
MRI Characteristics of Pediatric and Young-Adult Renal Cell Carcinoma: A Single-Center Retrospective Study and Literature Review
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
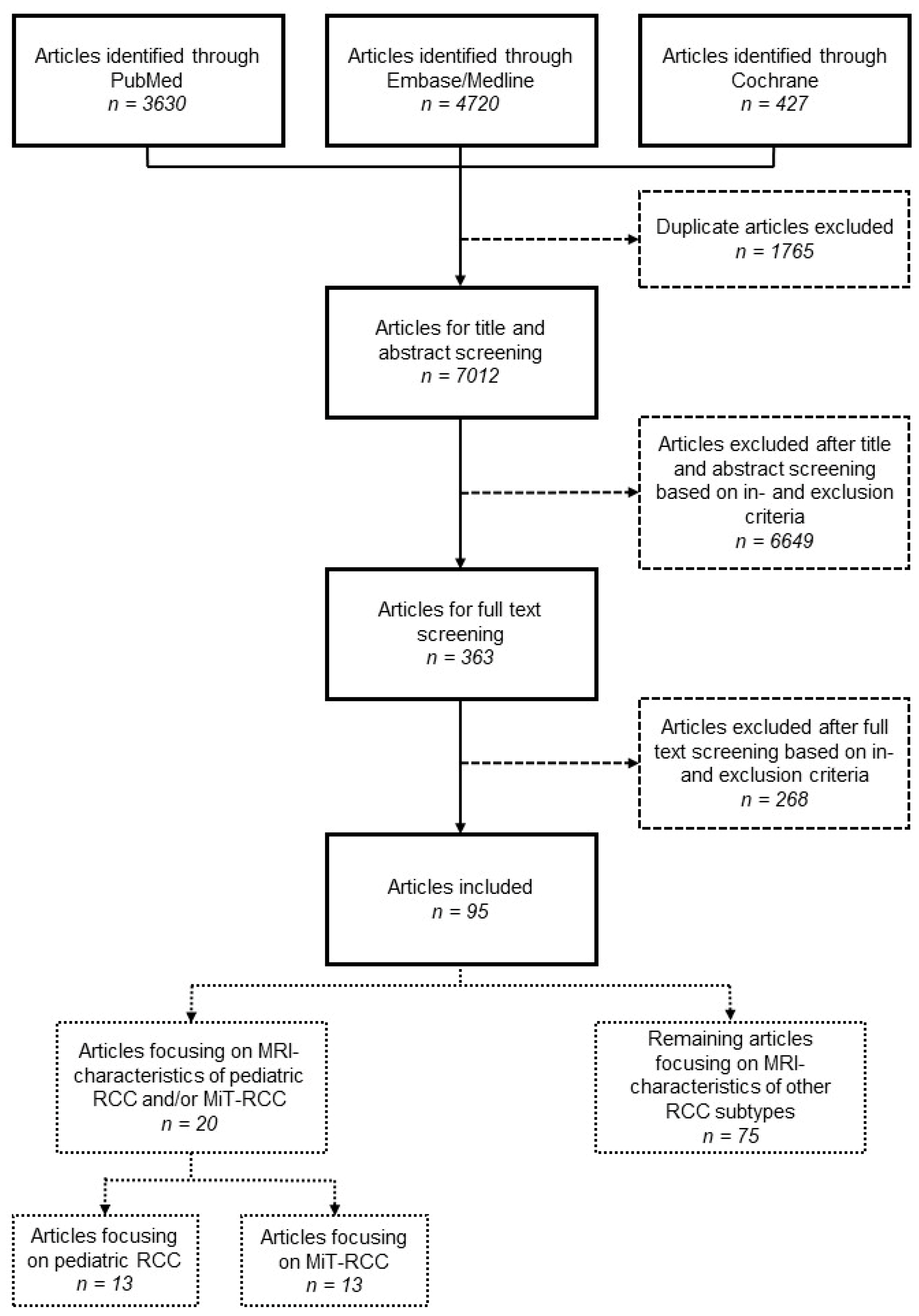
2. Materials and Methods
2.1. Patients
2.2. Magnetic Resonance Imaging Acquisition
2.3. Image Analysis
2.4. Histopathological Review
2.5. Statistical Analyses
2.6. Literature Review
3. Results
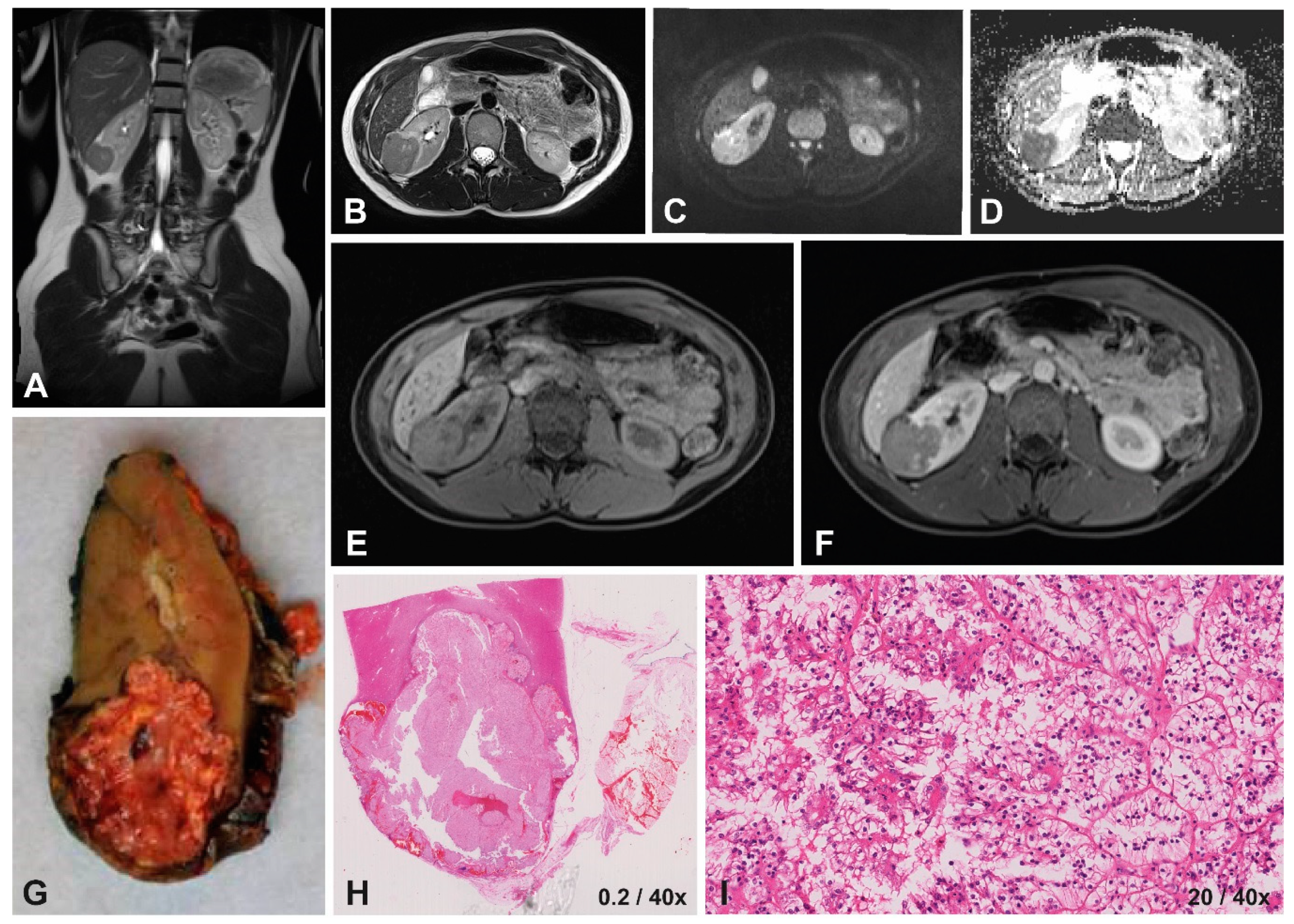
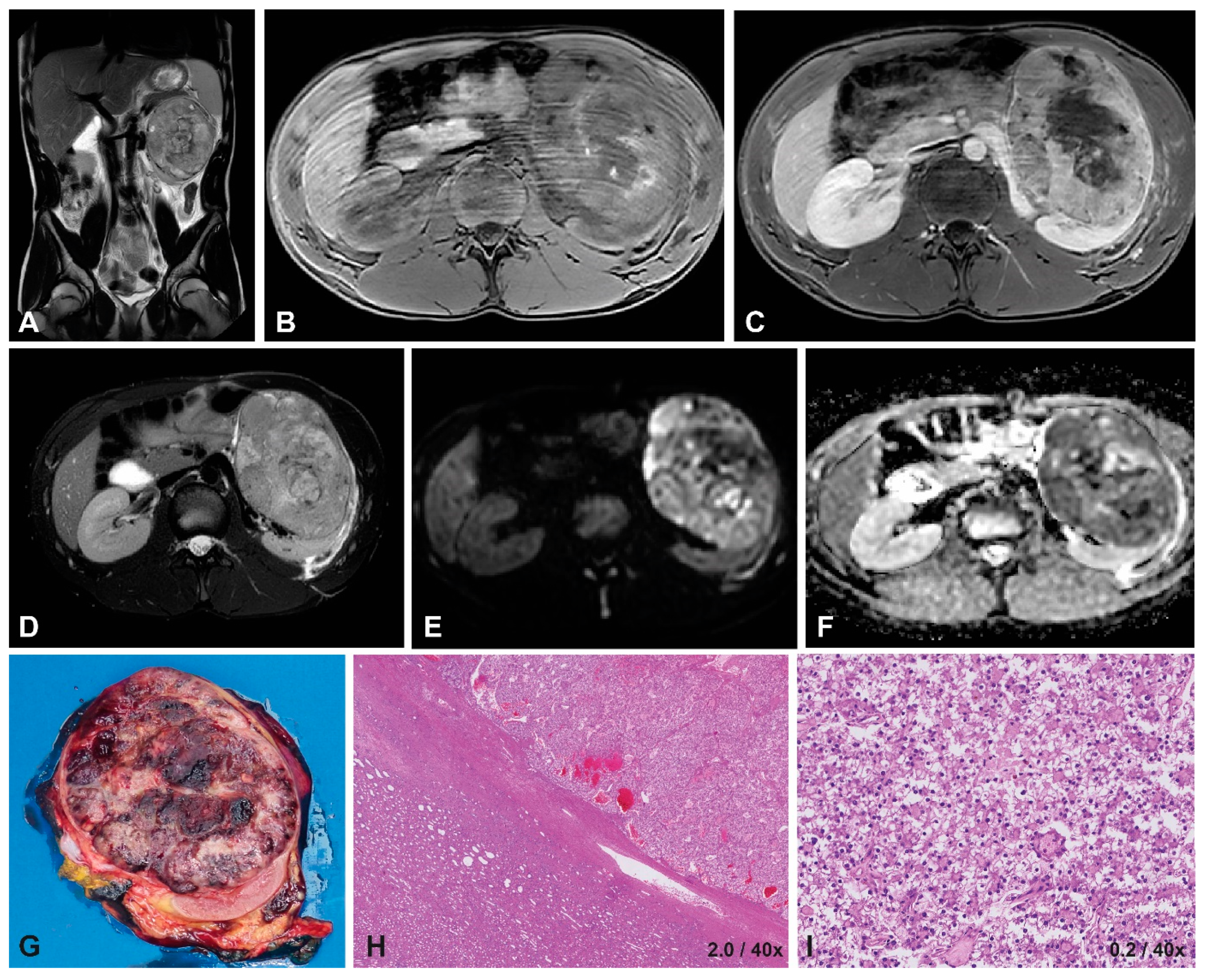
3.1. Case Presentation
3.1.1. Patient Characteristics
3.1.2. Histopathology
3.1.3. Imaging Characteristics at Diagnosis
3.1.4. Diffusion-Weighted Imaging
3.2. Literature Review
3.2.1. Pediatric and Young-Adult RCC
3.2.2. MiT-RCC
3.2.3. Other Subtypes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nakata, K.; Colombet, M.; Stiller, C.A.; Pritchard-Jones, K.; Steliarova-Foucher, E. Incidence of childhood renal tumours: An international population-based study. Int. J. Cancer 2020, 147, 3313–3327. [Google Scholar] [CrossRef] [PubMed]
- van der Beek, J.N.; Geller, J.I.; de Krijger, R.R.; Graf, N.; Pritchard-Jones, K.; Drost, J.; Verschuur, A.C.; Murphy, D.; Ray, S.; Spreafico, F.; et al. Characteristics and Outcome of Children with Renal Cell Carcinoma: A Narrative Review. Cancers 2020, 12, 1776. [Google Scholar] [CrossRef]
- van der Beek, J.N.; Hol, J.A.; Coulomb-l’Hermine, A.; Graf, N.; van Tinteren, H.; Pritchard-Jones, K.; Houwing, M.E.; de Krijger, R.R.; Vujanic, G.M.; Dzhuma, K.; et al. Characteristics and outcome of pediatric renal cell carcinoma patients registered in the International Society of Pediatric Oncology (SIOP) 93-01, 2001 and UK-IMPORT database: A report of the SIOP-Renal Tumor Study Group. Int. J. Cancer 2021, 148, 2724–2735. [Google Scholar] [CrossRef] [PubMed]
- Roy, P.; van Peer, S.E.; de Witte, M.M.; Tytgat, G.A.M.; Karim-Kos, H.E.; van Grotel, M.; van de Ven, C.P.; Mavinkurve-Groothuis, A.M.C.; Merks, J.H.M.; Kuiper, R.P.; et al. Characteristics and outcome of children with renal tumors in the Netherlands: The first five-year’s experience of national centralization. PLoS ONE 2022, 17, e0261729. [Google Scholar] [CrossRef] [PubMed]
- Ray, S.; Jones, R.; Pritchard-Jones, K.; Dzhuma, K.; van den Heuvel-Eibrink, M.; Tytgat, G.; van der Beek, J.; Oades, G.; Murphy, D. Pediatric and young adult renal cell carcinoma. Pediatr. Blood Cancer 2020, 67, e28675. [Google Scholar] [CrossRef]
- Watson, T.; Oostveen, M.; Rogers, H.; Pritchard-Jones, K.; Olsen, Ø. The role of imaging in the initial investigation of paediatric renal tumours. Lancet Child Adolesc. Health 2020, 4, 232–241. [Google Scholar] [CrossRef]
- de la Monneraye, Y.; Michon, J.; Pacquement, H.; Aerts, I.; Orbach, D.; Doz, F.; Bourdeaut, F.; Sarnacki, S.; Philippe-Chomette, P.; Audry, G.; et al. Indications and results of diagnostic biopsy in pediatric renal tumors: A retrospective analysis of 317 patients with critical review of SIOP guidelines. Pediatr. Blood Cancer 2019, 66, e27641. [Google Scholar] [CrossRef]
- Grover, S.B.; Antil, N.; Rajani, H.; Grover, H.; Kumar, R.; Mandal, A.K.; Bagga, D.; Katyan, A. Approach to pediatric renal tumors: An imaging review. Abdom. Radiol. 2019, 44, 619–641. [Google Scholar] [CrossRef]
- van der Beek, J.N.; Watson, T.A.; Nievelstein, R.A.J.; Brisse, H.J.; Morosi, C.; Lederman, H.M.; Coma, A.; Gavra, M.M.; Vult von Steyern, K.; Lakatos, K.; et al. MRI Characteristics of Pediatric Renal Tumors: A SIOP-RTSG Radiology Panel Delphi Study. J. Magn. Reson. Imaging 2021, 55, 543–552. [Google Scholar] [CrossRef]
- Jackson, T.J.; Brisse, H.J.; Pritchard-Jones, K.; Nakata, K.; Morosi, C.; Oue, T.; Irtan, S.; Vujanic, G.; van den Heuvel-Eibrink, M.M.; Graf, N.; et al. How we approach paediatric renal tumour core needle biopsy in the setting of preoperative chemotherapy: A Review from the SIOP Renal Tumour Study Group. Pediatr. Blood Cancer 2022, 69, e29702. [Google Scholar] [CrossRef]
