
Preliminary Experience with Virtual Monoenergetic Imaging and Iodine Mapping in the Primary Staging of Endometrial Cancer

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
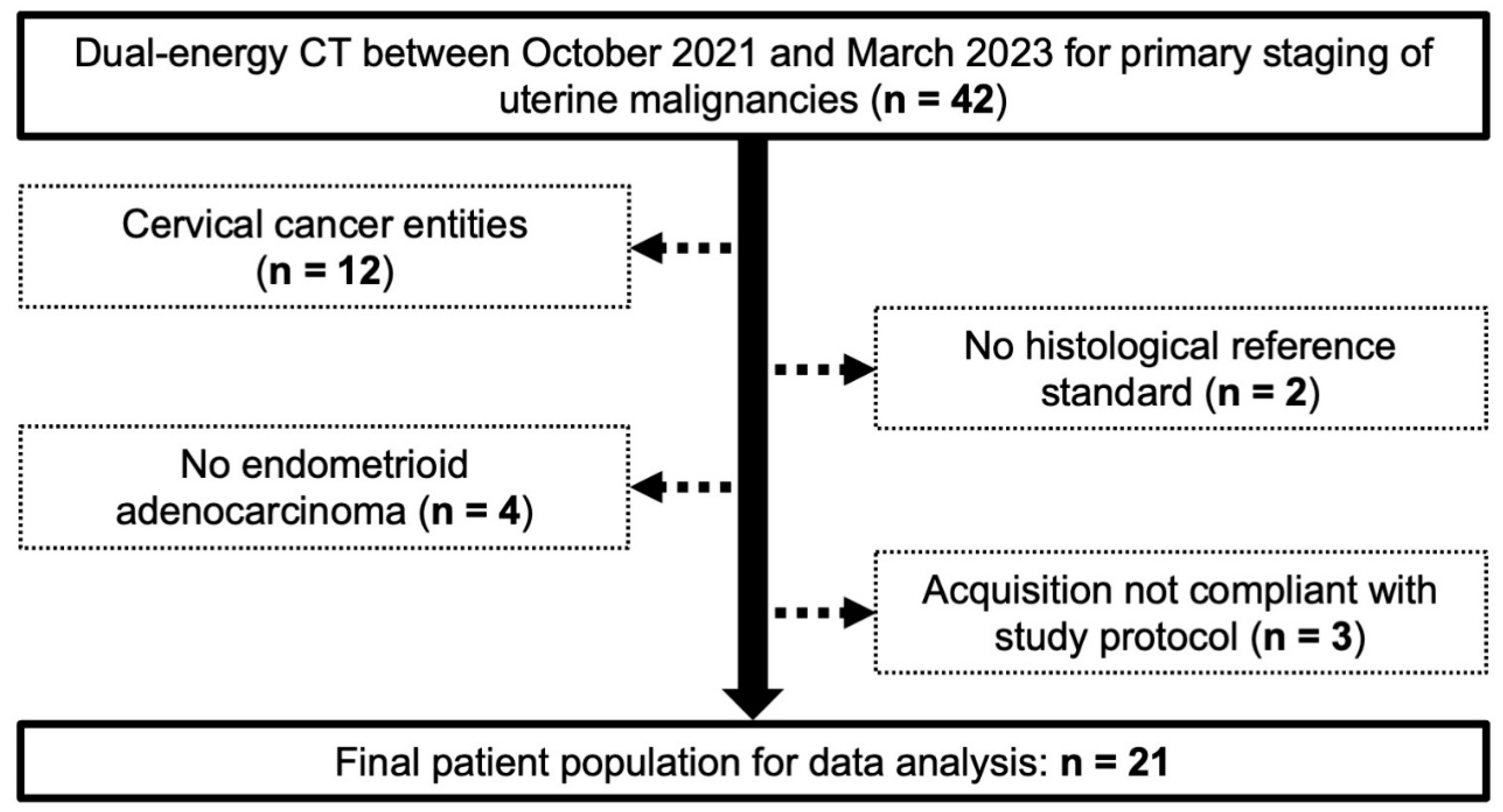
2.1. Patients
2.2. Imaging
2.3. Study Analysis
2.4. Statistics
3. Results
3.1. Study Sample
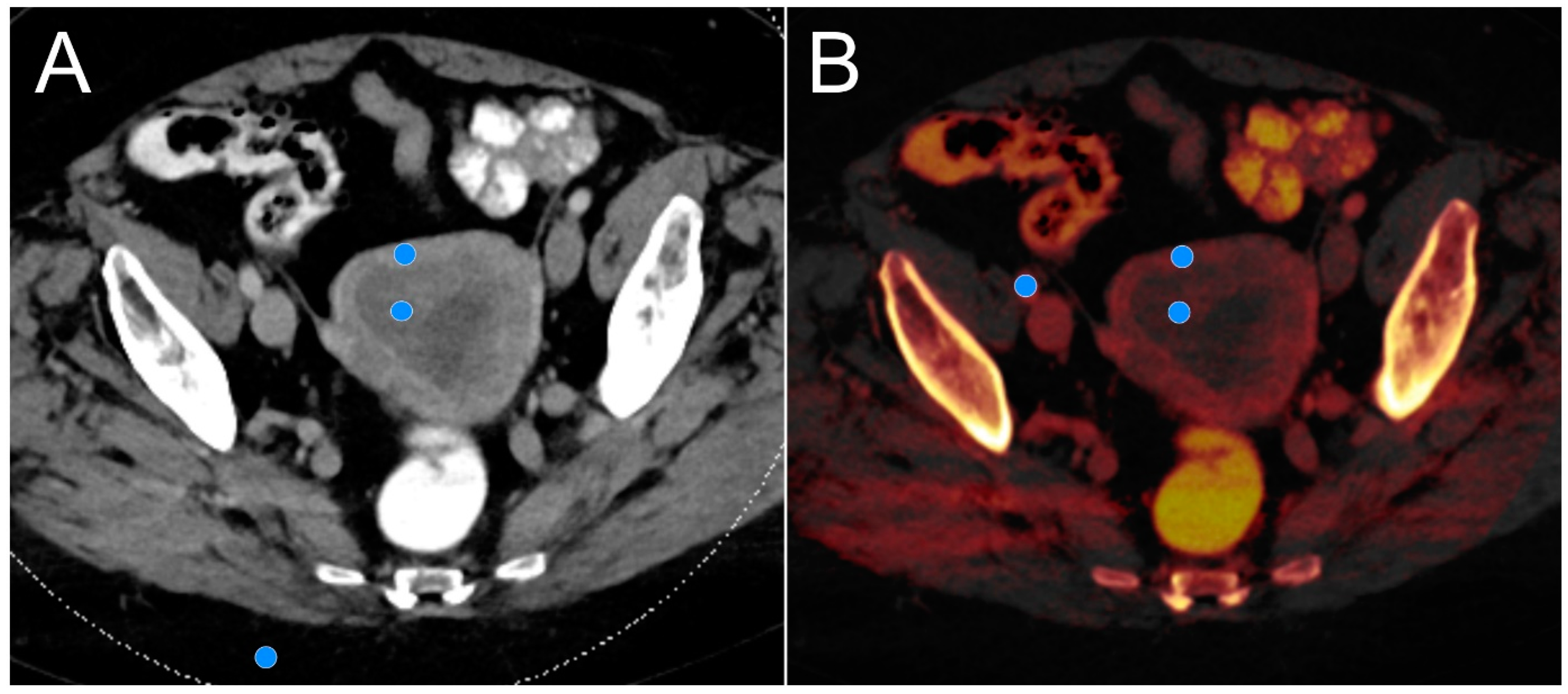
3.2. Objective Lesion Conspicuity Assessment
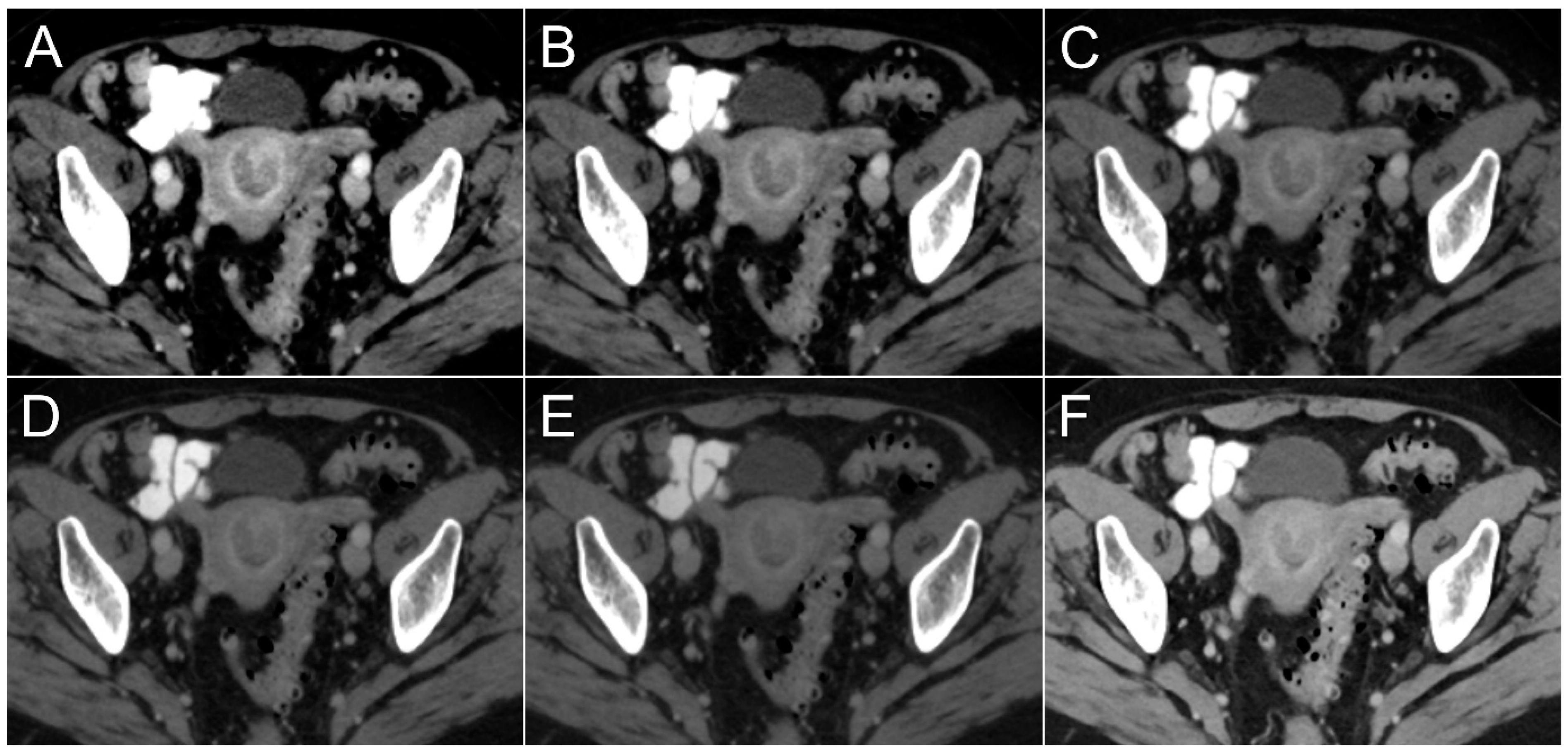
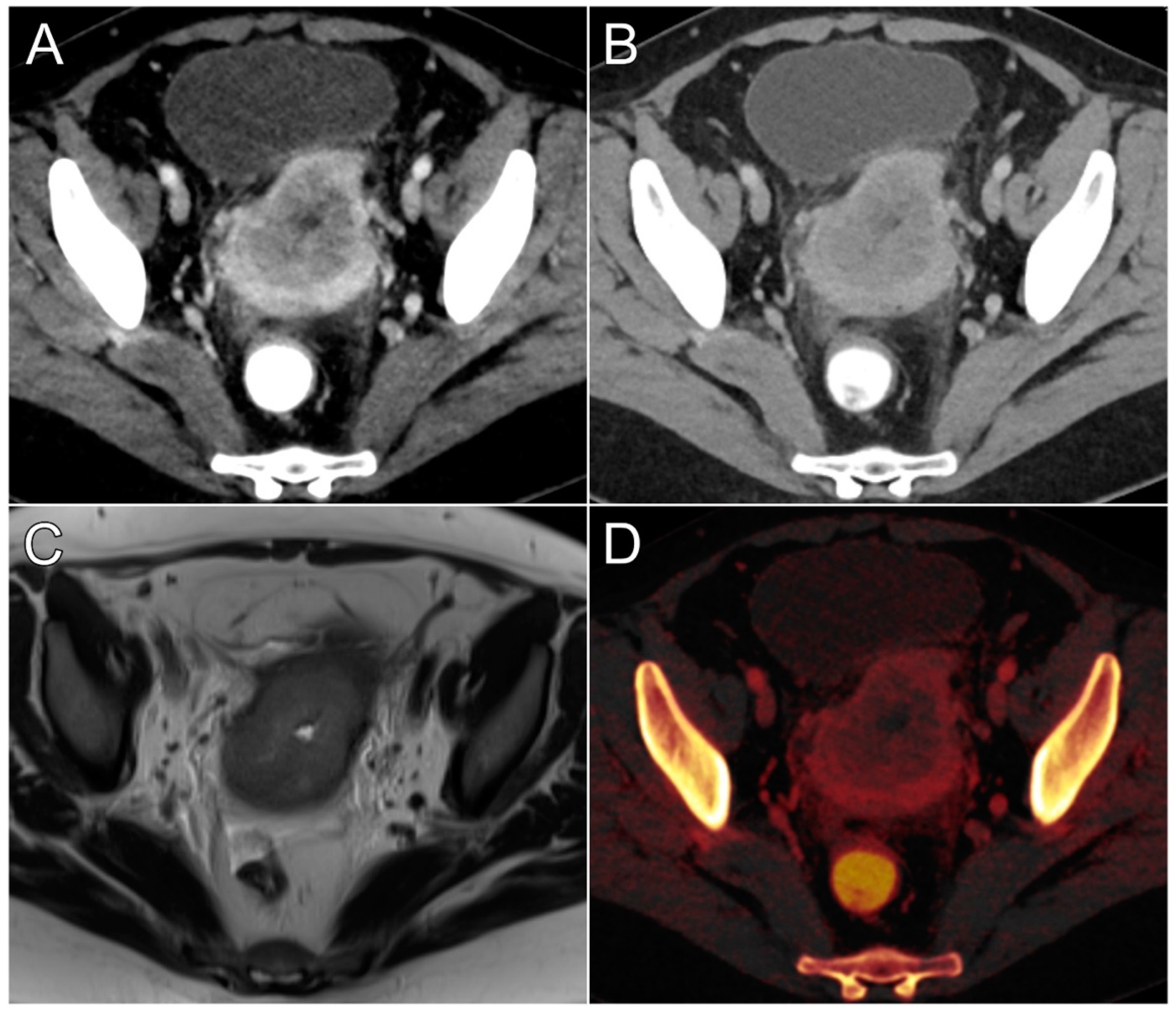
3.3. Subjective Lesion Conspicuity Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CNR | contrast-to-noise ratio |
| DECT | dual-energy computed tomography |
| EIA | external iliac artery |
| ICC | intraclass correlation coefficient |
| NIC | normalized iodine concentration |
| PEI | polyenergetic imaging/images |
| ROI | region of interest |
| VMI | virtual monoenergetic imaging/images |
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Nougaret, S.; Horta, M.; Sala, E.; Lakhman, Y.; Thomassin-Naggara, I.; Kido, A.; Masselli, G.; Bharwani, N.; Sadowski, E.; Ertmer, A.; et al. Endometrial Cancer MRI staging: Updated Guidelines of the European Society of Urogenital Radiology. Eur. Radiol. 2019, 29, 792–805. [Google Scholar] [CrossRef]
- Torres, M.L.; Weaver, A.L.; Kumar, S.; Uccella, S.; Famuyide, A.O.; Cliby, W.A.; Dowdy, S.C.; Gostout, B.S.; Mariani, A. Risk factors for developing endometrial cancer after benign endometrial sampling. Obstet. Gynecol. 2012, 120, 998–1004. [Google Scholar] [CrossRef]
