
Molecular and Dynamic Evaluation of Proteins Related to Resistance to Neoadjuvant Treatment with Chemoradiotherapy in Circulating Tumor Cells of Patients with Locally Advanced Rectal Cancer

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
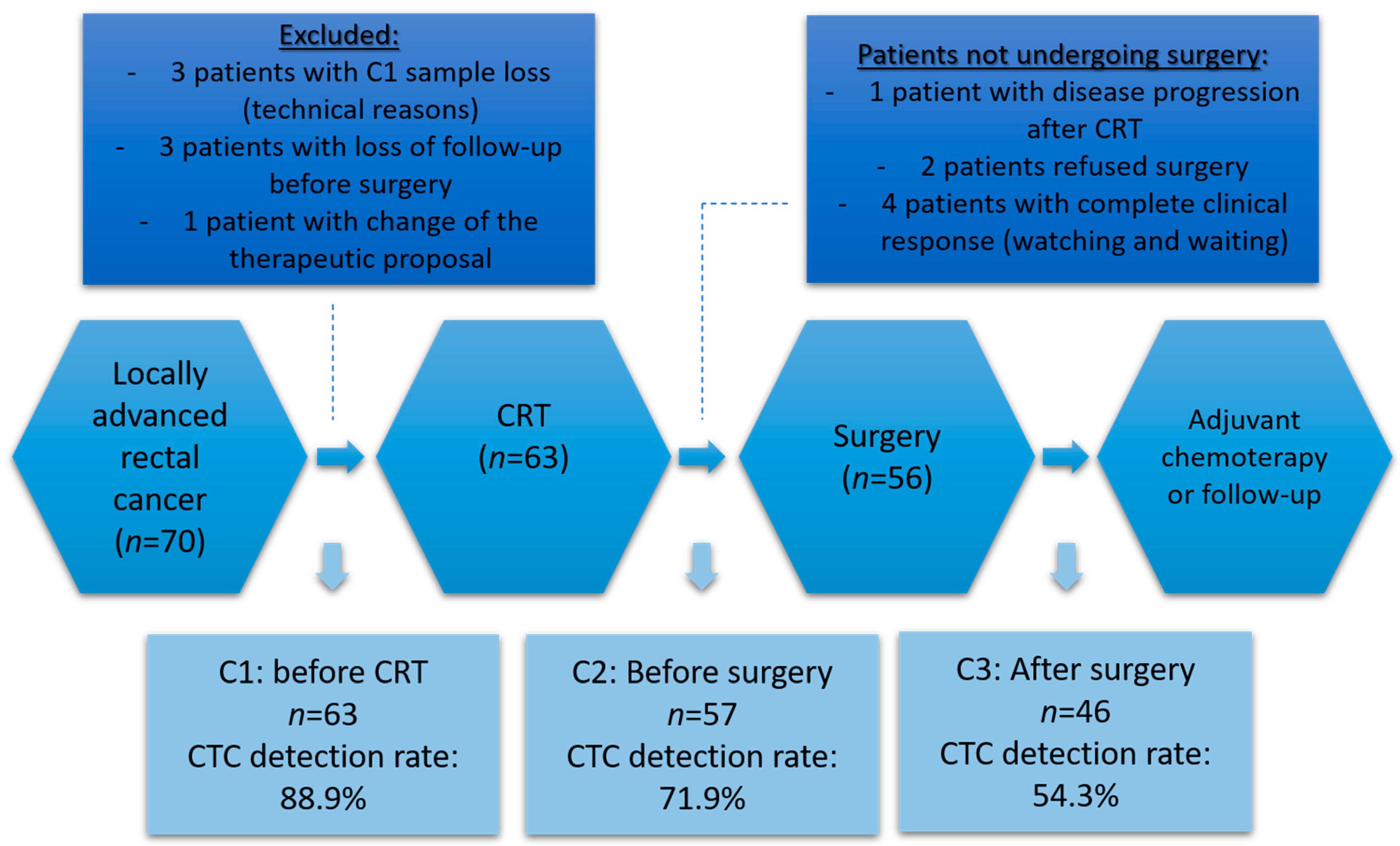
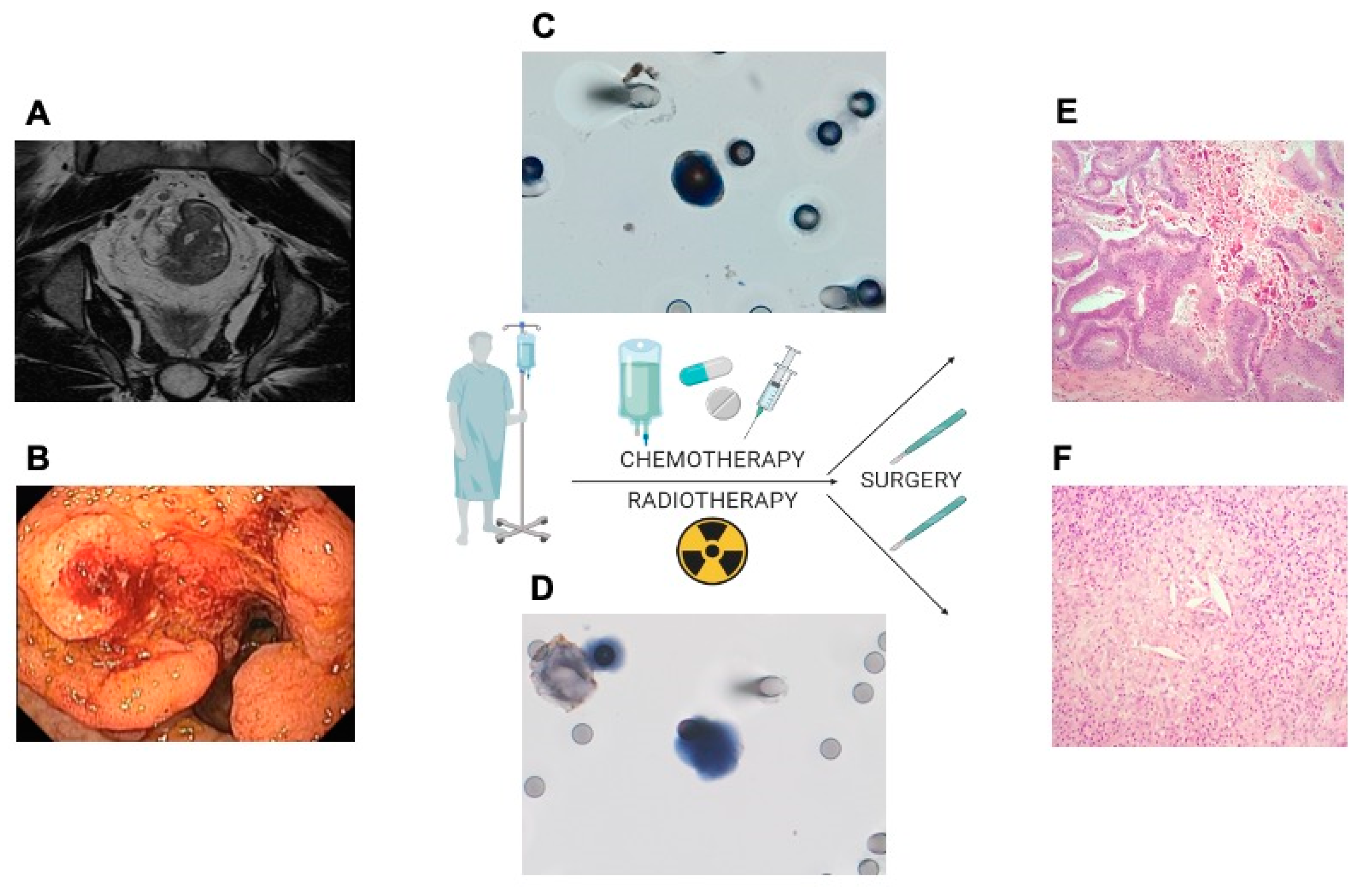
2.1. Patient Population and Study Design
2.2. Treatment
2.3. Ethics
2.4. Statistical Analysis
2.5. Assessment of Preoperative Clinical Response
2.6. Assessment of Pathological Response
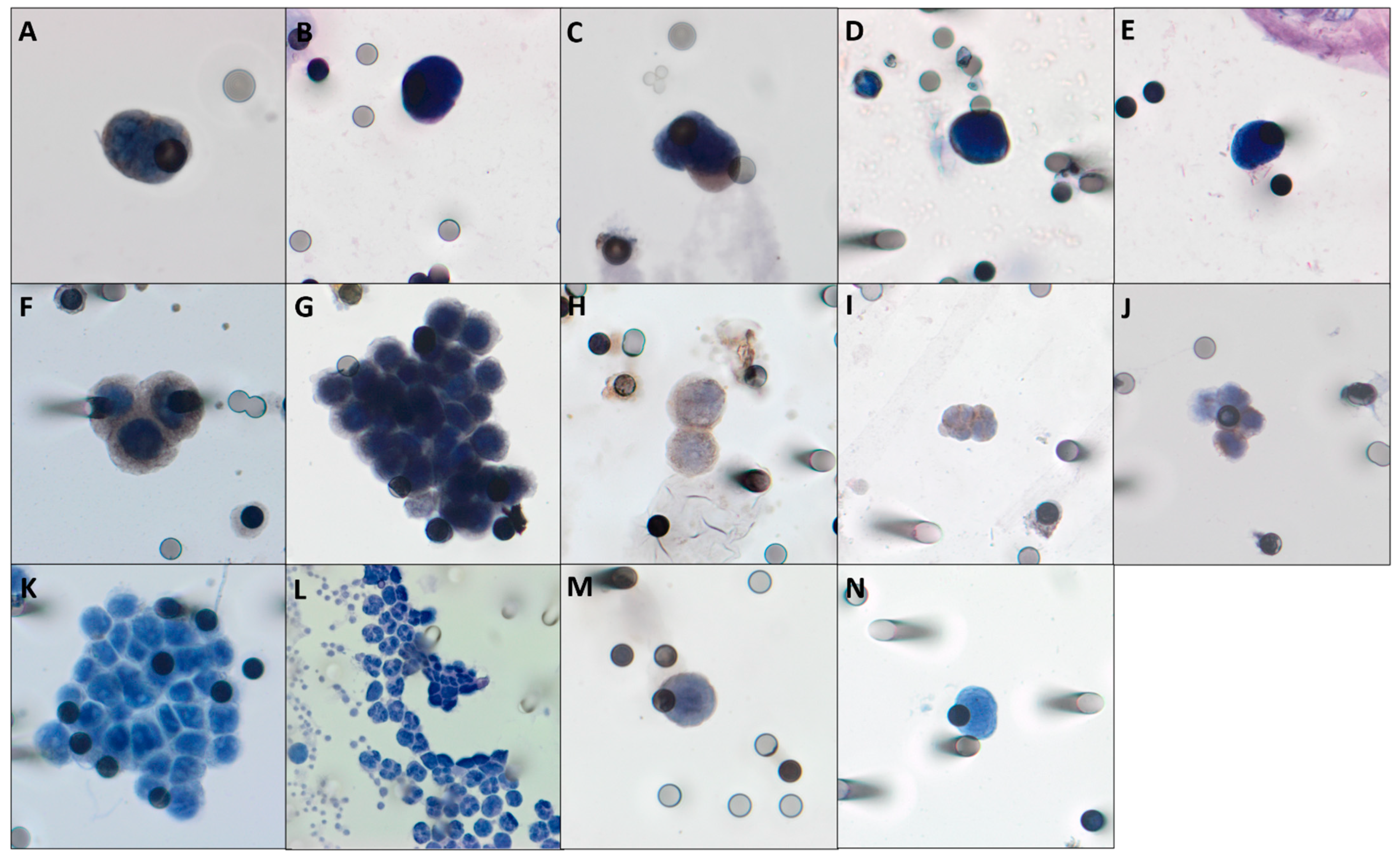
2.7. Isolation, Quantification and Protein Expression Analysis of CTCs
2.8. Survival Outcomes
2.9. Prognosis Evaluation
3. Results
3.1. Demographic and Clinical Variables
3.2. CTCs Count
3.3. Protein Expression in CTCs
3.4. Correlation between Clinical Characteristics, CTCs Kinetics and Protein Expression in CTCs with Pathological Response
3.4.1. Clinical Characteristics
3.4.2. CTCs Kinetics
3.4.3. RAD23B and TYMS Expression
3.5. Correlation between CTCs Kinetics and Protein Expression in CTCs with DFS and OS
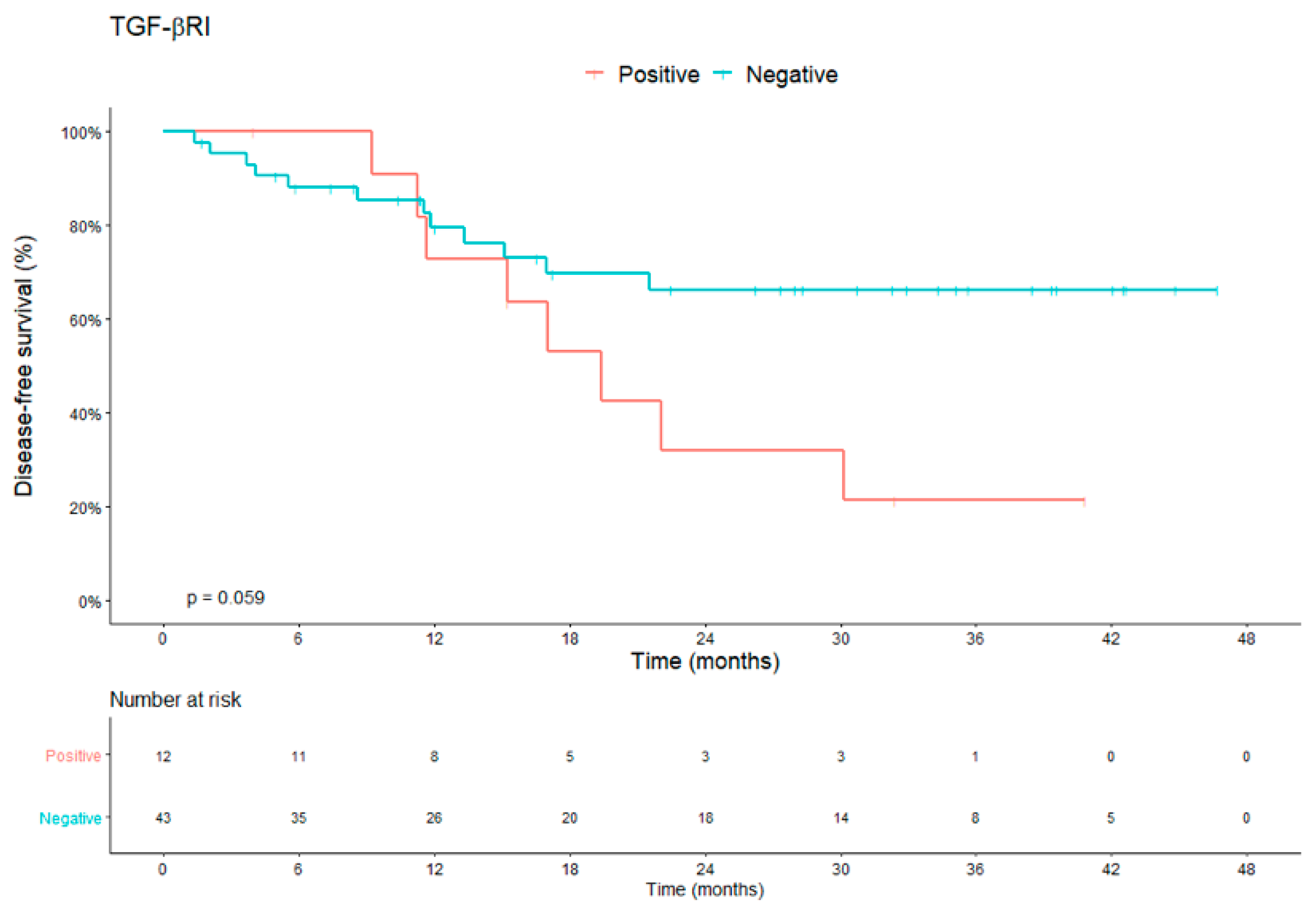
3.6. Protein Expression in CTCs x DFS and OS
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller Mph, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [Green Version]
- Feeney, G.; Sehgal, R.; Sheehan, M.; Hogan, A.; Regan, M.; Joyce, M.; Kerin, M. Neoadjuvant radiotherapy for rectal cancer management. World J. Gastroenterol. 2019, 25, 4850–4869. [Google Scholar] [CrossRef] [PubMed]
- James, D.B.; Mary, K.; Gospodarowicz, C.W. TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2016. [Google Scholar]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rodel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus Postoperative Chemoradiotherapy for Rectal Cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saklani, A.; Pandey, D.; Patel, S. RAPIDO protocol: A promising approach for high-risk locally advanced rectal cancers. Lancet Oncol. 2021, 22, 2–3. [Google Scholar] [CrossRef]
- Franke, A.J.; Parekh, H.; Starr, J.S.; Tan, S.A.; Iqbal, A.; George, T.J. Total Neoadjuvant Therapy: A Shifting Paradigm in Locally Advanced Rectal Cancer Management. Clin. Color. Cancer 2018, 17, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahadoer, R.R.; Dijkstra, E.A.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.-K.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 29–42. [Google Scholar] [CrossRef]
- Conroy, T.; Bosset, J.-F.; Etienne, P.-L.; Rio, E.; François, É.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouché, O.; Gargot, D.; et al. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 702–715. [Google Scholar] [CrossRef]
- Habr-Gama, A.; Julião, G.P.S.; Perez, R.O. Nonoperative Management of Rectal Cancer. Hematol. Clin. N. Am. 2015, 29, 135–151. [Google Scholar] [CrossRef]
- Sun, W.; Al-Rajabi, R.; Perez, R.O.; Abbasi, S.; Ash, R.; Habr-Gama, A. Controversies in Rectal Cancer Treatment and Management. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, 136–146. [Google Scholar] [CrossRef]
- Ryan, É.J.; Creavin, B.; Sheahan, K. Delivery of Personalized Care for Locally Advanced Rectal Cancer: Incorporating Pathological, Molecular Genetic, and Immunological Biomarkers Into the Multimodal Paradigm. Front. Oncol. 2020, 10, 1369. [Google Scholar] [CrossRef]
- Molinari, C.; Matteucci, F.; Caroli, P.; Passardi, A. Biomarkers and Molecular Imaging as Predictors of Response to Neoadjuvant Chemoradiotherapy in Patients With Locally Advanced Rectal Cancer. Clin. Color. Cancer 2015, 14, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Alix-Panabières, C.; Pantel, K. Liquid Biopsy: From Discovery to Clinical Application. Cancer Discov. 2021, 11, 858–873. [Google Scholar] [CrossRef] [PubMed]
- Heidrich, I.; Ačkar, L.; Mohammadi, P.M.; Pantel, K. Liquid biopsies: Potential and challenges. Int. J. Cancer 2021, 148, 528–545. [Google Scholar] [CrossRef]
- Massihnia, D.; Pizzutilo, E.G.; Amatu, A.; Tosi, F.M.; Ghezzi, S.; Bencardino, K.; Di Masi, P.; Righetti, E.; Patelli, G.; Scaglione, F.; et al. Liquid biopsy for rectal cancer: A systematic review. Cancer Treat. Rev. 2019, 79, 101893. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Li, G.; Wan, J.; Zhu, J.; Shen, W.; Zhang, Z. Circulating tumor cells: A promising marker of predicting tumor response in rectal cancer patients receiving neoadjuvant chemo-radiation therapy. Oncotarget 2016, 7, 69507–69517. [Google Scholar] [CrossRef] [Green Version]
- Flores, B.T.; E Silva, V.S.; Abdallah, E.A.; Mello, C.A.; Silva, M.L.G.; Mendes, G.G.; Braun, A.C.; Junior, S.A.; Chinen, L.T.D. Molecular and Kinetic Analyses of Circulating Tumor Cells as Predictive Markers of Treatment Response in Locally Advanced Rectal Cancer Patients. Cells 2019, 8, 641. [Google Scholar] [CrossRef] [Green Version]
- Aguiar, S.; Lopes, A.; Soares, F.A.; Rossi, M.; Ferreira, F.; Nakagawa, W.; Carvalho, A.; Filho, W. Prognostic and predictive value of the thymidylate synthase expression in patients with non-metastatic colorectal cancer. Eur. J. Surg. Oncol. 2005, 31, 863–868. [Google Scholar] [CrossRef]
- Formentini, A.; Henne-Bruns, D.; Kornmann, M. Thymidylate synthase expression and prognosis of patients with gastrointestinal cancers receiving adjuvant chemotherapy: A review. Langenbeck’s Arch. Surg. 2004, 389, 405–413. [Google Scholar] [CrossRef]
