
Early Results of a Screening Program for Skin Cancer in Liver Transplant Recipients: A Cohort Study
 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Participants—Inclusion and Exclusion Criteria
2.3. Data Sources
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Evaluation of the Screening Program during the Screening Period
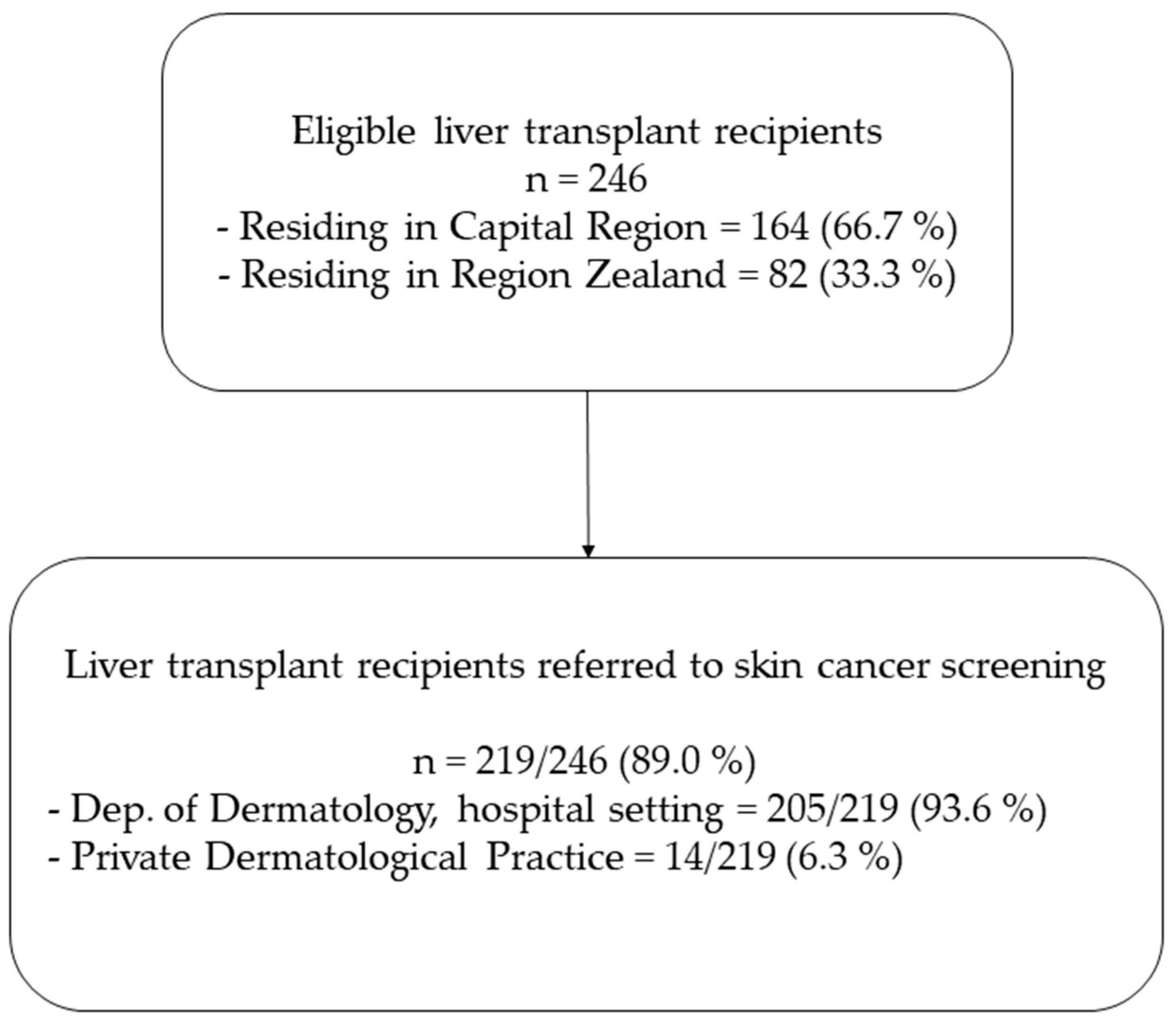
3.1.1. Referral Rates
3.1.2. Visiting Frequency during the Screening Period
3.1.3. Years from Liver Transplantation to the First Screening
3.2. Patient Characteristics
Patient Characteristics
3.3. Skin Cancer Incidence and Risk Factors
3.3.1. Incidence Proportions and Rates
3.3.2. Risk Factors for Skin Cancer/Preneoplastic Lesions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nordin, A.; Åberg, F.; Pukkala, E.; Pedersen, C.R.; Storm, H.H.; Rasmussen, A.; Bennet, W.; Olausson, M.; Wilczek, H.; Isoniemi, H. Decreasing Incidence of Cancer after Liver Transplantation-A Nordic Population-Based Study over 3 Decades. Am. J. Transpl. 2018, 18, 952–963. [Google Scholar] [CrossRef]
- Otley, C.C.; Pittelkow, M.R. Skin Cancer in Liver Transplant Recipients. Liver Transpl. 2000, 6, 253–262. [Google Scholar] [CrossRef]
- Berman, H.; Shimshak, S.; Reimer, D.; Brigham, T.; Hedges, M.S.; Degesys, C.; Tolaymat, L. Skin Cancer in Solid Organ Transplant Recipients: A Review for the Nondermatologist. Mayo Clin. Proc. 2022, 97, 2355–2368. [Google Scholar] [CrossRef]
- Howard, M.D.; Su, J.C.; Chong, A.H. Skin Cancer Following Solid Organ Transplantation: A Review of Risk Factors and Models of Care. Am. J. Clin. Dermatol. 2018, 19, 585–597. [Google Scholar] [CrossRef]
- Chockalingam, R.; Downing, C.; Tyring, S.K. Cutaneous Squamous Cell Carcinomas in Organ Transplant Recipients. J. Clin. Med. 2015, 4, 1229. [Google Scholar] [CrossRef]
- Gutierrez-Dalmau, A.; Campistol, J.M. Immunosuppressive Therapy and Malignancy in Organ Transplant Recipients: A Systematic Review. Drugs 2007, 67, 1167–1198. [Google Scholar] [CrossRef] [PubMed]
- Grulich, A.E.; van Leeuwen, M.T.; Falster, M.O.; Vajdic, C.M. Incidence of Cancers in People with HIV/AIDS Compared with Immunosuppressed Transplant Recipients: A Meta-Analysis. Lancet 2007, 370, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Acuna, S.A.; Huang, J.W.; Scott, A.L.; Micic, S.; Daly, C.; Brezden-Masley, C.; Kim, S.J.; Baxter, N.N. Cancer Screening Recommendations for Solid Organ Transplant Recipients: A Systematic Review of Clinical Practice Guidelines. Am. J. Transpl. 2017, 17, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Dharia, A.; Boulet, J.; Sridhar, V.S.; Kitchlu, A. Cancer Screening in Solid Organ Transplant Recipients: A Focus on Screening Liver, Lung, and Kidney Recipients for Cancers Related to the Transplanted Organ. Transplantation 2022, 106, E64–E65. [Google Scholar] [CrossRef] [PubMed]
