
A Detailed Study to Discover the Trade between Left Atrial Blood Flow, Expression of Calcium-Activated Potassium Channels and Valvular Atrial Fibrillation

 , , , , , , , , , , , , , , and
, , , , , , , , , , , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. CT Scanning and Image Processing
2.3. Simulation Model and Calculation Method
2.4. Bioassay
2.5. Statistical Analysis
3. Results
3.1. Detection of Inlet and Outlet Velocity in LA by Doppler Ultrasonography
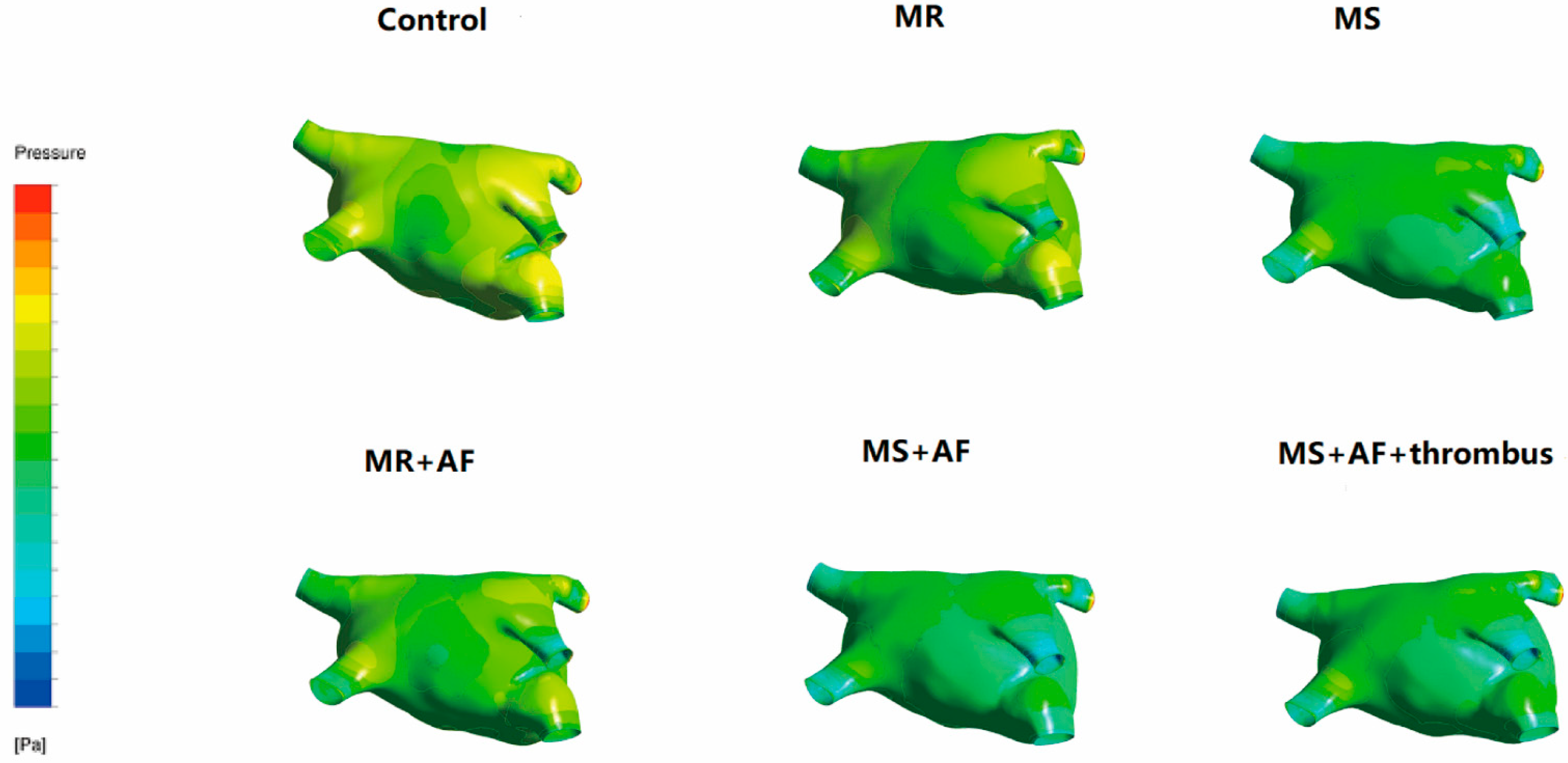
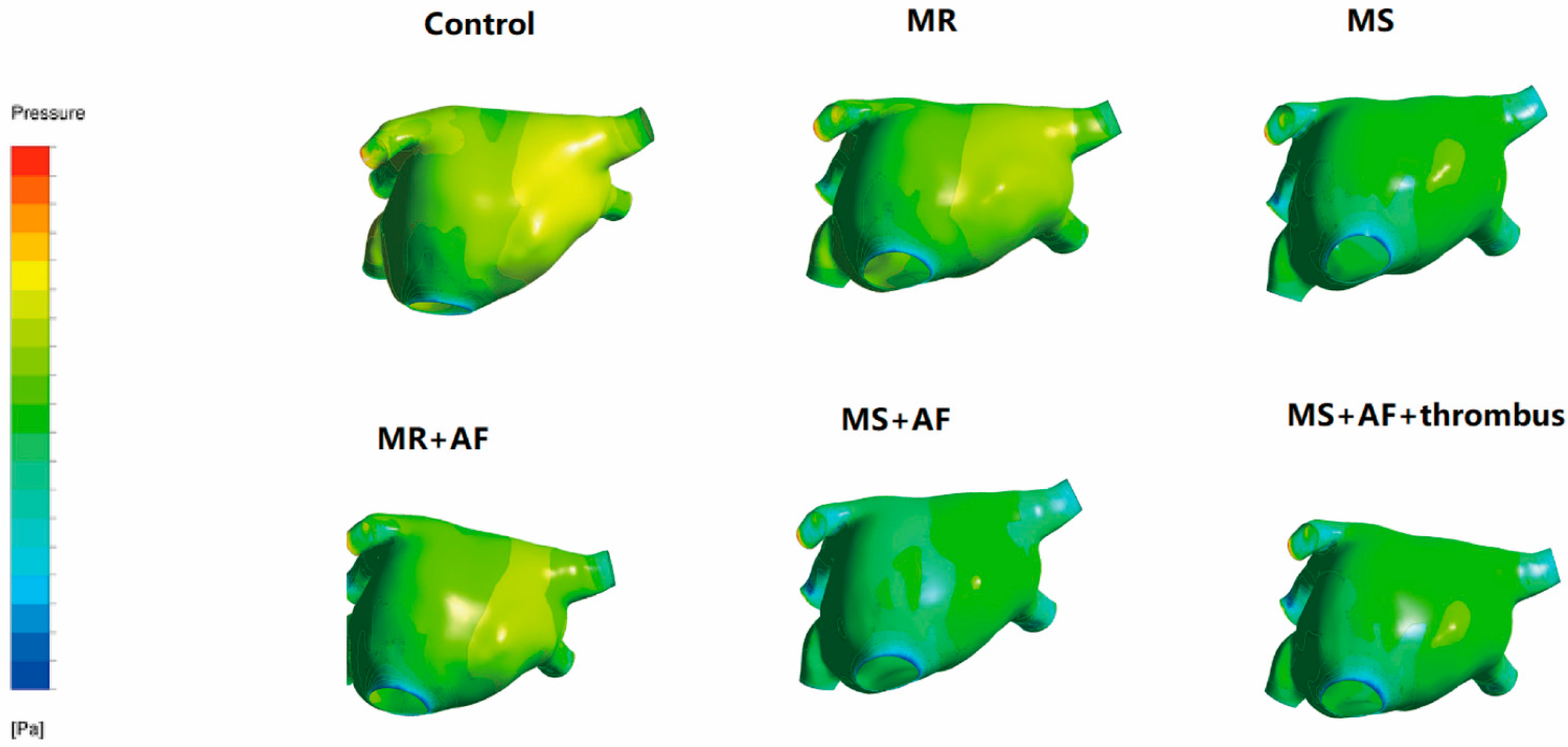
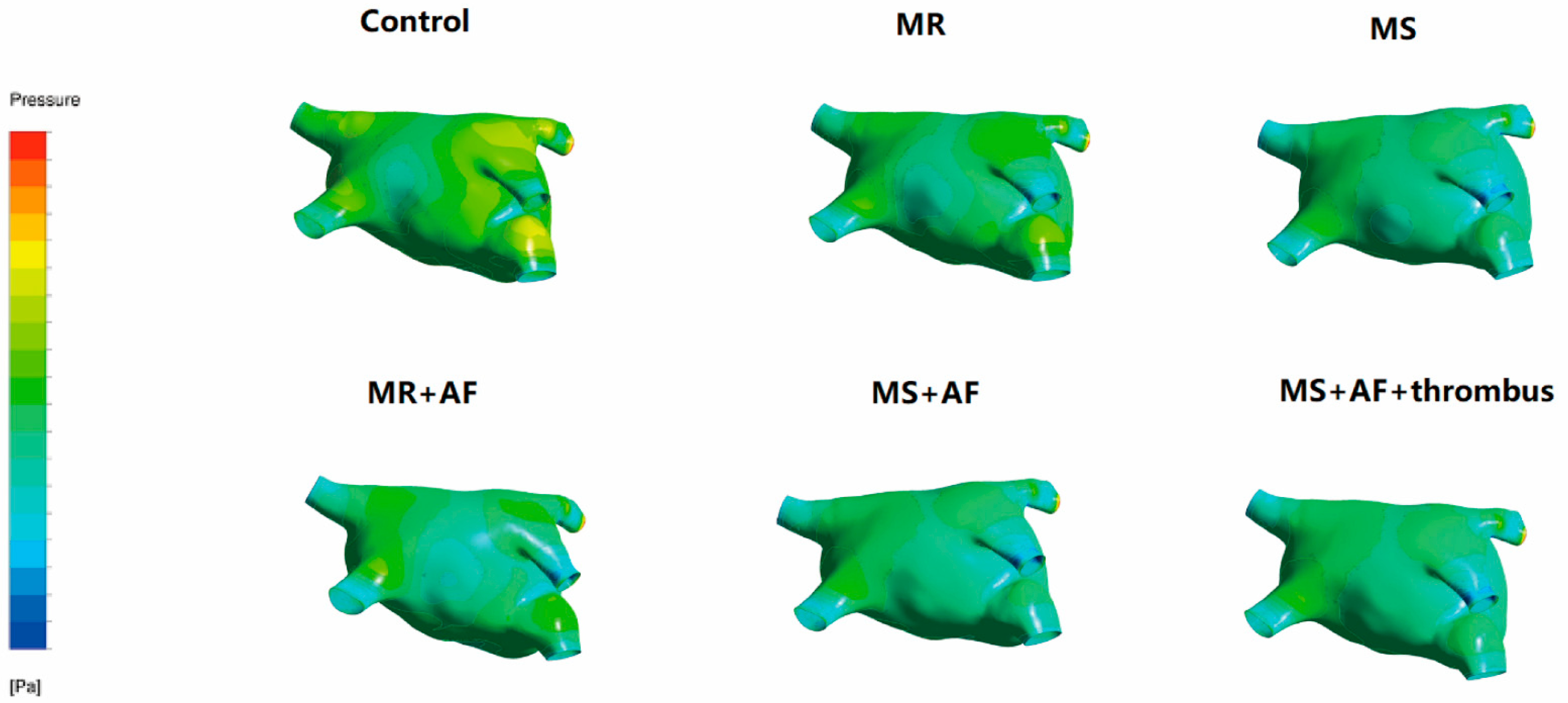
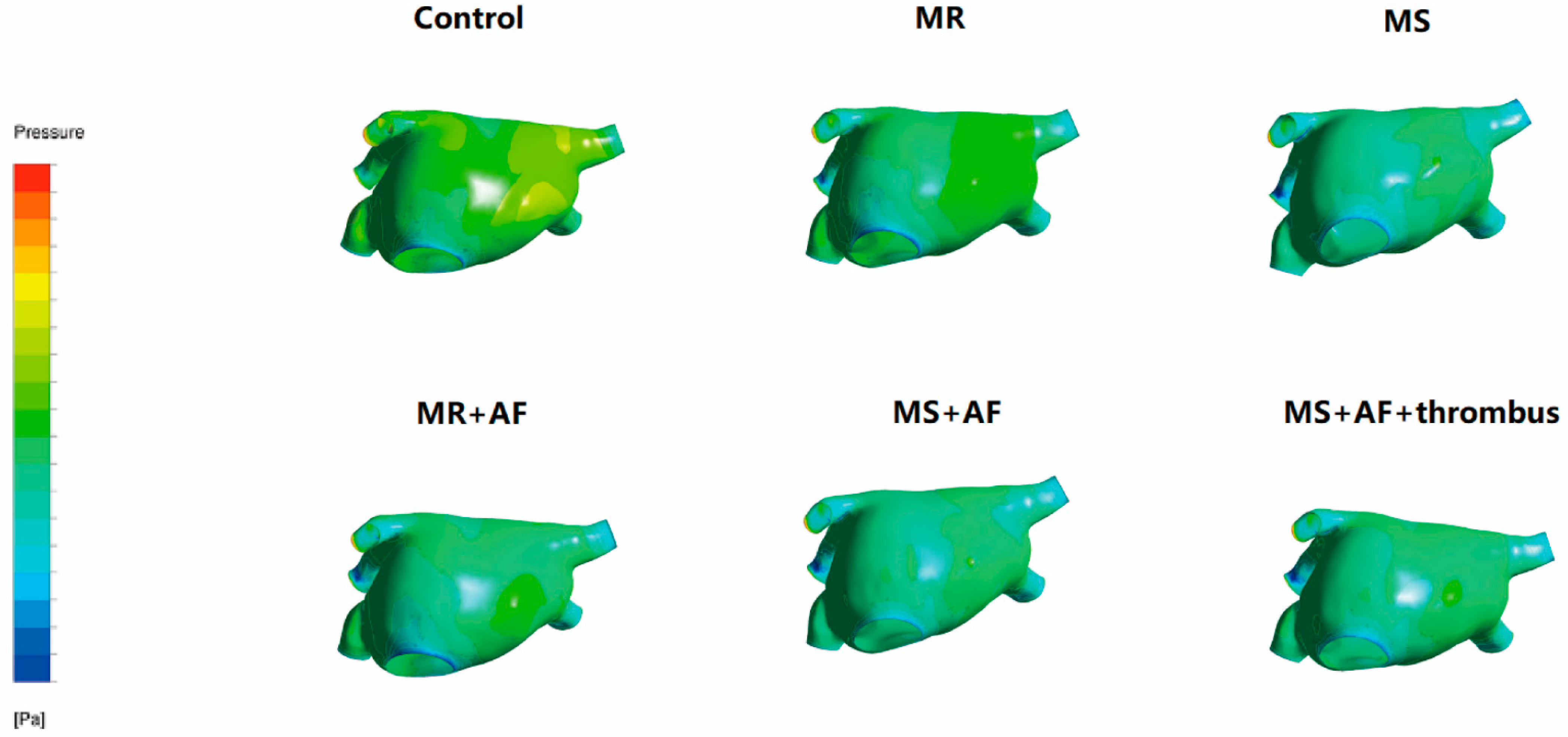
3.2. Distribution Diagram of LA Wall Pressure in Each Group
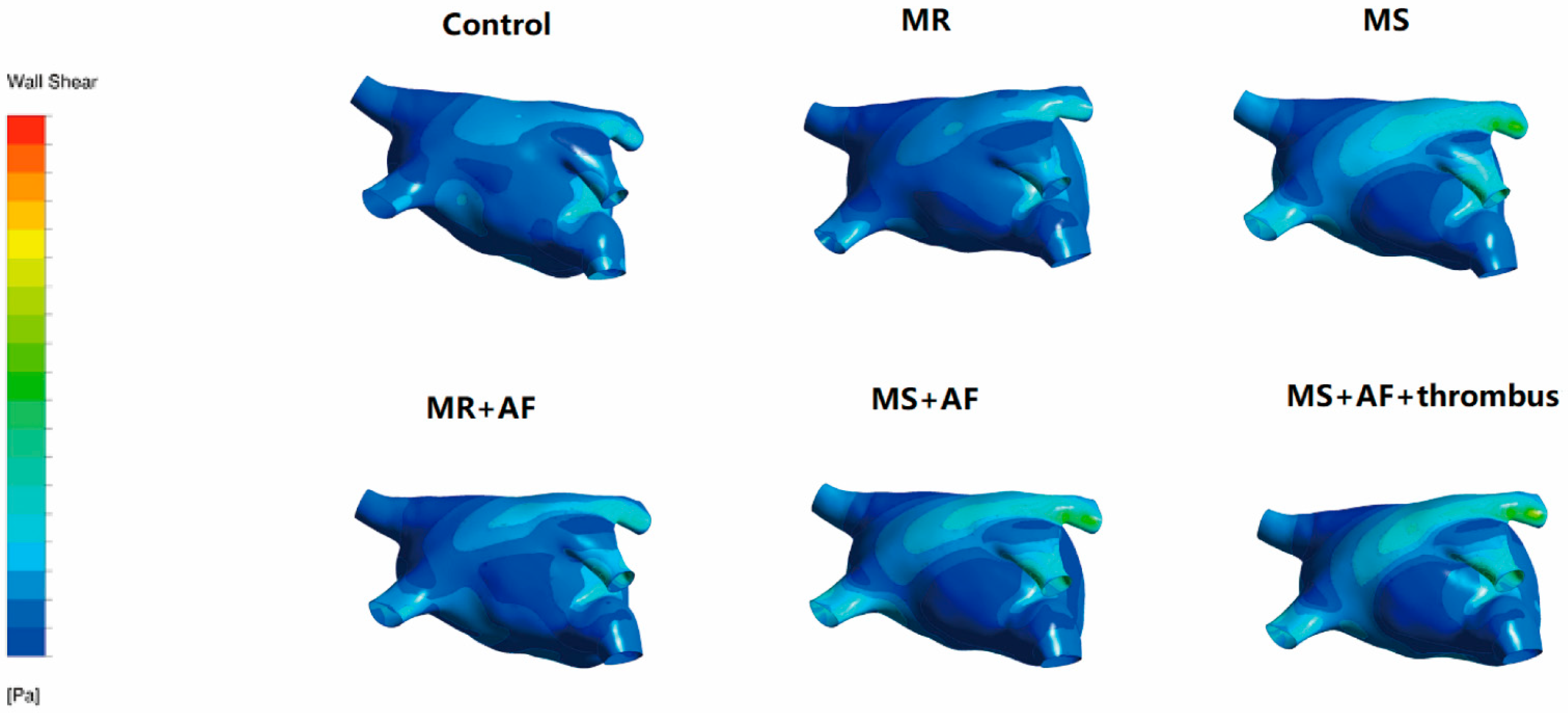
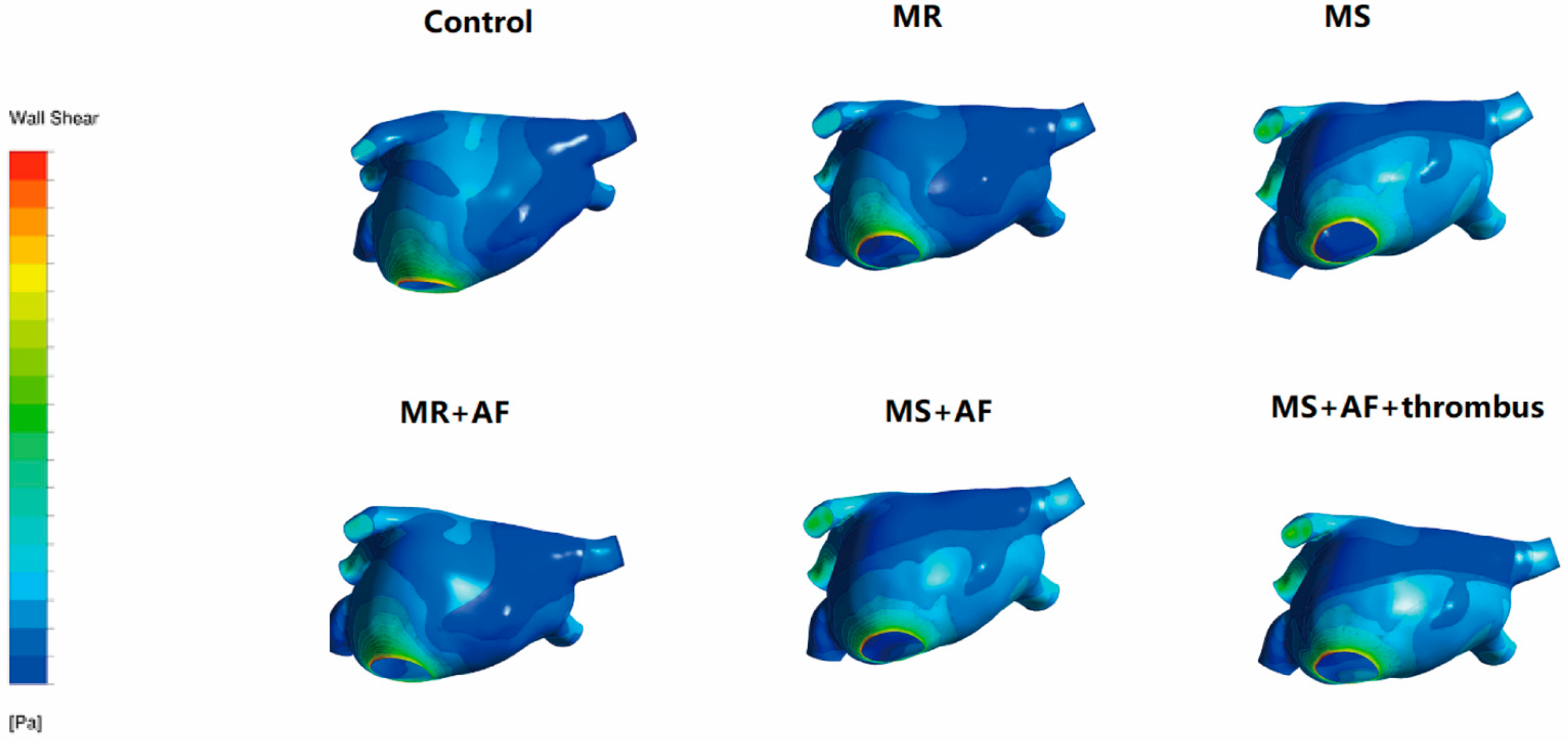
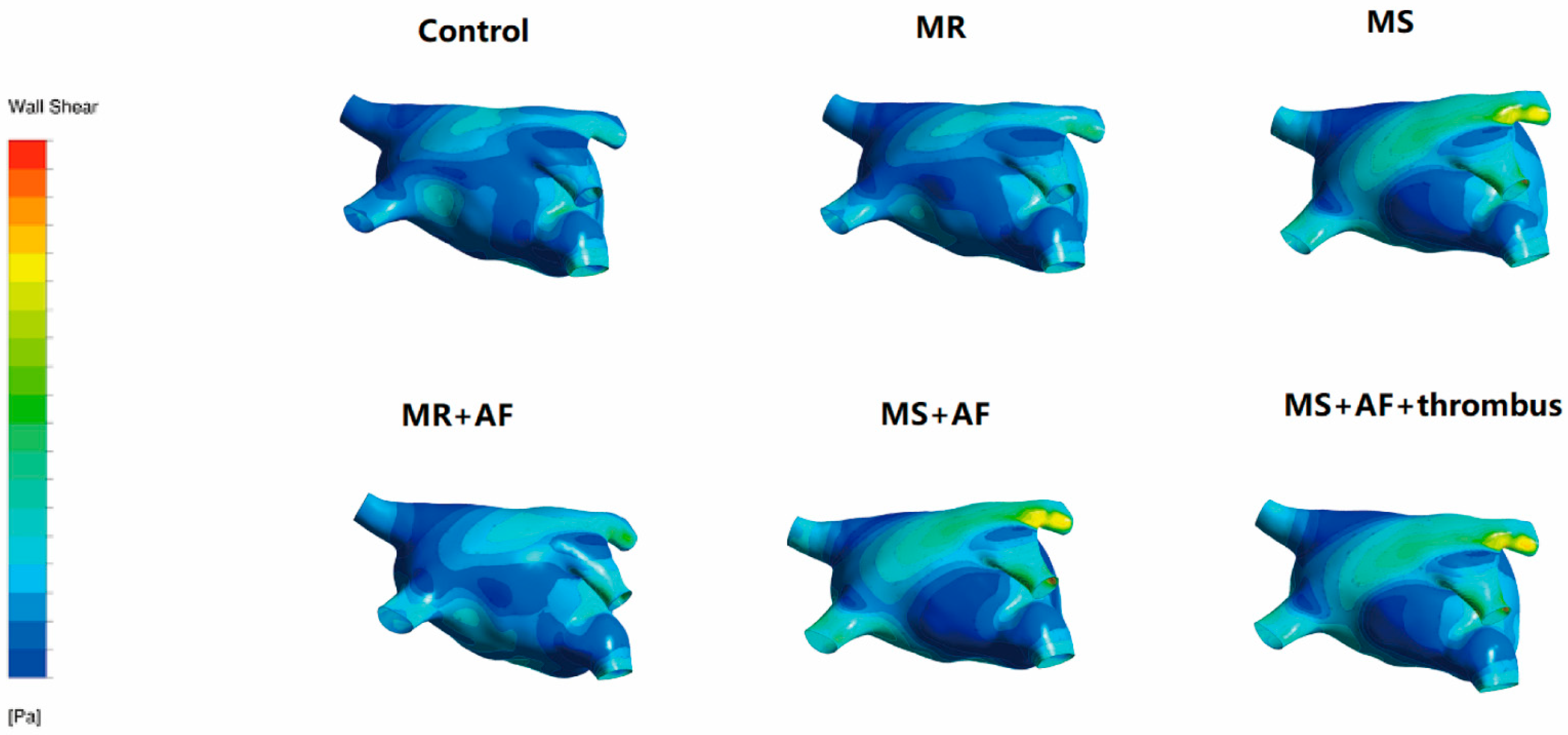
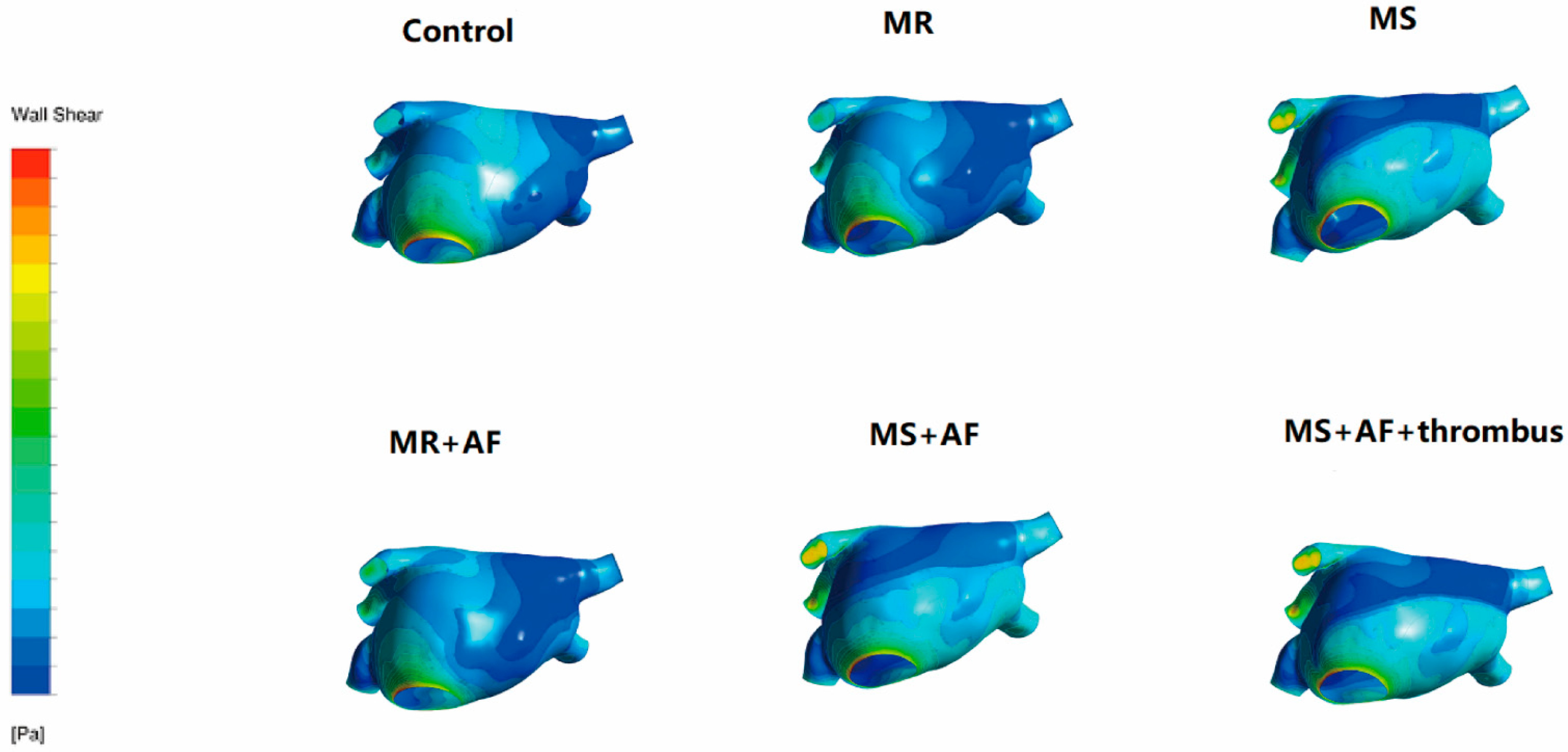
3.3. Distribution Map of TSS in Each Group in LA
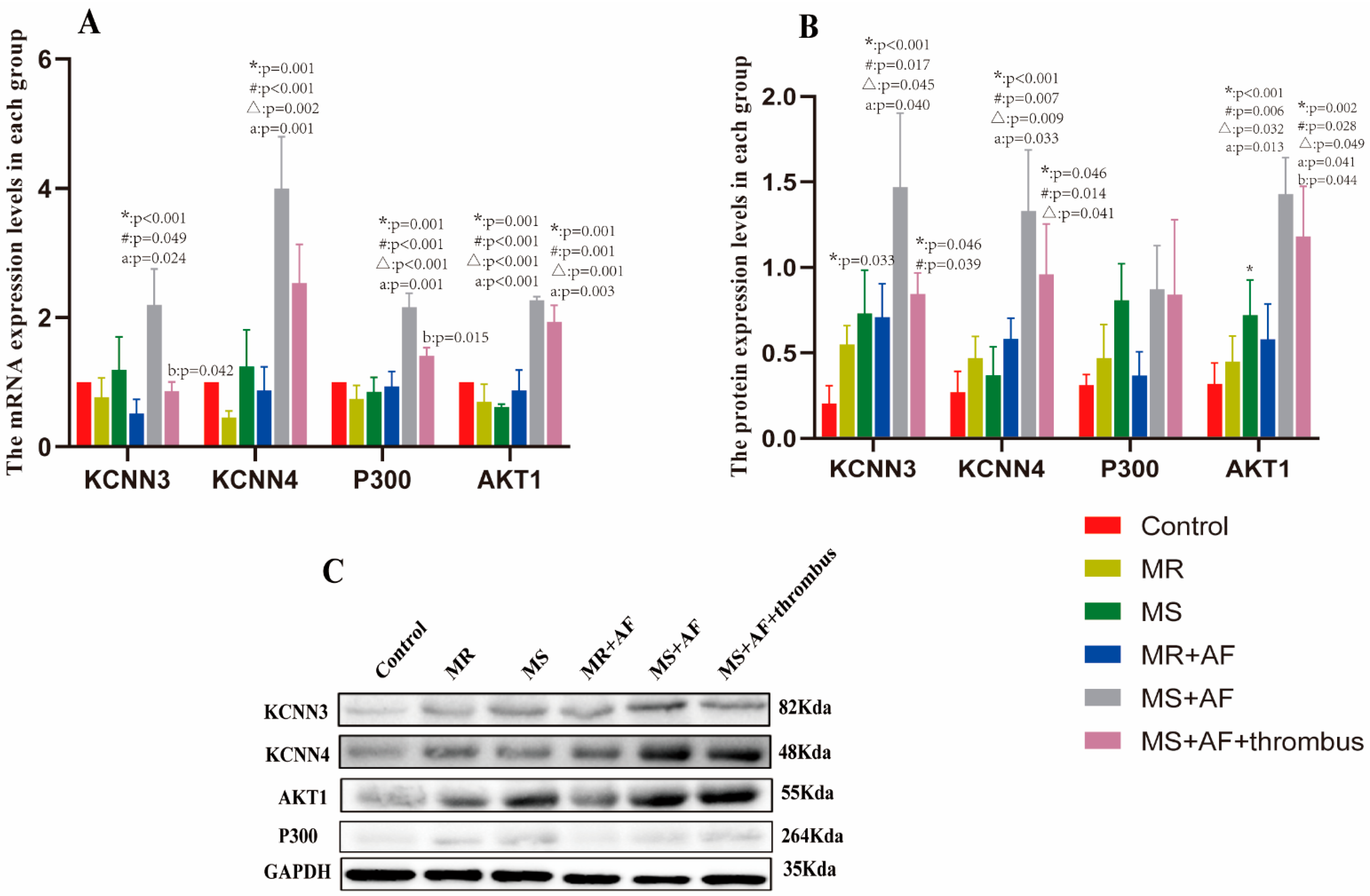
3.4. Real-Time PCR
3.5. Western Blot
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hausler, K.G.; Landmesser, U. Left atrial appendage closure in non-valvular atrial fibrillation. Herz 2019, 44, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.J.; Wolf, P.A.; Kelly-Hayes, M.; Beiser, A.S.; Kase, C.S.; Benjamin, E.J.; D’Agostino, R.B. Stroke severity in atrial fibrillation. The Framingham Study. Stroke 1996, 27, 1760–1764. [Google Scholar] [CrossRef] [PubMed]
- Goette, A.; Kalman, J.M.; Aguinaga, L.; Akar, J.; Cabrera, J.A.; Chen, S.A.; Chugh, S.S.; Corradi, D.; D’Avila, A.; Dobrev, D.; et al. EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: Definition, characterization, and clinical implication. Europace 2016, 18, 1455–1490. [Google Scholar] [CrossRef] [PubMed]
