
Differential Discontinuation Profiles between Pirfenidone and Nintedanib in Patients with Idiopathic Pulmonary Fibrosis

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Diagnosis of IPF and Data Collection
2.3. Disease Severity
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics, Laboratory and Physiological Data, and Prognosis
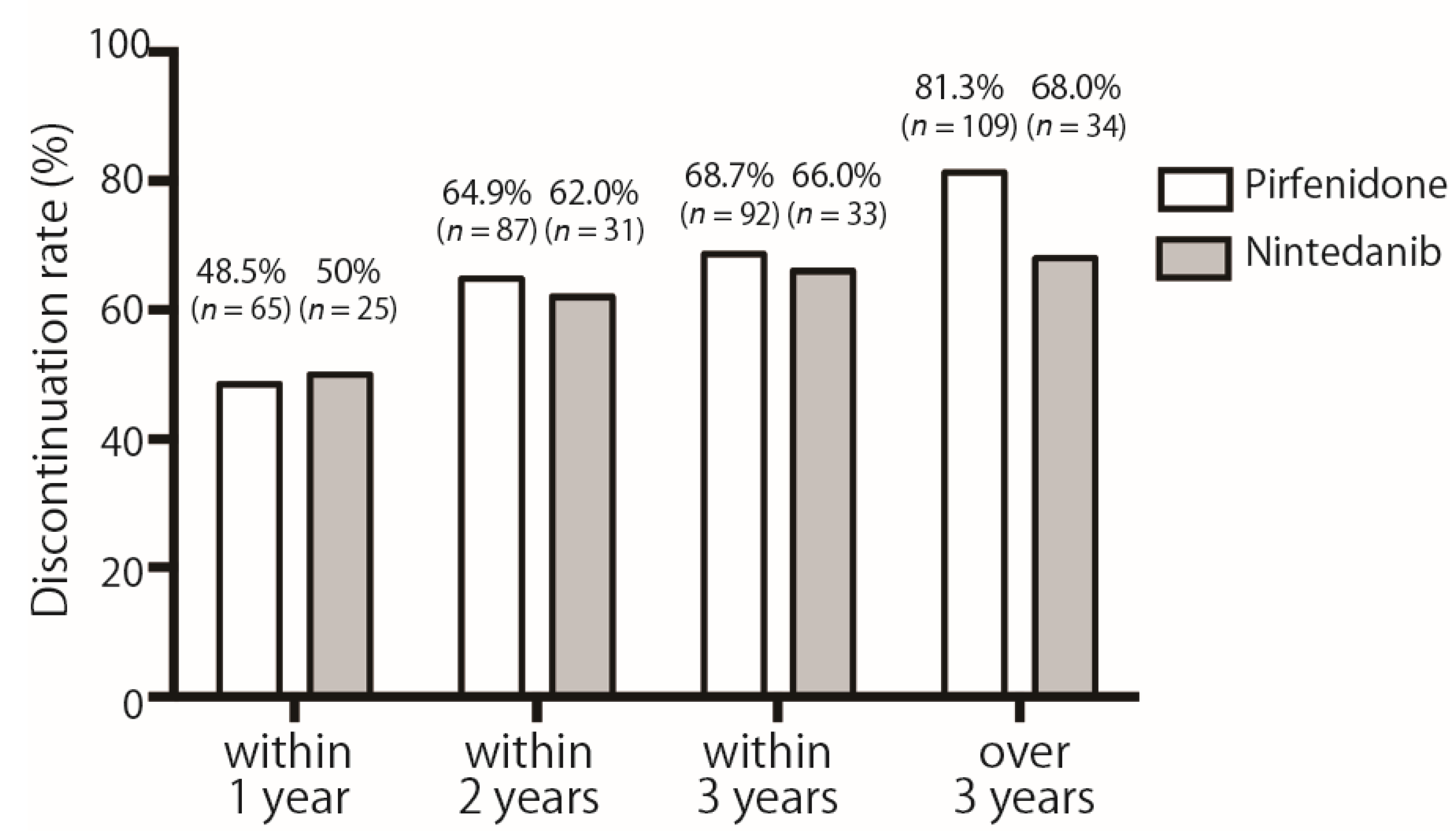
3.2. Discontinuation Rates over Time
3.3. Discontinuation Reasons
- (A)
- The adverse event discontinuation rate for pirfenidone was less than 50% from the first year, while nintedanib was still above 50% after the first year. The discontinuation rate of nintedanib due to adverse events in the first year was significantly higher than that of pirfenidone in the first year.
- (B)
- Comparison of first-year causes leading to discontinuation of pirfenidone and nintedanib. A comparison of reasons for discontinuation in the first year showed that nintedanib had fewer acute exacerbations and significantly more adverse events than pirfenidone. ** p < 0.01.
3.4. Survival Time
4. Discussion
4.1. Discontinuation of Pirfenidone
4.2. Discontinuation of Nintedanib
4.3. Risk Factors of Nintedanib Adverse Events
4.4. Discontinuation of Nintedanib in Asian Population
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trethewey, S.P.; Walters, G.I. The Role of Occupational and Environmental Exposures in the Pathogenesis of Idiopathic Pulmonary Fibrosis: A Narrative Literature Review. Medicina 2018, 54, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sack, C.; Raghu, G. Idiopathic pulmonary fibrosis: Unmasking cryptogenic environmental factors. Eur. Respir. J. 2019, 53, 1801699. [Google Scholar] [CrossRef] [PubMed]
- Koga, Y.; Satoh, T.; Kaira, K.; Hachisu, Y.; Ishii, Y.; Yajima, T.; Hisada, T.; Yokoo, H.; Dobashi, K. Progression of Idiopathic Pulmonary Fibrosis Is Associated with Silica/Silicate Inhalation. Environ. Sci. Technol. Let. 2021, 8, 903–910. [Google Scholar] [CrossRef]
- Koga, Y.; Hachisu, Y.; Tsurumaki, H.; Yatomi, M.; Kaira, K.; Ohta, S.; Ono, J.; Izuhara, K.; Dobashi, K.; Hisada, T. Pirfenidone Improves Familial Idiopathic Pulmonary Fibrosis without Affecting Serum Periostin Levels. Medicina 2019, 55, 161. [Google Scholar] [CrossRef] [Green Version]
- Fernandez Perez, E.R.; Daniels, C.E.; Schroeder, D.R.; St Sauver, J.; Hartman, T.E.; Bartholmai, B.J.; Yi, E.S.; Ryu, J.H. Incidence, prevalence, and clinical course of idiopathic pulmonary fibrosis: A population-based study. Chest 2010, 137, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Noble, P.W.; Albera, C.; Bradford, W.Z.; Costabel, U.; Glassberg, M.K.; Kardatzke, D.; King, T.E., Jr.; Lancaster, L.; Sahn, S.A.; Szwarcberg, J.; et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): Two randomised trials. Lancet 2011, 377, 1760–1769. [Google Scholar] [CrossRef]
- King, T.E., Jr.; Bradford, W.Z.; Castro-Bernardini, S.; Fagan, E.A.; Glaspole, I.; Glassberg, M.K.; Gorina, E.; Hopkins, P.M.; Kardatzke, D.; Lancaster, L.; et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2083–2092. [Google Scholar] [CrossRef] [Green Version]
- Richeldi, L.; Costabel, U.; Selman, M.; Kim, D.S.; Hansell, D.M.; Nicholson, A.G.; Brown, K.K.; Flaherty, K.R.; Noble, P.W.; Raghu, G.; et al. Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis. N. Engl. J. Med. 2011, 365, 1079–1087. [Google Scholar] [CrossRef] [Green Version]
- Richeldi, L.; du Bois, R.M.; Raghu, G.; Azuma, A.; Brown, K.K.; Costabel, U.; Cottin, V.; Flaherty, K.R.; Hansell, D.M.; Inoue, Y.; et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2071–2082. [Google Scholar] [CrossRef] [Green Version]
- Crestani, B.; Huggins, J.T.; Kaye, M.; Costabel, U.; Glaspole, I.; Ogura, T.; Song, J.W.; Stansen, W.; Quaresma, M.; Stowasser, S.; et al. Long-term safety and tolerability of nintedanib in patients with idiopathic pulmonary fibrosis: Results from the open-label extension study, INPULSIS-ON. Lancet Respir. Med. 2019, 7, 60–68. [Google Scholar] [CrossRef]
- Song, J.W.; Ogura, T.; Inoue, Y.; Xu, Z.; Quaresma, M.; Stowasser, S.; Stansen, W.; Crestani, B. Long-term treatment with nintedanib in Asian patients with idiopathic pulmonary fibrosis: Results from INPULSIS(R)-ON. Respirology 2020, 25, 410–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikeda, S.; Sekine, A.; Baba, T.; Yamakawa, H.; Morita, M.; Kitamura, H.; Ogura, T. Hepatotoxicity of nintedanib in patients with idiopathic pulmonary fibrosis: A single-center experience. Respir. Investig. 2017, 55, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Sasaki, S.; Tateyama, M.; Arai, Y.; Motomura, H.; Sumiyoshi, I.; Ochi, Y.; Watanabe, J.; Ihara, H.; Togo, S.; et al. Clinical Significance of Continuable Treatment with Nintedanib Over 12 Months for Idiopathic Pulmonary Fibrosis in a Real-World Setting. Drug Des. Devel. Ther. 2021, 15, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef] [PubMed]
- Kondoh, S.; Chiba, H.; Nishikiori, H.; Umeda, Y.; Kuronuma, K.; Otsuka, M.; Yamada, G.; Ohnishi, H.; Mori, M.; Kondoh, Y.; et al. Validation of the Japanese disease severity classification and the GAP model in Japanese patients with idiopathic pulmonary fibrosis. Respir. Investig. 2016, 54, 327–333. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ’EZR’ for medical statistics. Bone Marrow. Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hachisu, Y.; Murata, K.; Takei, K.; Tsuchiya, T.; Tsurumaki, H.; Koga, Y.; Horie, T.; Takise, A.; Hisada, T. Prognostic nutritional index as a predictor of mortality in nontuberculous mycobacterial lung disease. J. Thorac. Dis. 2020, 12, 3101–3109. [Google Scholar] [CrossRef]
- Hachisu, Y.; Koga, Y.; Kasama, S.; Kaira, K.; Yatomi, M.; Aoki-Saito, H.; Tsurumaki, H.; Kamide, Y.; Sunaga, N.; Maeno, T.; et al. Treatment with Tumor Necrosis Factor-alpha Inhibitors, History of Allergy, and Hypercalcemia Are Risk Factors of Immune Reconstitution Inflammatory Syndrome in HIV-Negative Pulmonary Tuberculosis Patients. J. Clin. Med. 2019, 9, 96. [Google Scholar] [CrossRef] [Green Version]
- Hachisu, Y.; Murata, K.; Takei, K.; Tsuchiya, T.; Tsurumaki, H.; Koga, Y.; Horie, T.; Takise, A.; Hisada, T. Possible Serological Markers to Predict Mortality in Acute Exacerbation of Idiopathic Pulmonary Fibrosis. Medicina 2019, 55, 132. [Google Scholar] [CrossRef] [Green Version]
- Ogura, T.; Azuma, A.; Inoue, Y.; Taniguchi, H.; Chida, K.; Bando, M.; Niimi, Y.; Kakutani, S.; Suga, M.; Sugiyama, Y.; et al. All-case post-marketing surveillance of 1371 patients treated with pirfenidone for idiopathic pulmonary fibrosis. Respir. Investig. 2015, 53, 232–241. [Google Scholar] [CrossRef]
- Ogawa, K.; Miyamoto, A.; Hanada, S.; Takahashi, Y.; Murase, K.; Mochizuki, S.; Uruga, H.; Takaya, H.; Morokawa, N.; Kishi, K. The Efficacy and Safety of Long-term Pirfenidone Therapy in Patients with Idiopathic Pulmonary Fibrosis. Intern. Med. 2018, 57, 2813–2818. [Google Scholar] [CrossRef] [Green Version]
- Barratt, S.L.; Mulholland, S.; Al Jbour, K.; Steer, H.; Gutsche, M.; Foley, N.; Srivastava, R.; Sharp, C.; Adamali, H.I. South-West of England’s Experience of the Safety and Tolerability Pirfenidone and Nintedanib for the Treatment of Idiopathic Pulmonary Fibrosis (IPF). Front. Pharm. 2018, 9, 1480. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, S.; Sekine, A.; Baba, T.; Katano, T.; Tabata, E.; Shintani, R.; Yamakawa, H.; Niwa, T.; Oda, T.; Okuda, R.; et al. Low starting-dosage of nintedanib for the reduction of early termination. Respir. Investig. 2019, 57, 282–285. [Google Scholar] [CrossRef]
