
Discriminative Value of Serum Irisin in Prediction of Heart Failure with Different Phenotypes among Patients with Type 2 Diabetes Mellitus
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
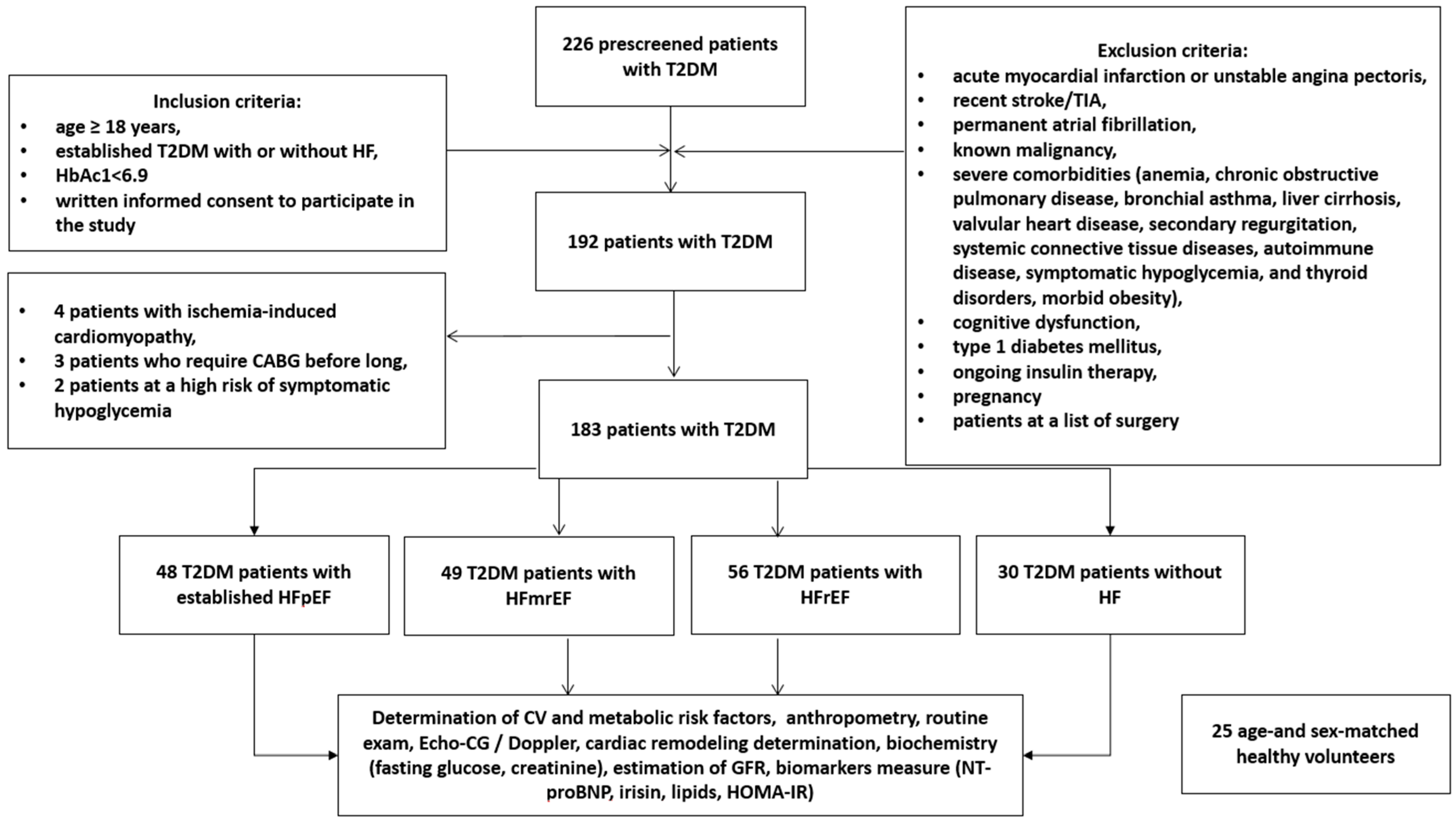
2.1. Study Design and Cohorts of Participants
2.2. Determination of Patients’ Background, Risk Factors and Comorbidities
2.3. Anthropometric Measurements and Clinical Examinations
2.4. Concomitant Medications
2.5. Echocardiography and Doppler Method
2.6. Estimating Glomerular Filtration Rate
2.7. Insulin Resistance Determination
2.8. Blood Sampling and Biomarker Measurements
2.9. Statistics
3. Results
3.1. General Characteristics of the Patients Included in the Study
3.2. Circulating Levels of Irisin in T2DM Patients and Healthy Volunteers
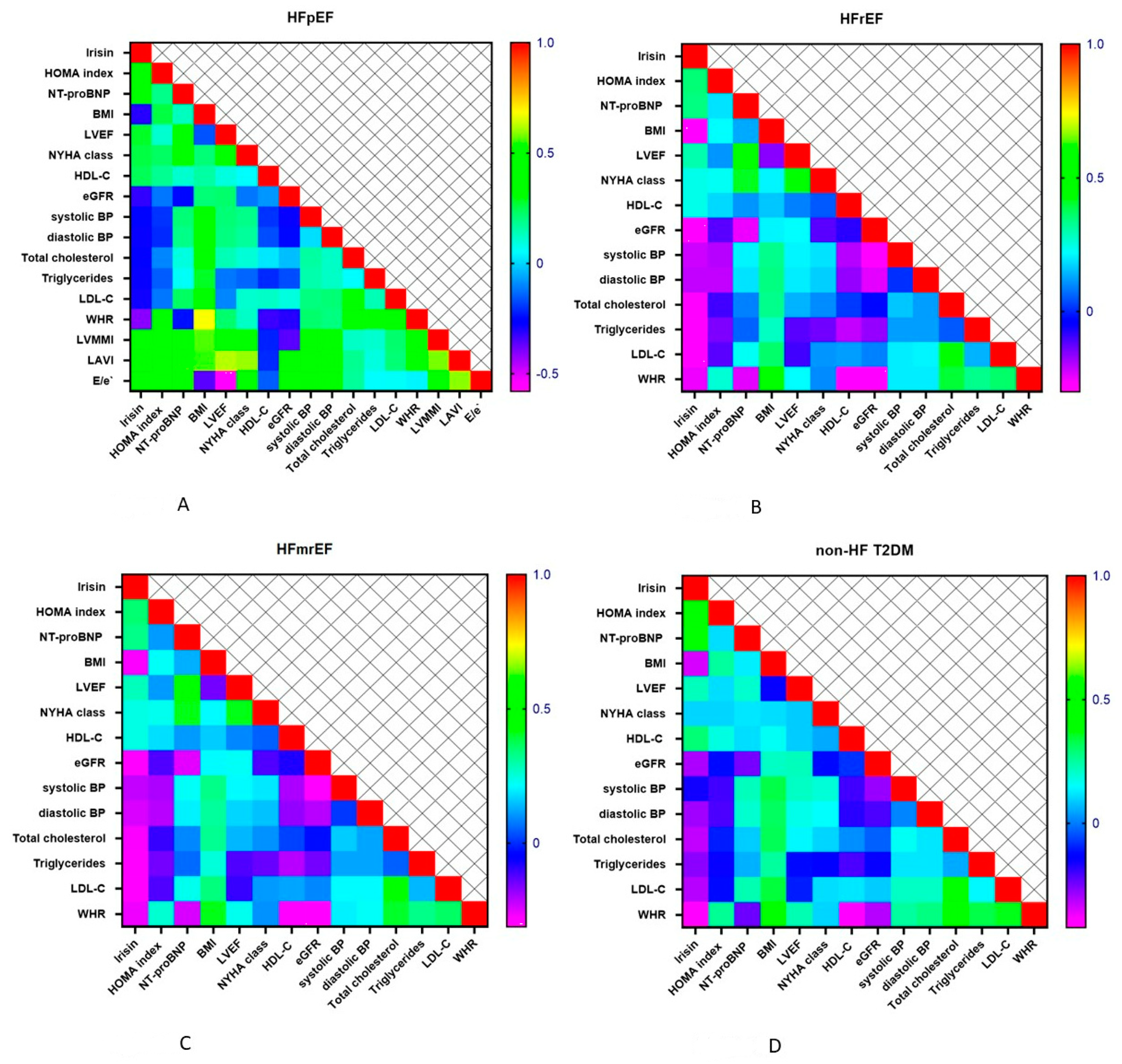
3.3. Spearman’s Correlation between Irisin Level and HOMA Index, NT-proBNP, Lipid Profile and Hemodynamics Parameters
3.4. Predictive Models for Different Phenotypes of HF
3.5. Comparison of the Predictive Models
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Cho, D.-H.; Yoo, B.-S. Current Prevalence, Incidence, and Outcomes of Heart Failure with Preserved Ejection Fraction. Heart Fail. Clin. 2021, 17, 315–326. [Google Scholar] [CrossRef]
- Chen, Y.; Voors, A.A.; Jaarsma, T.; Lang, C.C.; Sama, I.E.; Akkerhuis, K.M.; Boersma, E.; Hillege, H.L.; Postmus, D. A heart failure phenotype stratified model for predicting 1-year mortality in patients admitted with acute heart failure: Results from an individual participant data meta-analysis of four prospective European cohorts. BMC Med. 2021, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Savarese, G.; Vedin, O.; D’Amario, D.; Uijl, A.; Dahlström, U.; Rosano, G.; Lam, C.S.; Lund, L.H. Prevalence and Prognostic Implications of Longitudinal Ejection Fraction Change in Heart Failure. JACC Heart Fail. 2019, 7, 306–317. [Google Scholar] [CrossRef]
- Chen, L.; Huang, Z.; Zhao, X.; Liang, J.; Lu, X.; He, Y.; Kang, Y.; Xie, Y.; Liu, J.; Liu, Y.; et al. Predictors and Mortality for Worsening Left Ventricular Ejection Fraction in Patients With HFpEF. Front. Cardiovasc. Med. 2022, 9, 820178. [Google Scholar] [CrossRef]
- Aimo, A.; Gaggin, H.K.; Barison, A.; Emdin, M.; Januzzi, J.L., Jr. Imaging, Biomarker, and Clinical Predictors of Cardiac Remodeling in Heart Failure With Reduced Ejection Fraction. JACC Heart Fail. 2019, 7, 782–794. [Google Scholar] [CrossRef]
- Daubert, M.A.; Adams, K.; Yow, E.; Barnhart, H.X.; Douglas, P.S.; Rimmer, S.; Norris, C.; Cooper, L.; Leifer, E.; Desvigne-Nickens, P.; et al. NT-proBNP Goal Achievement Is Associated With Significant Reverse Remodeling and Improved Clinical Outcomes in HFrEF. JACC Heart Fail. 2019, 7, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Daubert, M.A.; Yow, E.; Barnhart, H.X.; Piña, I.L.; Ahmad, T.; Leifer, E.; Cooper, L.; Desvigne-Nickens, P.; Fiuzat, M.; Adams, K.; et al. Differences in NT-proBNP Response and Prognosis in Men and Women With Heart Failure With Reduced Ejection Fraction. J. Am. Heart Assoc. 2021, 10, e019712. [Google Scholar] [CrossRef]