- Simo-Vicens, R.; Sauter, D.R.P.; Grunnet, M.; Diness, J.G.; Bentzen, B.H. Effect of antiarrhythmic drugs on small conductance calcium—Activated potassium channels. Eur. J. Pharmacol. 2017, 803, 118–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulati, S.; Solheim, O.; Carlsen, S.M.; Oie, L.R.; Jensberg, H.; Gulati, A.M.; Madsbu, M.A.; Giannadakis, C.; Jakola, A.S.; Salvesen, O. Risk of intracranial hemorrhage (RICH) in users of oral antithrombotic drugs: Nationwide pharmacoepidemiological study. PLoS ONE 2018, 13, e0202575. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Li, R.J.; Li, G.N.; Li, B.; Wang, Y.; Ma, R.W.; Yang, B.H.; Lu, S.L.; Zhang, G.M. Comparison between Doppler echocardiography and hot-film anemometry in measuring the turbulent shear stress downstream of artificial mitral valves: A methodological study. Chin. Med. J. 2013, 126, 2174–2178. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Yang, Q.; Yang, Y.; Yang, G.; Wan, J.; Ma, Z.; Du, L.; Sun, Y.; Zetahang, G. Laminar shear stress alters endothelial KCa2.3 expression in H9c2 cells partially via regulating the PI3K/Akt/p300 axis. Int. J. Mol. Med. 2019, 43, 1289–1298. [Google Scholar] [CrossRef]
- Diness, J.G.; Skibsbye, L.; Simó-Vicens, R.; Santos, J.L.; Lundegaard, P.; Citerni, C.; Sauter, D.R.P.; Bomholtz, S.H.; Svendsen, J.H.; Olesen, S.-P.; et al. Termination of Vernakalant-Resistant Atrial Fibrillation by Inhibition of Small-Conductance Ca(2+)-Activated K(+) Channels in Pigs. Circ. Arrhythm. Electrophysiol. 2017, 10, 005125. [Google Scholar] [CrossRef]