- Kato, M.; Sasaki, S.; Nakamura, T.; Kurokawa, K.; Yamada, T.; Ochi, Y.; Ihara, H.; Takahashi, F.; Takahashi, K. Gastrointestinal adverse effects of nintedanib and the associated risk factors in patients with idiopathic pulmonary fibrosis. Sci. Rep. 2019, 9, 12062. [Google Scholar] [CrossRef] [Green Version]
- Hirasawa, Y.; Abe, M.; Terada, J.; Sakayori, M.; Suzuki, K.; Yoshioka, K.; Kawasaki, T.; Tsushima, K.; Tatsumi, K. Tolerability of nintedanib-related diarrhea in patients with idiopathic pulmonary fibrosis. Pulm. Pharm. 2020, 62, 101917. [Google Scholar] [CrossRef]
- Mazzei, M.E.; Richeldi, L.; Collard, H.R. Nintedanib in the treatment of idiopathic pulmonary fibrosis. Ther. Adv. Respir. Dis. 2015, 9, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, S.; Sekine, A.; Baba, T.; Yamanaka, Y.; Sadoyama, S.; Yamakawa, H.; Oda, T.; Okuda, R.; Kitamura, H.; Okudela, K.; et al. Low body surface area predicts hepatotoxicity of nintedanib in patients with idiopathic pulmonary fibrosis. Sci. Rep. 2017, 7, 10811. [Google Scholar] [CrossRef] [PubMed]
- Azuma, A.; Taniguchi, H.; Inoue, Y.; Kondoh, Y.; Ogura, T.; Homma, S.; Fujimoto, T.; Sakamoto, W.; Sugiyama, Y.; Nukiwa, T. Nintedanib in Japanese patients with idiopathic pulmonary fibrosis: A subgroup analysis of the INPULSIS(R) randomized trials. Respirology 2017, 22, 750–757. [Google Scholar] [CrossRef] [Green Version]
- Bargagli, E.; Piccioli, C.; Rosi, E.; Torricelli, E.; Turi, L.; Piccioli, E.; Pistolesi, M.; Ferrari, K.; Voltolini, L. Pirfenidone and Nintedanib in idiopathic pulmonary fibrosis: Real-life experience in an Italian referral centre. Pulmonology 2019, 25, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Cerri, S.; Monari, M.; Guerrieri, A.; Donatelli, P.; Bassi, I.; Garuti, M.; Luppi, F.; Betti, S.; Bandelli, G.; Carpano, M.; et al. Real-life comparison of pirfenidone and nintedanib in patients with idiopathic pulmonary fibrosis: A 24-month assessment. Respir. Med. 2019, 159, 105803. [Google Scholar] [CrossRef] [PubMed]
- Cameli, P.; Refini, R.M.; Bergantini, L.; d’Alessandro, M.; Alonzi, V.; Magnoni, C.; Rottoli, P.; Sestini, P.; Bargagli, E. Long-Term Follow-Up of Patients With Idiopathic Pulmonary Fibrosis Treated With Pirfenidone or Nintedanib: A Real-Life Comparison Study. Front. Mol. Biosci. 2020, 7, 581828. [Google Scholar] [CrossRef] [PubMed]
- Koyauchi, T.; Suzuki, Y.; Sato, K.; Hozumi, H.; Karayama, M.; Furuhashi, K.; Fujisawa, T.; Enomoto, N.; Nakamura, Y.; Inui, N.; et al. Quality of dying and death in patients with interstitial lung disease compared with lung cancer: An observational study. Thorax 2021, 76, 248–255. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | All Patients (n = 184) | Pirfenidone (n = 134) | Nintedanib (n = 50) | p Value |
|---|---|---|---|---|
| Characteristics | ||||
| Age (years) | 71 (39–90) | 71 (43–90) | 72 (39–87) | 0.237 |
| Male (male/female) | 141 (76.6) | 98/36 (73.1%) | 43/7 (86%) | 0.079 |
| Body mass index (kg/m2) | 22.6 (13.7–36.7) | 22.3 (13.7–36.7) | 23.1 (14.3–28.1) | 0.307 |