- Chen, H.; Chhor, M.; Rayner, B.S.; McGrath, K.; McClements, L. Evaluation of the diagnostic accuracy of current biomarkers in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Arch. Cardiovasc. Dis. 2021, 114, 793–804. [Google Scholar] [CrossRef] [PubMed]
- Topf, A.; Mirna, M.; Ohnewein, B.; Jirak, P.; Kopp, K.; Fejzic, D.; Haslinger, M.; Motloch, L.J.; Hoppe, U.C.; Berezin, A.; et al. The Diagnostic and Therapeutic Value of Multimarker Analysis in Heart Failure. An Approach to Biomarker-Targeted Therapy. Front. Cardiovasc. Med. 2020, 7, 579567. [Google Scholar] [CrossRef]
- Kim, H.; Wrann, C.D.; Jedrychowski, M.; Vidoni, S.; Kitase, Y.; Nagano, K.; Zhou, C.; Chou, J.; Parkman, V.A.; Novick, S.J.; et al. Irisin mediates effects on bone and fat via alphaV integrin receptors. Cell 2018, 175, 1756–1768.e17. [Google Scholar] [CrossRef]
- Kurdiova, T.; Balaz, M.; Vician, M.; Maderova, D.; Vlcek, M.; Valkovic, L.; Srbecky, M.; Imrich, R.; Kyselovicova, O.; Belan, V.; et al. Effects of obesity, diabetes and exercise on Fndc5 gene expression and irisin release in human skeletal muscle and adipose tissue: In vivo andin vitro studies. J. Physiol. 2014, 592, 1091–1107. [Google Scholar] [CrossRef]
- Waseem, R.; Shamsi, A.; Mohammad, T.; Hassan, I.; Kazim, S.N.; Chaudhary, A.A.; Rudayni, H.A.; Al-Zharani, M.; Ahmad, F.; Islam, A. FNDC5/Irisin: Physiology and Pathophysiology. Molecules 2022, 27, 1118. [Google Scholar] [CrossRef] [PubMed]
- Korta, P.; Pocheć, E.; Mazur-Biały, A. Irisin as a Multifunctional Protein: Implications for Health and Certain Diseases. Medicina 2019, 55, 485. [Google Scholar] [CrossRef] [PubMed]
- Boström, P.; Wu, J.; Jedrychowski, M.P.; Korde, A.; Ye, L.; Lo, J.C.; Rasbach, K.A.; Boström, E.A.; Choi, J.H.; Long, J.Z.; et al. A PGC1-α-dependent myokine that drives brown-fat-like development of white fat and thermogenesis. Nature 2012, 481, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Colaianni, G.; Storlino, G.; Sanesi, L.; Colucci, S.; Grano, M. Myokines and Osteokines in the Pathogenesis of Muscle and Bone Diseases. Curr. Osteoporos. Rep. 2020, 18, 401–407. [Google Scholar] [CrossRef]
- Moreno-Navarrete, J.M.; Ortega, F.J.; Serrano, M.; Guerra, E.; Pardo, G.; Tinahones, F.; Ricart, W.; Fernández-Real, J.M. Irisin Is Expressed and Produced by Human Muscle and Adipose Tissue in Association With Obesity and Insulin Resistance. J. Clin. Endocrinol. Metab. 2013, 98, E769–E778. [Google Scholar] [CrossRef] [PubMed]