- Skibsbye, L.; Poulet, C.; Diness, J.G.; Bentzen, B.H.; Yuan, L.; Kappert, U.; Matschke, K.; Wettwer, E.; Ravens, U.; Grunnet, M.; et al. Small-conductance calcium-activated potassium (SK) channels contribute to action potential repolarization in human atria. Cardiovasc. Res. 2014, 103, 156–167. [Google Scholar] [CrossRef] [Green Version]
- Diness, J.G.; Sorensen, U.S.; Nissen, J.D.; Al-Shahib, B.; Jespersen, T.; Grunnet, M.; Hansen, R.S. Inhibition of small-conductance Ca2+-activated K+ channels terminates and protects against atrial fibrillation. Circ. Arrhythm. Electrophysiol. 2010, 3, 380–390. [Google Scholar] [CrossRef] [Green Version]
- Qi, X.Y.; Diness, J.G.; Brundel, B.J.; Zhou, X.B.; Naud, P.; Wu, C.T.; Huang, H.; Harada, M.; Aflaki, M.; Dobrev, D.; et al. Role of small-conductance calcium-activated potassium channels in atrial electrophysiology and fibrillation in the dog. Circulation 2014, 129, 430–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Windler, R.; de Wit, C. Perspectives: The Ca2+-dependent K+-channel KCa3.1 as a therapeutic target in cardiovascular disease. Eur. Heart J. Suppl. 2014, 16, 30–32. [Google Scholar] [CrossRef] [Green Version]
- Christophersen, P.; Wulff, H. Pharmacological gating modulation of small- and intermediate-conductance Ca(2+)-activated K(+) channels (KCa2.x and KCa3.1). Channels 2015, 9, 336–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caballero, A.D.; Lain, S. Numerical simulation of non-Newtonian blood flow dynamics in human thoracic aorta. Comput Methods Biomech. Biomed. Eng. 2015, 18, 1200–1216. [Google Scholar] [CrossRef]