- Crow, L.D.; Jambusaria-Pahlajani, A.; Chung, C.L.; Baran, D.A.; Lowenstein, S.E.; Abdelmalek, M.; Ahmed, R.L.; Anadkat, M.J.; Arcasoy, S.M.; Berg, D.; et al. Initial Skin Cancer Screening for Solid Organ Transplant Recipients in the United States: Delphi Method Development of Expert Consensus Guidelines. Transpl. Int. 2019, 32, 1268–1276. [Google Scholar] [CrossRef]
- Chan, A.W.; Fung, K.; Austin, P.C.; Kim, S.J.; Singer, L.G.; Baxter, N.N.; Alhusayen, R.; Rochon, P.A. Improved Keratinocyte Carcinoma Outcomes with Annual Dermatology Assessment after Solid Organ Transplantation: Population-Based Cohort Study. Am. J. Transpl. 2019, 19, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Finkenstedt, A.; Graziadei, I.W.; Oberaigner, W.; Hilbe, W.; Nachbaur, K.; Mark, W.; Margreiter, R.; Vogel, W. Extensive Surveillance Promotes Early Diagnosis and Improved Survival of De Novo Malignancies in Liver Transplant Recipients. Am. J. Transpl. 2009, 9, 2355–2361. [Google Scholar] [CrossRef] [PubMed]
- Fekecs, T.; Kádár, Z.; Battyáni, Z.; Kalmár-Nagy, K.; Szakály, P.; Horváth, Ó.P.; Wéber, G.; Ferencz, A. Incidence of Nonmelanoma Skin Cancer after Human Organ Transplantation: Single-Center Experience in Hungary. Transpl. Proc. 2010, 42, 2333–2335. [Google Scholar] [CrossRef] [PubMed]
- Fuente, M.J.; Sabat, M.; Roca, J.; Lauzurica, R.; Fernández-Figueras, M.T.; Ferrándiz, C. A Prospective Study of the Incidence of Skin Cancer and Its Risk Factors in a Spanish Mediterranean Population of Kidney Transplant Recipients. Br. J. Dermatol. 2003, 149, 1221–1226. [Google Scholar] [CrossRef] [PubMed]
- Wenande, E.; Togsverd-Bo, K.; Hastrup, A.; Lei, U.; Philipsen, P.A.; Haedersdal, M. Skin Cancer Development Is Strongly Associated with Actinic Keratosis in Solid Organ Transplant Recipients: A Danish Cohort Study. Dermatology 2023, 239, 393–402. [Google Scholar] [CrossRef]
- Harwood, C.A.; Mesher, D.; McGregor, J.M.; Mitchell, L.; Leedham-Green, M.; Raftery, M.; Cerio, R.; Leigh, I.M.; Sasieni, P.; Proby, C.M. A Surveillance Model for Skin Cancer in Organ Transplant Recipients: A 22-Year Prospective Study in an Ethnically Diverse Population. Am. J. Transpl. 2013, 13, 119–129. [Google Scholar] [CrossRef]