- Bottarelli, L.; De’ Angelis, G.L.; Azzoni, C.; Di Mario, F.; De’ Angelis, N.; Leandro, G.; Fornaroli, F.; Gaiani, F.; Negri, F. Potential Predictive Biomarkers in Locally Advanced Rectal Cancer Treated with Preoperative Chemo-Radiotherapy. Acta Biomed. 2018, 89, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Kuremsky, J.G.; Tepper, J.E.; McLeod, H.L. Biomarkers for Response to Neoadjuvant Chemoradiation for Rectal Cancer. Int. J. Radiat. Oncol. 2009, 74, 673–688. [Google Scholar] [CrossRef]
- Shen, Y.N.; Bae, I.-S.; Park, G.H.; Choi, H.S.; Lee, K.-H.; Kim, S.H. MicroRNA-196b enhances the radiosensitivity of SNU-638 gastric cancer cells by targeting RAD23B. Biomed. Pharmacother. 2018, 105, 362–369. [Google Scholar] [CrossRef]
- Dantuma, N.P.; Heinen, C.; Hoogstraten, D. The ubiquitin receptor Rad23: At the crossroads of nucleotide excision repair and proteasomal degradation. DNA Repair 2009, 8, 449–460. [Google Scholar] [CrossRef]
- Abbasi, R.; Ramroth, H.; Becher, H.; Dietz, A.; Schmezer, P.; Popanda, O. Laryngeal cancer risk associated with smoking and alcohol consumption is modified by genetic polymorphisms inERCC5,ERCC6andRAD23Bbut not by polymorphisms in five other nucleotide excision repair genes. Int. J. Cancer 2009, 125, 1431–1439. [Google Scholar] [CrossRef]
- Corrò, C.; Dutoit, V.; Koessler, T. Emerging Trends for Radio-Immunotherapy in Rectal Cancer. Cancers 2021, 13, 1374. [Google Scholar] [CrossRef]
- Boustani, J.; Derangère, V.; Bertaut, A.; Adotevi, O.; Morgand, V.; Charon-Barra, C.; Ghiringhelli, F.; Mirjolet, C. Radiotherapy Scheme Effect on PD-L1 Expression for Locally Advanced Rectal Cancer. Cells 2020, 9, 2071. [Google Scholar] [CrossRef]
- Richter, I.; Jirasek, T.; Dvorak, J.; Cermakova, E.; Rehakova, P.; Bartos, J. The prognostic effect of neoadjuvant chemoradiotherapy on the change of PD-L1 expression in patients with locally advanced rectal adenocarcinoma. J. BUON 2017, 22, 875–881. [Google Scholar]
- Hecht, M.; Büttner-Herold, M.; Erlenbach-Wünsch, K.; Haderlein, M.; Croner, R.; Grützmann, R.; Hartmann, A.; Fietkau, R.; Distel, L.V. PD-L1 is upregulated by radiochemotherapy in rectal adenocarcinoma patients and associated with a favourable prognosis. Eur. J. Cancer 2016, 65, 52–60. [Google Scholar] [CrossRef]
- Huemer, F.; Klieser, E.; Neureiter, D.; Schlintl, V.; Rinnerthaler, G.; Pagès, F.; Kirilovsky, A.; El Sissy, C.; Iglseder, W.; Singhartinger, F.; et al. Impact of PD-L1 Scores and Changes on Clinical Outcome in Rectal Cancer Patients Undergoing Neoadjuvant Chemoradiotherapy. J. Clin. Med. 2020, 9, 2775. [Google Scholar] [CrossRef]