- Armandi, A.; Rosso, C.; Nicolosi, A.; Caviglia, G.P.; Abate, M.L.; Olivero, A.; D’Amato, D.; Vernero, M.; Gaggini, M.; Saracco, G.M.; et al. Crosstalk between Irisin Levels, Liver Fibrogenesis and Liver Damage in Non-Obese, Non-Diabetic Individuals with Non-Alcoholic Fatty Liver Disease. J. Clin. Med. 2022, 11, 635. [Google Scholar] [CrossRef]
- Yan, W.; Chen, Y.; Guo, Y.; Xia, Y.; Li, C.; Du, Y.; Lin, C.; Xu, X.; Qi, T.; Fan, M.; et al. Irisin Promotes Cardiac Homing of Intravenously Delivered MSCs and Protects against Ischemic Heart Injury. Adv. Sci. 2022, 9, 2103697. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Kou, W.; Xu, X.; Zhou, S.; Luan, P.; Xu, X.; Li, H.; Zhuang, J.; Wang, J.; Zhao, Y.; et al. FNDC5/Irisin inhibits pathological cardiac hypertrophy. Clin. Sci. 2019, 133, 611–627. [Google Scholar] [CrossRef]
- Akyuz, A.; Mert, B.; Gur, D.O.; Efe, M.M.; Aykac, H.; Alpsoy, S.; Guzel, S. Association of Lower Serum Irisin Levels With Diabetes Mellitus: Irrespective Of Coronary Collateral Circulation, And SYNTAX Score. North. Clin. Istanb. 2021, 8, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Saadeldin, M.K.; Elshaer, S.S.; Emara, I.A.; Maged, M.; Abdel-Aziz, A.K. Serum sclerostin and irisin as predictive markers for atherosclerosis in Egyptian type II diabetic female patients: A case control study. PLoS ONE 2018, 13, e0206761. [Google Scholar] [CrossRef]
- El-Mottaleb, N.A.A.; Galal, H.M.; El Maghraby, K.M.; Gadallah, A.I. Serum irisin level in myocardial infarction patients with or without heart failure. Can. J. Physiol. Pharmacol. 2019, 97, 932–938 . [Google Scholar] [CrossRef] [PubMed]
- Kalkan, A.K.; Cakmak, H.A.; Erturk, M.; Kalkan, K.E.; Uzun, F.; Tasbulak, O.; Diker, V.O.; Aydin, S.; Celik, A. Adropin and Irisin in Patients with Cardiac Cachexia. Arq. Bras. Cardiol. 2018, 111, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.; Gao, R.; Bei, Y.; Li, J.; Zhang, H.; Zhou, Y.; Yao, W.; Xu, D.; Zhou, F.; Jin, M.; et al. Serum Irisin Predicts Mortality Risk in Acute Heart Failure Patients. Cell. Physiol. Biochem. 2017, 42, 615–622. [Google Scholar] [CrossRef]
- Berezin, A.E.; Berezin, A.A.; Lichtenauer, M. Myokines and Heart Failure: Challenging Role in Adverse Cardiac Remodeling, Myopathy, and Clinical Outcomes. Dis. Markers 2021, 2021, 6644631. [Google Scholar] [CrossRef]
- Seferovic, P.M.; Ponikowski, P.; Anker, S.D.; Bauersachs, J.; Chioncel, O.; Cleland, J.G.; De Boer, R.A.; Drexel, H.; Ben Gal, T.; Hill, L.; et al. Clinical practice update on heart failure 2019: Pharmacotherapy, procedures, devices and patient management. An expert consensus meeting report of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 1169–1186. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Cefula, W. Standards of medical care in diabetes-2014: Summary of revisions. Diabetes Care 2015, 38, S1–S93. [Google Scholar]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidemias: The Task Force for the Management of Dyslipidemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) Developed with the special contribution of the European Associa-tion for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis 2016, 253, 281–344. [Google Scholar] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [Green Version]
