
Lower Limb Perfusion Asymmetries in Humans at Rest and Following Activity—A Collective View
by
 , and
, and
Luis Monteiro Rodrigues
1,*,† ,
,
Clemente Gomes Rocha
1,
Margarida Esteves Florindo
1,2 and
João Gregório
1,† 1
Research Center for Biosciences and Health Technologies, Universidade Lusófona CBIOS, Campo Grande, 376, 1749-024 Lisboa, Portugal
2
Department Physiotherapy, ESSCVP—The Portuguese Red Cross Health School, 1749-024 Lisboa, Portugal
*
Author to whom correspondence should be addressed.
†
Shared senior authorship.
Symmetry 2021, 13(12), 2348; https://0-doi-org.brum.beds.ac.uk/10.3390/sym13122348
Submission received: 14 October 2021
/
Revised: 26 November 2021
/
Accepted: 1 December 2021
/
Published: 7 December 2021
(This article belongs to the Special Issue Motion, Gait Analysis and Asymmetry)
Abstract
:The significance of lower limb perfusion asymmetries remains unknown in healthy individuals. Our study aims to understand how factors such as posture, sex, age, and body weight relate to perfusion. Data from studies previously published by our group, including experiments using laser Doppler flowmetry as the gold standard for perfusion measurements in baseline, (various) challenge, and recovery phases was assembled from a total of 139 healthy participants. Body position was shown to be a primary determinant of perfusion asymmetry, especially in women. Effects of sex and age were also analyzed. In a supine position, perfusion asymmetries seemed to relate negatively in the aged group of participants, where challenge and recovery seemed to follow different processes. In the upright position, young men and women have shown comparable distributions and asymmetry ratios at baseline and recovery. In the aged group, differences between sexes were observed at baseline, but again, the course of the asymmetry ratios with challenge was essentially similar in men and women. Our analysis suggests that ageing is a critical determinant in our upright study sample, as higher baseline asymmetries and longer recoveries after challenge were linked in older males with higher body mass index (BMI).
1. Introduction
Asymmetries in arterial blood pressure between paired limbs and peripheral vascular disease (PVD) have been identified and reported for more than 100 years [1,2,3,4]. These findings were primarily obtained from limited clinical and anatomical observations; however, technological advances have enabled much more thorough study [5,6], fueled as well by the current notoriety of PVD, the third global cause of cerebrovascular stroke [7,8]. A relationship between arterial geometry of the radial, mesenteric, and femoral arteries and local hemodynamics has been established in PVD [9,10], while bilateral perfusion asymmetries in healthy young women were explained by hemodynamic and arterial morphometric changes in paired legs [9,10,11]. Recent observations on the impact of flow-related stress (shear-stress, turbulence, pulsatility) on local microcirculation suggests that all of these might differently modulate the course of pathological processes and explain the uneven perfusion impairment in these patients [12,13,14].
In the absence of vascular disease, the significance of these asymmetries has not been thoroughly investigated. Blood flow has long been primarily related to muscle mass [15], while increased levels of circulatory stress seem to produce more asymmetries and influence the development of vascular and muscle-perfusion lesions [5,6,7,8]. Direct relationships between hemodynamics and muscle activation and force generation have also been proposed to explain this scale of strength or force competence between the preferred (or dominant) and the contralateral (non-preferred) limb [16,17,18,19,20,21]. In sports medicine and rehabilitation, muscular asymmetries have gained particular relevance in regard to strength and conditioning [20]. An inverse relationship between force asymmetry and muscular performance has been reported [21,22,23], and interlimb differences have been suggested to involve higher non-contact injury risk likely accentuated by the sporting activity [21,24]. Recent data indicated that comparable amounts of blood flow are necessary for distal muscle activation in dominant and nondominant limbs, even for common activities as gait [25,26]. This “preference” asymmetry has been regarded as a variable in rehabilitation when one of the limbs is injured [16,17,18,19,20]. Footedness has been reported to follow handedness in right-handed people and assumed as a dominance criteria [20,27], although a wide variety of tests have been proposed to verify this preference [18]. Evidence also suggests that some differences are sex-related, and several reviews have focused on the impact(s) of distal perfusion impairment in known clinical conditions [28,29,30,31]. In vascular medicine, sex is regarded as an important independent variable, while hemodynamical adaptive responses to many stressors, including exercise, appear to be different between males and females [30]. Lower vasoconstriction and vascular resistance were observed in female skeletal muscle compared to males, along with an increased resistance to fatigue [32]. In the lower limb, healthy females consistently showed lower perfusion values than males, while higher skin microvascular reactivity to vascular occlusion was recently reported in the female upper limb [29,32].