- Littooij, A.S.; Nikkels, P.G.; Hulsbergen-van de Kaa, C.A.; van de Ven, C.P.; van den Heuvel-Eibrink, M.M.; Olsen, Ø.E. Apparent diffusion coefficient as it relates to histopathology findings in post-chemotherapy nephroblastoma: A feasibility study. Pediatr. Radiol. 2017, 47, 1608–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hales, P.W.; Olsen, Ø.E.; Sebire, N.J.; Pritchard-Jones, K.; Clark, C.A. A multi-Gaussian model for apparent diffusion coefficient histogram analysis of Wilms’ tumour subtype and response to chemotherapy. NMR Biomed 2015, 28, 948–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razek, A.A.; Farouk, A.; Mousa, A.; Nabil, N. Role of diffusion-weighted magnetic resonance imaging in characterization of renal tumors. J. Comput. Assist. Tomogr. 2011, 35, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Pan, J.; Shen, Y.; Bai, X.; Wang, Y.; Wang, H.; Ye, H. High signal renal tumors on DWI: The diagnostic value of morphological characteristics. Abdom. Radiol. 2019, 44, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Hötker, A.M.; Lollert, A.; Mazaheri, Y.; Müller, S.; Schenk, J.P.; Mildenberger, P.C.; Akin, O.; Graf, N.; Staatz, G. Diffusion-weighted MRI in the assessment of nephroblastoma: Results of a multi-center trial. Abdom. Radiol. 2020, 45, 3202–3212. [Google Scholar] [CrossRef]
- Littooij, A.S.; Sebire, N.J.; Olsen Ø, E. Whole-tumor apparent diffusion coefficient measurements in nephroblastoma: Can it identify blastemal predominance? J. Magn. Reson. Imaging 2017, 45, 1316–1324. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Kwon, Y.S.; Labib, M.; Foran, D.J.; Singer, E.A. Magnetic Resonance Imaging as a Biomarker for Renal Cell Carcinoma. Dis. Mrk. 2015, 2015, 648495. [Google Scholar] [CrossRef] [Green Version]
- Geller, J.I.; Cost, N.G.; Chi, Y.Y.; Perlman, E.J.; Kim, Y.; Cajaiba, M.; Mullen, E.A.; Glick, R.D.; Khanna, G.; Daw, N.C.; et al. A prospective study of pediatric renal cell carcinoma: A report from the Children’s Oncology Group study AREN0321. J. Clin. Oncol. 2018, 36, 10516. [Google Scholar] [CrossRef]
- Wang, W.; Ding, J.; Li, Y.; Wang, C.; Zhou, L.; Zhu, H.; Peng, W. Magnetic resonance imaging and computed tomography characteristics of renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusion. PLoS ONE 2014, 9, e99990. [Google Scholar] [CrossRef]
- Murphy, G.; Jhaveri, K. The expanding role of imaging in the management of renal cell carcinoma. Expert. Rev. Anticancer. Ther. 2011, 11, 1871–1888. [Google Scholar] [CrossRef]
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Gore, J.L.; Sun, M.; Wood, C.; Russo, P. Epidemiology of Renal Cell Carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Geller, J.I.; Ehrlich, P.F.; Cost, N.G.; Khanna, G.; Mullen, E.A.; Gratias, E.J.; Naranjo, A.; Dome, J.S.; Perlman, E.J. Characterization of adolescent and pediatric renal cell carcinoma: A report from the Children’s Oncology Group study AREN03B2. Cancer 2015, 121, 2457–2464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selle, B.; Furtwangler, R.; Graf, N.; Kaatsch, P.; Bruder, E.; Leuschner, I. Population-based study of renal cell carcinoma in children in Germany, 1980–2005: More frequently localized tumors and underlying disorders compared with adult counterparts. Cancer 2006, 107, 2906–2914. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Xie, P.; Peng, W.; Zhou, Z. Renal carcinomas associated with Xp11.2 translocations/TFE3 gene fusions: Findings on MRI and computed tomography imaging. J. Magn. Reson. Imaging 2014, 40, 440–447. [Google Scholar] [CrossRef]
- He, M.; Cai, J.; Zhu, K.; Gu, W.; Li, M.; Xiong, J.; Guan, Z.; Wang, J.; Shu, Q. Renal cell carcinoma in children and adolescents: Single-center experience and literature review. Medicine 2021, 100, e23717. [Google Scholar] [CrossRef]
- Cajaiba, M.M.; Dyer, L.M.; Geller, J.I.; Jennings, L.J.; George, D.; Kirschmann, D.; Rohan, S.M.; Cost, N.G.; Khanna, G.; Mullen, E.A.; et al. The classification of pediatric and young adult renal cell carcinomas registered on the children’s oncology group (COG) protocol AREN03B2 after focused genetic testing. Cancer 2018, 124, 3381–3389. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Beltran, A.; Scarpelli, M.; Montironi, R.; Kirkali, Z. 2004 WHO classification of the renal tumors of the adults. Eur. Urol. 2006, 49, 798–805. [Google Scholar] [CrossRef]
- Chung, E.M.; Lattin, G.E., Jr.; Fagen, K.E.; Kim, A.M.; Pavio, M.A.; Fehringer, A.J.; Conran, R.M. Renal Tumors of Childhood: Radiologic-Pathologic Correlation Part 2. The 2nd Decade: From the Radiologic Pathology Archives. Radiographics 2017, 37, 1538–1558. [Google Scholar] [CrossRef] [Green Version]
- Couvidat, C.; Eiss, D.; Verkarre, V.; Merran, S.; Correas, J.M.; Mejean, A.; Helenon, O. Renal papillary carcinoma: CT and MRI features. Diagn. Interv. Imaging 2014, 95, 1055–1063. [Google Scholar] [CrossRef] [Green Version]
- Schieda, N.; Lim, R.S.; McInnes, M.D.F.; Thomassin, I.; Renard-Penna, R.; Tavolaro, S.; Cornelis, F.H. Characterization of small (<4 cm) solid renal masses by computed tomography and magnetic resonance imaging: Current evidence and further development. Diagn. Interv. Imaging 2018, 99, 443–455. [Google Scholar] [CrossRef]
- Lopes Vendrami, C.; Parada Villavicencio, C.; DeJulio, T.J.; Chatterjee, A.; Casalino, D.D.; Horowitz, J.M.; Oberlin, D.T.; Yang, G.Y.; Nikolaidis, P.; Miller, F.H. Differentiation of Solid Renal Tumors with Multiparametric MR Imaging. Radiographics 2017, 37, 2026–2042. [Google Scholar] [CrossRef] [PubMed]
- Gurel, S.; Narra, V.; Elsayes, K.M.; Siegel, C.L.; Chen, Z.E.; Brown, J.J. Subtypes of renal cell carcinoma: MRI and pathological features. Diagn. Interv. Radiol. 2013, 19, 304–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muglia, V.F.; Prando, A. Renal cell carcinoma: Histological classification and correlation with imaging findings. Radiol. Bras. 2015, 48, 166–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Sung, D.J.; Sim, K.C.; Han, N.Y.; Park, B.J.; Kim, M.J.; Cho, S.B. Renal tumors with low signal intensities on T2-weighted MR image: Radiologic-pathologic correlation. Abdom. Radiol. 2017, 42, 2108–2118. [Google Scholar] [CrossRef]
- Laguna, B.; Westphalen, A.C.; Guimarães, C.T.; Whang, Z.; Simko, J.; Zagoria, R. Uncommon malignant renal tumors and atypical presentation of common ones: A guide for radiologists. Abdom. Radiol. 2019, 44, 1430–1452. [Google Scholar] [CrossRef]
- Spreafico, F.; Collini, P.; Terenziani, M.; Marchiano, A.; Piva, L. Renal cell carcinoma in children and adolescents. Expert. Rev. Anticancer Ther. 2010, 10, 1967–1978. [Google Scholar] [CrossRef]
- Vujanic, G.M.; Gessler, M.; Ooms, A.; Collini, P.; Coulomb-l’Hermine, A.; D’Hooghe, E.; de Krijger, R.R.; Perotti, D.; Pritchard-Jones, K.; Vokuhl, C.; et al. The UMBRELLA SIOP-RTSG 2016 Wilms tumour pathology and molecular biology protocol. Nat. Rev. Urol. 2018, 15, 693–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feinstein, A.R.; Cicchetti, D.V. High agreement but low kappa: I. The problems of two paradoxes. J. Clin. Epidemiol. 1990, 43, 543–549. [Google Scholar] [CrossRef]
- de Vet, H.C.; Mokkink, L.B.; Terwee, C.B.; Hoekstra, O.S.; Knol, D.L. Clinicians are right not to like Cohen’s κ. BMJ 2013, 346, f2125. [Google Scholar] [CrossRef] [Green Version]
- Hallgren, K.A. Computing Inter-Rater Reliability for Observational Data: An Overview and Tutorial. Tutor Quant. Methods Psychol. 2012, 8, 23–34. [Google Scholar] [CrossRef] [Green Version]
- Hol, J.A.; Jongmans, M.C.J.; Littooij, A.S.; de Krijger, R.R.; Kuiper, R.P.; van Harssel, J.J.T.; Mensenkamp, A.; Simons, M.; Tytgat, G.A.M.; van den Heuvel-Eibrink, M.M.; et al. Renal cell carcinoma in young FH mutation carriers: Case series and review of the literature. Fam. Cancer 2020, 19, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noreña-Rengifo, B.D.; Ochoa-Gaviria, J.; Vélez-Escobar, A.; Muñoz, J.P.; Riveros-Ángel, M. Renal Medullary Carcinoma in an Adolescent With Unknown Sickle Cell Trait. Cureus 2021, 13, e14473. [Google Scholar] [CrossRef] [PubMed]
- Koetter, P.; Martin, K. Management of renal cell carcinoma presenting during teenage pregnancy. J. Pediatr. Surg. Case Rep. 2020, 63, 101664. [Google Scholar] [CrossRef]
- Schaefer, B.A.; Johnson, T.S.; Hooper, D.K.; Nathan, J.D.; Geller, J.I. TFE3-positive renal cell carcinoma occurring in three children with dysfunctional kidneys on immunosuppression. Pediatr. Transpl. 2017, 21, e12912. [Google Scholar] [CrossRef] [PubMed]
- Okabe, K.; Kitamura, H.; Nishiyama, N.; Masumori, N. A case of chromophobe renal cell carcinoma in a 12-year-old girl. Int. Cancer Conf. J. 2016, 5, 36–39. [Google Scholar] [CrossRef]
- Zou, Y.; Xu, J.; Zhang, M. Long-term follow-up and clinical course of a rare case of von Hippel-Lindau disease: A case report and review of the literature. Oncol. Lett. 2016, 11, 3273–3278. [Google Scholar] [CrossRef] [Green Version]
- Koo, H.J.; Choi, H.J.; Kim, M.H.; Cho, K.S. Radiologic-pathologic correlation of renal cell carcinoma associated with Xp11.2 translocation. Acta. Radiol. 2013, 54, 827–834. [Google Scholar] [CrossRef]
- Dang, T.T.; Ziv, E.; Weinstein, S.; Meng, M.V.; Wang, Z.; Coakley, F.V. Computed tomography and magnetic resonance imaging of adult renal cell carcinoma associated with Xp11.2 translocation. J. Comput. Assist. Tomogr. 2012, 36, 669–674. [Google Scholar] [CrossRef]
- Downey, R.T.; Dillman, J.R.; Ladino-Torres, M.F.; McHugh, J.B.; Ehrlich, P.F.; Strouse, P.J. CT and MRI appearances and radiologic staging of pediatric renal cell carcinoma. Pediatr. Radiol. 2012, 42, 410–417, quiz 513–414. [Google Scholar] [CrossRef]
- Kato, H.; Kanematsu, M.; Yokoi, S.; Miwa, K.; Horie, K.; Deguchi, T.; Hirose, Y. Renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusion: Radiological findings mimicking papillary subtype. J. Magn. Reson. Imaging 2011, 33, 217–220. [Google Scholar] [CrossRef]
- Blitman, N.M.; Berkenblit, R.G.; Rozenblit, A.M.; Levin, T.L. Renal medullary carcinoma: CT and MRI features. AJR Am. J. Roentgenol. 2005, 185, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Adachi, T.; Nakatani, T.; Minami, H.; Ikemoto, S.; Esaki, K.; Morimoto, H.; Takase, T. Renal cell carcinoma with hemorrhagic cyst formation in a 4-year-old boy. Int. J. Urol. 2003, 10, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.J., Jr.; Mostofi, F.K.; Sesterhenn, I.A. Renal medullary carcinoma. The seventh sickle cell nephropathy. Am. J. Surg. Pathol. 1995, 19, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tohi, Y.; Harada, S.; Kuroda, N.; Tanaka, K.; Inoue, K.; Kadota, K.; Haba, R.; Nishiyama, Y.; Ueda, N.; Sugimoto, M. 6p.21 translocation renal cell carcinoma in the elderly: Radiological findings mimicking fat poor angiomyolipoma or papillary renal cell carcinoma. Int. Cancer Conf. J. 2021, 10, 233–238. [Google Scholar] [CrossRef]
- Dai, C.; Sheng, R.; Ding, Y.; Yang, M.; Hou, J.; Zhou, J. Magnetic resonance imaging findings of renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusion in adults: A pilot study. Abdom. Radiol. 2019, 44, 209–217. [Google Scholar] [CrossRef]
- Gong, P.; Zhuang, Q.; Wang, K.; Xu, R.; Chen, Y.; Wang, X.; Yin, S. Adult-onset renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusion: 3 case reports and review of literature. Medicine 2018, 97, e11023. [Google Scholar] [CrossRef]
- Chen, X.; Zhu, Q.; Li, B.; Cui, W.; Zhou, H.; Duan, N.; Liu, Y.; Kundra, V.; Wang, Z. Renal cell carcinoma associated with Xp11.2 translocation/TFE gene fusion: Imaging findings in 21 patients. Eur. Radiol. 2017, 27, 543–552. [Google Scholar] [CrossRef]
- Yu, L.; Li, J.; Xu, S.; Navia Miranda, M.; Wang, G.; Duan, Y. An Xp11.2 translocation renal cell carcinoma with SMARCB1 (INI1) inactivation in adult end-stage renal disease: A case report. Diagn. Pathol. 2016, 11, 98. [Google Scholar] [CrossRef] [Green Version]
- D’Antonio, A.; Addesso, M.; Nappi, O.; Zeppa, P. Unsuspected Xp11 Translocation Renal Neoplasm Associated with Contralateral Clear Cell Carcinoma. Int. J. Surg. Pathol. 2016, 24, 248–252. [Google Scholar] [CrossRef]
- Wang, X.; Kong, W.; Wang, Y.; Wang, Y.; Chen, Y.; Shi, Z.; Liu, Y. Analysis of CT, MRI imaging features of renal cell carcinoma with different histopathological types. J. Buon 2021, 26, 2053–2058. [Google Scholar]
- Paschall, A.K.; Nikpanah, M.; Farhadi, F.; Jones, E.C.; Wakim, P.G.; Dwyer, A.J.; Gautam, R.; Merino, M.J.; Srinivasan, R.; Linehan, W.M.; et al. Hereditary leiomyomatosis and renal cell carcinoma (HLRCC) syndrome: Spectrum of imaging findings. Clin. Imaging 2020, 68, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Oliva, M.R.; Glickman, J.N.; Zou, K.H.; Teo, S.Y.; Mortelé, K.J.; Rocha, M.S.; Silverman, S.G. Renal cell carcinoma: t1 and t2 signal intensity characteristics of papillary and clear cell types correlated with pathology. AJR Am. J. Roentgenol. 2009, 192, 1524–1530. [Google Scholar] [CrossRef] [PubMed]
- Hotker, A.M.; Mazaheri, Y.; Wibmer, A.; Karlo, C.A.; Zheng, J.; Moskowitz, C.S.; Tickoo, S.K.; Russo, P.; Hricak, H.; Akin, O. Differentiation of clear cell renal cell carcinoma from other renal cortical tumors by use of a quantitative multiparametric MRI approach. Am. J. Roentgenol. 2017, 208, W85–W91. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Cheng, L.; Zhang, X.; Wang, D.; Guo, A.; Gao, Y.; Ye, H. Renal cell carcinoma: Diffusion-weighted MR imaging for subtype differentiation at 3.0 T. Radiology 2010, 257, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Roy, C.; El Ghali, S.; Buy, X.; Lindner, V.; Gangi, A. Papillary renal cell carcinoma in allograft kidney. Eur. Radiol. 2005, 15, 661–665. [Google Scholar] [CrossRef]
- de Silva, S.; Lockhart, K.R.; Aslan, P.; Nash, P.; Hutton, A.; Malouf, D.; Lee, D.; Cozzi, P.; MacLean, F.; Thompson, J. The diagnostic utility of diffusion weighted MRI imaging and ADC ratio to distinguish benign from malignant renal masses: Sorting the kittens from the tigers. BMC Urol. 2021, 21, 67. [Google Scholar] [CrossRef]
- Paschall, A.K.; Mirmomen, S.M.; Symons, R.; Pourmorteza, A.; Gautam, R.; Sahai, A.; Dwyer, A.J.; Merino, M.J.; Metwalli, A.R.; Linehan, W.M.; et al. Differentiating papillary type I RCC from clear cell RCC and oncocytoma: Application of whole-lesion volumetric ADC measurement. Abdom. Radiol. 2018, 43, 2424–2430. [Google Scholar] [CrossRef]
- van der Beek, J.N.; Artunduaga, M.; Schenk, J.P.; Eklund, M.J.; Smith, E.A.; Lederman, H.M.; Warwick, A.B.; Littooij, A.S.; Khanna, G. Similarities and controversies in imaging of pediatric renal tumors: A SIOP-RTSG and COG collaboration. Pediatr. Blood Cancer 2022, e30080. [Google Scholar] [CrossRef]
- Chung, E.M.; Graeber, A.R.; Conran, R.M. Renal Tumors of Childhood: Radiologic-Pathologic Correlation Part 1. The 1st Decade: From the Radiologic Pathology Archives. Radiographics 2016, 36, 499–522. [Google Scholar] [CrossRef] [Green Version]
- Geller, E.; Kochan, P.S. Renal neoplasms of childhood. Radiol. Clin. N. Am. 2011, 49, 689–709. [Google Scholar] [CrossRef]
- Lonergan, G.J.; Martínez-León, M.I.; Agrons, G.A.; Montemarano, H.; Suarez, E.S. Nephrogenic rests, nephroblastomatosis, and associated lesions of the kidney. Radiographics 1998, 18, 947–968. [Google Scholar] [CrossRef]
- Stanescu, A.L.; Acharya, P.T.; Lee, E.Y.; Phillips, G.S. Pediatric Renal Neoplasms:: MR Imaging-Based Practical Diagnostic Approach. Magn. Reson. Imaging Clin. N. Am. 2019, 27, 279–290. [Google Scholar] [CrossRef]
- Hartman, D.S.; Davis, C.J., Jr.; Madewell, J.E.; Friedman, A.C. Primary malignant renal tumors in the second decade of life: Wilms tumor versus renal cell carcinoma. J. Urol. 1982, 127, 888–891. [Google Scholar] [CrossRef]
- Lowe, L.H.; Isuani, B.H.; Heller, R.M.; Stein, S.M.; Johnson, J.E.; Navarro, O.M.; Hernanz-Schulman, M. Pediatric renal masses: Wilms tumor and beyond. Radiographics 2000, 20, 1585–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swinson, S.; McHugh, K. Urogenital tumours in childhood. Cancer Imaging 2011, 11, S48–S64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riccabona, M. Imaging of renal tumours in infancy and childhood. Eur. Radiol. 2003, 13 (Suppl. 4), L116–L129. [Google Scholar] [CrossRef] [PubMed]
- Birkemeier, K.L. Imaging of solid congenital abdominal masses: A review of the literature and practical approach to image interpretation. Pediatr. Radiol. 2020, 50, 1907–1920. [Google Scholar] [CrossRef]
- Liu, C.; Zhang, W.; Song, H. Nephron-sparing surgery in the treatment of pediatric renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusions. J. Pediatr. Surg. 2017, 52, 1492–1495. [Google Scholar] [CrossRef]
- Zhu, Q.Q.; Wang, Z.Q.; Zhu, W.R.; Chen, W.X.; Wu, J.T. The multislice CT findings of renal carcinoma associated with XP11.2 translocation/TFE gene fusion and collecting duct carcinoma. Acta. Radiol. 2013, 54, 355–362. [Google Scholar] [CrossRef]
- Ross, H.; Argani, P. Xp11 translocation renal cell carcinoma. Pathology 2010, 42, 369–373. [Google Scholar] [CrossRef]
- Camparo, P.; Vasiliu, V.; Molinie, V.; Couturier, J.; Dykema, K.J.; Petillo, D.; Furge, K.A.; Comperat, E.M.; Lae, M.; Bouvier, R.; et al. Renal translocation carcinomas: Clinicopathologic, immunohistochemical, and gene expression profiling analysis of 31 cases with a review of the literature. Am. J. Surg. Pathol. 2008, 32, 656–670. [Google Scholar] [CrossRef]
- Xu, H.S.; Balcacer, P.; Zhang, Z.; Zhang, L.; Yee, E.U.; Sun, M.R.; Tsai, L.L. Characterizing T2 iso- and hypo-intense renal masses on MRI: Can templated algorithms improve accuracy? Clin. Imaging 2021, 72, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Kay, F.U.; Canvasser, N.E.; Xi, Y.; Pinho, D.F.; Costa, D.N.; Diaz de Leon, A.; Khatri, G.; Leyendecker, J.R.; Yokoo, T.; Lay, A.H.; et al. Diagnostic Performance and Interreader Agreement of a Standardized MR Imaging Approach in the Prediction of Small Renal Mass Histology. Radiology 2018, 287, 543–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aslan, M.; Aslan, A.; Arıöz Habibi, H.; Kalyoncu Uçar, A.; Özmen, E.; Bakan, S.; Kuruğoğlu, S.; Adaletli, İ. Diffusion-weighted MRI for differentiating Wilms tumor from neuroblastoma. Diagn. Interv. Radiol. 2017, 23, 403–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schenk, J.P.; Graf, N.; Günther, P.; Ley, S.; Göppl, M.; Kulozik, A.; Rohrschneider, W.K.; Tröger, J. Role of MRI in the management of patients with nephroblastoma. Eur. Radiol. 2008, 18, 683–691. [Google Scholar] [CrossRef]
- Siegel, M.J.; Chung, E.M. Wilms’ tumor and other pediatric renal masses. Magn. Reson. Imaging Clin. N. Am. 2008, 16, 479–497. [Google Scholar] [CrossRef] [PubMed]
- Hotker, A.M.; Mazaheri, Y.; Wibmer, A.; Zheng, J.; Moskowitz, C.S.; Tickoo, S.K.; Russo, P.; Hricak, H.; Akin, O. Use of DWI in the differentiation of renal cortical tumors. Am. J. Roentgenol. 2016, 206, 100–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meeus, E.M.; Zarinabad, N.; Manias, K.A.; Novak, J.; Rose, H.E.L.; Dehghani, H.; Foster, K.; Morland, B.; Peet, A.C. Diffusion-weighted MRI and intravoxel incoherent motion model for diagnosis of pediatric solid abdominal tumors. J. Magn. Reson. Imaging 2018, 47, 1475–1486. [Google Scholar] [CrossRef] [Green Version]
- Sobh, D.M.; El Hawary, G.E.S.M.; Abou El Ghar, M.; El-Diasty, T.A.E.M.; El-Sayed Settein, M.; ElShaer, S.; Tantawy, M.S.E. Role of diffusion weighted MR imaging in characterization of focal kidney and upper urinary tract lesions. Egypt. J. Radiol. Nucl. Med. 2016, 47, 1689–1700. [Google Scholar] [CrossRef] [Green Version]
- Zhu, J.; Luo, X.; Gao, J.; Li, S.; Li, C.; Chen, M. Application of diffusion kurtosis tensor MR imaging in characterization of renal cell carcinomas with different pathological types and grades. Cancer Imaging 2021, 21, 30. [Google Scholar] [CrossRef]
- Burkart, M.; Sanford, S.; Dinner, S.; Sharp, L.; Kinahan, K. Future health of AYA survivors. Pediatr. Blood Cancer 2019, 66, e27516. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Fidler-Benaoudia, M.; Keegan, T.H.; Hipp, H.S.; Jemal, A.; Siegel, R.L. Cancer statistics for adolescents and young adults, 2020. CA Cancer J. Clin. 2020, 70, 443–459. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient nr. | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| T2-weighted imaging | ||||||
| Repetition time (ms) | 7500 | 447 | 1400 | 454 | 2457 | 2457 |
| Echo time (ms) | 123 | 90 | 92 | 90 | 100 | 100 |
| Slice thickness (mm) | 5.5 | 1.15 | 4 | 1.15 | 5 | 5 |
| Echo train length | 17 | 85 | 256 | 85 | 39 | 39 |
| Slicing gap | 6.5 | 1.15 | 4.4 | 1.15 | 5 | 5 |
| Acquisition matrix | 320 × 224 | 348 × 348 | 384 × 194 | 348 × 348 | 452 × 78 | 452 × 78 |
| T1-weighted imaging | ||||||
| Repetition time (ms) | 6.3 | 5.5 | 4.7 | 5.4 | 5.5 | 5.5 |
| Echo time (ms) | 3.1 | 2.7 | 2.4 | 2.7 | 2.7 | 2.7 |
| Slice thickness (mm) | 5 | 3 | 3 | 3 | 3 | 3 |
| Echo train length | 1 | 60 | 1 | 60 | 60 | 60 |
| Slicing gap | 2.5 | 1.5 | NS | 1.5 | 1.5 | 1.5 |
| Acquisition matrix | 288 × 192 | 232 × 233 | 320 × 170 | 232 × 233 | 232 × 233 | 260 × 261 |
| Diffusion weighted imaging | ||||||
| Repetition time (ms) | 13333 | 2084 | 5300 | 2084 | 2398 | 2398 |
| Echo time (ms) | 634 | 72 | 75 | 72 | 73 | 73 |
| Slice thickness (mm) | 6 | 5 | 6 | 5 | 5 | 5 |
| Echo train length | 1 | 35 | 1 | 35 | 35 | 35 |
| Slicing gap | 7.2 | 5 | 7.2 | 5 | 5 | 5 |
| Acquisition matrix | NS | 88 × 70 | 192 × 153 | 88 × 70 | 88 × 70 | 88 × 70 |
| b values | 0/50/600/1000 | 0/50/200/400/800 | 0/500 | 0/50/200/400/800 | 0/100/1000 | 0/100/1000 |
| Patient nr. | 1 | 2 | 3 | 4 | 5 | 6 | ||
|---|---|---|---|---|---|---|---|---|
| Clinical characteristics | Age (months) | 184 | 63 | 179 | 109 | 63 | 193 | |
| Sex | Female | Female | Female | Male | Female | Male | ||
| Tumor side | Right | Left | Right | Left | Right | Left | ||
| Pre-operative chemotherapy | No | Yes | No | No | Yes | No | ||
| Surgical approach | TN | TN | TN | TN | TN | TN | ||
| Tumor stage | 1 | 1 | 2 | 3 | 1 | 3 | ||
| Biopsy performed | No | No | Yes | No | No | No | ||
| Pathology findings | Weight of the specimen (gram) | 2100 | NS | 210 | 610 | 753 | 820 | |
| Tested for MiT-RCC (test) | No | Yes (FISH) | Yes (FISH) | Yes (FISH) | Yes (FISH, RNA-seq) | Yes (RNA-seq) | ||
| Histopathological subtype | FH-RCC | ccRCC | MiT-RCC | NOS | ccRCC | MiT-RCC | ||
| Genetic analysis | FH-mutation d | NS | NS | NS | None | NS | ||
| General tumor characteristics on MRI | Tumor volume (cm3) | 2191 | 110 | 29 | 353 | 433 | 554 | |
| Location of the tumor | Indist | Central | Peripheral | Peripheral | Central | Indist | ||
| Regional lymph nodes | No | No | No | No | No | No | ||
| Shape | Lobulated | Round | Lobulated | Lobulated | Lobulated | Round | ||
| Margins | Well-def | Well-def | Ill-def | Ill-def | Well-def | Well-def | ||
| Pseudocapsule | Yes | Yes | No | No | Yes | Yes | ||
| Growth pattern on MRI | Capsule rupture/invasion | No | No | Yes | Yes | No | No | |
| Infiltrative growth pattern | No | No | Yes | No | No | No | ||
| Venous invasion/Tumor thrombus | No | No | No | No | No | No | ||
| MRI characteristics of solid components of the tumor | T2W imaging | Pattern | Hetero | Homo | Homo | Homo | Homo | Hetero |
| Intensity | Hypo, Iso | Iso | Hypo | Hypo | Hypo | Hypo | ||
| T1W imaging | Pattern | Hetero | Homo | Homo | Homo | Homo | Hetero | |
| Intensity | Iso | Iso | Iso | Hypo | Iso | Hypo | ||
| Enhancement, degree and pattern | Strong, homo | Mild, homo | Strong, homo | Strong, homo | NA a | Mild, hetero | ||
| Hemorrhage, degree | No | Yes, ext b | No | Yes, minimal | No | Yes, min c | ||
| Necrosis | No | No | No | No | No | Yes | ||
| Cysts | Yes | Yes b | No | No | No | Yes | ||
| Septation | No | No | No | No | No | No | ||
| Fatty tissue | No | No | No | No | No | No | ||
| Subcapsular fluid | No | No | No | No | No | Yes c | ||
| Increased vascularity | No | No | Yes | Yes | No | Yes | ||
| Median surface ROIs (cm2) | 4.29 | 0.45 | 2.66 | 9.06 | 18.14 | 2.61 | ||
| Median ADC valued (×10−3 mm2/s) | 1.20 | 1.05 | 0.98 | 1.20 | 0.70 | 0.80 | ||
| Author (Year) | Country | Nr. of Patients | Age (Years) | Sex (M:F) | Histological Subtype | Study Design | Tumor Side (L:R) | Tumor Size (largest Diameter in cm) | Tumor Location | T1-Weighted Imaging Appearance | T2-Weighted Imaging Appearance | Contrast-Enhanced Imaging Appearance | Tumor Composition and Growth Pattern | Necrosis (nr. of Total) | Hemorrhage (nr. of Total) | Vascular Involvement (nr. of Total) | Intra-Tumoral Fat | Regional Lymph Node Involvement/Lymph node Metastases (nr. of Total) | (Distant) Metastases Other Than Lymph Nodes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Norena-Rengifo (2021) [42] | Col | 1 | 12 | 1:0 | RMC | CR | 1:0 | NS | central | inter | hetero, hypo | hypovascular | solid, infiltrative | 1 | NS | absent | absent | renal hilum, para-aortic | absent |
| Koetter (2020) [43] | USA | 1 | 16 | 0:1 | P1 | CR | 1:0 | 17.3 | exophytic | NS | NS | hetero | cystic–solid | 1 | NS | absent | NS | peri-aortic, peri-caval | absent |
| Schaefer (2017) [44] | USA | 1 | 14 | 1:0 | MiT | CR | 0:1 | 5.2 | upper pole | homo | hetero | NS | solid | NS | NS | absent | NS | absent | absent |
| Okabe (2016) [45] | Japan | 1 | 4 | 1:0 | CHR | CR | 0:1 | 2.5 | NS | hypo | hetero, hyper | NS | well defined | 1 | NS | NS | NS | NS | NS |
| Zhou (2016) [46] | China | 1 | 17 | 1:0 | CC a | CR | B | 0.2–2.0 a | B | hypo | hypo | strong | multiple B a | NS | NS | absent | NS | absent | synchronous CNS hemangioblastoma and pancreatic neuroendocrine tumor |
| Liu (2014) [24] | China | 3 | 15–33 | 1:2 | MiT | CR | 1:2 | 18; 6; 11 | cortical | hyper | hetero, hypo | hetero hypo | solid (2); cystic (1); infiltrative (3) | focal (2), central (1) | inter-tumor (3) | absent | NS | regional (2) | absent |
| Wang (2014) [19] | USA | 7 b | 13–33 | 3:4 | MiT | RS | 4:3 | 3.5–22 | medullary (2); medullary cortical (4); exophytic (1) | iso (1); hyper (1); hetero (5) | hypo (1); hyper (1); hetero (5) | hetero: mild (1); moderate (4); marked rim/capsule (2) | irregular (6); not irregular (1); well defined (4); ill defined (3) | 7 | 6 | 3 | NS | regional (4), cervical (1) | absent |
| Koo (2013) [47] | South Korea | 1 | 28 | 0:1 | MiT | RS | 0:1 | 2.7 | NS | NS | hetero, hyper | NS | well defined | NS | NS | NS | absent | NS | absent |
| Dang (2012) [48] | USA | 2 | 18; 31 | 1:1 | MiT | RS | 0:1 B | 8.9; 4.9 | NS | hetero, hyper | NS | limited hetero (1); NS (1) | NS | 1 | 2 | absent | NS | absent | absent |
| Downey (2012) [49] | USA | 2 c | NS | NS | NS | RS | NS | NS | NS | hetero, hyper (1); NS (1) | NS | hetero | NS | NS | intra-tumoral (1) | NS | NS | NS | NS |
| Kato (2011) [50] | Japan | 1 | 18 | 1:0 | MiT | CR | 0:1 | 4.1 | peripheral | NS | hetero, hypo rim, central hyper | delayed peripheral hyper, rim hyper | well demarcated | NS | NS | NS | absent (hemosiderin) | NS | NS |
| Blitman (2005) [51] | USA | 6 (3) d | 15–27 | 3:3 | RMC | RS | 0:6 | NS | central | NS | NS | hetero | infiltrative, ill-defined margins | 4 | intra-tumoral (4); sub-capsular (1) | ipsilateral renal vein (2); encasement vascular pedicle (3) | NS | cervical (6); retroperitoneal (5) e | liver (2); lung (3) |
| Adachi (2003) [52] | Japan | 1 | 4 | 1:0 | CCP | CR | 1:0 | NS | NS | NS | NS | hyper walls | complicated cyst | NS | cystic (1) | NS | NS | absent | absent |
| Author (Year) | Country | Nr. of Patients | Age (Median Years, Range) | Sex (M:F) | Study Design | Tumor Side (L:R) | Tumor Size (Largest Diameter in cm) | Tumor Location | T1-Weighted Imaging Appearance | T2-Weighted Imaging Appearance | Contrast-Enhanced Imaging Appearance | Diffusion Restriction (ADC value x10−3 mm2/s) | Tumor Composition and Growth Pattern | Necrosis (nr. of Total) | Hemorrhage (nr. of Total) | Vascular Involvement (nr. of Total) | Intra-Tumoral Fat | Regional Lymph Node involvement/Lymph Node Metastases (nr. of total) | (Distant) Metastases Other than Lymph Nodes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tohi (2021) [54] | Japan | 1 | 78 | 1:0 | CR | R | 2.0 | posterior | iso | hypo | NS | no restriction a | well circumscribed, no capsule | NS | NS | NS | absent | absent | absent |
| Dai (2019) [55] | China | 16 | 47.4 (20–76) | 9:7 | RS | 9:7 | 1.7–14.6 | endophytic epicenter (14) | hypo (2), iso (5), hyper (9) | hetero (14); hypo (13), iso (6), hyper (2) | hetero (7) | hyper on DWI (b0/500) ((16) | irregular (9), regular (7); complete capsule (11), incomplete capsule (5); solid (11), cystic (2), mixed (3) | NS | 5 | 2 | absent | 3 | retroperitoneal space and liver (1); lung (1) |
| Gong (2018) [56] | China | 2 | 50; 45 | 1:1 | CR | 1:1 | 10.6; 5.2 | upper pole (1); lower pole (1) | iso (1), hypo (1) | hypo (2) | hetero (1) | NS | irregular (1) | 1 | NS | absent | NS | 1 | absent |
| Chen (2017) [57] | China | 2 | 46; 30 | 0:2 | RS | 0:2 | 7.8; NS | NS | hetero iso (2) | hetero (2); hyper (1), hypo (1) | hetero (2) | relatively high signal on DWI (b0/800) (1) | oval (17), irregular (4); solid (4), cystic (1), mixed (16) b | NS | NS | v. renalis (1) | NS | 1 | liver (1) |
| Schaefer (2017) [44] | USA | 1 | 14 | 1:0 | CR | 0:1 | 5.2 | upper pole | homo | hetero | NS | NS | solid | NS | NS | absent | NS | absent | absent |
| Yu (2016) [58] | China | 1 | 40 | 1:0 | CR | 0:1 | 12 | NS | iso | hetero hypo-hyper | NS | NS | well defined, irregular | 1 | patchy (1) | absent | NS | 1 | absent |
| D’Antonio (2016) [59] | Italy | 1 | 71 | 0:1 | CR | B c | 12.0 | NS | hetero | hyper | NS | NS | poorly circumscribed (1) | 1 | 1 | NS | NS | NS | NS |
| Liu (2014) [24] | China | 4 | 15–45 | 1:3 | RS | 1:3 | 4–18 | cortical (4) | hyper (4) | hypo (3), hyper (1) | Hypo | NS | infiltrative (4); solid (3); cystic (1) | focal (3), center (1) | inter-tumor (4) | absent | absent | lymphadenopathy (3) | absent |
| Wang (2014) [19] | USA | 9 | 13–46 | 3:6 | RS | 4:5 | 2–22 | medullary (3), medullary cortical (4), exophytic (1), pelvis (1) | iso (1), hyper (3), hetero (5) | hypo (1), hyper (2), hetero (60) | hetero: mild (1), moderate (6), marked rim/capsule (2) | NS | capsule (3); irregular (8); oval (1); well defined (5); ill defined (4) | 8 | 7 | 4 | NS | regional (5), cervical (1) | absent |
| Koo (2013) [47] | South Korea | 2 | 28; 71 | 0:2 | RS | 0:2 | 2.7; 4.6 | NS | NS | hetero, hypo (2) | NS | NS | well defined (2) | NS | intra-tumoral (1) | NS | absent | NS | absent |
| Dang (2012) [48] | USA | 2 | 18; 31 | RS | 0:1 B | 8.9; 4.9 | NS | hetero, hyper | NS | limited hetero (1); NS (1) | NS | NS | 1 | 2 | absent | NS | absent | absent | |
| Razek (2011) [13] | Egypt | 4 | 5–67 d | NS | PS | NS | NS | NS | NS | NS | NS | mean 1.50 ±0.97 (1.37–1.62) (b0/800) | NS | NS | NS | NS | NS | NS | NS |
| Kato (2011) [50] | Japan | 1 | 18 | 1:0 | CR | 0:1 | 4.1 | peripheral | NS | hetero, hypo rim, central hyper | delayed peripheral hyper, rim hyper | NS | well demarcated | NS | NS | NS | absent (hemosiderin) | NS | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beek, J.N.v.d.; Krijger, R.R.d.; Nievelstein, R.A.J.; Bex, A.; Klijn, A.J.; Heuvel-Eibrink, M.M.v.d.; Littooij, A.S. MRI Characteristics of Pediatric and Young-Adult Renal Cell Carcinoma: A Single-Center Retrospective Study and Literature Review. Cancers 2023, 15, 1401. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15051401
Beek JNvd, Krijger RRd, Nievelstein RAJ, Bex A, Klijn AJ, Heuvel-Eibrink MMvd, Littooij AS. MRI Characteristics of Pediatric and Young-Adult Renal Cell Carcinoma: A Single-Center Retrospective Study and Literature Review. Cancers. 2023; 15(5):1401. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15051401
Chicago/Turabian StyleBeek, Justine N. van der, Ronald R. de Krijger, Rutger A. J. Nievelstein, Axel Bex, Aart J. Klijn, Marry M. van den Heuvel-Eibrink, and Annemieke S. Littooij. 2023. "MRI Characteristics of Pediatric and Young-Adult Renal Cell Carcinoma: A Single-Center Retrospective Study and Literature Review" Cancers 15, no. 5: 1401. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15051401