- Lin, M.Y.; Dobrotwir, A.; McNally, O.; Abu-Rustum, N.R.; Narayan, K. Role of imaging in the routine management of endometrial cancer. Int. J. Gynaecol. Obstet. 2018, 143 (Suppl. S2), 109–117. [Google Scholar] [CrossRef]
- Lalwani, N.; Dubinsky, T.; Javitt, M.C.; Gaffney, D.K.; Glanc, P.; Elshaikh, M.A.; Kim, Y.B.; Lee, L.J.; Pannu, H.K.; Royal, H.D.; et al. ACR Appropriateness Criteria® pretreatment evaluation and follow-up of endometrial cancer. Ultrasound Q. 2014, 30, 21–28. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Leng, S.; Yu, L.; Fletcher, J.G. Dual- and Multi-Energy CT: Principles, Technical Approaches, and Clinical Applications. Radiology 2015, 276, 637–653. [Google Scholar] [CrossRef] [PubMed]
- Adam, S.Z.; Rabinowich, A.; Kessner, R.; Blachar, A. Spectral CT of the abdomen: Where are we now? Insights Imaging 2021, 12, 138. [Google Scholar] [CrossRef] [PubMed]
- Hounsfield, G.N. Computerized transverse axial scanning (tomography): Part 1. Description of system. Br. J. Radiol. 2014, 46, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- De Cecco, C.N.; Darnell, A.; Rengo, M.; Muscogiuri, G.; Bellini, D.; Ayuso, C.; Laghi, A. Dual-energy CT: Oncologic applications. AJR Am. J. Roentgenol. 2012, 199 (Suppl. S5), S98–S105. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Zhou, Y.; Zheng, Q.; Yan, G.; Liao, H.; Du, S.; Zhang, X.; Lv, F.; Zhang, Z.; Li, Y.M. Dual-energy CT with virtual monoenergetic images and iodine maps improves tumor conspicuity in patients with pancreatic ductal adenocarcinoma. Insights Imaging 2022, 13, 153. [Google Scholar] [CrossRef] [PubMed]
- Nagayama, Y.; Tanoue, S.; Inoue, T.; Oda, S.; Nakaura, T.; Utsunomiya, D.; Yamashita, Y. Dual-layer spectral CT improves image quality of multiphasic pancreas CT in patients with pancreatic ductal adenocarcinoma. Eur. Radiol. 2020, 30, 394–403. [Google Scholar] [CrossRef]
- Rizzo, S.; Femia, M.; Radice, D.; Del Grande, M.; Franchi, D.; Origgi, D.; Buscarino, V.; Mauro, A.; Bellomi, M. Evaluation of deep myometrial invasion in endometrial cancer patients: Is dual-energy CT an option? Radiol. Med. 2018, 123, 13–19. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Böning, G.; Feldhaus, F.; Adelt, S.; Kahn, J.; Fehrenbach, U.; Streitparth, F. Clinical routine use of virtual monochromatic datasets based on spectral CT in patients with hypervascularized abdominal tumors—Evaluation of effectiveness and efficiency. Acta Radiol. 2019, 60, 425–432. [Google Scholar] [CrossRef]
- Martin, S.S.; Wichmann, J.L.; Pfeifer, S.; Leithner, D.; Lenga, L.; Reynolds, M.A.; D’Angelo, T.; Hammerstingl, R.; Gruber-Rouh, T.; Vogl, T.J.; et al. Impact of noise-optimized virtual monoenergetic dual-energy computed tomography on image quality in patients with renal cell carcinoma. Eur. J. Radiol. 