
Translational Stroke Research Review: Using the Mouse to Model Human Futile Recanalization and Reperfusion Injury in Ischemic Brain Tissue

 , , , and
, , , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. From Bedside
3. From Bench
- (1)
- Are there experimental animal models capable of reproducing human LVO stroke and subsequent recanalization? Are there animal models for age, sex, and comorbid human conditions?
- (2)
- Can animal stroke models assess early endpoints, such as hemorrhagic transformation or cerebral edema?
- (3)
- Which mechanistic insight could be given by preclinical research to explain the different evolution of hypoperfused tissue?
3.1. Experimental Animal Model of Occlusion/Reperfusion: Pros and Cons
Limitations on Animal Models Use for Age, Sex, and Comorbid Human Conditions
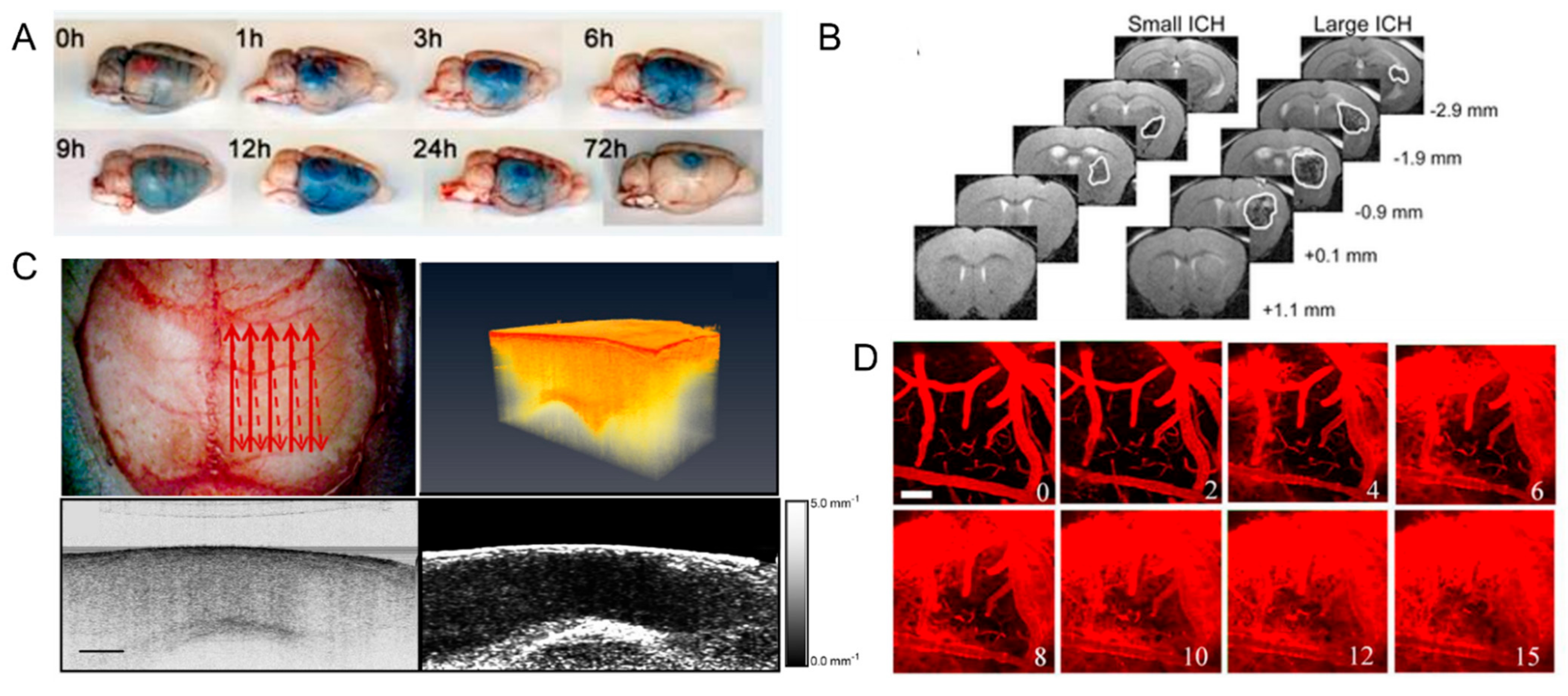
3.2. Hemorrhage and Edema Evaluation in Preclinical Research: From the Macro- to Micro-Scale
3.2.1. Ex-Vivo Studies
3.2.2. In-Vivo Studies
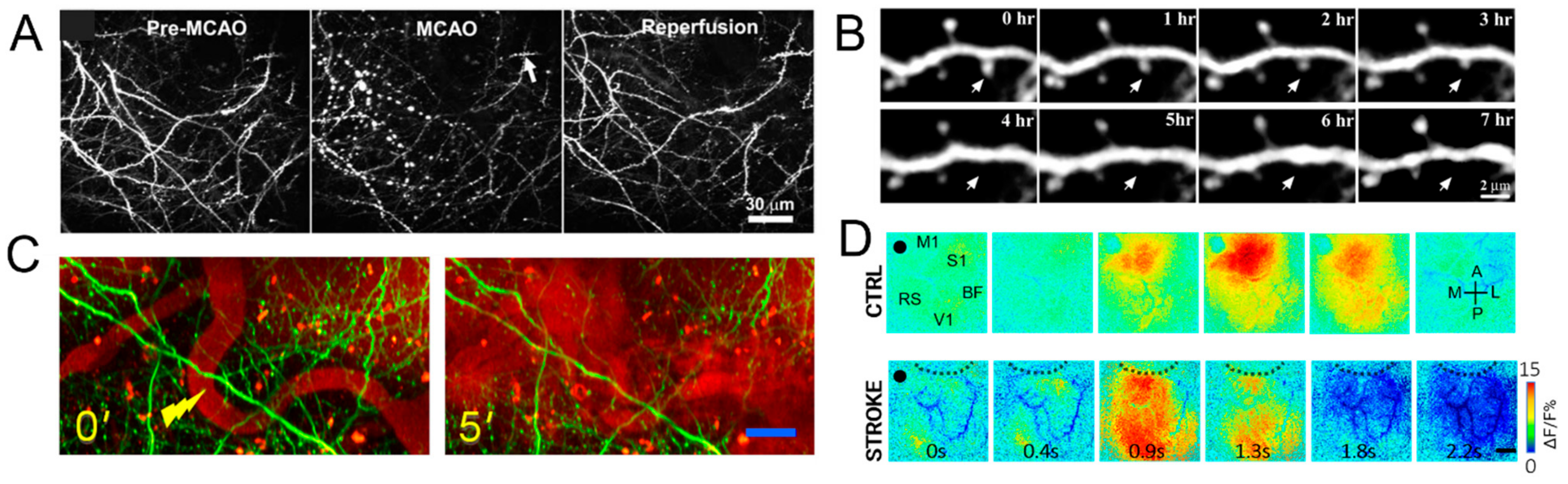
3.3. Optical Imaging to Investigate Structural and Functional Plasticity in Mouse Models of Stroke
4. Conclusions
- Stroke is most prevalent in elderly men and women, whereas preclinical models mostly test young animals.