- Marwick, T.H.; Gillebert, T.C.; Aurigemma, G.; Chirinos, J.; Derumeaux, G.; Galderisi, M.; Gottdiener, J.; Haluska, B.; Ofili, E.; Segers, P.; et al. Recommendations on the Use of Echocardiography in Adult Hypertension: A Report from the European Association of Cardiovascular Imaging (EACVI) and the American Society of Echocardiography (ASE). J. Am. Soc. Echocardiogr. 2015, 28, 727–754. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., III; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314 . [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F., III; Feldman, H.I. For the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Sobieszek, G.; Powrózek, T.; Mazurek, M.; Skwarek-Dziekanowska, A.; Małecka-Massalska, T. Electrical and Hormonal Biomarkers in Cachectic Elderly Women with Chronic Heart Failure. J. Clin. Med. 2020, 9, 1021. [Google Scholar] [CrossRef]
- Han, X.; Zhang, S.; Chen, Z.; Adhikari, B.K.; Zhang, Y.; Zhang, J.; Sun, J.; Wang, Y. Cardiac biomarkers of heart failure in chronic kidney disease. Clin. Chim. Acta 2020, 510, 298–310. [Google Scholar] [CrossRef]
- Berezin, A.E.; Berezin, A.A. Circulating Cardiac Biomarkers in Diabetes Mellitus: A New Dawn for Risk Stratification—A Narrative Review. Diabetes Ther. 2020, 11, 1271–1291. [Google Scholar] [CrossRef]
- Ho, M.-Y.; Wang, C.-Y. Role of Irisin in Myocardial Infarction, Heart Failure, and Cardiac Hypertrophy. Cells 2021, 10, 2103. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, S.D.; Frangogiannis, N.G. The Biological Basis for Cardiac Repair After Myocardial Infarction. From Inflammation to Fibrosis. Circ. Res. 2016, 119, 91–112. [Google Scholar] [CrossRef] [PubMed]
- Kawada, T. Serum Irisin and Diabetic Nephropathy in Patients with Diabetes Mellitus. Horm. Metab. Res. 2021, 53, 825. [Google Scholar] [CrossRef] [PubMed]
- Du, X.-L.; Jiang, W.-X.; Lv, Z.-T. Lower Circulating Irisin Level in Patients with Diabetes Mellitus: A Systematic Review and Meta-Analysis. Horm. Metab. Res. 2016, 48, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Peng, Q.; Wang, X.; Wu, K.; Liu, K.; Wang, S.; Chen, X. Irisin attenuates H2O2-induced apoptosis in cardiomyocytes via microRNA-19b/AKT/mTOR signaling pathway. Int. J. Clin. Exp. Pathol. 2017, 10, 7707–7717. [Google Scholar]
- Deng, J.; Zhang, N.; Chen, F.; Yang, C.; Ning, H.; Xiao, C.; Sun, K.; Liu, Y.; Yang, M.; Hu, T.; et al. Irisin ameliorates high glucose-induced cardiomyocytes injury via AMPK/mTOR signal pathway. Cell Biol. Int. 2020, 44, 2315–2325. [Google Scholar] [CrossRef]