- Angenete, E.; Langenskiöld, M.; Palmgren, I.; Falk, P.; Öresland, T.; Ivarsson, M.-L. Transforming growth factor beta-1 in rectal tumour, mucosa and plasma in relation to radiotherapy and clinical outcome in rectal cancer patients. Int. J. Color. Dis. 2007, 22, 1331–1338. [Google Scholar] [CrossRef]
- Ryan, R.; Gibbons, D.; Hyland, J.M.P.; Treanor, D.; White, A.; Mulcahy, H.E.; O’Donoghue, D.P.; Moriarty, M.; Fennelly, D.; Sheahan, K. Pathological response following long-course neoadjuvant chemoradiotherapy for locally advanced rectal cancer. Histopathology 2005, 47, 141–146. [Google Scholar] [CrossRef]
- Mace, A.G.; Pai, R.K.; Stocchi, L.; Kalady, M.F. American Joint Committee on Cancer and College of American Pathologists Regression Grade. Dis. Colon Rectum 2015, 58, 32–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebs, M.; Hou, J.-M.; Sloane, R.S.; Lancashire, L.; Priest, L.; Nonaka, D.; Ward, T.H.; Backen, A.; Clack, G.; Hughes, A.; et al. Analysis of Circulating Tumor Cells in Patients with Non-small Cell Lung Cancer Using Epithelial Marker-Dependent and -Independent Approaches. J. Thorac. Oncol. 2012, 7, 306–315. [Google Scholar] [CrossRef] [Green Version]
- Khoja, L.; Backen, A.; Sloane, R.S.; Menasce, L.; Ryder, D.; Krebs, M.; Board, R.; Clack, G.; Hughes, A.; Blackhall, F.; et al. A pilot study to explore circulating tumour cells in pancreatic cancer as a novel biomarker. Br. J. Cancer 2011, 106, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.T.; Heneghan, H.; Winter, D.C. Systematic review and meta-analysis of outcomes following pathological complete response to neoadjuvant chemoradiotherapy for rectal cancer. Br. J. Surg. 2012, 99, 918–928. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.E.; Warrier, S.K.; Lynch, A.C.; Heriot, A.G. Assessing pathological complete response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer: A systematic review. Color. Dis. 2015, 17, 849–861. [Google Scholar] [CrossRef] [PubMed]
- Maas, M.; Nelemans, P.J.; Valentini, V.; Das, P.; Rödel, C.; Kuo, L.-J.; Calvo, F.A.; García-Aguilar, J.; Glynne-Jones, R.; Haustermans, K.; et al. Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: A pooled analysis of individual patient data. Lancet Oncol. 2010, 11, 835–844. [Google Scholar] [CrossRef]
- Muíño, R.C.; Cuadros, M.; Zambudio, N.; Segura-Jiménez, I.; Cano, C.; Palma, P. Predictive Biomarkers to Chemoradiation in Locally Advanced Rectal Cancer. BioMed Res. Int. 2015, 2015, 921435. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Feng, L.; Li, M.; Ju, H.; Ding, Y.; Lan, M.; Song, S.; Han, W.; Yu, L.; Wei, M.; et al. College of American Pathologists Tumor Regression Grading System for Long-Term Outcome in Patients with Locally Advanced Rectal Cancer. Oncologist 2021, 26, e780–e793. [Google Scholar] [CrossRef]
- Van der Valk, M.J.M.; Hilling, D.; Bastiaannet, E.; Kranenbarg, E.M.-K.; Beets, G.L.; Figueiredo, N.L.; Habr-Gama, A.; Perez, R.O.; Renehan, A.G.; van de Velde, C.J.H.; et al. Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): An international multicentre registry study. Lancet 2018, 391, 2537–2545. [Google Scholar] [CrossRef] [Green Version]
- López-Campos, F.; Martín-Martín, M.; Fornell-Pérez, R.; García-Pérez, J.C.; Die-Trill, J.; Fuentes-Mateos, R.; López-Durán, S.; Domínguez-Rullán, J.; Ferreiro, R.; Riquelme-Oliveira, A.; et al. Watch and wait approach in rectal cancer: Current controversies and future directions. World J. Gastroenterol. 2020, 26, 4218–4239. [Google Scholar] [CrossRef] [PubMed]
- Caturegli, I.; Molin, M.D.; Laird, C.; Molitoris, J.K.; Bafford, A.C. Limited Role for Routine Restaging After Neoadjuvant Therapy in Locally Advanced Rectal Cancer. J. Surg. Res. 2020, 256, 317–327. [Google Scholar] [CrossRef]
- Seo, N.; Kim, H.; Cho, M.S.; Lim, J.S. Response Assessment with MRI after Chemoradiotherapy in Rectal Cancer: Current Evidences. Korean J. Radiol. 2019, 20, 1003–1018. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Aguilar, J.; Patil, S.; Kim, J.K.; Yuval, J.B.; Thompson, H.; Verheij, F.; Lee, M.; Saltz, L.B.; on behalf of the OPRA. Consortium Preliminary results of the organ preservation of rectal adenocarcinoma (OPRA) trial. J. Clin. Oncol. 2020, 38, 4008. [Google Scholar] [CrossRef]
- Hubenak, J.R.; Zhang, Q.; Branch, C.D.; Kronowitz, S.J. Mechanisms of Injury to Normal Tissue after Radiotherapy. Plast. Reconstr. Surg. 2014, 133, 49e–56e. [Google Scholar] [CrossRef] [Green Version]
- Huerta, S.; Gao, X.; Saha, D. Mechanisms of resistance to ionizing radiation in rectal cancer. Expert Rev. Mol. Diagn. 2009, 9, 469–480. [Google Scholar] [CrossRef]
- Allal, A.S.; Kähne, T.; Reverdin, A.K.; Lippert, H.; Schlegel, W.; Reymond, M.-A. Radioresistance-related proteins in rectal cancer. Proteomics 2004, 4, 2261–2269. [Google Scholar] [CrossRef]
- Kasi, A.; Abbasi, S.; Handa, S.; Al-Rajabi, R.; Saeed, A.; Baranda, J.; Sun, W. Total Neoadjuvant Therapy vs Standard Therapy in Locally Advanced Rectal Cancer. JAMA Netw. Open 2020, 3, e2030097. [Google Scholar] [CrossRef]
- E Silva, V.S.; Chinen, L.; Abdallah, E.A.; Damascena, A.; Paludo, J.; Chojniak, R.; Dettino, A.; Mello, C.A.L.; Alves, V.S.; Fanelli, M.F. Early detection of poor outcome in patients with metastatic colorectal cancer: Tumor kinetics evaluated by circulating tumor cells. OncoTargets Ther. 2016, 9, 7503–7513. [Google Scholar] [CrossRef] [Green Version]
- Silva, V.; Abdallah, E.; Brito, A.; Braun, A.; Tariki, M.; de Mello, C.; Calsavara, V.; Riechelmann, R.; Chinen, L. Baseline and Kinetic Circulating Tumor Cell Counts Are Prognostic Factors in a Prospective Study of Metastatic Colorectal Cancer. Diagnostics 2021, 11, 502. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, L.; Bensi, M.; Corallo, S.; Bergamo, F.; Pellegrini, I.; Rasola, C.; Borelli, B.; Tamburini, E.; Randon, G.; Galuppo, S.; et al. Phase II study of preoperative (PREOP) chemoradiotherapy (CTRT) plus avelumab (AVE) in patients (PTS) with locally advanced rectal cancer (LARC): The AVANA study. J. Clin. Oncol. 2021, 39, 3511. [Google Scholar] [CrossRef]
- Zaborowski, A.; Stakelum, A.; Winter, D.C. Systematic review of outcomes after total neoadjuvant therapy for locally advanced rectal cancer. Br. J. Surg. 2019, 106, 979–987. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Features | N | % |
|---|---|---|
| Total number of patients | 63 | 100 |
| Age (years) at recruitment | ||
| Median | 56 | |
| Range (min–max) | 34–92 | |
| Gender | ||
| Male | 36 | 57.1 |
| Female | 27 | 42.9 |
| ECOG Performance Status | ||
| 0 | 51 | 80.9 |
| 1 | 12 | 19.1 |
| Tumor differentiation | ||
| Well differentiated | 7 | 11.1 |
| Moderately differentiated | 54 | 85.7 |
| Poorly differentiated | 2 | 3.2 |
| Distance of tumor from dentate line (cm) | ||
| <4 | 34 | 54 |
| 4–8 | 29 | 46 |
| Median | 4 | |
| Range (min-max) | 0.5–8 | |
| Clinical Tumor Stage (cT) | ||
| cT1 or cT2 | 6 | 9.5 |
| cT3 | 51 | 81 |
| cT4 | 6 | 9.5 |
| Clinical Nodal Stage (cN) | ||
| cN0 | 5 | 7.9 |
| cN1 | 38 | 60.3 |
| cN2 | 20 | 31.8 |
| CEA in diagnosis (ng/mL; n = 61) | ||
| >3 | 32 | 52.5 |
| ≤3 | 29 | 47.5 |
| Ca 19.9 in diagnosis (U/mL; n = 55) | ||
| >37 | 10 | 18.2 |
| ≤37 | 45 | 81.8 |
| Neoadjuvant Chemotherapy | ||
| Capecitabine | 29 | 46 |
| 5-Fluorouracil (5-FU) | 34 | 54 |
| Pathological Tumor Stage (pT; n = 56) | ||
| ypT0-ypT2 | 34 | 60.7 |
| ypT3-ypT4 | 22 | 39.3 |
| Pathological Nodal Stage (pN; n = 56) | ||
| ypN0 | 45 | 80.4 |
| ypN1-ypN2 | 11 | 19.6 |
| Degree of tumor regression (TRG) (n = 56) | ||
| 0 | 13 | 23.2 |
| 1 | 17 | 30.4 |
| 2 | 18 | 32.1 |
| 3 | 7 | 12.5 |
| Unknown | 1 | 1.8 |
| Pathological Complete Response (n = 56) | ||
| Yes | 13 | 23.2 |
| No | 43 | 76.8 |
| MMR (mismatchrepair) | ||
| Proficient | 38 | 60.3 |
| Deficient | 0 | 0 |
| Unknown | 25 | 39.7 |
| Adjuvant Chemotherapy | ||
| Yes | 40 | 63.5 |
| No | 23 | 36.5 |
| Locoregional failure and distant metastasis | ||
| Yes | 22 | 34.9 |
| No | 41 | 65.1 |
| Category | Univariable Logistic Regression Model | Multivariable Logistic Regression Model | |||||
|---|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | ||
| Gender | Male | 1.0 | 1.0 | ||||
| Female | 4.050 | 1.064–15.409 | 0.040 | 3.180 | 0.626–16.163 | 0.163 | |
| CEA (ng/mL) | ≤3.0 | 1.0 | 1.0 | ||||
| >3.0 | 0.329 | 0.087–1.247 | 0.102 | 0.346 | 0.065–1.858 | 0.216 | |
| Clinical Tumor Stage | cT2 | 1.0 | 1.0 | ||||
| cT3 | 0.083 | 0.008–0.899 | 0.041 | 0.568 | 0.032–10.081 | 0.700 | |
| cT4 | 0.067 | 0.003–1.509 | 0.089 | 0.936 | 0.020–42.968 | 0.973 | |
| Chemotherapy | 5-FU | 1.0 | |||||
| Capecitabine | 0.919 | 0.257–3.292 | 0.897 | --- | --- | --- | |
| RAD23B CTC1 | Negative | 1.0 | 1.0 | ||||
| Positive | 0.077 | 0.009–0.661 | 0.019 | 0.064 | 0.006–0.751 | 0.029 | |
| TYMS CTC1 | Negative | 1.0 | |||||
| Positive | 0.821 | 0.208–3.239 | 0.779 | --- | --- | --- | |
| CTC2 > CTC1 | No | 1.0 | 0.052–4.487 | 0.524 | --- | --- | --- |
| Yes | 0.485 | ||||||
| Category | Univariable Cox Regression Model | Multivariable Cox Regression Model | |||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | ||
| pCR | No | 1.0 | 1.0 | ||||
| Yes | 0.138 | 0.018–1.029 | 0.053 | 0.388 | 0.146–1.032 | 0.058 | |
| CEA (ng/mL) | ≤3.0 | 1.0 | --- | ||||
| >3.0 | 2.527 | 0.969–6.590 | 0.058 | --- | --- | --- | |
| CTC2 > CTC1 | No | 1.0 | 1.0 | ||||
| Yes | 7.042 | 2.111–23.491 | 0.001 | 12.463 | 2.998–51.811 | 0.001 | |
| RAD23B CTC1 | Negative | 1.0 | --- | ||||
| Positive | 1.655 | 0.651–4.206 | 0.290 | --- | --- | --- | |
| TGF-βRI combined CTC | Negative | 1.0 | 1.0 | ||||
| Positive | 2.314 | 0.944–5.676 | 0.067 | 2.235 | 0.830–6.018 | 0.111 | |
| Adjuvant Chemotherapy | No | 1.0 | --- | --- | --- | ||
| Yes | 0.537 | 0.217–1.348 | 0.185 | --- | --- | --- | |
| Category | Univariable Cox Regression Model | Multivariable Cox Regression Model | |||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | ||
| pCR | No | 1.0 | 1.0 | ||||
| Yes | 0.440 | 0.054–3.579 | 0.443 | 0.378 | 0.081–1.771 | 0.217 | |
| CEA (ng/mL) | ≤3.0 | 1.0 | --- | ||||
| >3.0 | 2.576 | 0.498–13.333 | 0.259 | --- | --- | --- | |
| CTC2 > CTC1 | No | 1.0 | 1.0 | ||||
| Yes | 6.502 | 1.531–27.607 | 0.011 | 5.503 | 1.255–24.122 | 0.024 | |
| RAD CTC1 | Negative | 1.0 | --- | ||||
| Positive | 1.602 | 0.375–6.847 | 0.525 | --- | --- | --- | |
| Adjuvant Chemotherapy | No | 1.0 | --- | ||||
| Yes | 0.379 | 0.097–1.476 | 0.162 | --- | --- | --- | |
| TGF-βRI combined CTC | Negative | 1.0 | 1.0 | ||||
| Positive | 2.117 | 0.567–7.908 | 0.265 | 1.849 | 0.397–8.611 | 0.433 | |
| Strengths of the Future Perspectives | Limitations |
|---|---|
| Molecular and dynamic evaluation of proteins in circulating tumor cells allow complementary predictive and prognostic evaluation; | The proteins TGF-βRI and PD-L1 were not evaluated in all CTC samples; |