- Baldwin, S.; Au, S. One-Year Review of the SCREEN (Skin Cancer Post-Transplant) Clinic: What We Have Learned. J. Cutan. Med. Surg. 2017, 21, 80–81. [Google Scholar] [CrossRef]
- Piai, G.; Battarra, V.C.; Miglioresi, L.; Nacca, M.; Valente, G. How to Improve Compliance With Dermatologic Screening in Liver Transplant Recipients: Experience in a (Spoke) Peripheral Center for Follow-Up. Transpl. Proc. 2019, 51, 184–186. [Google Scholar] [CrossRef]
- Papier, K.; Gordon, L.G.; Khosrotehrani, K.; Isbel, N.; Campbell, S.; Griffin, A.; Green, A.C. Management of Organ Transplant Recipients Attending a High-Throughput Skin Cancer Surgery and Surveillance Clinic in Queensland. Br. J. Dermatol. 2019, 180, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Paganelli, A.; Magistri, P.; Kaleci, S.; Chester, J.; Pezzini, C.; Catellani, B.; Ciardo, S.; Casari, A.; Giusti, F.; Bassoli, S.; et al. De Novo Skin Neoplasms in Liver-Transplanted Patients: Single-Center Prospective Evaluation of 105 Cases. Medicina 2022, 58, 1444. [Google Scholar] [CrossRef] [PubMed]
- Herrero, J.I.; España, A.; Quiroga, J.; Sangro, B.; Pardo, F.; Alvárez-Cienfuegos, J.; Prieto, J. Nonmelanoma Skin Cancer after Liver Transplantation. Study of Risk Factors. Liver Transpl. 2005, 11, 1100–1106. [Google Scholar] [CrossRef]
- Krynitz, B.; Edgren, G.; Lindelöf, B.; Baecklund, E.; Brattström, C.; Wilczek, H.; Smedby, K.E. Risk of Skin Cancer and Other Malignancies in Kidney, Liver, Heart and Lung Transplant Recipients 1970 to 2008—A Swedish Population-Based Study. Int. J. Cancer 2013, 132, 1429–1438. [Google Scholar] [CrossRef] [PubMed]
- Collett, D.; Mumford, L.; Banner, N.R.; Neuberger, J.; Watson, C. Comparison of the Incidence of Malignancy in Recipients of Different Types of Organ: A UK Registry Audit. Am. J. Transpl. 2010, 10, 1889–1896. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Patobank–En Landsdækkende Databank Fra Pato-Anatomiske Undersøgelser. Available online: https://www.patobank.dk/ (accessed on 25 October 2023).
- Gupta, V.; Sharma, V.K. Skin Typing: Fitzpatrick Grading and Others. Clin. Dermatol. 2019, 37, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Videnscenter for Transplantation (VCT). Available online: https://www.rigshospitalet.dk/afdelinger-og-klinikker/hjerte/infektionssygdomme/viroimmunologisk-forskningsenhed/forskningsprojekter/Sider/VCT.aspx (accessed on 25 October 2023).