- Matsuo, Y.; Gleitsmann, K.; Mangner, N.; Werner, S.; Fischer, T.; Bowen, T.S.; Kricke, A.; Matsumoto, Y.; Kurabayashi, M.; Schuler, G.; et al. Fibronectin type III domain containing 5 expression in skeletal muscle in chronic heart failure-relevance of inflammatory cytokines. J. Cachex-Sarcopenia Muscle 2015, 6, 62–72. [Google Scholar] [CrossRef]
- Berezin, A.A.; Lichtenauer, M.; Boxhammer, E.; Fushtey, I.M.; Berezin, A.E. Serum Levels of Irisin Predict Cumulative Clinical Outcomes in Heart Failure Patients With Type 2 Diabetes Mellitus. Front. Physiol. 2022, 13, 922775. [Google Scholar] [CrossRef]
- Peng, Q.; Ding, R.; Wang, X.; Yang, P.; Jiang, F.; Chen, X. Effect of Irisin on Pressure Overload–Induced Cardiac Remodeling. Arch. Med. Res. 2021, 52, 182–190. [Google Scholar] [CrossRef]
- Philippou, A.; Xanthis, D.; Chryssanthopοulos, C.; Maridaki, M.; Koutsilieris, M. Heart Failure–Induced Skeletal Muscle Wasting. Curr. Hear. Fail. Rep. 2020, 17, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Schnyder, S.; Handschin, C. Skeletal muscle as an endocrine organ: PGC-1α, myokines and exercise. Bone 2015, 80, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Li, R.-L.; Wu, S.-S.; Wu, Y.; Wang, X.-X.; Chen, H.-Y.; Xin, J.-J.; Li, H.; Lan, J.; Xue, K.-Y.; Li, X.; et al. Irisin alleviates pressure overload-induced cardiac hypertrophy by inducing protective autophagy via mTOR-independent activation of the AMPK-ULK1 pathway. J. Mol. Cell. Cardiol. 2018, 121, 242–255. [Google Scholar] [CrossRef]
- van Empel, V.; Rocca, H.-P.B.-L. Inflammation in HFpEF: Key or circumstantial? Int. J. Cardiol. 2015, 189, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Berezin, A. Endogenous vascular repair system in cardiovascular disease: The role of endothelial progenitor cells. Australas. Med. J. 2019, 12, 42–48. [Google Scholar] [CrossRef]
- Paulus, W.J.; Tschöpe, C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J. Am. Coll Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Szaroszyk, M.; Kattih, B.; Martin-Garrido, A.; Trogisch, F.A.; Dittrich, G.M.; Grund, A.; Abouissa, A.; Derlin, K.; Meier, M.; Holler, T.; et al. Skeletal muscle derived Musclin protects the heart during pathological overload. Nat. Commun. 2022, 13, 149. [Google Scholar] [CrossRef]
- Silvestrini, A.; Bruno, C.; Vergani, E.; Venuti, A.; Favuzzi, A.M.R.; Guidi, F.; Nicolotti, N.; Meucci, E.; Mordente, A.; Mancini, A. Circulating irisin levels in heart failure with preserved or reduced ejection fraction: A pilot study. PLoS ONE 2019, 14, e0210320. [Google Scholar] [CrossRef]
- Ou-Yang, W.-L.; Guo, B.; Xu, F.; Lin, X.; Li, F.-X.; Shan, S.-K.; Wu, F.; Wang, Y.; Zheng, M.-H.; Xu, Q.-S.; et al. The Controversial Role of Irisin in Clinical Management of Coronary Heart Disease. Front. Endocrinol. 2021, 12, 678309. [Google Scholar] [CrossRef] [PubMed]