To the best of our knowledge, no review has approached the physiological significance of lower limb asymmetries in regular dynamic activities in the absence of disease. Our group’s research has been centered on the identification of adaptive homeostatic responses to distal changes in microcirculatory dynamics. We have detected baseline perfusion asymmetries in healthy participants, of both sexes and different ages, submitted to different procedures meant to (temporarily) modify peripheral perfusion in the lower limb. From massage [33,34,35] to the venoarteriolar reflex [36], plantar flexion [37], unipodal squat/hemi-squat, and walking [38,39], we were able to identify and follow each hemodynamical adaptive process impacting not only local perfusion but also systemic hemodynamics in humans as in mice [36,40]. Therefore, the aim of the present analysis was to collectively assess the association of sex, age, and body mass index (BMI) with perfusion asymmetries at rest and in the recovery period after a controlled challenge from the studies published previously by our group (Table 1). A deeper understanding of the physiological significance of these asymmetries is essential, we believe, to improve our knowledge of pathogenesis and therapeutics.
2. Methods
This experimental study focuses on a convenience sample of 139 healthy participants of both sexes selected as part of separate projects involving the study of the perfusion adaptive responses to different circulatory challengers (Table 1 and Table 2).
2.1. Participants
Data were collected from participants included in previous studies regarding perfusion of the human lower limb, sharing specific predefined inclusion/non-inclusion criteria [33,34,35,36,37,38,39,40]. Participants were all non-athletes reporting regularly low physical activity and absence of any metabolic disease (diabetes, dyslipidaemia). Blood pressure (systolic—SYS; diastolic—DIA, in mmHg), height (centimeters), and weight (kg) were registered. Body mass index (BMI) was calculated. Vascular status, defined by the ankle–arm index (ABI), a common indicator of vascular health [41,42], was also registered. All participants were normotensive, non-smokers, and free of any medication or food supplementation. The consumption of vasoactive beverages (e.g., caffeine and alcohol) was restricted prior to measurements. Participants were duly informed of the objectives of each study, including all methods and technologies to be used. All study procedures followed the principles established by the Helsinki Declaration and subsequent amendments [43] and were previously approved by the Lusofona School of Health Sciences Ethics Committee.
2.2. Experiment
Table 1 summarizes the protocols of each of the previously published studies. All study measurements were taken by the same operators, in the same facilities, with controlled room temperature (25 ± 1 °C), humidity (40–60%), and light to minimize any environmental effects on the participants and measuring systems.
Regardless of the objectives within the design of each of the studies listed in Table 1, limb perfusion was always recorded in in three sequential phases:
- Phase I, corresponding to the baseline measurements; Phase II, corresponding to the application of the specific challenger in each protocol, chosen to modify perfusion; and Phase III, corresponding to recovery. Each phase had a duration of 5 to 10 min.
Challengers were categorized as follows:
- Passive—The application of superficial massage to the leg with participants in a supine position. A trained therapist applied an effleurage procedure (a variant of the so-called “Swedish Massage”) to participants lying on a padded exam table. These protocols involved 56 participants (mean age {SD} 32.64 {16.64}; 50% female). Details on these protocols are shown in Table 1 and results have been published elsewhere [31,33,34,35].
- Active—Quasi-static and dynamic movement in an upright position. With participants (n = 83, mean age {SD} 28.01 {9.10}; 50.6% female) beginning standing in the upright position, the impact of quasi-static (plantar flexion, squat, and hemi-squat) or dynamic movement (step-in-place and walking) on perfusion was analyzed. Further notes on these protocols are shown in Table 1 and complete results published elsewhere [37,38,39].
2.3. Variables of Interest
The principal common outcome variable was perfusion. All perfusion-related variables were obtained from sensors placed in both feet using various optical technologies. All studies shared the use of laser Doppler flowmetry (LDF) (Perimed PF5010 System, Stockholm, Sweden), considered the “gold standard” for perfusion evaluation [38,39]. Data were quantified in terms of blood perfusion (BP) expressed in arbitrary units (BPUs). Outcome variables such as mean perfusion from both legs and legs’ ratios were calculated. Blood pressure, height, and weight were obtained, and BMI calculated for all participants. Age and sex were obtained through the inclusion questionnaire.
For the regression models, some variables were categorized. Age was categorized in two groups—young (<30 years) and aged adults (>30 years old), as there were no differences in mean age among the participants in different protocols, but a positive correlation with perfusion was observed. Furthermore, although the men within the studies were taller and heavier than women, differences in BMI across protocols were not significant. Thus, a new variable was designed according to two BMI categories—normal weight (BMI < 25.0), and overweight/obese (BMI ≥ 25.0). A categorical variable for individual mean perfusion at baseline was also designed, dividing the individuals into quartiles (Q1 to Q4), where the lower quartiles (Q1–Q3) corresponded to individuals with lower perfusion and the 4th quartile (Q4) corresponded to individuals with the highest perfusion.
2.4. Statistical Analysis
Statistical analysis was performed with SPSS v.22.0 (IBM Corp., Armonk, NY, USA). A 95% level of confidence was adopted. Parametric (t-test for independent samples, one-way ANOVA, with post-hoc Tukey’s HSD for pairwise comparison of multiple samples) or non-parametric tests (Mann–Whitney for independent samples, Wilcoxon signed rank test for paired samples, and Kruskal–Wallis for pairwise comparison of multiple samples) were performed, depending on the previous verification of normality of data distribution by the Shapiro–Wilk test, to assess differences between variables. The effect size (r) for non-parametric tests was also computed [44] (check Supplementary Materials). Binomial logistic regressions were performed to evaluate the association of independent variables to the perfusion values and asymmetries of the lower limbs.
3. Results and Discussion
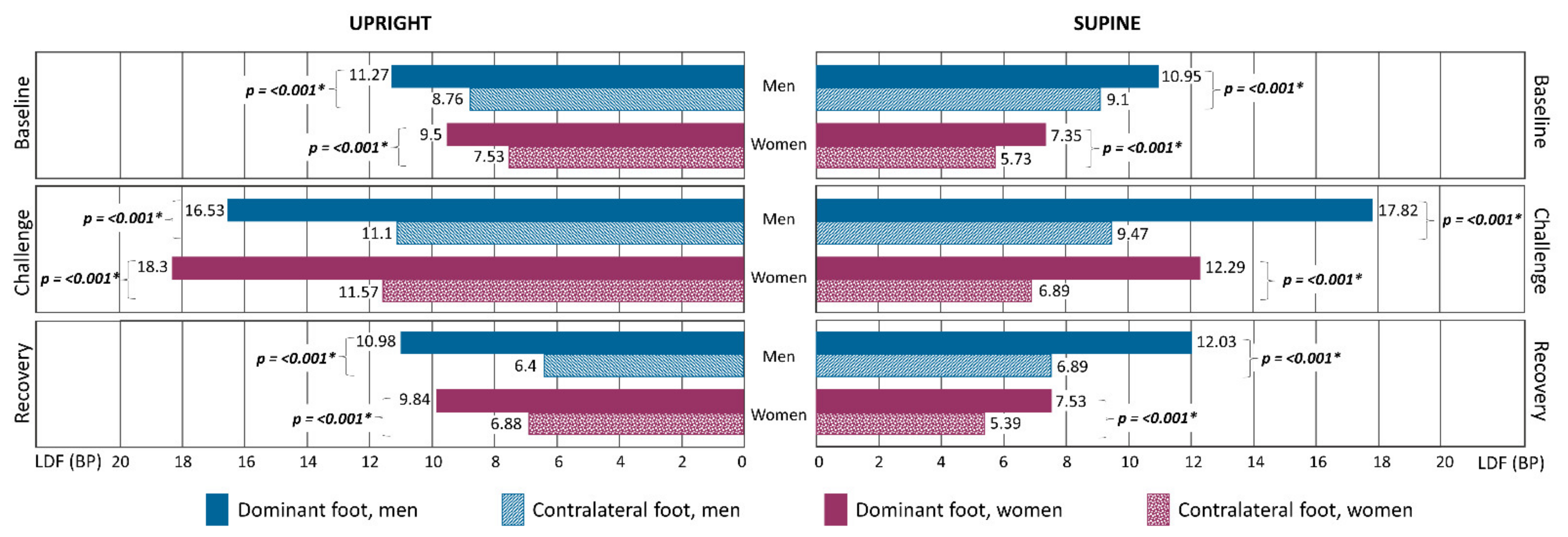
Our studies’ population shared common characteristics (Table 2). Complementary characterization of participants is shown as Supplementary Material (Tables S1–S5). Although 99.3% of participants (138/139) presented different LDF values between right and left limbs at baseline and following recovery, these differences were not statistically significant (Figure 1). A positive correlation (p < 0.001) between age and perfusion, both at baseline and recovery was found, meaning that aged individuals tend to show higher perfusion variations in the lower limbs in the absence of disease. This tendency is in line with previously published studies [7,28,35,39,45,46]. Considering the perfusion means from both limbs of each participant, regression models reveal that at baseline, higher perfusions are associated with being male, higher BMI, and being older than 30 years. However, the fully adjusted model shows that only sex is significantly associated with higher perfusions in the lower limb (Table 3). This finding implies that at baseline (or resting), men are more likely to present a higher perfusion value. On the other hand, considering the full adjusted model in the recovery phase, higher perfusions are significantly associated with older individuals (Table 3). This suggests that in recovery, older individuals are more likely to show higher perfusion values in the lower limbs.
Regarding the perfusion asymmetry, we consistently noted a higher perfusion prevalence in the right foot in men before and after the challenge in both supine and upright positions. In women, this asymmetry was less obvious (Figure 1). To facilitate comparison, a simplified measure of this asymmetry was defined for each participant as a ratio obtained by the dominant/contralateral quotient, assuming the higher foot perfusion criteria for the dominant limb versus the lower foot perfusion as the contralateral limb [18,19,27]. To assess the relative influence of different variables on these perfusion asymmetries, we categorized the perfusion asymmetry ratio into quartiles, where the first to third quartiles (Q1–Q3) represent individuals with the lowest asymmetries and the fourth quartile (Q4) represents individuals with the highest asymmetries. The regression model for this new variable shows that individuals in the supine position were more likely to show higher ratios, i.e., greater limb asymmetries (OR: 2.957 [1.343–6.510]; p = 0.007).
Body position was regarded as a variable in the assessment of skin perfusion, as we analyzed and compared data from supine and upright positions. However, regression models adjusted for body position demonstrated that none of our variables of interest were significantly associated with higher ratios at baseline (data not shown). Taking this analysis further, however, we found a broadly similar profile in men and women when considering all individuals and the evolution of their perfusion asymmetries during the applied protocols (Figure 2). We noted that the upright position reduces the median in both sexes in all experimental phases. These reductions are particularly noted at baseline and clearly expressive in women (p = 0.009). Moreover, in the upright position, data from men was apparently more homogeneous in the other experimental phases compared to women, whose data dispersion was much more expressive in all phases (Figure 2). We know that postural changes from upright to seated or horizontal involve huge variations of pressure in the lower limbs [32,47,48]. No matter the known physiological differences between sexes at baseline, our analysis has shown that challenges evoked a similar evolution of pre-existing perfusion asymmetries in both men and women. The lower stress conditions of decubitus (supine) position in the lower limb allow the physiological adaptive mechanisms to function adequately no matter the anatomo-physiological differences between sexes. In the upright position, the response to the increase of circulatory stress seems to be better managed in men as shown by the data homogeneity and faster recovery than women.
Although the regression model for asymmetry revealed no significant differences (Table 3), a deeper look into this overview suggests that these asymmetries resolve differently according to age and sex. Baseline in supine positions have shown similar medians in younger individuals, although more homogeneous in men (Figure 3a). Age changed these baseline distributions, moving medians in opposite directions with a marked dispersion in men (Figure 3b). The evolution pattern in challenge and recovery phases revealed a similar profile in both sexes in young individuals (Figure 3a), in line with the observations illustrated in Figure 2. Again, the reduction of circulatory stress likely facilitated the adaptive mechanisms involved, although some differences persist as young men seemed to recover faster than young women. In the aged group, these profiles changed considerably. In men, asymmetries increased continuously through recovery, while in women the asymmetry ratio decreased (Figure 3b).
In the upright position, young men and women had comparable distributions and asymmetry ratios at baseline that increased similarly with challenge. In recovery, female values were already near baseline, which again suggests that the adaptive response to challenge is different in young men compared to young women (Figure 4a). In contrast, inverse asymmetry medians were observed in the aged group at baseline, higher for men and lower for women, with inversed data dispersion around the median (Figure 4b). However, in both sexes, the challenge reduced data dispersion and increased the median asymmetry ratio, followed by a similar decrease in recovery (Figure 4). Gender-related differences have been associated with the prevalence of vascular disease (e.g., PAD, Raynaud disease) [8,28,49,50] and with the vascular risk associated with diabetes [51,52], although the potential mechanisms involved have not been identified. Recent research suggests that the physiological response to long-term exercise programs vary between males and females [30]. Our data seem to indicate that in the presence of these (baseline) differences, the response of physiological systems to different challenges is broadly similar between sexes (Figure 2, Figure 3 and Figure 4). Significant research has been published on the effect of age, recognizing its role as a main variable in cardiovascular health [39,45,46]. Recent data have shown that perfusion is age dependent, and that movement reduces dorsal foot perfusion in depth, depending on the movement intensity [39]. Our current analysis reveals that posture substantially modifies the evolution of perfusion asymmetries during the experiments in aged individuals, especially in the supine position. However, the upright profiles from males and females were very similar (Figure 4).
Some limitations should be recognized in this study: (a) our regression results cannot be extrapolated to the general population as they only reflect the convenience sample gathered from our studies in those specific experimental conditions; it is fair to think this modest sample size may have played a role in limiting the significance of some of the statistical comparisons conducted—a post-hoc power analysis revealed that both for supine (n = 56) and upright (n = 83) positions, the sample size was adequate for detecting differences in perfusion across phases (power of 95.9% and 99.8%, respectively); (b) dominance seems to have paramount relevance, recommending its verification by reference methods; and finally (c) flow-related variables were obtained with single-point measurements of LDF in different sites in the foot. To this final limitation, however, all results were confirmed by the simultaneous application of other technologies (data available within each published paper) [33,34,35,36,37,38,39,40].
4. Conclusions
Lower limb intra- and interindividual perfusion baseline differences exist, associated with sex and age as main determinants. Our results suggest that essential (perfusion) adaptive mechanisms seem to operate similarly in the absence of disease. Nevertheless, in the present sample analysis, ageing was the most important determinant when upright, where older individuals (principally males, with higher BMI values) show higher asymmetry ratios at baseline and longer recoveries after challenge. The pathophysiological significance and potential predictive utility of these limb asymmetries should be further explored.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/sym13122348/s1, Table S1. Participant characteristics—differences between protocols by sex; Table S2. Participant characteristics—differences between men and women; Table S3. Perfusion differences between right and left limbs; Table S4. Differences of LDF perfusion values; Table S5. Differences of LDF perfusion values by body position.
Author Contributions
Conceptualization, L.M.R.; Data curation, J.G.; Investigation, C.G.R. and M.E.F.; Methodology, L.M.R., C.G.R. and M.E.F.; Software, J.G.; Supervision, L.M.R.; Validation, C.G.R. and M.E.F.; Writing—original draft, L.M.R.; Writing—review and editing, J.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by FCT—Foundation for Science and Technology, I.P., grants UIDB/04567/2020 and UIDP/04567/2020. João Gregório is funded FCT—Foundation for Science and Technology, I.P., with the grant CEEC/CBIOS/EPH/2018 for Scientific Employment Stimulus.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Lusofona School of Health Sciences Ethics Committee (approval codes: CE 01/2012.03 from November 2012; CE 03/2013.12 from February 2013; CE P03.20/2020 from May 2020).
Informed Consent Statement
Not applicable.
Acknowledgments
To all participants and to all CBIOS researchers involved in the reported studies.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bouley, J.F. Claudication Intermittent des Membres Posterieurs, determinee par L’obliteration des Arteres Femorales. Recl. Méd. Vét. 1831, 8, 517–527. [Google Scholar]
- Hensen, H. Beitrage zur Physiologie und pathologie des Blutdrucks (Contributions to the physiology and pathology of blood pressure). Dtsch. Arch. Med. 1900, 67, 436. [Google Scholar]
- Cheatle, T.R.; Coleridge-Smith, P.D.; Scurr, J.H. The investigation of peripheral vascular disease—A historical perspective. Vasc. Med. Rev. 1991, 2, 101–109. [Google Scholar] [CrossRef]
- Zusmanovich, F.N.; Elizarova, S.N. Dinamika perfuzionnogo davleniia v nizhnikh konechnostiakh v pokoe i posle fizicheskoĭ nagruzki (Perfusion pressure dynamics in lower extremities at rest and after exercise). Fiziol. Cheloveka 2002, 28, 133–136. [Google Scholar] [PubMed]
- Seder, J.S.; Botvinick, E.H.; Rahimtoola, S.H.; Goldstone, J.; Price, D.C. Detecting and localizing peripheral arterial disease: Assessment of 201Tl scintigraphy. Am. J. Roentgenol. 1981, 137, 373–380. [Google Scholar] [CrossRef] [Green Version]
- Collins, R.; Burch, J.; Cranny, G.; Aguiar-Ibáñez, R.; Craig, D.; Wright, K.; Berry, E.; Gough, M.; Kleijnen, J.; Westwood, M. Duplex ultrasonography, magnetic resonance angiography, and computed tomography angiography for diagnosis and assessment of symptomatic, lower limb peripheral arterial disease: Systematic review. BMJ 2007, 334, 1257. [Google Scholar] [CrossRef] [Green Version]
- Rodgers, J.L.; Jones, J.; Bolleddu, S.I.; Vanthenapalli, S.; Rodgers, L.E.; Shah, K.; Karia, K.; Panguluri, S.K. Cardiovascular Risks Associated with Gender and Aging. J. Cardiovasc. Dev. Dis. 2019, 6, 19. [Google Scholar] [CrossRef] [Green Version]
- Eid, M.A.; Mehta, K.S.; Goodney, P.P. Epidemiology of peripheral artery disease. Semin. Vasc. Surg. 2021, 34, 38–46. [Google Scholar] [CrossRef]
- Wood, N.B.; Zhao, S.Z.; Zambanini, A.; Jackson, M.; Gedroyc, W.; Thom, S.A.; Hughes, A.D.; Xu, X.Y. Curvature and tortuosity of the superficial femoral artery: A possible risk factor for peripheral arterial disease. J. Appl. Physiol. 2006, 101, 1412–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisen, L.A.; Minami, T.; Sekiguchi, H.; Berger, J.S.; Mayo, P.; Narasimhan, M. Ultrasound demonstration of asymmetry between the left and right femoral and radial arteries. Chest 2006, 130, 201S. [Google Scholar] [CrossRef]
- Marcinkevics, Z.; Lukstina, Z.; Rubins, U.; Grabovskis, A.; Aivars, J.I. Bilateral difference of superficial and deep femoral artery haemodynamic and anatomical parameters. Artery Res. 2013, 7, 201–210. [Google Scholar] [CrossRef]
- Mei, C.C.; Zhang, J.; Jing, H.X. Fluid mechanics of Windkessel effect. Med. Biol. Eng. Comput. 2018, 56, 1357–1366. [Google Scholar] [CrossRef] [PubMed]
- Climie, R.E.; Gallo, A.; Picone, D.S.; Di Lascio, N.; van Sloten, T.T.; Guala, A.; Mayer, C.C.; Hametner, B.; Bruno, R.M. Measuring the Interaction Between the Macro- and Micro-Vasculature. Front. Cardiovasc. Med. 2019, 6, 169. [Google Scholar] [CrossRef] [Green Version]
- Cracowski, J.L.; Roustit, M. Human Skin Microcirculation. Compr. Physiol. 2020, 10, 1105–1154. [Google Scholar] [CrossRef] [PubMed]
- Siegel, M.E.; Siemsen, J.K. A new noninvasive approach to peripheral vascular disease: Thallium-201 leg scans. Am. J. Roentgenol. 1978, 131, 827–830. [Google Scholar] [CrossRef] [Green Version]
- Bishop, C.; Read, P.; Chavda, S.; Turner, A. Asymmetries of the Lower Limb: The Calculation Conundrum in Strength Training and Conditioning. Strength Cond. J. 2016, 38, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Vaisman, A.; Guiloff, R.; Rojas, J.; Delgado, I.; Figueroa, D.; Calvo, R. Lower Limb Symmetry: Comparison of Muscular Power Between Dominant and Nondominant Legs in Healthy Young Adults Associated with Single-Leg-Dominant Sports. Orthop. J. Sports Med. 2017, 5, 2325967117744240. [Google Scholar] [CrossRef] [PubMed]
- Van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.G.; van Cingel, R.E.H. How to determine leg dominance: The agreement between self-reported and observed performance in healthy adults. PLoS ONE 2017, 12, e0189876. [Google Scholar]
- Bellenfant, K.B.; Robbins, G.L.; Rogers, R.R.; Kopec, T.J.; Ballmann, C.G. Effects of Dominant and Nondominant Limb Immobilization on Muscle Activation and Physical Demand during Ambulation with Axillary Crutches. J. Funct. Morphol. Kinesiol. 2021, 6, 16. [Google Scholar] [CrossRef]
- Lanshammar, K.; Ribom, E.L. Differences in muscle strength in dominant and non-dominant leg in females aged 20–39 years—A population-based study. Phys. Ther. Sport 2011, 12, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Maloney, S.J. The Relationship between Asymmetry and Athletic Performance: A Critical Review. J. Strength Cond. Res. 2019, 33, 2579–2593. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.R.; Ratamess, N.A.; Klatt, M.; Faigenbaum, A.D.; Kang, J. Do Bilateral Power Deficits Influence Direction-Specific Movement Patterns? Res. Sports Med. 2007, 15, 125–132. [Google Scholar] [CrossRef]
- Bell, D.R.; Sanfilippo, J.L.; Binkley, N.; Heiderscheit, B.C. Lean mass asymmetry influences force and power asymmetry during jumping in collegiate athletes. J. Strength Cond. Res. 2014, 28, 884–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heil, J.; Loffing, F.; Büsch, D. The Influence of Exercise-Induced Fatigue on Inter-Limb Asymmetries: A Systematic Review. Sports Med. Open 2020, 6, 39. [Google Scholar] [CrossRef] [PubMed]
- Kadoguchi, T.; Horiuchi, M.; Kinugawa, S.; Okita, K. Heterogeneity in the vasodilatory function of individual extremities. Vascular 2020, 28, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Jungmann, P.M.; Pfirrmann, C.; Federau, C. Characterization of lower limb muscle activation patterns during walking and running with Intravoxel Incoherent Motion (IVIM) MR perfusion imaging. Magn. Reson. Imaging 2019, 63, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Peter, M.; Durding, B.M. Footedness of left- and right-handers. Am. J. Psychol. 1979, 92, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Srivaratharajah, K.; Abramson, B.L. Women and Peripheral Arterial Disease: A Review of Sex Differences in Epidemiology, Clinical Manifestations, and Outcomes. Can. J. Cardiol. 2018, 34, 356–361. [Google Scholar] [CrossRef]
- Huxley, V.H.; Kemp, S.S. Sex-Specific Characteristics of the Microcirculation. Adv. Exp. Med. Biol. 2018, 1065, 307–328. [Google Scholar] [CrossRef]
- Ansdell, P.; Thomas, K.; Hicks, K.M.; Hunter, S.K.; Howatson, G.; Goodall, S. Physiological sex differences affect the integrative response to exercise: Acute and chronic implications. Exp. Physiol. 2020, 105, 2007–2021. [Google Scholar] [CrossRef]
- Gregório, J.; Silva., H.; Rocha, C.; Rodrigues, L.M. Perfusion is sex related but response to massage evokes the same hemodynamic adaptation in both sexes—Results from an exploratory factor analysis. Proceed Physioma 2019—1st Int Meeting Portuguese Physiological Society. Biomed. Biopharm. Res. 2019, 16, 31–32. [Google Scholar] [CrossRef]
- Bassareo, P.P.; Crisafulli, A. Gender Differences in Hemodynamic Regulation and Cardiovascular Adaptations to Dynamic Exercise. Curr. Cardiol. Rev. 2020, 16, 65–72. [Google Scholar] [CrossRef]
- Rocha, C.; Macedo, A.; Nuno, S.; Silva, H.; Ferreira, H.; Rodrigues, L.M. Exploring the perfusion modifications occurring with massage in the human lower limbs by non-contact polarized spectroscopy. Biomed. Biopharm. Res. 2018, 15, 196–204. [Google Scholar] [CrossRef]
- Rocha, C.; Silva, H.; Ferreira, H.; Rodrigues, L.M. Comparing the effects of human hind limb massage by analysis of Laser Doppler flowmetry and Photoplethysmography signal components using the wavelet transform. Biomed. Biopharm. Res. 2018, 15, 70–81. [Google Scholar] [CrossRef]
- Rodrigues, L.M.; Rocha, C.; Ferreira, H.Á.; Silva, H.N. Lower limb massage in humans increases local perfusion and impacts systemic hemodynamics. J. Appl. Physiol. 2020, 128, 1217–1226. [Google Scholar] [CrossRef] [PubMed]
- Silva, H.; Ferreira, H.Á.; da Silva, H.P.; Monteiro Rodrigues, L. The Venoarteriolar Reflex Significantly Reduces Contralateral Perfusion as Part of the Lower Limb Circulatory Homeostasis in vivo. Front. Physiol. 2018, 9, e1123. [Google Scholar] [CrossRef] [Green Version]
- Florindo, M.; Silva, H.; Rodrigues, L.M. Impact of the isometric contraction of the calf on the local microcirculation. Biomed. Biopharm. Res. 2017, 14, 179–186. [Google Scholar] [CrossRef]
- Nuno, S.; Florindo, M.; Silva, H.; Rodrigues, L.M. Studying the impact of different body positioning, squatting, and unipodal flexion on perfusion in the lower limb—An exploratory approach complemented with optical spectroscopy (TiVi). Biomed. Biopharm. Res. 2020, 17, 187–196. [Google Scholar] [CrossRef]
- Florindo, M.; Nuno, S.L.; Rodrigues, L.M. Lower limb dynamic activity significantly reduces foot skin perfusion- exploring data with different optical sensors in age-grouped healthy adults. Skin Pharmacol. Physiol. 2021. [Google Scholar] [CrossRef]
- Rodrigues, L.M.; Silva, H.; Ferreira, H.; Renault, M.-A.; Gadeau, A.-P. Observations on the perfusion recovery of regenerative angiogenesis in an ischemic limb model under hyperoxia. Physiol. Rep. 2018, 6, e13736. [Google Scholar] [CrossRef]
- Aboyans, V.; Criqui, M.H.; Abraham, P.; Allison, M.A.; Creager, M.A.; Diehm, C.; Fowkes, F.G.; Hiatt, W.R.; Jönsson, B.; Lacroix, P.; et al. American Heart Association Council on Peripheral Vascular Disease, Council on Epidemiology and Prevention, Council on Clinical Cardiology, Council on Cardiovascular Radiology and Intervention, and Council on Cardiovascular Surgery and Anesthesia. Measurement and interpretation of the ankle-brachial index: A scientific statement from the American Heart Association. Circulation 2012, 126, 2890–2909. [Google Scholar] [CrossRef] [Green Version]
- Czell, D.; Schreier, R.; Rupp, I.R.; Eberhard, S.; Colombo, G.; Dietz, V. Influence of passive leg movements on blood circulation on the tilt table in healthy adults. JNER 2004, 1, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Gelder, L.M.A.; Angelini, L.; Buckley, E.E.; Mazzà, C. A Proposal for a Linear Calculation of Gait Asymmetry. Symmetry 2021, 13, 1560. [Google Scholar] [CrossRef]
- Abiri, B.; Vafa, M. Dietary Restriction, Cardiovascular aging and age-related cardiovascular diseases: A review of the evidence. In Reviews on Biomarker Studies in Aging and Anti-Aging Research. Advances in Experimental Medicine and Biology; Guest, P., Ed.; Springer: Cham, Switzerland, 2019; Volume 1178. [Google Scholar] [CrossRef]
- Xu, X.; Wang, B.; Ren, C.; Hu, J.; Greenberg, D.A.; Chen, T.; Xie, L.; Jin, K. Age-related Impairment of Vascular Structure and Functions. Aging Dis. 2017, 8, 590–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shinozaki, N. Effect of body position on skin perfusion pressure in patients with severe peripheral arterial disease. Circ. J. 2012, 76, 2863–2866. [Google Scholar] [CrossRef] [Green Version]
- Kawasaki, T.; