
Internet Access and Use by Patients with Gynecologic Malignancies: A Cross-Sectional Study

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Digital Device Availability
3.2. Digital Device Use
3.3. Internet Access
3.4. Use of the Internet as a Source of Information
3.5. Use of the Internet as a Source of Information, Physician–Patient Interactions, and Therapy Decision-Making
3.6. Use of the Internet for Communication Purposes
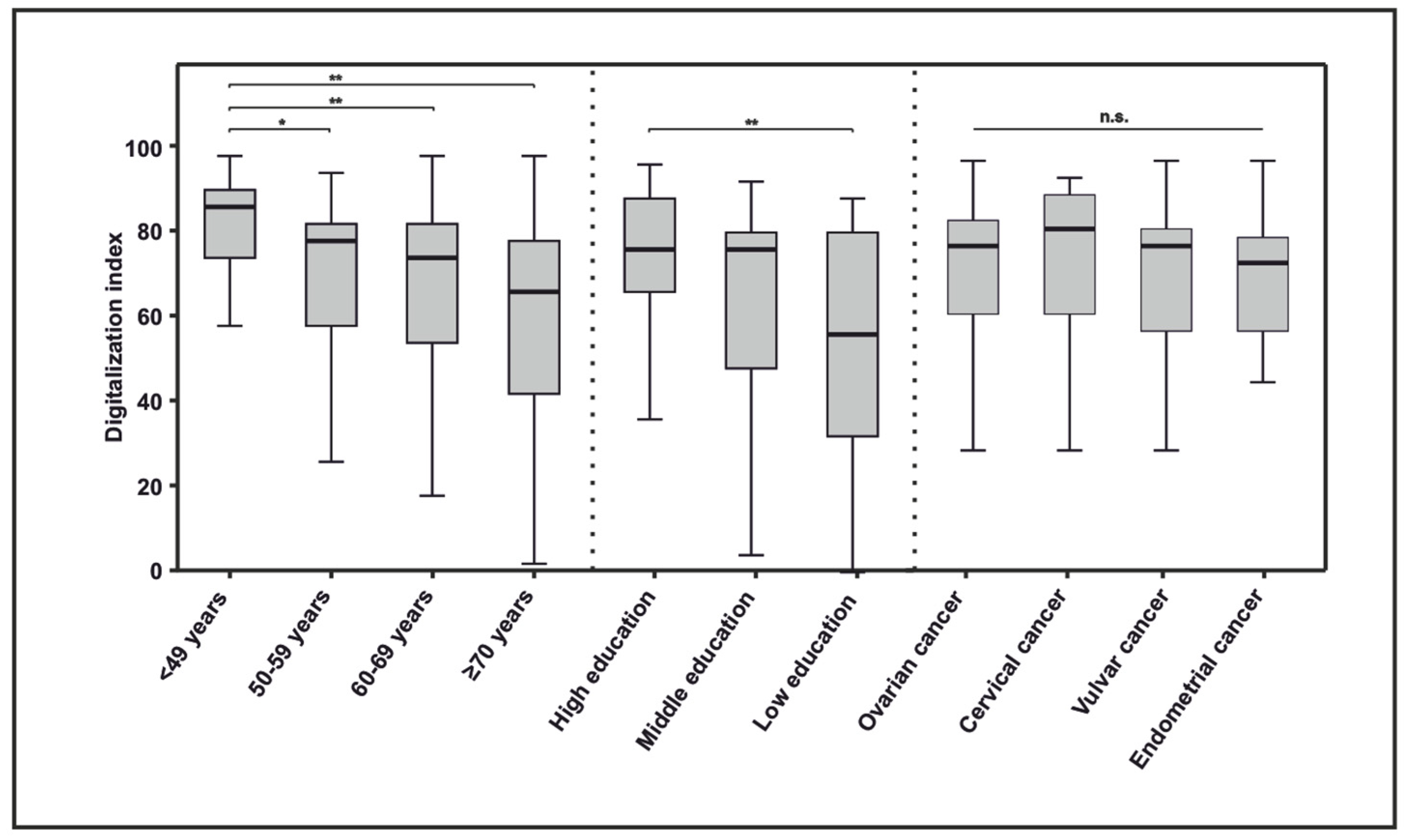
3.7. Digitalization Index
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Kruse, C.S.; Bolton, K.; Freriks, G. The effect of patient portals on quality outcomes and its implications to meaningful use: A systematic review. J. Med. Internet Res. 2015, 17, e44. [Google Scholar] [CrossRef] [PubMed]
- Turner, K.; Clary, A.; Hong, Y.R.; Alishahi Tabriz, A.; Shea, C.M. Patient Portal Barriers and Group Differences: Cross-Sectional National Survey Study. J. Med. Internet Res. 2020, 22, e18870. [Google Scholar] [CrossRef]
- Steffens, D.; Denehy, L.; Solomon, M.; Koh, C.; Ansari, N.; McBride, K.; Carey, S.; Bartyn, J.; Lawrence, A.S.; Sheehan, K.; et al. Consumer Perspectives on the Adoption of a Prehabilitation Multimodal Online Program for Patients Undergoing Cancer Surgery. Cancers 2023, 15, 5039. [Google Scholar] [CrossRef] [PubMed]
- Garavand, A.; Khodaveisi, T.; Aslani, N.; Hosseiniravandi, M.; Shams, R.; Behmanesh, A. Telemedicine in cancer care during COVID-19 pandemic: A systematic mapping study. Health Technol. 2023, 1–14. [Google Scholar] [CrossRef]
- Mostafaei, A.; Sadeghi-Ghyassi, F.; Kabiri, N.; Hajebrahimi, S. Experiences of patients and providers while using telemedicine in cancer care during COVID-19 pandemic: A systematic review and meta-synthesis of qualitative literature. Support. Care Cancer 2022, 30, 10483–10494. [Google Scholar] [CrossRef] [PubMed]
- Koksal, M.O.; Akgul, B. The role of digital health technologies in disaster response. Lancet 2023, 401, 1566–1567. [Google Scholar] [CrossRef]
- Huang, Y.; Upadhyay, U.; Dhar, E.; Kuo, L.J.; Syed-Abdul, S. A Scoping Review to Assess Adherence to and Clinical Outcomes of Wearable Devices in the Cancer Population. Cancers 2022, 14, 4437. [Google Scholar] [CrossRef] [PubMed]
- Griffin, J.M.; Kroner, B.L.; Wong, S.L.; Preiss, L.; Smith, A.W.; Cheville, A.L.; Mitchell, S.A.; Lancki, N.; Hassett, M.J.; Schrag, D.; et al. Disparities in Electronic Health Record Portal Access and Use among Patients with Cancer. J. Natl. Cancer Inst. 2023, 116, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Mallmann, C.A.; Domrose, C.M.; Schroder, L.; Engelhardt, D.; Bach, F.; Rueckel, H.; Abramian, A.; Kaiser, C.; Mustea, A.; Faridi, A.; et al. Digital Technical and Informal Resources of Breast Cancer Patients From 2012 to 2020: Questionnaire-Based Longitudinal Trend Study. JMIR Cancer 2021, 7, e20964. [Google Scholar] [CrossRef]