- Wenwen, G.; Baihui, Z.; Xia, W. Lower irisin levels in coronary artery disease: A meta-analysis. Minerva Endocrinol. 2020, 45, 61–69. [Google Scholar] [CrossRef]
- Li, X.-T.; Zhang, M.-W.; Zhang, Z.-Z.; Cao, Y.-D.; Liu, X.-Y.; Miao, R.; Xu, Y.; Song, X.-F.; Song, J.-W.; Liu, Y.; et al. Abnormal apelin-ACE2 and SGLT2 signaling contribute to adverse cardiorenal injury in patients with COVID-19. Int. J. Cardiol. 2021, 336, 123–129. [Google Scholar] [CrossRef]
- Janovska, P.; Melenovsky, V.; Svobodova, M.; Havlenova, T.; Kratochvilova, H.; Haluzik, M.; Hoskova, E.; Pelikanova, T.; Kautzner, J.; Monzo, L.; et al. Dysregulation of epicardial adipose tissue in cachexia due to heart failure: The role of natriuretic peptides and cardiolipin. J. Cachexia Sarcopenia Muscle 2020, 11, 1614–1627 . [Google Scholar] [CrossRef] [PubMed]
- Berezin, A.; Fushtey, I.; Berezin, A. Utility of irisin and apelin in prediction of heart failure phenotypes in type 2 diabetes mellitus patients. J. Hypertens. 2022, 40, e84–e85. [Google Scholar] [CrossRef]
- Kałużna, M.; Pawlaczyk, K.; Schwermer, K.; Hoppe, K.; Człapka-Matyasik, M.; Ibrahim, A.; Sawicka-Gutaj, N.; Minczykowski, A.; Ziemnicka, K.; Oko, A.; et al. Adropin and irisin: New biomarkers of cardiac status in patients with end-stage renal disease? A preliminary study. Adv. Clin. Exp. Med. 2019, 28, 347–353. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Healthy Volunteers (n = 25) | Entire Patient Cohort (n = 183) | T2DM Patients (n = 183) | p Value | |||
|---|---|---|---|---|---|---|---|
| HfpEF (n = 48) | HFmrEF (n = 49) | HFrEF (n = 56) | Non-HF (n = 30) | ||||
| Age, year | 48 (42–55) | 51 (41–62) | 52 (43–62) | 52 (41–64) | 53(42–60) | 51(41–60) | 0.86 |
| Male, n (%) | 17 (68.0) | 118 (64.5) | 31 (64.6) | 32 (65.3) | 37 (66.1) | 18 (60.0) | 0.82 |
| Dyslipidemia, n (%) | 0 | 152 (83.1) # | 38 (79.2) | 41 (83.7) | 48 (85.7) | 25 (83.3) | 0.82 |
| Hypertension, n (%) | 0 | 158 (86.3) # | 43 (89.5) | 39 (79.6) | 50 (89.2) | 26 (86.7) | 0.79 |
| Smoking, n (%) | 5 (20.0) | 89 (48.6) # | 21 (43.8) | 25 (51.0) | 27 (48.2) | 16 (53.3) | 0.05 |
| Abdominal obesity, n (%) | 0 | 84 (45.9) # | 22 (45.8) | 24 (48.9) | 25 (44.6) | 13 (43.3) | 0.88 |
| Microalbuminuria, n (%) | 0 | 56 (30.6) # | 14 (29.1) | 16 (32.7) | 17 (30.4) | 9 (30.0) | 0.84 |
| LV hypertrophy, n (%) | 0 | 144 (78.7) # | 41 (85.4) | 39 (79.6) | 43 (78.8) | 21 (70.0) | 0.001 |
| BMI, kg/m2 | 21.9 ± 0.5 | 25.8 ± 2.1 # | 25.5 ± 2.4 | 25.6 ± 2.8 | 25.2 ± 2.1 | 26.3 ± 2.6 | 0.88 |
| Waist circumference, sm | 75.0 ± 2.6 | 85.6 ± 2.9 # | 85.4 ± 3.2 | 85.1 ± 3.2 | 85.0 ± 3.4 | 86.5 ± 3.1 | 0.86 |
| WHR, units | 0.78 ± 0.02 | 0.86 ± 0.03 # | 0.85 ± 0.07 | 0.85 ± 0.05 | 0.84 ± 0.04 | 0.87 ± 0.03 | 0.86 |