- Sun, A.; Fan, Y.; Deng, X. Intentionally induced swirling flow may improve the hemodynamic performance of coronary bifurcation stenting. Catheter. Cardiovasc. Interv. 2012, 79, 371–377. [Google Scholar] [CrossRef]
- Shahcheraghi, N.; Dwyer, H.A.; Cheer, A.Y.; Barakat, A.I.; Rutaganira, T. Unsteady and three-dimensional simulation of blood flow in the human aortic arch. J. Biomech. Eng. 2002, 124, 378–387. [Google Scholar] [CrossRef]
- Zhang, G.; Shi, Y.; Tang, H.; Zhang, E.; Guo, Z.; Fan, Y.; Pu, F.; Zeng, Z. A methodological study of measuring quantitatively turbulent shear stree downstream of mitral stenosis in vivo using Doppler echocardiography. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi 2002, 19, 71–75. [Google Scholar]
- Paul, M.C.; Larman, A. Investigation of spiral blood flow in a model of arterial stenosis. Med. Eng. Phys. 2009, 31, 1195–1203. [Google Scholar] [CrossRef] [Green Version]
- Bustin, S.A.; Wittwer, C.T. MIQE: A Step Toward More Robust and Reproducible Quantitative PCR. Clin. Chem. 2017, 63, 1537–1538. [Google Scholar] [CrossRef] [Green Version]
- Jernigan, S.R.; Buckner, G.D.; Eischen, J.W.; Cormier, D.R. Finite element modeling of the left atrium to facilitate the design of an endoscopic atrial retractor. J. Biomech. Eng. 2007, 129, 825–837. [Google Scholar] [CrossRef]