2017, 97, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bellini, D.; Gupta, S.; Ramirez-Giraldo, J.C.; Fu, W.; Stinnett, S.S.; Patel, B.; Mileto, A.; Marin, D. Use of a Noise Optimized Monoenergetic Algorithm for Patient-Size Independent Selection of an Optimal Energy Level During Dual-Energy CT of the Pancreas. J. Comput. Assist. Tomogr. 2017, 41, 39–47. [Google Scholar] [CrossRef]
- Hanson, G.J.; Michalak, G.J.; Childs, R.; McCollough, B.; Kurup, A.N.; Hough, D.M.; Frye, J.M.; Fidler, J.L.; Venkatesh, S.K.; Leng, S.; et al. Low kV versus dual-energy virtual monoenergetic CT imaging for proven liver lesions: What are the advantages and trade-offs in conspicuity and image quality? A pilot study. Abdom. Radiol. 2018, 43, 1404–1412. [Google Scholar] [CrossRef]
- Beer, L.; Toepker, M.; Ba-Ssalamah, A.; Schestak, C.; Dutschke, A.; Schindl, M.; Wressnegger, A.; Ringl, H.; Apfaltrer, P. Objective and subjective comparison of virtual monoenergetic vs. polychromatic images in patients with pancreatic ductal adenocarcinoma. Eur. Radiol. 2019, 29, 3617–3625. [Google Scholar] [CrossRef]
- Kulkarni, N.M.; Fung, A.; Kambadakone, A.R.; Yeh, B.M. CT Techniques, Protocols, Advancements and Future Directions in Liver Diseases. Magn. Reson. Imaging Clin. N. Am. 2021, 29, 305. [Google Scholar] [CrossRef]
- Tawfik, A.M.; Razek, A.A.; Kerl, J.M.; Nour-Eldin, N.E.; Bauer, R.; Vogl, T.J. Comparison of dual-energy CT-derived iodine content and iodine overlay of normal, inflammatory and metastatic squamous cell carcinoma cervical lymph nodes. Eur. Radiol. 2014, 24, 574–580. [Google Scholar] [CrossRef]