- Stroke is more devastating in patients with multiple comorbidities not often captured by preclinical models.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nie, X.; Pu, Y.; Zhang, Z.; Liu, X.; Duan, W.; Liu, L. Futile Recanalization after Endovascular Therapy in Acute Ischemic Stroke. Biomed. Res. Int. 2018, 2018, 5879548. [Google Scholar] [CrossRef] [Green Version]
- Stoll, G.; Pham, M. Beyond recanalization—A call for action in acute stroke. Nat. Rev. Neurol. 2020, 16, 591–592. [Google Scholar] [CrossRef] [PubMed]
- Ter Schiphorst, A.; Charron, S.; Hassen, W.B.; Provost, C.; Naggara, O.; Benzakoun, J.; Seners, P.; Turc, G.; Baron, J.C.; Oppenheim, C. Tissue no-reflow despite full recanalization following thrombectomy for anterior circulation stroke with proximal occlusion: A clinical study. J. Cereb. Blood Flow Metab. 2021, 41, 253–266. [Google Scholar] [CrossRef]
- Hacke, W.; Schwab, S.; Horn, M.; Spranger, M.; De Georgia, M.; von Kummer, R. ‘Malignant’ middle cerebral artery territory infarction: Clinical course and prognostic signs. Arch. Neurol. 1996, 53, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Brogan, M.E.; Manno, E.M. Treatment of malignant brain edema and increased intracranial pressure after stroke. Curr. Treat. Opt. Neurol. 2015, 17, 327. [Google Scholar] [CrossRef] [PubMed]
- Shaw, C.M.; Alvord, E.C., Jr.; Berry, R.G. Swelling of the brain following ischemic infarction with arterial occlusion. Arch. Neurol. 1959, 1, 161–177. [Google Scholar] [CrossRef]
- Juttler, E.; Schellinger, P.D.; Aschoff, A.; Zweckberger, K.; Unterberg, A.; Hacke, W. Clinical review: Therapy for refractory intracranial hypertension in ischaemic stroke. Crit. Care 2007, 11, 231. [Google Scholar] [CrossRef] [Green Version]
- Cook, A.M.; Morgan Jones, G.; Hawryluk, G.W.J.; Mailloux, P.; McLaughlin, D.; Papangelou, A.; Samuel, S.; Tokumaru, S.; Venkatasubramanian, C.; Zacko, C.; et al. Guidelines for the Acute Treatment of Cerebral Edema in Neurocritical Care Patients. Neurocrit. Care 2020, 32, 647–666. [Google Scholar] [CrossRef] [Green Version]
- Battey, T.W.; Karki, M.; Singhal, A.B.; Wu, O.; Sadaghiani, S.; Campbell, B.C.; Davis, S.M.; Donnan, G.A.; Sheth, K.N.; Kimberly, W.T. Brain edema predicts outcome after nonlacunar ischemic stroke. Stroke 2014, 45, 3643–3648. [Google Scholar] [CrossRef] [Green Version]
- Del Zoppo, G.J. The neurovascular unit in the setting of stroke. J. Intern. Med. 2010, 267, 156–171. [Google Scholar] [CrossRef] [Green Version]
- Stokum, J.A.; Gerzanich, V.; Simard, J.M. Molecular pathophysiology of cerebral edema. J. Cereb. Blood Flow Metab. 2016, 36, 513–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernier, L.P.; Brunner, C.; Cottarelli, A.; Balbi, M. Location Matters: Navigating Regional Heterogeneity of the Neurovascular Unit. Front. Cell Neurosci. 2021, 15, 696540. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, S.; Iadecola, C. Revisiting the neurovascular unit. Nat. Neurosci. 2021, 24, 1198–1209. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.Y. Advancement in stroke research. Stroke Vasc. Neurol. 2019, 4, 61–62. [Google Scholar] [CrossRef] [Green Version]
- Zhou, M.; Shi, S.X.; Liu, N.; Jiang, Y.; Karim, M.S.; Vodovoz, S.J.; Wang, X.; Zhang, B.; Dumont, A.S. Caveolae-Mediated Endothelial Transcytosis across the Blood-Brain Barrier in Acute Ischemic Stroke. J. Clin. Med. 2021, 10, 3795. [Google Scholar] [CrossRef]
- Dong, M.X.; Hu, Q.C.; Shen, P.; Pan, J.X.; Wei, Y.D.; Liu, Y.Y.; Ren, Y.F.; Liang, Z.H.; Wang, H.Y.; Zhao, L.B.; et al. Recombinant Tissue Plasminogen Activator Induces Neurological Side Effects Independent on Thrombolysis in Mechanical Animal Models of Focal Cerebral Infarction: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158848. [Google Scholar] [CrossRef]
- Hussein, H.M.; Saleem, M.A.; Qureshi, A.I. Rates and predictors of futile recanalization in patients undergoing endovascular treatment in a multicenter clinical trial. Neuroradiology 2018, 60, 557–563. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, B.J.; Han, M.K.; Park, T.H.; Lee, K.B.; Lee, B.C.; Yu, K.H.; Oh, M.S.; Cha, J.K.; Kim, D.H.; et al. Futile reperfusion and predicted therapeutic benefits after successful endovascular treatment according to initial stroke severity. BMC Neurol. 2019, 19, 11. [Google Scholar] [CrossRef]