- Phelps, R.G.; Taylor, J.; Simpson, K.; Samuel, J.; Turner, A.N. Patients’ continuing use of an online health record: A quantitative evaluation of 14,000 patient years of access data. J. Med. Internet Res. 2014, 16, e241. [Google Scholar] [CrossRef]
- Gerber, D.E.; Laccetti, A.L.; Chen, B.; Yan, J.; Cai, J.; Gates, S.; Xie, Y.; Lee, S.J. Predictors and intensity of online access to electronic medical records among patients with cancer. J. Oncol. Pract. 2014, 10, e307–e312. [Google Scholar] [CrossRef] [PubMed]
- Luoh, R.P.; Tevaarwerk, A.J.; Chandereng, T.; Smith, E.M.; Carroll, C.B.; Emamekhoo, H.; Sesto, M.E. Patterns and predictors of cancer-specific patient health portal usage among patients with cancer: Results from the UWCCC Survivorship Program. Cancer Med. 2021, 10, 7373–7382. [Google Scholar] [CrossRef] [PubMed]
- Vlooswijk, C.; Husson, O.; Krahmer, E.J.; Bijlsma, R.; Kaal, S.E.J.; Sleeman, S.H.E.; van de Poll-Franse, L.V.; van der Graaf, W.T.A.; Bol, N.; van Eenbergen, M.C. Differences in Internet Use and eHealth Needs of Adolescent and Young Adult Versus Older Cancer Patients; Results from the PROFILES Registry. Cancers 2021, 13, 6308. [Google Scholar] [CrossRef] [PubMed]
- Yao, R.; Zhang, W.; Evans, R.; Cao, G.; Rui, T.; Shen, L. Inequities in Health Care Services Caused by the Adoption of Digital Health Technologies: Scoping Review. J. Med. Internet Res. 2022, 24, e34144. [Google Scholar] [CrossRef] [PubMed]
- Merkel, S.; Hess, M. The Use of Internet-Based Health and Care Services by Elderly People in Europe and the Importance of the Country Context: Multilevel Study. JMIR Aging 2020, 3, e15491. [Google Scholar] [CrossRef] [PubMed]
- Grossman, L.V.; Masterson Creber, R.M.; Ancker, J.S.; Ryan, B.; Polubriaginof, F.; Qian, M.; Alarcon, I.; Restaino, S.; Bakken, S.; Hripcsak, G.; et al. Technology Access, Technical Assistance, and Disparities in Inpatient Portal Use. Appl. Clin. Inform. 2019, 10, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ye, S.; Zhou, Y.; Mao, F.; Guo, H.; Lin, Y.; Zhang, X.; Shen, S.; Shi, N.; Wang, X.; et al. Web-Based Medical Information Searching by Chinese Patients With Breast Cancer and its Influence on Survival: Observational Study. J. Med. Internet Res. 2020, 22, e16768. [Google Scholar] [CrossRef] [PubMed]
- van Eenbergen, M.C.; van de Poll-Franse, L.V.; Heine, P.; Mols, F. The Impact of Participation in Online Cancer Communities on Patient Reported Outcomes: Systematic Review. JMIR Cancer 2017, 3, e15. [Google Scholar] [CrossRef] [PubMed]
- Omboni, S.; Caserini, M.; Coronetti, C. Telemedicine and M-Health in Hypertension Management: Technologies, Applications and Clinical Evidence. High Blood Press. Cardiovasc. Prev. 2016, 23, 187–196. [Google Scholar] [CrossRef]
- Castleton, K.; Fong, T.; Wang-Gillam, A.; Waqar, M.A.; Jeffe, D.B.; Kehlenbrink, L.; Gao, F.; Govindan, R. A survey of Internet utilization among patients with cancer. Support. Care Cancer 2011, 19, 1183–1190. [Google Scholar] [CrossRef]
- Eysenbach, G. The impact of the Internet on cancer outcomes. CA Cancer J. Clin. 2003, 53, 356–371. [Google Scholar] [CrossRef] [PubMed]
- van de Poll-Franse, L.V.; van Eenbergen, M.C. Internet use by cancer survivors: Current use and future wishes. Support. Care Cancer 2008, 16, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- van Eenbergen, M.; Vromans, R.D.; Boll, D.; Kil, P.J.M.; Vos, C.M.; Krahmer, E.J.; Mols, F.; van de Poll-Franse, L.V. Changes in internet use and wishes of cancer survivors: A comparison between 2005 and 2017. Cancer 2020, 126, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Barbosa Neves, B.; Fonseca, J.R.S.; Amaro, F.; Pasqualotti, A. Social capital and Internet use in an age-comparative perspective with a focus on later life. PLoS ONE 2018, 13, e0192119. [Google Scholar] [CrossRef] [PubMed]
- Holmes, M.M. Why People Living With and Beyond Cancer Use the Internet. Integr. Cancer Ther. 2019, 18, 1534735419829830. [Google Scholar] [CrossRef] [PubMed]
- George, G.C.; Iwuanyanwu, E.C.; Buford, A.S.; Piha-Paul, S.A.; Subbiah, V.; Fu, S.; Karp, D.D.; Pant, S.; Hinojosa, C.O.; Hess, K.R.; et al. Cancer-Related Internet Use and Its Association With Patient Decision Making and Trust in Physicians Among Patients in an Early Drug Development Clinic: A Questionnaire-Based Cross-Sectional Observational Study. J. Med. Internet Res. 2019, 21, e10348. [Google Scholar] [CrossRef] [PubMed]
- Davis Giardina, T.; Menon, S.; Parrish, D.E.; Sittig, D.F.; Singh, H. Patient access to medical records and healthcare outcomes: A systematic review. J. Am. Med. Inform. Assoc. 2014, 21, 737–741. [Google Scholar] [CrossRef]
- Shaffer, K.M.; Turner, K.L.; Siwik, C.; Gonzalez, B.D.; Upasani, R.; Glazer, J.V.; Ferguson, R.J.; Joshua, C.; Low, C.A. Digital health and telehealth in cancer care: A scoping review of reviews. Lancet Digit Health 2023, 5, e316–e327. [Google Scholar] [CrossRef]
- Torrent-Sellens, J.; Diaz-Chao, A.; Soler-Ramos, I.; Saigi-Rubio, F. Modelling and Predicting eHealth Usage in Europe: A Multidimensional Approach From an Online Survey of 13,000 European Union Internet Users. J. Med. Internet Res. 2016, 18, e188. [Google Scholar] [CrossRef]
- Rodriguez, J.A.; Lipsitz, S.R.; Lyles, C.R.; Samal, L. Association Between Patient Portal Use and Broadband Access: A National Evaluation. J. Gen. Intern. Med. 2020, 35, 3719–3720. [Google Scholar] [CrossRef]
- Perzynski, A.T.; Roach, M.J.; Shick, S.; Callahan, B.; Gunzler, D.; Cebul, R.; Kaelber, D.C.; Huml, A.; Thornton, J.D.; Einstadter, D. Patient portals and broadband internet inequality. J. Am. Med. Inform. Assoc. 2017, 24, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Lleras de Frutos, M.; Casellas-Grau, A.; Sumalla, E.C.; de Gracia, M.; Borras, J.M.; Ochoa Arnedo, C. A systematic and comprehensive review of internet use in cancer patients: Psychological factors. Psychooncology 2020, 29, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Riviere, C.; Brureau, L.; Parnot, C.; Becherirat, S.; Duverger, C.; Picchi, H.; Le Roy, A.; Vuagnat, P.; Schernberg, A.; Vanquaethem, H.; et al. Effectiveness of a digital telemonitoring platform for cancer care of older patients: The ConnectElderlyPatientToDoctor study. Int. J. Cancer 2023, 152, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Bertera, E.M.; Bertera, R.L.; Morgan, R.; Wuertz, E.; Attey, A.M.O. Training Older Adults to Access Health Information. Educ. Gerontol. 2007, 33, 483–500. [Google Scholar] [CrossRef]
- Patel, K.B.; Turner, K.; Alishahi Tabriz, A.; Gonzalez, B.D.; Oswald, L.B.; Nguyen, O.T.; Hong, Y.R.; Jim, H.S.L.; Nichols, A.C.; Wang, X.; et al. Estimated Indirect Cost Savings of Using Telehealth Among Nonelderly Patients With Cancer. JAMA Netw. Open 2023, 6, e2250211. [Google Scholar] [CrossRef] [PubMed]
- Waseem, N.; Boulanger, M.; Yanek, L.R.; Feliciano, J.L. Disparities in Telemedicine Success and Their Association With Adverse Outcomes in Patients With Thoracic Cancer During the COVID-19 Pandemic. JAMA Netw. Open 2022, 5, e2220543. [Google Scholar] [CrossRef]
- Knudsen, K.E.; Willman, C.; Winn, R. Optimizing the Use of Telemedicine in Oncology Care: Postpandemic Opportunities. Clin. Cancer Res. 2021, 27, 933–936. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | N or Mean (Standard Deviation) | |
|---|---|---|
| Age (spread) | 56.2 years (20–82) | |
| Age ≤ 49 years | 39/150 | |
| Age 50–59 years | 45/150 | |
| Age 60–69 years | 43/150 | |
| Age ≥ 70 years | 23/150 | |
| Cancer entity | Ovarian cancer | 48/150 |
| Cervical cancer | 39/150 | |
| Vulvar cancer | 35/150 | |
| Endometrial cancer | 28/150 | |
| Origin | Germany | 120/147 |
| Other | 27/147 | |
| Education | No degree/low educational attainment | 21/148 |
| Middle educational attainment | 47/148 | |
| High school/College degree | 80/148 | |
| Household size | Living alone | 49/145 |
| Household size ≥ two persons | 96/145 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bach, F.; Engelhardt, D.; Mallmann, C.A.; Tamir, S.; Schröder, L.; Domröse, C.M.; Mallmann, M.R. Internet Access and Use by Patients with Gynecologic Malignancies: A Cross-Sectional Study. Cancers 2024, 16, 1677. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091677
Bach F, Engelhardt D, Mallmann CA, Tamir S, Schröder L, Domröse CM, Mallmann MR. Internet Access and Use by Patients with Gynecologic Malignancies: A Cross-Sectional Study. Cancers. 2024; 16(9):1677. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091677
Chicago/Turabian StyleBach, Frederik, David Engelhardt, Christoph A. Mallmann, Sina Tamir, Lars Schröder, Christian M. Domröse, and Michael R. Mallmann. 2024. "Internet Access and Use by Patients with Gynecologic Malignancies: A Cross-Sectional Study" Cancers 16, no. 9: 1677. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091677