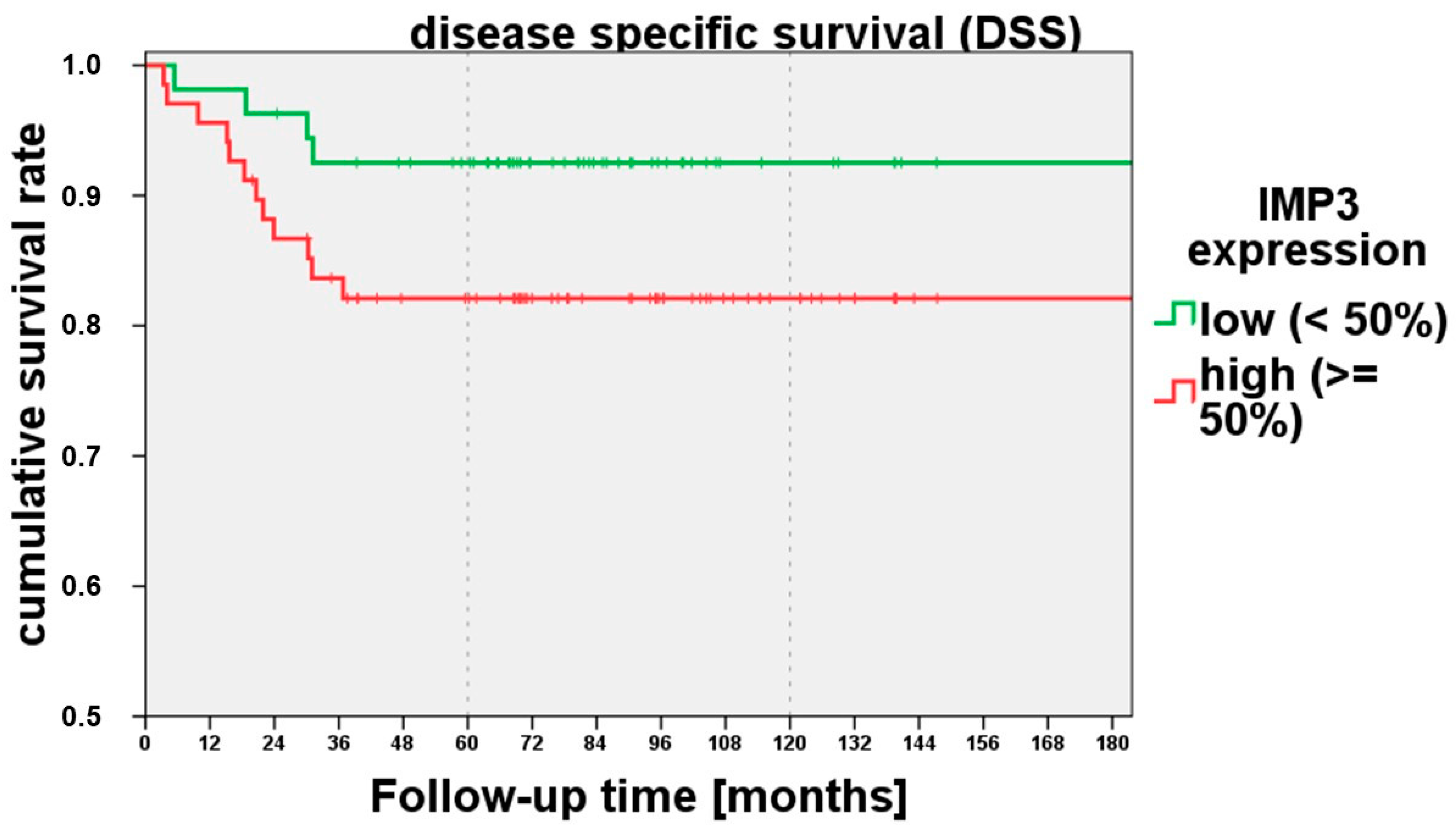
To examine whether the 50% expression cutoff was also able to predict the disease-specific survival, we analysed IMP3 Expression Category III with disease-related death. Higher IMP3 expression showed a tendency (
p = 0.092) towards disease-related death in the IMP3 expression category in the log rank test (Mantel–Cox). A higher IMP3 expression of >50% showed a lower disease-specific survival (
Figure 3).
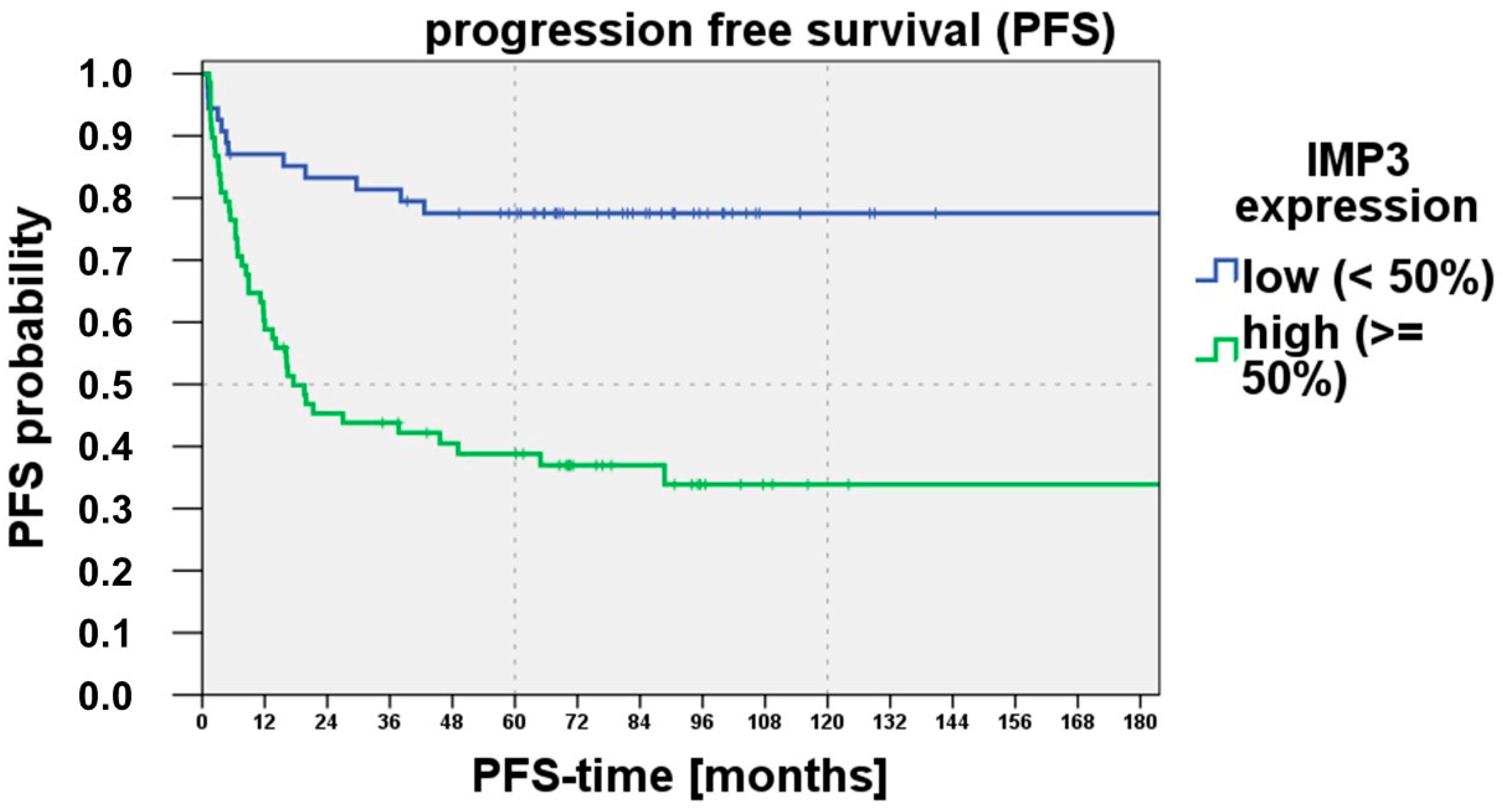
Another important clinical outcome parameter is progression-free survival. A higher IMP3 expression >50% was correlated also with a shorter progression-free survival. The log rank test (Mantel–Cox) showed significant differences (
p < 0.001).
Figure 4 demonstrates the Kaplan–Meier curve for progression-free survival and IMP3 expression (IMP3 Analysis Category III (<50%, >50%)).
3.10. Concluding Remarks on the Results
The tumour marker IMP3 seems to be suitable for outcome prediction in LSCC and ECSCC. We observed a significant risk prediction potential for LNMs and, in particular, with IMP3 Analysis Category III (<50%, >50%). The evaluation was fast, efficient, and simple.


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}