- Patel, B.N.; Vernuccio, F.; Meyer, M.; Godwin, B.; Rosenberg, M.; Rudnick, N.; Harring, S.; Nelson, R.; Ramirez-Giraldo, J.C.; Farjat, A.; et al. Dual-Energy CT Material Density Iodine Quantification for Distinguishing Vascular From Nonvascular Renal Lesions: Normalization Reduces Intermanufacturer Threshold Variability. AJR Am. J. Roentgenol. 2019, 212, 366–376. [Google Scholar] [CrossRef]
- Wu, Y.Y.; Wei, C.; Wang, C.B.; Li, N.Y.; Zhang, P.; Dong, J.N. Preoperative Prediction of Cervical Nodal Metastasis in Papillary Thyroid Carcinoma: Value of Quantitative Dual-Energy CT Parameters and Qualitative Morphologic Features. AJR Am. J. Roentgenol. 2021, 216, 1335–1343. [Google Scholar] [CrossRef]
- Huflage, H.; Kunz, A.S.; Hendel, R.; Kraft, J.; Weick, S.; Razinskas, G.; Sauer, S.T.; Pennig, L.; Bley, T.A.; Grunz, J.P. Obesity-Related Pitfalls of Virtual versus True Non-Contrast Imaging-An Intraindividual Comparison in 253 Oncologic Patients. Diagnostics 2023, 13, 1558. [Google Scholar] [CrossRef]
- Higashigaito, K.; Euler, A.; Eberhard, M.; Flohr, T.G.; Schmidt, B.; Alkadhi, H. Contrast-Enhanced Abdominal CT with Clinical Photon-Counting Detector CT: Assessment of Image Quality Comparison with Energy-Integrating Detector, C.T. Acad. Radiol. 2022, 29, 689–697. [Google Scholar] [CrossRef]