- Ducroux, E.; Boillot, O.; Ocampo, M.A.; Decullier, E.; Roux, A.; Dumortier, J.; Kanitakis, J.; Jullien, D.; Euvrard, S. Skin Cancers after Liver Transplantation: Retrospective Single-Center Study on 371 Recipients. Transplantation 2014, 98, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Garrett, G.L.; Blanc, P.D.; Boscardin, J.; Lloyd, A.A.; Ahmed, R.L.; Anthony, T.; Bibee, K.; Breithaupt, A.; Cannon, J.; Chen, A.; et al. Incidence of and Risk Factors for Skin Cancer in Organ Transplant Recipients in the United States. JAMA Dermatol. 2017, 153, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Modaresi Esfeh, J.; Hanouneh, I.A.; Dalal, D.; Tabba, A.; Lopez, R.; Pagadala, M.; Eghtesad, B.; Zein, N.N. The Incidence and Risk Factors of De Novo Skin Cancer in the Liver Transplant Recipients. Int. J. Organ. Transpl. Med. 2012, 3, 157. [Google Scholar] [CrossRef]
- Ramsay, H.M.; Fryer, A.A.; Reece, S.; Smith, A.G.; Harden, P.N. Clinical Risk Factors Associated with Nonmelanoma Skin Cancer in Renal Transplant Recipients. Am. J. Kidney Dis. 2000, 36, 167–176. [Google Scholar] [CrossRef]
- Campos, G.R.; Boin, I.d.F.S.F.; de Campos Junior, I.D.; Cintra, M.L. Study of Factors Affecting the Incidence of Skin Cancer in patientsafter Liver Transplant. An. Bras. Dermatol. 2017, 92, 492. [Google Scholar] [CrossRef]
- Sargen, M.R.; Cahoon, E.K.; Yu, K.J.; Madeleine, M.M.; Zeng, Y.; Rees, J.R.; Lynch, C.F.; Engels, E.A. Spectrum of Nonkeratinocyte Skin Cancer Risk among Solid Organ Transplant Recipients in the US. JAMA Dermatol. 2022, 158, 414–425. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Characteristic | Recipients without Skin Cancer/Preneoplastic Lesions, n = 173 | Recipients with Skin Cancer/Preneoplastic Lesions, n = 32 | p |
|---|---|---|---|
| Age, median (IQR) | 55.7 (47.2–63.5) | 67.4 (60.8–73.6) | <0.01 * |
| Sex, male, n (%) | 98 (56.6%) | 20 (62.5%) | 0.67 |
| Age at LTX•, yrs., median (IQR) | 48.9 (39.0–55.0) | 49.6 (42.9–55.7) | 0.45 |
| Time since LTX, yrs., median (IQR) | 6.0 (3.0–10.0) | 14.0 (11.8–23.3) | <0.01 * |
| Follow-up, yrs., median (IQR) | 1.0 (0.0–3.0) | 3.0 (2.0–3.0) | <0.01 * |
| Number of visits to dermatologist, median, (IQR) | 2.0 (1.0–3.0) | 5.0 (3.0–7.5) | <0.01 * |
| Dermatological visits, n (%) ≥2 visits <2 visits | 98/170 (57.6%) 72/170 (42.4%) | 24/27 (88.9%) 3/27 (9.4%) | <0.01 * |
| Dermatological skin cancer screening ≤ 2 yrs. after LTX, n (%) | 70/157 (44.6%) | 2/31 (6.5%) | <0.01 * |
| Indication for LTX, n (%) Cirrhosis (alcoholic and cryptogenic) Primary sclerosing cholangitis Primary biliary cholangitis Hepatitis C Hepatocellular carcinoma Other | 40/173 (23.1%) 50/173 (28.9%) 13/173 (7.5%) 3/173 (1.7%) 13/173 (8.0%) 45/173 (26.0%) | 5/32 (15.6%) 5/32 (15.6%) 3/32 (9.4%) 0/32 (0.0%) 1/32 (3.1%) 15/32 (46.9%) | 0.96 |
| Smoking status, n (%) Current Former Never | 22/171 (12.9%) 64/171 (37.4%) 85/171 (49.7%) | 4/31 (22.6%) 7/31 (22.6%) 16/31 (51.6%) | 0.19 |
| Current immunosuppression, n (%) CNI (Tacrolimus, Ciclosporin) mTOR inhibitor (Everolimus) Mycophenolate Azathioprin Corticosteroid | 157/173 (90.8%) 17/173 (9.8%) 131/173 (75.7%) 13/173 (7.5%) 81/173 (46.8%) | 29/32 (90.6%) 2/32 (6.3%) 23/32 (71.9%) 5/32 (15.6%) 16/32 (50.0%) | 0.66 |