| CTC kinetics (favorable kinetics versus unfavorable kinetics) enable prognostic assessment during treatment and thus evaluate more intensive treatment regimens; | Probably because of the limitation of the number of samples, we could not demonstrate any prognostic difference in relation to PD-L1 expression. |
| The absence of RAD23B expression in CTCs may identify radiosensitive patients and improve selection for sphincter preservation strategy; | |
| The expression of TGF-βRI in CTCs may assist the prognostic evaluation of locally advanced rectal cancer (LARC) patients and be used as target molecule for future clinical trials; | Sample size, volume of blood collected and availability of ISET spots should be explored in future clinical trials for the incorporation of liquid biopsy in the therapeutic management of patients with rectal cancer undergoing neoadjuvant treatment. |
| Serial blood collection during treatment makes the dynamic analysis of the expression of PD-L1 in CTCs feasible and, therefore, permit to evaluate the possible incorporation of immunotherapy in the neoadjuvant treatment of LARC. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, V.S.e.; Abdallah, E.A.; Flores, B.d.C.T.; Braun, A.C.; Costa, D.d.J.F.; Ruano, A.P.C.; Gasparini, V.A.; Silva, M.L.G.; Mendes, G.G.; Claro, L.C.L.; et al. Molecular and Dynamic Evaluation of Proteins Related to Resistance to Neoadjuvant Treatment with Chemoradiotherapy in Circulating Tumor Cells of Patients with Locally Advanced Rectal Cancer. Cells 2021, 10, 1539. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10061539
Silva VSe, Abdallah EA, Flores BdCT, Braun AC, Costa DdJF, Ruano APC, Gasparini VA, Silva MLG, Mendes GG, Claro LCL, et al. Molecular and Dynamic Evaluation of Proteins Related to Resistance to Neoadjuvant Treatment with Chemoradiotherapy in Circulating Tumor Cells of Patients with Locally Advanced Rectal Cancer. Cells. 2021; 10(6):1539. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10061539
Chicago/Turabian StyleSilva, Virgílio Souza e, Emne Ali Abdallah, Bianca de Cássia Troncarelli Flores, Alexcia Camila Braun, Daniela de Jesus Ferreira Costa, Anna Paula Carreta Ruano, Vanessa Alves Gasparini, Maria Letícia Gobo Silva, Gustavo Gomes Mendes, Laura Carolina Lopez Claro, and et al. 2021. "Molecular and Dynamic Evaluation of Proteins Related to Resistance to Neoadjuvant Treatment with Chemoradiotherapy in Circulating Tumor Cells of Patients with Locally Advanced Rectal Cancer" Cells 10, no. 6: 1539. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10061539