- Alawieh, A.; Vargas, J.; Fargen, K.M.; Langley, E.F.; Starke, R.M.; De Leacy, R.; Chatterjee, R.; Rai, A.; Dumont, T.; Kan, P.; et al. Impact of Procedure Time on Outcomes of Thrombectomy for Stroke. J. Am. Coll. Cardiol. 2019, 73, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.; Mitchell, P.J.; Demchuk, A.M.; Davalos, A.; Majoie, C.B.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Leiva-Salinas, C.; Jiang, B.; Wintermark, M. Computed Tomography, Computed Tomography Angiography, and Perfusion Computed Tomography Evaluation of Acute Ischemic Stroke. Neuroimaging Clin. N. Am. 2018, 28, 565–572. [Google Scholar] [CrossRef]
- Menon, B.K.; d’Esterre, C.D.; Qazi, E.M.; Almekhlafi, M.; Hahn, L.; Demchuk, A.M.; Goyal, M. Multiphase CT Angiography: A New Tool for the Imaging Triage of Patients with Acute Ischemic Stroke. Radiology 2015, 275, 510–520. [Google Scholar] [CrossRef] [Green Version]
- Wintermark, M.; Flanders, A.E.; Velthuis, B.; Meuli, R.; van Leeuwen, M.; Goldsher, D.; Pineda, C.; Serena, J.; van der Schaaf, I.; Waaijer, A.; et al. Perfusion-CT assessment of infarct core and penumbra: Receiver operating characteristic curve analysis in 130 patients suspected of acute hemispheric stroke. Stroke 2006, 37, 979–985. [Google Scholar] [CrossRef] [Green Version]
- Casetta, I.; Fainardi, E.; Saia, V.; Pracucci, G.; Padroni, M.; Renieri, L.; Nencini, P.; Inzitari, D.; Morosetti, D.; Sallustio, F.; et al. Endovascular Thrombectomy for Acute Ischemic Stroke Beyond 6 Hours from Onset: A Real-World Experience. Stroke 2020, 51, 2051–2057. [Google Scholar] [CrossRef]
- Muddasani, V.; de Havenon, A.; McNally, J.S.; Baradaran, H.; Alexander, M.D. MR Perfusion in the Evaluation of Mechanical Thrombectomy Candidacy. Top. Magn. Reson. Imaging 2021, 30, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Kamalian, S.; Lev, M.H. Stroke Imaging. Radiol. Clin. N. Am. 2019, 57, 717–732. [Google Scholar] [CrossRef] [PubMed]
- Atchaneeyasakul, K.; Shang, T.; Haussen, D.; Ortiz, G.; Yavagal, D. Impact of MRI Selection on Triage of Endovascular Therapy in Acute Ischemic Stroke: The MRI in Acute Management of Ischemic Stroke (MIAMIS) Registry. Interv. Neurol. 2020, 8, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Zang, N.; Lin, Z.; Huang, K.; Pan, Y.; Wu, Y.; Wu, Y.; Wang, S.; Wang, D.; Ji, Z.; Pan, S. Biomarkers of Unfavorable Outcome in Acute Ischemic Stroke Patients with Successful Recanalization by Endovascular Thrombectomy. Cerebrovasc. Dis. 2020, 49, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Makris, K.; Haliassos, A.; Chondrogianni, M.; Tsivgoulis, G. Blood biomarkers in ischemic stroke: Potential role and challenges in clinical practice and research. Crit. Rev. Clin. Lab. Sci. 2018, 55, 294–328. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, F.; Koenig, J.I.; Ayata, C.; Back, S.A.; Becker, K.; Broderick, J.P.; Carmichael, S.T.; Cho, S.; Cipolla, M.J.; Corbett, D.; et al. Translational Stroke Research: Vision and Opportunities. Stroke 2017, 48, 2632–2637. [Google Scholar] [CrossRef]
- McCabe, C.; Arroja, M.M.; Reid, E.; Macrae, I.M. Animal models of ischaemic stroke and characterisation of the ischaemic penumbra. Neuropharmacology 2018, 134, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Koizumi, J. Experimental studies of ischemic brain edema. I. A new experimental model of cerebral embolism in rats in which recirculation can be introduced in the ischemic area. Jpn. J. Stroke 1986, 8, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Longa, E.Z.; Weinstein, P.R.; Carlson, S.; Cummins, R. Reversible middle cerebral artery occlusion without craniectomy in rats. Stroke 1989, 20, 84–91. [Google Scholar] [CrossRef] [Green Version]
- Macrae, I.M. Preclinical stroke research—Advantages and disadvantages of the most common rodent models of focal ischaemia. Br. J. Pharmacol. 2011, 164, 1062–1078. [Google Scholar] [CrossRef] [Green Version]
- Fluri, F.; Schuhmann, M.K.; Kleinschnitz, C. Animal models of ischemic stroke and their application in clinical research. Drug Des. Dev. Ther. 2015, 9, 3445–3454. [Google Scholar] [CrossRef] [Green Version]