- Koizumi, R.; Funamoto, K.; Hayase, T.; Kanke, Y.; Shibata, M.; Shiraishi, Y.; Yambe, T. Numerical analysis of hemodynamic changes in the left atrium due to atrial fibrillation. J. Biomech. 2015, 48, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Takai, J.; Santu, A.; Zheng, H.; Koh, S.D.; Ohta, M.; Filimban, L.M.; Lemaître, V.; Teraoka, R.; Jo, H.; Miura, H. Laminar shear stress upregulates endothelial Ca2⁺-activated K⁺ channels KCa2.3 and KCa3.1 via a Ca2⁺/calmodulin-dependent protein kinase kinase/Akt/p300 cascade. Am. J. Physiol. Heart Circ. Physiol. 2013, 305, 484–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stead, W.W.; Lin, H.S. A Vision for 21st Century Health Care and Wellness—Computational Technology for Effective Health Care—NCBI Bookshelf; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Kohler, R.; Olivan-Viguera, A.; Wulff, H. Endothelial Small- and Intermediate-Conductance K Channels and Endothelium-Dependent Hyperpolarization as Drug Targets in Cardiovascular Disease. Adv. Pharmacol. 2016, 77, 65–104. [Google Scholar] [CrossRef] [PubMed]
- Triggle, C.R.; Samuel, S.M.; Ravishankar, S.; Marei, I.; Arunachalam, G.; Ding, H. The endothelium: Influencing vascular smooth muscle in many ways. Can. J. Physiol. Pharmacol. 2012, 90, 713–738. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Yang, J.; Zhou, B.; Chen, J.; Li, J.; Li, Q.; Xiong, H.; Liu, F. NLRP3 RNAi of Injected Synoviocytes Inhibits the Inflammatory Responses in Articular Cavity and Alleviates the Injury of Articular Cartilage in a Rabbit Model. J. Biomater. Tissue Eng. 2018, 8, 1010–1016. [Google Scholar] [CrossRef]
- Shikama, N.; Lutz, W.; Kretzschmar, R.; Sauter, N.; Roth, J.F.; Marino, S.; Wittwer, J.; Scheidweiler, A.; Eckner, R. Essential function of p300 acetyltransferase activity in heart, lung and small intestine formation. EMBO J. 2003, 22, 5175–5185. [Google Scholar] [CrossRef] [Green Version]