| Sun exposure, n (%) † Outdoor work Leisure exposure Sun damage/Actinic degeneration | 17/69 (24.6%) 29/72 (40.3%) 26/80 (32.5%) | 4/12 (33.3%) 9/14 (64.3%) 10/14 (71.4%) | 0.75 |
| Fitzpatrick skin phototype, n (%) I, II, III IV, V, VI | 57/68 (83.8%) 11/68 (16.2%) | 9/11 (81.8%) 2/11 (18.2%) | 1.00 |
| Incidence | Incidence Proportion, (%) | Incidence Rate, per 1000 Person-Year |
|---|---|---|
| Skin cancer (BCC, SCC, or MM) BCC SCC MM | 24/205 (11.7%) 18/205 (8.8%) 10/205 (4.9%) 0/205 (0.0%) | 71.5 51.3 27.1 0.0 |
| Preneoplastic lesions (actinic keratosis or Bowen’s disease) Actinic keratosis Bowen’s Disease | 20/205 (9.6%) 17/205 (8.3%) 5/205 (2.4%) | 58.0 48.3 13.2 |
| Skin cancer/preneoplastic lesions (incl. BCC, SCC, MM, actinic keratosis, or Bowen’s disease) | 32/205 (15.6%) | 103.2 |
| Risk Factors for Skin Cancer | Univariable HR (95% CI) | p | Multivariable HR (95% CI) | p |
|---|---|---|---|---|
| Age, pr. decade | 2.41 (1.56–3.71) | <0.01 * | 1.44 (0.89–2.32) | 0.14 |
| Time since LTX, pr. decade | 3.15 (2.01–4.94) | <0.01 * | 1.61 (0.81–3.21) | 0.18 |
| Actinic keratosis, yes vs. no | 8.81 (3.88–20.00) | <0.01 * | 2.75 (0.81–9.40) | 0.11 |
| Risk Factors for Preneoplastic Lesions | Univariable HR (95% CI) | p | Multivariable HR (95% CI) | p |
|---|---|---|---|---|
| Age, pr. decade | 2.72 (1.65–4.48) | <0.01 * | 1.52 (0.91–2.55) | 0.11 |
| Time since LTX, pr. decade | 4.31 (2.64–7.02) | <0.01 * | 3.19 (1.65–6.18) | <0.01 * |
| Dermatological skin cancer screening ≤ 2 yrs. after LTX, yes vs. no | 0.15 (0.03–0.63) | 0.01 * | 0.93 (0.16–5.44) | 0.94 |
| Risk Factors for Skin Cancer/Preneoplastic Lesions | Univariable HR (95% CI) | p | Multivariable HR (95% CI) | p |
|---|---|---|---|---|
| Age, pr. decade | 2.52 (1.71–3.72) | <0.01 * | 1.46 (1.00–2.18) | 0.06 |
| Time since LTX, pr. decade | 4.18 (2.80–6.25) | <0.01 * | 2.81 (1.64–4.80) | <0.01 * |
| Dermatological skin cancer screening ≤ 2 yrs. after LTX, yes vs. no | 0.09 (0.02–0.37) | <0.01 * | 0.36 (0.08–1.79) | 0.21 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akdag, D.; Rasmussen, A.; Nielsen, S.D.; Møller, D.L.; Togsverd-Bo, K.; Wenande, E.; Haedersdal, M.; Pommergaard, H.-C. Early Results of a Screening Program for Skin Cancer in Liver Transplant Recipients: A Cohort Study. Cancers 2024, 16, 1224. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16061224
Akdag D, Rasmussen A, Nielsen SD, Møller DL, Togsverd-Bo K, Wenande E, Haedersdal M, Pommergaard H-C. Early Results of a Screening Program for Skin Cancer in Liver Transplant Recipients: A Cohort Study. Cancers. 2024; 16(6):1224. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16061224
Chicago/Turabian StyleAkdag, Delal, Allan Rasmussen, Susanne Dam Nielsen, Dina Leth Møller, Katrine Togsverd-Bo, Emily Wenande, Merete Haedersdal, and Hans-Christian Pommergaard. 2024. "Early Results of a Screening Program for Skin Cancer in Liver Transplant Recipients: A Cohort Study" Cancers 16, no. 6: 1224. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16061224