- Howells, D.W.; Porritt, M.J.; Rewell, S.S.; O’Collins, V.; Sena, E.S.; van der Worp, H.B.; Traystman, R.J.; Macleod, M.R. Different strokes for different folks: The rich diversity of animal models of focal cerebral ischemia. J. Cereb. Blood Flow Metab. 2010, 30, 1412–1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carmichael, S.T. Rodent models of focal stroke: Size, mechanism, and purpose. NeuroRx 2005, 2, 396–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCabe, C.; Gallagher, L.; Gsell, W.; Graham, D.; Dominiczak, A.F.; Macrae, I.M. Differences in the evolution of the ischemic penumbra in stroke-prone spontaneously hypertensive and Wistar-Kyoto rats. Stroke 2009, 40, 3864–3868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, X.; Fisher, M.; Shen, Q.; Sotak, C.H.; Duong, T.Q. Characterizing the diffusion/perfusion mismatch in experimental focal cerebral ischemia. Ann. Neurol. 2004, 55, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Shen, Q.; Meng, X.; Fisher, M.; Sotak, C.H.; Duong, T.Q. Pixel-by-pixel spatiotemporal progression of focal ischemia derived using quantitative perfusion and diffusion imaging. J. Cereb. Blood Flow Metab. 2003, 23, 1479–1488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henninger, N.; Bouley, J.; Nelligan, J.M.; Sicard, K.M.; Fisher, M. Normobaric hyperoxia delays perfusion/diffusion mismatch evolution, reduces infarct volume, and differentially affects neuronal cell death pathways after suture middle cerebral artery occlusion in rats. J. Cereb. Blood Flow Metab. 2007, 27, 1632–1642. [Google Scholar] [CrossRef]
- Henninger, N.; Fisher, M. Stimulating circle of Willis nerve fibers preserves the diffusion-perfusion mismatch in experimental stroke. Stroke 2007, 38, 2779–2786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaller, B.; Graf, R. Cerebral ischemia and reperfusion: The pathophysiologic concept as a basis for clinical therapy. J. Cereb. Blood Flow Metab. 2004, 24, 351–371. [Google Scholar] [CrossRef] [Green Version]
- Wardlaw, J.M.; Murray, V.; Berge, E.; del Zoppo, G.; Sandercock, P.; Lindley, R.L.; Cohen, G. Recombinant tissue plasminogen activator for acute ischaemic stroke: An updated systematic review and meta-analysis. Lancet 2012, 379, 2364–2372. [Google Scholar] [CrossRef] [Green Version]
- Hossmann, K.A. The two pathophysiologies of focal brain ischemia: Implications for translational stroke research. J. Cereb. Blood Flow Metab. 2012, 32, 1310–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutherland, B.A.; Neuhaus, A.A.; Couch, Y.; Balami, J.S.; DeLuca, G.C.; Hadley, G.; Harris, S.L.; Grey, A.N.; Buchan, A.M. The transient intraluminal filament middle cerebral artery occlusion model as a model of endovascular thrombectomy in stroke. J. Cereb. Blood Flow Metab. 2016, 36, 363–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aronowski, J.; Strong, R.; Grotta, J.C. Reperfusion injury: Demonstration of brain damage produced by reperfusion after transient focal ischemia in rats. J. Cereb. Blood Flow Metab. 1997, 17, 1048–1056. [Google Scholar] [CrossRef]
- Nagel, S.; Su, Y.; Horstmann, S.; Heiland, S.; Gardner, H.; Koziol, J.; Martinez-Torres, F.J.; Wagner, S. Minocycline and hypothermia for reperfusion injury after focal cerebral ischemia in the rat: Effects on BBB breakdown and MMP expression in the acute and subacute phase. Brain Res. 2008, 1188, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.W.; Zhang, Y.Y.; Su, J.; Liu, A.F.; Wang, K.; Li, C.; Liu, Y.E.; Zhang, Y.Q.; Lv, J.; Jiang, W.J. Ischemia Reperfusion Injury after Gradual versus Rapid Flow Restoration for Middle Cerebral Artery Occlusion Rats. Sci. Rep. 2018, 8, 1638. [Google Scholar] [CrossRef] [Green Version]
- Sharkey, J.; Ritchie, I.M.; Kelly, P.A. Perivascular microapplication of endothelin-1: A new model of focal cerebral ischaemia in the rat. J. Cereb. Blood Flow Metab. 1993, 13, 865–871. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, M.J.; Clemens, J.A. Rodent models of focal cerebral ischemia. Curr. Protoc. Neurosci. 2001, 12, 32. [Google Scholar] [CrossRef]
- Mecca, A.P.; O’Connor, T.E.; Katovich, M.J.; Sumners, C. Candesartan pretreatment is cerebroprotective in a rat model of endothelin-1-induced middle cerebral artery occlusion. Exp. Physiol. 2009, 94, 937–946. [Google Scholar] [CrossRef] [Green Version]
- Braeuninger, S.; Kleinschnitz, C. Rodent models of focal cerebral ischemia: Procedural pitfalls and translational problems. Exp Transl. Stroke Med. 2009, 1, 8. [Google Scholar] [CrossRef] [Green Version]
- Olsen, T.S.; Lassen, N.A. A dynamic concept of middle cerebral artery occlusion and cerebral infarction in the acute state based on interpreting severe hyperemia as a sign of embolic migration. Stroke 1984, 15, 458–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomsick, T.A. Intravenous thrombolysis for acute ischemic stroke. J. Vasc. Interv. Radiol. 2004, 15, S67–S76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietrich, W.D.; Watson, B.D.; Busto, R.; Ginsberg, M.D.; Bethea, J.R. Photochemically induced cerebral infarction. I. Early microvascular alterations. Acta Neuropathol. 1987, 72, 315–325. [Google Scholar] [CrossRef]