- Manning, B.D.; Cantley, L.C. AKT/PKB signaling: Navigating downstream. Cell 2007, 129, 1261–1274. [Google Scholar] [CrossRef] [Green Version]
- Shiojima, I.; Yefremashvili, M.; Luo, Z.; Kureishi, Y.; Takahashi, A.; Tao, J.; Rosenzweig, A.; Kahn, C.R.; Abel, E.D.; Walsh, K. Akt signaling mediates postnatal heart growth in response to insulin and nutritional status. J. Biol. Chem. 2002, 277, 37670–37677. [Google Scholar] [CrossRef] [Green Version]
- Migdady, I.; Russman, A.; Buletko, A.B. Atrial Fibrillation and Ischemic Stroke: A Clinical Review. Semin. Neurol. 2021, 41, 348–364. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Gender | Age (Years) | Weight (kg) | |
|---|---|---|---|---|
| Males | Females | |||
| Control | 6 | 9 | 63.00 + 14.68 | 73.32 + 7.15 |
| MR | 7 | 8 | 55.60 + 12.03 | 67.65 + 8.42 |
| MS | 8 | 7 | 52.50 + 16.38 | 54.78 + 6.21 |
| MR+AF | 6 | 9 | 58.00 + 10.44 | 65.31 + 14.22 |
| MS+AF | 5 | 10 | 59.75 + 4.27 | 67.84 + 9.75 |
| MS+AF+ thrombus | 9 | 6 | 53.25 + 3.30 | 70.87 + 9.46 |
| p-value | 0.743 | 0.642 | ||
| ID | Forward Primer (5′–3′) | Reverse Primer (5′–3′) |
|---|---|---|
| IKCa2.3 | GACTTTCACAGACACGGACGG | GCTGCACAGCAAGCTCTTCAC |
| IKCa3.1 | CCAGGCTTCTTGTAGCACTCG | CCCCATCACATTCCTGACCAT |
| P300 | GTAGCAGCAGAGGGCAATGAG | GGCCTTGGCTTAGATGATGAG |
| AKT1 | GGTCGTGGGTCTGGAAAGAGT | GGCAAGGTGATCCTGGTGAAG |
| GAPDH | GGACCTGACCTGCCGTCTAG | GTAGCCCAGGATGCCCTTGA |