| Body surface area (DuBois, m2) | 1.65 (1.18–2.58) | 1.63 (1.18–2.16) | 1.66 (1.23–2.58) | 0.232 |
| Physiologic Marker before Treatment | ||||
| FVC (L) | 2.20 (0.62–4.56) | 2.17 (0.62–4.56) | 2.31 (1.03–4.16) | 0.838 |
| %FVC (%) | 71.8 (27.4–124.9) | 74.0 (27.4–124.9) | 70.0 (31.0–116.5) | 0.761 |
| %DLCO (%) | 52.6 (31.0–137.4) | 54.4 (3.1–137.4) | 51.4 (17.1–76.7) | 0.138 |
| JRS severity grade (I/II/III/IV/unknown) | 23/12/63/61//25 | 20/7/40/46//21 | 3/5/23/15//4 | 0.104 |
| GAP staging system (−2~0/1/2/3) | 6/8/26/29 | 6/5/20/21 | 0/3/6/8 | |
| (4/5/6/7/8//unknown) | 28/19/6/4/1//57 | 20/12/3/3/0//44 | 8/7/3/1/1//13 | 0.624 |
| Serological Marker | ||||
| Albumin (g/dL) | 3.9 (2.1–4.7) | 3.8 (2.1–4.6) | 4.0 (2.6–4.7) | 0.018 * |
| CRP (mg/dL) | 0.26 (0.00–21.87) | 0.29 (0.00–21.87) | 0.25 (0.03–2.67) | 0.280 |
| KL-6 (U/mL) | 1260.0 (223.0–9370.0) | 1253.0 (303.0–9370.0) | 1305.0 (223.0–8593.0) | 0.762 |
| SP-D (ng/mL) | 237.0 (20.6–1100.0) | 237.0 (29.5–1100.0) | 259.5 (20.6–728.0) | 0.544 |
| Treatment Period and Disease Progress | ||||
| Final amount (mg) | 1153 ± 420.6 | 249 ± 59.69 | ||
| Observation periods (days) | 390 (2–2575) | 389 (2–2575) | 395 (5–1172) | 0.758 |
| Administration period (days) | 378 (2–2575) | 387 (2–2575) | 351 (5–1172) | 0.651 |
| FVC decline per a year (L) | 0.110 (−3.26–8.21) | 0.100(−3.26–8.21) | 0.180 (−0.70–1.26) | 0.573 |
| Pirfenidone (n = 109) | Nintedanib (n = 34) | p Value | |
|---|---|---|---|
| Acute exacerbation | 23 (21.1%) | 8 (23.5%) | 0.819 |
| Disease progression | 15 (13.8%) | 3 (8.8%) | 0.766 |
| Hospital transfer | 15 (13.8%) | 1 (2.9%) | 0.199 |
| Lung cancer | 5 (4.6%) | 2 (5.9%) | 0.674 |
| Adverse effects | 34 (31.2%) | 24 (70.6%) | 0.016 * |
| Photosensitivity | 2 (1.8%) | 0 (0.0%) | 1.000 |
| Anorexia/ Nausea | 16 (14.7%) | 6 (17.6%) | 0.790 |
| Diarrhea | 2 (1.8%) | 5 (14.7%) | 0.013 * |
| Liver disorder | 0 (0.0%) | 9 (26.5%) | <0.001 ** |
| Cardiac disease | 1 (0.9%) | 0 (0.0%) | 1.000 |
| Thrombosis | 0 (0.0%) | 0 (0.0%) | 1.000 |
| Other adverse effects | 13 (11.9%) | 10 (29.4%) | 0.072 |
| Other reasons except the above | 9 (8.2%) | 0 (0.0%) | 0.209 |
| Unknown | 11 (10.1%) | 2 (5.9%) | 0.734 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takehara, K.; Koga, Y.; Hachisu, Y.; Utsugi, M.; Sawada, Y.; Saito, Y.; Yoshimi, S.; Yatomi, M.; Shin, Y.; Wakamatsu, I.; et al. Differential Discontinuation Profiles between Pirfenidone and Nintedanib in Patients with Idiopathic Pulmonary Fibrosis. Cells 2022, 11, 143. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11010143
Takehara K, Koga Y, Hachisu Y, Utsugi M, Sawada Y, Saito Y, Yoshimi S, Yatomi M, Shin Y, Wakamatsu I, et al. Differential Discontinuation Profiles between Pirfenidone and Nintedanib in Patients with Idiopathic Pulmonary Fibrosis. Cells. 2022; 11(1):143. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11010143
Chicago/Turabian StyleTakehara, Kazutaka, Yasuhiko Koga, Yoshimasa Hachisu, Mitsuyoshi Utsugi, Yuri Sawada, Yasuyuki Saito, Seishi Yoshimi, Masakiyo Yatomi, Yuki Shin, Ikuo Wakamatsu, and et al. 2022. "Differential Discontinuation Profiles between Pirfenidone and Nintedanib in Patients with Idiopathic Pulmonary Fibrosis" Cells 11, no. 1: 143. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11010143