- Qian, C.; Li, P.C.; Jiao, Y.; Yao, H.H.; Chen, Y.C.; Yang, J.; Ding, J.; Yang, X.Y.; Teng, G.J. Precise Characterization of the Penumbra Revealed by MRI: A Modified Photothrombotic Stroke Model Study. PLoS ONE 2016, 11, e0153756. [Google Scholar] [CrossRef] [PubMed]
- Schroeter, M.; Jander, S.; Stoll, G. Non-invasive induction of focal cerebral ischemia in mice by photothrombosis of cortical microvessels: Characterization of inflammatory responses. J. Neurosci. Methods 2002, 117, 43–49. [Google Scholar] [CrossRef]
- Yao, H.; Sugimori, H.; Fukuda, K.; Takada, J.; Ooboshi, H.; Kitazono, T.; Ibayashi, S.; Iida, M. Photothrombotic middle cerebral artery occlusion and reperfusion laser system in spontaneously hypertensive rats. Stroke 2003, 34, 2716–2721. [Google Scholar] [CrossRef]
- Watson, B.D.; Prado, R.; Veloso, A.; Brunschwig, J.P.; Dietrich, W.D. Cerebral blood flow restoration and reperfusion injury after ultraviolet laser-facilitated middle cerebral artery recanalization in rat thrombotic stroke. Stroke 2002, 33, 428–434. [Google Scholar] [CrossRef] [Green Version]
- Kleim, J.A.; Boychuk, J.A.; Adkins, D.L. Rat models of upper extremity impairment in stroke. ILAR J. 2007, 48, 374–384. [Google Scholar] [CrossRef] [Green Version]
- Lerman, L.O.; Kurtz, T.W.; Touyz, R.M.; Ellison, D.H.; Chade, A.R.; Crowley, S.D.; Mattson, D.L.; Mullins, J.J.; Osborn, J.; Eirin, A.; et al. Animal Models of Hypertension: A Scientific Statement From the American Heart Association. Hypertension 2019, 73, e87–e120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Candelario-Jalil, E.; Paul, S. Impact of aging and comorbidities on ischemic stroke outcomes in preclinical animal models: A translational perspective. Exp. Neurol. 2021, 335, 113494. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.C.; Lucke-Wold, B.; Lucke-Wold, N.; Elliott, A.S.; Logsdon, A.F.; Rosen, C.L.; Huber, J.D. Neuroprotection for ischemic stroke: Moving past shortcomings and identifying promising directions. Int. J. Mol. Sci. 2013, 14, 1890–1917. [Google Scholar] [CrossRef] [PubMed]
- Bennion, D.M.; Isenberg, J.D.; Harmel, A.T.; DeMars, K.; Dang, A.N.; Jones, C.H.; Pignataro, M.E.; Graham, J.T.; Steckelings, U.M.; Alexander, J.C.; et al. Post-stroke angiotensin II type 2 receptor activation provides long-term neuroprotection in aged rats. PLoS ONE 2017, 12, e0180738. [Google Scholar] [CrossRef] [Green Version]
- DeMars, K.M.; Yang, C.; Candelario-Jalil, E. Neuroprotective effects of targeting BET proteins for degradation with dBET1 in aged mice subjected to ischemic stroke. Neurochem. Int. 2019, 127, 94–102. [Google Scholar] [CrossRef]
- Yang, C.; DeMars, K.M.; Alexander, J.C.; Febo, M.; Candelario-Jalil, E. Sustained Neurological Recovery after Stroke in Aged Rats Treated with a Novel Prostacyclin Analog. Stroke 2017, 48, 1948–1956. [Google Scholar] [CrossRef]
- Yamakura, T.; Harris, R.A. Effects of gaseous anesthetics nitrous oxide and xenon on ligand-gated ion channels. Comparison with isoflurane and ethanol. Anesthesiology 2000, 93, 1095–1101. [Google Scholar] [CrossRef]
- Kotani, N.; Akaike, N. The effects of volatile anesthetics on synaptic and extrasynaptic GABA-induced neurotransmission. Brain Res. Bull. 2013, 93, 69–79. [Google Scholar] [CrossRef]
- Strebel, S.; Lam, A.M.; Matta, B.; Mayberg, T.S.; Aaslid, R.; Newell, D.W. Dynamic and static cerebral autoregulation during isoflurane, desflurane, and propofol anesthesia. Anesthesiology 1995, 83, 66–76. [Google Scholar] [CrossRef]
- Balbi, M.; Vanni, M.P.; Silasi, G.; Sekino, Y.; Bolanos, L.; LeDue, J.M.; Murphy, T.H. Targeted ischemic stroke induction and mesoscopic imaging assessment of blood flow and ischemic depolarization in awake mice. Neurophotonics 2017, 4, 035001. [Google Scholar] [CrossRef]
- Crapser, J.; Ritzel, R.; Verma, R.; Venna, V.R.; Liu, F.; Chauhan, A.; Koellhoffer, E.; Patel, A.; Ricker, A.; Maas, K.; et al. Ischemic stroke induces gut permeability and enhances bacterial translocation leading to sepsis in aged mice. Aging 2016, 8, 1049–1063. [Google Scholar] [CrossRef] [Green Version]
- McCann, S.K.; Lawrence, C.B. Comorbidity and age in the modelling of stroke: Are we still failing to consider the characteristics of stroke patients? BMJ Open Sci. 2020, 4, e100013. [Google Scholar] [CrossRef]