| Control (cm/s) (n = 15) | MR (cm/s) (n = 15) | MS (cm/s) (n = 15) | MR+AF (cm/s) (n = 15) | MS+AF (cm/s) (n = 15) | MS+AF+Thrombus (cm/s) (n = 15) | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Pulmonary vein | LSPV | 41.3 ± 20.91 | 41.3 ± 20.13 | 47.36 ± 10.34 | 31.36 ± 4.34 | 18.01 ± 8.47 *,#,Δ | 16.61 ± 10.19 *,#,Δ | 0.031 |
| LIPV | 41.5 ± 17.42 | 40.9 ± 18.93 | 47.54 ± 11.36 | 31.73 ± 6.19 | 18.27 ± 7.61 *,#,Δ | 18.24 ± 16.52 *,#,Δ | 0.003 | |
| RSPV | 45.2 ± 19.92 | 37.8 ± 15.52 | 48.83 ± 9.69 | 32.71 ± 8.21 | 19.69 ± 8.89 *,#,Δ | 18.19 ± 14.90 *,#,Δ | 0.024 | |
| RIPV | 42.2 ± 17.84 | 39.1 ± 17.02 | 46.57 ± 12.26 | 31.92 ± 6.78 | 17.69 ± 7.26 *,#,Δ | 17.26 ± 16.25 *,#,Δ | 0.001 | |
| LAA | 56.3 ± 15.12 | 44 ± 4.84 | 34.8 ± 10.82 | 30.7 ± 3.36 * | 18.54 ± 17.21 *,# | 11.8 ± 2.16 *,#,Δ | 0.019 | |
| Mitral orifice | 74.67 ± 16.32 | 78.36 ± 18.14 | 200.18 ± 14.89 *,# | 80.17 ± 15.49 Δ | 214.67 ± 18.26 *,#,a | 214.26 ± 16.78 *,#,a | 0.015 |
| Group | Control (n = 15) | MR (n = 15) | MS (n = 15) | MR+AF (n = 15) | MS+AF (n = 15) | MS+AF+ Thrombus (n = 15) | F | p Value |
|---|---|---|---|---|---|---|---|---|
| KCNN3 | 1 | 0.77 ± 0.51 | 1.19 ± 0.12 | 0.51 ± 0.38 | 2.19 ± 0.96 *,#,a | 0.86 ± 0.24 b | 1.635 | 0.225 |
| KCNN4 | 1 | 0.45 ± 0.17 | 1.23 ± 0.99 | 0.87 ± 0.64 | 4.00 ± 1.38 *,#,Δ,a | 3.20 ± 1.03 | 2.309 | 0.109 |
| P300 | 1 | 0.74 ± 0.37 | 0.85 ± 0.39 | 0.93 ± 0.41 | 2.16 ± 0.38 *,#,Δ,a | 1.40 ± 0.22 b | 11.624 | 0.002 |
| AKT1 | 1 | 0.69 ± 0.47 | 0.61 ± 0.79 | 0.87 ± 0.56 | 2.27 ± 0.99 *,#,Δ,a | 1.93 ± 0.45 *,#,Δ,a | 7.884 | <0.001 |
| Group | Control (n = 15) | MR (n = 15) | MS (n = 15) | MR+AF (n = 15) | MS+AF (n = 15) | MS+AF+ Thrombus (n = 15) | F | p Value |
|---|---|---|---|---|---|---|---|---|
| IKCa2.3 | 0.23 ± 0.14 | 0.55 ± 0.19 | 0.73 ± 0.44 * | 0.71 ± 0.34 | 1.47 ± 0.75 *,#,Δ,a | 0.84 ± 0.21 *,# | 10.620 | 0.042 |
| IKCa3.1 | 0.27 ± 0.21 | 0.47 ± 0.22 | 0.37 ± 0.29 | 0.58 ± 0.21 | 1.33 ± 0.62 *,#,Δ,a | 0.96 ± 0.51 *,#,Δ | 15.229 | <0.001 |
| P300 | 0.31 ± 0.11 | 0.47 ± 0.34 | 0.81 ± 0.37 | 0.37 ± 0.24 | 0.87 ± 0.44 | 0.84 ± 0.76 | 2.623 | 1.334 |
| AKT1 | 0.32 ± 0.21 | 0.45 ± 0.26 | 0.73 ± 0.37 * | 0.58 ± 0.36 | 1.43 ± 0.37 *,#,Δ,a | 1.18 ± 0.51 *,#,Δ,a,b | 11.711 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, P.; Ferdous, M.; Wang, X.; Li, G.; Ma, R.; Pan, X.; Zhang, H.; Zhang, G.; Luo, Z.; Kottu, L.; et al. A Detailed Study to Discover the Trade between Left Atrial Blood Flow, Expression of Calcium-Activated Potassium Channels and Valvular Atrial Fibrillation. Cells 2022, 11, 1383. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11091383
Shen P, Ferdous M, Wang X, Li G, Ma R, Pan X, Zhang H, Zhang G, Luo Z, Kottu L, et al. A Detailed Study to Discover the Trade between Left Atrial Blood Flow, Expression of Calcium-Activated Potassium Channels and Valvular Atrial Fibrillation. Cells. 2022; 11(9):1383. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11091383
Chicago/Turabian StyleShen, Pin, Misbahul Ferdous, Xiaoqi Wang, Guojian Li, Runwei Ma, Xiangbin Pan, Hongming Zhang, Guimin Zhang, Zhiling Luo, Lakshme Kottu, and et al. 2022. "A Detailed Study to Discover the Trade between Left Atrial Blood Flow, Expression of Calcium-Activated Potassium Channels and Valvular Atrial Fibrillation" Cells 11, no. 9: 1383. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11091383