| II/III NYHA class, n | 0 | 103/50 # | 31/17 | 30/19 | 42/14 | - | 0.14 |
| SBP, mm Hg | 127 ± 4 | 132 ± 5 | 130 ± 4 | 130 ± 6 | 128 ± 5 | 135 ± 5 | 0.81 |
| DBP, mm Hg | 75 ± 3 | 80 ± 4 | 78 ± 4 | 76 ± 5 | 74 ± 4 | 84 ± 3 | 0.80 |
| LVEDV, mL | 88 ± 4 | 154 ± 9 # | 159 ± 5 | 161 ± 4 | 162 ± 8 | 147 ± 6 | 0.001 |
| LVESV, mL | 30 ± 3 | 62 ± 7 # | 66 ± 4 | 86 ± 6 | 104 ± 4 | 59 ± 3 | 0.001 |
| LVEF, % | 66 ± 2 | 59 ± 6 # | 58 ± 3 | 46 ± 3 | 35 ± 4 | 60 ± 2 | 0.001 |
| LVMMI, g/m2 | 80.7 ± 0.06 | 151 ± 6.12# | 149 ± 4 | 154 ± 5 | 156 ± 7 | 137 ± 3 | 0.01 |
| LAVI, mL/m2 | 22 ± 4 | 39 ± 8 # | 36 ± 4 | 38 ± 4 | 41 ± 3 | 30 ± 5 | 0.03 |
| E/e’, unit | 5.4 ± 0.1 | 13.9 ± 0.5 # | 12.8 ± 0.2 | 13.5 ± 0.3 | 15.1 ± 0.3 | 7.2 ± 0.4 | 0.001 |
| eGFR, mL/min/1.73 m2 | 108 ± 5.10 | 83 ± 6.0 # | 81 ± 4.2 | 75 ± 4.0 | 73 ± 3.5 | 86 ± 3.5 | 0.01 |
| HOMA-IR | 1.53 ± 0.30 | 7.65 ± 3.7 # | 7.90 ± 3.0 | 7.95 ± 2.3 | 8.02 ± 2.1 | 7.15 ± 2.4 | 0.14 |
| NT-proBNP, pmol/mL | 52 (33–74) | 2718 (1380–3720) # | 998 (745–1126) | 3115 (2380–3750) | 3125 (2540–3810) | 105 (72–142) | 0.001 |
| Fasting glucose, mmol/L | 4.22 ± 0.70 | 5.84 ± 1.2 # | 5.70 ± 1.5 | 5.62 ± 1.3 | 5.45 ± 1.2 | 5.92 ± 1.3 | 0.28 |
| Creatinine, mcmol/L | 52.5 ± 9.3 | 108.8 ± 12.0 # | 103.7 ± 9.8 | 108.6 ± 8.5 | 112.5 ± 6.1 | 95.1 ± 10.4 | 0.26 |
| HbA1c, % | 4.20 ± 0.95 | 6.65 ± 0.04 # | 6.54 ± 0.03 | 6.59 ± 0.02 | 6.55 ± 0.03 | 6.70 ± 0.05 | 0.70 |
| TC, mmol/L | 4.6 ± 0.09 | 6.41 ± 0.05 # | 6.37 ± 0.68 | 6.43 ± 0.60 | 6.40 ± 0.46 | 6.42 ± 0.55 | 0.82 |
| HDL-C, mmol/L | 1.2 ± 0.03 | 0.95 ± 0.21 # | 0.97 ± 0.22 | 0.97 ± 0.17 | 0.95 ± 0.14 | 0.93 ± 0.24 | 0.80 |
| LDL-C, mmol/L | 2.8 ± 0.05 | 4.43 ± 0.20 # | 4.42 ± 0.12 | 4.38 ± 0.10 | 4.35 ± 0.11 | 4.51 ± 0.15 | 0.68 |
| TG, mmol/L | 1.3 ± 0.04 | 2.26 ± 0.04 # | 2.23 ± 0.19 | 2.21 ± 0.17 | 2.20 ± 0.12 | 2.30 ± 1.12 | 0.64 |
| SGLT2i, n (%) | 0 | 171 (93.4) | 48 (100) | 49 (100) | 56 (100) | 18 (60) | 0.82 |
| ACEIs/ARBs/ARNI, n (%) | 0 | 158 (86.3) # | 43 (89.5) | 39 (79.6) | 50 (89.2) | 26 (86.7) | 0.80 |
| Variables | Dependent Variables | |||||
|---|---|---|---|---|---|---|
| Univariate Log Regression | Multivariate Log Regression | |||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Dependent variable: HFpEF | ||||||
| Irisin < 10.4 ng/mL | 1.52 | 1.16–2.86 | 0.001 | 1.30 | 1.08–2.15 | 0.001 |
| LV hypertrophy | 1.12 | 1.06–1.19 | 0.044 | 1.05 | 1.00–1.11 | 0.14 |
| eGFR | 0.93 | 0.89–1.02 | 0.94 | - | ||
| BMI > 34 kg/m2 | 1.07 | 1.02–1.11 | 0.046 | 1.05 | 1.00–1.08 | 0.062 |
| NT-proBNP > 750 pmol/mL | 1.54 | 1.06–2.33 | 0.001 | 1.17 | 1.02–1.26 | 0.042 |
| Age | 1.03 | 1.02–1.05 | 0.048 | 1.03 | 1.00–1.04 | 0.16 |
| Smoking | 1.04 | 0.98–1.07 | 0.92 | - | ||
| E/e’ > 11 units | 1.12 | 1.06–1.20 | 0.001 | 1.04 | 1.00–1.06 | 0.42 |