- Albertson, A.J.; Landsness, E.C.; Tang, M.J.; Yan, P.; Miao, H.; Rosenthal, Z.P.; Kim, B.; Culver, J.C.; Bauer, A.Q.; Lee, J.-M. Normal Aging in Mice is Associated with a Global Reduction in Cortical Spectral Power and Network-Specific Declines in Functional Connectivity. bioRxiv 2021. [Google Scholar] [CrossRef]
- Mostany, R.; Anstey, J.E.; Crump, K.L.; Maco, B.; Knott, G.; Portera-Cailliau, C. Altered synaptic dynamics during normal brain aging. J. Neurosci. 2013, 33, 4094–4104. [Google Scholar] [CrossRef] [PubMed]
- Dickstein, D.L.; Weaver, C.M.; Luebke, J.I.; Hof, P.R. Dendritic spine changes associated with normal aging. Neuroscience 2013, 251, 21–32. [Google Scholar] [CrossRef] [Green Version]
- Hermann, D.M.; Doeppner, T.R.; Popa-Wagner, A. Opportunities and Limitations of Vascular Risk Factor Models in Studying Plasticity-Promoting and Restorative Ischemic Stroke Therapies. Neural. Plast. 2019, 2019, 9785476. [Google Scholar] [CrossRef] [Green Version]
- Hermann, D.M.; Kleinschnitz, C. Modeling Vascular Risk Factors for the Development of Ischemic Stroke Therapies. Stroke 2019, 50, 1310–1317. [Google Scholar] [CrossRef]
- Hermann, D.M.; Popa-Wagner, A.; Kleinschnitz, C.; Doeppner, T.R. Animal models of ischemic stroke and their impact on drug discovery. Expert Opin. Drug Discov. 2019, 14, 315–326. [Google Scholar] [CrossRef]
- Dhande, I.S.; Kneedler, S.C.; Zhu, Y.; Joshi, A.S.; Hicks, M.J.; Wenderfer, S.E.; Braun, M.C.; Doris, P.A. Natural genetic variation in Stim1 creates stroke in the spontaneously hypertensive rat. Genes Immun. 2020, 21, 182–192. [Google Scholar] [CrossRef] [Green Version]
- Durukan, A.; Tatlisumak, T. Acute ischemic stroke: Overview of major experimental rodent models, pathophysiology, and therapy of focal cerebral ischemia. Pharmacol. Biochem. Behav. 2007, 87, 179–197. [Google Scholar] [CrossRef] [PubMed]
- Allegra Mascaro, A.L.; Conti, E.; Lai, S.; Di Giovanna, A.P.; Spalletti, C.; Alia, C.; Panarese, A.; Scaglione, A.; Sacconi, L.; Micera, S.; et al. Combined Rehabilitation Promotes the Recovery of Structural and Functional Features of Healthy Neuronal Networks after Stroke. Cell Rep. 2019, 28, 3474–3485.e6. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Yamaguchi, M.; Zhou, C.; Calvert, J.W.; Tang, J.; Zhang, J.H. Neurovascular protection reduces early brain injury after subarachnoid hemorrhage. Stroke 2004, 35, 2412–2417. [Google Scholar] [CrossRef] [Green Version]
- Stoll, G.; Kleinschnitz, C.; Meuth, S.G.; Braeuninger, S.; Ip, C.W.; Wessig, C.; Nolte, I.; Bendszus, M. Transient widespread blood-brain barrier alterations after cerebral photothrombosis as revealed by gadofluorine M-enhanced magnetic resonance imaging. J. Cereb. Blood Flow Metab. 2009, 29, 331–341. [Google Scholar] [CrossRef]
- Weise, G.; Stoll, G. Magnetic resonance imaging of blood brain/nerve barrier dysfunction and leukocyte infiltration: Closely related or discordant? Front. Neurol. 2012, 3, 178. [Google Scholar] [CrossRef] [Green Version]
- Xiong, Y.; Zhu, W.Z.; Zhang, Q.; Wang, W. Observation of post-MCAO cortical inflammatory edema in rats by 7.0 Tesla MRI. J. Huazhong Univ. Sci. Technol. Med. Sci. 2014, 34, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Nhan, T.; Burgess, A.; Cho, E.E.; Stefanovic, B.; Lilge, L.; Hynynen, K. Drug delivery to the brain by focused ultrasound induced blood-brain barrier disruption: Quantitative evaluation of enhanced permeability of cerebral vasculature using two-photon microscopy. J. Control Release 2013, 172, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.Q.; Suzuki, Y.; Kondo, K.; Kawano, K.; Ikeda, Y.; Umemura, K. A novel MCA occlusion model of photothrombotic ischemia with cyclic flow reductions: Development of cerebral hemorrhage induced by heparin. Brain Res. Brain Res. Protoc. 2002, 9, 85–92. [Google Scholar] [CrossRef]
- Choi, K.H.; Kim, H.S.; Park, M.S.; Kim, J.T.; Kim, J.H.; Cho, K.A.; Lee, M.C.; Lee, H.J.; Cho, K.H. Regulation of Caveolin-1 Expression Determines Early Brain Edema after Experimental Focal Cerebral Ischemia. Stroke 2016, 47, 1336–1343. [Google Scholar] [CrossRef] [Green Version]
- Choi, K.H.; Kim, H.S.; Park, M.S.; Lee, E.B.; Lee, J.K.; Kim, J.T.; Kim, J.H.; Lee, M.C.; Lee, H.J.; Cho, K.H. Overexpression of caveolin-1 attenuates brain edema by inhibiting tight junction degradation. Oncotarget 2016, 7, 67857–67867. [Google Scholar] [CrossRef] [Green Version]
- Kubotera, H.; Ikeshima-Kataoka, H.; Hatashita, Y.; Allegra Mascaro, A.L.; Pavone, F.S.; Inoue, T. Astrocytic endfeet re-cover blood vessels after removal by laser ablation. Sci. Rep. 2019, 9, 1263. [Google Scholar] [CrossRef] [Green Version]
- Knight, R.A.; Han, Y.; Nagaraja, T.N.; Whitton, P.; Ding, J.; Chopp, M.; Seyfried, D.M. Temporal MRI assessment of intracerebral hemorrhage in rats. Stroke 2008, 39, 2596–2602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsushita, H.; Hijioka, M.; Hisatsune, A.; Isohama, Y.; Iwamoto, S.; Terasawa, H.; Katsuki, H. MRI-based analysis of intracerebral hemorrhage in mice reveals relationship between hematoma expansion and the severity of symptoms. PLoS ONE 2013, 8, e67691. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, C.L.; Szu, J.I.; Eberle, M.M.; Wang, Y.; Hsu, M.S.; Binder, D.K.; Park, B.H. Decreased light attenuation in cerebral cortex during cerebral edema detected using optical coherence tomography. Neurophotonics 2014, 1, 025004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimoto, J.G. Optical coherence tomography for ultrahigh resolution in vivo imaging. Nat. Biotechnol. 2003, 21, 1361–1367. [Google Scholar] [CrossRef]
- Raymond, S.B.; Skoch, J.; Hynynen, K.; Bacskai, B.J. Multiphoton imaging of ultrasound/Optison mediated cerebrovascular effects in vivo. J. Cereb. Blood Flow Metab. 2007, 27, 393–403. [Google Scholar] [CrossRef] [Green Version]
- Raymond, S.B.; Skoch, J.; Bacskai, B.J.; Hynynen, K. Modular design for in vivo optical imaging and ultrasound treatment in the murine brain. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2007, 54, 431–434. [Google Scholar] [CrossRef]
- Denk, W.; Svoboda, K. Photon upmanship: Why multiphoton imaging is more than a gimmick. Neuron 1997, 18, 351–357. [Google Scholar] [CrossRef] [Green Version]
- Feng, G.; Mellor, R.H.; Bernstein, M.; Keller-Peck, C.; Nguyen, Q.T.; Wallace, M.; Nerbonne, J.M.; Lichtman, J.W.; Sanes, J.R. Imaging neuronal subsets in transgenic mice expressing multiple spectral variants of GFP. Neuron 2000, 28, 41–51. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Boyd, J.; Delaney, K.; Murphy, T.H. Rapid reversible changes in dendritic spine structure in vivo gated by the degree of ischemia. J. Neurosci. 2005, 25, 5333–5338. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Murphy, T.H. Imaging the impact of cortical microcirculation on synaptic structure and sensory-evoked hemodynamic responses in vivo. PLoS Biol. 2007, 5, e119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, T.H.; Li, P.; Betts, K.; Liu, R. Two-photon imaging of stroke onset in vivo reveals that NMDA-receptor independent ischemic depolarization is the major cause of rapid reversible damage to dendrites and spines. J. Neurosci. 2008, 28, 1756–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conti, E.; Scaglione, A.; de Vito, G.; Calugi, F.; Pasquini, M.; Pizzorusso, T.; Micera, S.; Allegra Mascaro, A.L.; Pavone, F.S. Combining Optogenetic Stimulation and Motor Training Improves Functional Recovery and Perilesional Cortical Activity. Neurorehabil. Neural Repair 2021. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Murphy, T.H. Two-photon imaging during prolonged middle cerebral artery occlusion in mice reveals recovery of dendritic structure after reperfusion. J. Neurosci. 2008, 28, 11970–11979. [Google Scholar] [CrossRef]
- Brown, C.E.; Li, P.; Boyd, J.D.; Delaney, K.R.; Murphy, T.H. Extensive turnover of dendritic spines and vascular remodeling in cortical tissues recovering from stroke. J. Neurosci. 2007, 27, 4101–4109. [Google Scholar] [CrossRef] [Green Version]
- Allegra Mascaro, A.L.; Sacconi, L.; Pavone, F.S. Multi-photon nanosurgery in live brain. Front. Neuroenerg. 2010, 2, 21. [Google Scholar] [CrossRef] [PubMed]
- Harrison, T.C.; Silasi, G.; Boyd, J.D.; Murphy, T.H. Displacement of sensory maps and disorganization of motor cortex after targeted stroke in mice. Stroke 2013, 44, 2300–2306. [Google Scholar] [CrossRef] [Green Version]
- Lim, D.H.; LeDue, J.M.; Mohajerani, M.H.; Murphy, T.H. Optogenetic mapping after stroke reveals network-wide scaling of functional connections and heterogeneous recovery of the peri-infarct. J. Neurosci. 2014, 34, 16455–16466. [Google Scholar] [CrossRef] [Green Version]
- Siegel, J.S.; Ramsey, L.E.; Snyder, A.Z.; Metcalf, N.V.; Chacko, R.V.; Weinberger, K.; Baldassarre, A.; Hacker, C.D.; Shulman, G.L.; Corbetta, M. Disruptions of network connectivity predict impairment in multiple behavioral domains after stroke. Proc. Natl. Acad. Sci. USA 2016, 113, E4367–E4376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginsberg, M.D. Expanding the concept of neuroprotection for acute ischemic stroke: The pivotal roles of reperfusion and the collateral circulation. Prog. Neurobiol. 2016, 145–146, 46–77. [Google Scholar] [CrossRef]
- Smajlovic, D. Strokes in young adults: Epidemiology and prevention. Vasc. Health Risk Manag. 2015, 11, 157–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marini, C.; Russo, T.; Felzani, G. Incidence of stroke in young adults: A review. Stroke Res. Treat. 2010, 2011, 535672. [Google Scholar] [CrossRef] [Green Version]
- Yemisci, M.; Eikermann-Haerter, K. Aura and Stroke: Relationship and what we have learnt from preclinical models. J. Headache Pain 2019, 20, 63. [Google Scholar] [CrossRef]
- Dreier, J.P.; Lemale, C.L.; Kola, V.; Friedman, A.; Schoknecht, K. Spreading depolarization is not an epiphenomenon but the principal mechanism of the cytotoxic edema in various gray matter structures of the brain during stroke. Neuropharmacology 2018, 134, 189–207. [Google Scholar] [CrossRef] [PubMed]
- Lindemann, J.; Rakers, C.; Matuskova, H.; Simon, B.J.; Kinfe, T.; Petzold, G.C. Vagus nerve stimulation reduces spreading depolarization burden and cortical infarct volume in a rat model of stroke. PLoS ONE 2020, 15, e0236444. [Google Scholar] [CrossRef] [PubMed]
- Hartings, J.A. Spreading depolarization monitoring in neurocritical care of acute brain injury. Curr. Opin. Crit. Care 2017, 23, 94–102. [Google Scholar] [CrossRef]
- Gorji, A. Spreading depression: A review of the clinical relevance. Brain Res. Brain Res. Rev. 2001, 38, 33–60. [Google Scholar] [CrossRef]
- Nedergaard, M.; Astrup, J. Infarct rim: Effect of hyperglycemia on direct current potential and [14C]2-deoxyglucose phosphorylation. J. Cereb. Blood Flow Metab. 1986, 6, 607–615. [Google Scholar] [CrossRef] [Green Version]
- Siesjo, B.K.; Bengtsson, F. Calcium fluxes, calcium antagonists, and calcium-related pathology in brain ischemia, hypoglycemia, and spreading depression: A unifying hypothesis. J. Cereb. Blood Flow Metab. 1989, 9, 127–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somjen, G.G.; Aitken, P.G.; Balestrino, M.; Herreras, O.; Kawasaki, K. Spreading depression-like depolarization and selective vulnerability of neurons. A brief review. Stroke 1990, 21, III179–III183. [Google Scholar]
- Takano, T.; Tian, G.F.; Peng, W.; Lou, N.; Lovatt, D.; Hansen, A.J.; Kasischke, K.A.; Nedergaard, M. Cortical spreading depression causes and coincides with tissue hypoxia. Nat. Neurosci. 2007, 10, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Dreier, J.P.; Korner, K.; Ebert, N.; Gorner, A.; Rubin, I.; Back, T.; Lindauer, U.; Wolf, T.; Villringer, A.; Einhaupl, K.M.; et al. Nitric oxide scavenging by hemoglobin or nitric oxide synthase inhibition by N-nitro-L-arginine induces cortical spreading ischemia when K+ is increased in the subarachnoid space. J. Cereb. Blood Flow Metab. 1998, 18, 978–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, H.T.; Tuohy, M.C.; Chow, D.; Kozberg, M.G.; Kim, S.H.; Shaik, M.A.; Hillman, E.M.C. Neurovascular dynamics of repeated cortical spreading depolarizations after acute brain injury. Cell Rep. 2021, 37, 109794. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conti, E.; Piccardi, B.; Sodero, A.; Tudisco, L.; Lombardo, I.; Fainardi, E.; Nencini, P.; Sarti, C.; Allegra Mascaro, A.L.; Baldereschi, M. Translational Stroke Research Review: Using the Mouse to Model Human Futile Recanalization and Reperfusion Injury in Ischemic Brain Tissue. Cells 2021, 10, 3308. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10123308
Conti E, Piccardi B, Sodero A, Tudisco L, Lombardo I, Fainardi E, Nencini P, Sarti C, Allegra Mascaro AL, Baldereschi M. Translational Stroke Research Review: Using the Mouse to Model Human Futile Recanalization and Reperfusion Injury in Ischemic Brain Tissue. Cells. 2021; 10(12):3308. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10123308
Chicago/Turabian StyleConti, Emilia, Benedetta Piccardi, Alessandro Sodero, Laura Tudisco, Ivano Lombardo, Enrico Fainardi, Patrizia Nencini, Cristina Sarti, Anna Letizia Allegra Mascaro, and Marzia Baldereschi. 2021. "Translational Stroke Research Review: Using the Mouse to Model Human Futile Recanalization and Reperfusion Injury in Ischemic Brain Tissue" Cells 10, no. 12: 3308. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10123308