- Wrazidlo, R.; Walder, L.; Estler, A.; Gutjahr, R.; Schmidt, B.; Faby, S.; Fritz, J.; Nikolaou, K.; Horger, M.; Hagen, F. Radiation Dose Reduction in Contrast-Enhanced Abdominal CT: Comparison of Photon-Counting Detector CT with 2nd Generation Dual-Source Dual-Energy CT in an oncologic cohort. Acad. Radiol. 2023, 30, 855–862. [Google Scholar] [CrossRef]
- Corr, B.; Cosgrove, C.; Spinosa, D.; Guntupalli, S. Endometrial cancer: Molecular classification and future treatments. BMJ Med. 2022, 1, e000152. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Size | 21 Women |
|---|---|
| Age [years] | 66.8 ± 12 |
| Size [cm] | 164.9 ± 6.0 |
| Weight [kg] | 85.5 ± 17.0 |
| BMI [kg/cm2] | 31.4 ± 6.0 |
| T stage T1a T1b T2 T3a T3b T4 | 7 (33.3%) 5 (23.8%) 2 (9.5%) 3 (14.3%) 3 (14.3%) 1 (4.8%) |
| Grading Grade 1 Grade 2 Grade 3 | 2 (9.5%) 9 (42.9%) 10 (47.6%) |
| 40 keV | 50 keV | 60 keV | 70 keV | 80 keV | PEI | |
|---|---|---|---|---|---|---|
| Image noise [HU] | 25.0 ± 5.2 | 22.8 ± 20.0 | 13.9 ± 2.8 | 11.4 ± 2.2 | 9.9 ± 1.9 | 7.8 ± 1.5 |
| Tumor contrast [HU] | 106.6 ± 45.0 | 75.5 ± 28.3 | 49.9 ± 21.1 | 36.8 ± 16.0 | 28.3 ± 13.0 | 31.7 ± 13.1 |
| CNR | 4.4 ± 2.0 | 4.1 ± 1.9 | 3.7 ± 1.4 | 3.3 ± 1.5 | 3.0 ± 1.4 | 4.2 ± 2.1 |
| NICtumor [mg/mL] | 0.3 ± 0.1 | |||||
| NICmyometrium [mg/mL] | 0.6 ± 0.1 | |||||
| Tumor Conspicuity | 40 keV | 50 keV | 60 keV | 70 keV | 80 keV | PEI |
|---|---|---|---|---|---|---|
| Very high (5) | 43 (68.3%) | 16 (25.4%) | 2 (3.2%) | 0 (0%) | 0 (0%) | 0 (0%) |
| High (4) | 18 (28.6%) | 39 (61.9%) | 24 (38.1%) | 11 (17.5%) | 4 (6.3%) | 12 (19.0%) |
| Moderate (3) | 2 (3.2%) | 8 (12.7%) | 35 (55.5%) | 33 (52.4%) | 19 (30.2%) | 42 (66.7%) |
| Fair (2) | 0 (0%) | 0 (0%) | 2 (3.2%) | 19 (30.2%) | 31 (49.2%) | 9 (14.3%) |
| Low (1) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 9 (14.3%) | 0 (0%) |
| Median (IQR) | 5 (4–5) | 4 (4–4.5) | 3 (3–4) | 3 (2–3) | 2 (2–3) | 3 (3–3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sauer, S.T.; Huflage, H.; Christner, S.A.; Patzer, T.S.; Kiesel, M.; Quenzer, A.; Kunz, A.S.; Bley, T.A.; Grunz, J.-P. Preliminary Experience with Virtual Monoenergetic Imaging and Iodine Mapping in the Primary Staging of Endometrial Cancer. Cancers 2024, 16, 1229. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16061229
Sauer ST, Huflage H, Christner SA, Patzer TS, Kiesel M, Quenzer A, Kunz AS, Bley TA, Grunz J-P. Preliminary Experience with Virtual Monoenergetic Imaging and Iodine Mapping in the Primary Staging of Endometrial Cancer. Cancers. 2024; 16(6):1229. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16061229
Chicago/Turabian StyleSauer, Stephanie Tina, Henner Huflage, Sara Aniki Christner, Theresa Sophie Patzer, Matthias Kiesel, Anne Quenzer, Andreas Steven Kunz, Thorsten Alexander Bley, and Jan-Peter Grunz. 2024. "Preliminary Experience with Virtual Monoenergetic Imaging and Iodine Mapping in the Primary Staging of Endometrial Cancer" Cancers 16, no. 6: 1229. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16061229