| LAVI > 34 mL/m2 | 1.20 | 1.11–1.36 | 0.001 | 1.06 | 1.02–1.13 | 0.042 |
| Dependent variable: HFmrEF | ||||||
| Irisin < 8.65 ng/mL | 1.37 | 1.12–1.55 | 0.001 | 1.14 | 1.02–1.77 | 0.045 |
| NT-proBNP > 2450 pmol/mL | 1.46 | 1.16–2.33 | 0.001 | 1.47 | 1.22–2.66 | 0.001 |
| LV hypertrophy | 1.09 | 1.02–1.15 | 0.001 | 1.07 | 1.00–1.12 | 0.62 |
| E/e’ > 11 units | 1.02 | 1.00–1.05 | 0.92 | - | ||
| LAVI > 34 mL/m2 | 1.10 | 1.02–1.17 | 0.001 | 1.08 | 1.02–1.19 | 0.014 |
| Dependent variable: HFrEF | ||||||
| Irisin < 8.30 ng/mL | 1.38 | 1.17–1.62 | 0.001 | 1.19 | 1.05–1.30 | 0.001 |
| NT-proBNP > 2450 pmol/mL | 1.54 | 1.14–2.70 | 0.001 | 1.47 | 1.22–2.66 | 0.001 |
| LV hypertrophy | 1.06 | 1.00–1.12 | 0.86 | - | ||
| LAVI > 34 mL/m2 | 1.11 | 1.01–1.15 | 0.048 | 1.09 | 1.02–1.16 | 0.010 |
| eGFR | 1.07 | 1.02–1.14 | 0.042 | 1.05 | 1.00–1.09 | 0.058 |
| Predictive Models | Dependent Variable: HF | |||||
|---|---|---|---|---|---|---|
| AUC | NRI | IDI | ||||
| M (95% CI) | p Value | M (95% CI) | p Value | M (95% CI) | p Value | |
| Dependent variable: HFpEF | ||||||
| Model 1 (NT-proBNP > 750 pg/mL) | 0.70 (0.63–0.76) | - | Reference | - | Reference | - |
| Model 2 (NT-proBNP > 750 pg/mL + irisin < 10.4 ng/mL) | 0.85 (0.78–0.92) | 0.001 | 0.63 (0.61–0.66) | 0.045 | 0.56 (0.51–0.60) | 0.012 |
| Dependent variable: HFmrEF | ||||||
| Model 1 (NT-proBNP > 2450 pg/mL) | 0.76 (0.68–0.85) | - | Reference | - | Reference | - |
| Model 2 (NT-proBNP > 750 pg/mL + irisin < 8.65 ng/mL) | 0.79 (0.65–0.90) | 0.16 | 0.35 (0.33–0.38) | 0.28 | 0.22 (0.21–0.24) | 0.66 |
| Dependent variable: HFmrEF | ||||||
| Model 1 (NT-proBNP > 2450 pg/mL) | 0.85 (0.76–0.94) | - | Reference | - | Reference | - |
| Model 2 (NT-proBNP > 750 pg/mL + irisin < 8.30 ng/mL) | 0.87 (0.79–0.95) | 0.64 | 0.35 (0.33–0.38) | 0.66 | 0.27 (0.22–0.31) | 0.72 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berezin, A.A.; Lichtenauer, M.; Boxhammer, E.; Stöhr, E.; Berezin, A.E. Discriminative Value of Serum Irisin in Prediction of Heart Failure with Different Phenotypes among Patients with Type 2 Diabetes Mellitus. Cells 2022, 11, 2794. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11182794
Berezin AA, Lichtenauer M, Boxhammer E, Stöhr E, Berezin AE. Discriminative Value of Serum Irisin in Prediction of Heart Failure with Different Phenotypes among Patients with Type 2 Diabetes Mellitus. Cells. 2022; 11(18):2794. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11182794
Chicago/Turabian StyleBerezin, Alexander A., Michael Lichtenauer, Elke Boxhammer, Eric Stöhr, and Alexander E. Berezin. 2022. "Discriminative Value of Serum Irisin in Prediction of Heart Failure with Different Phenotypes among Patients with Type 2 Diabetes Mellitus" Cells 11, no. 18: 2794. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11182794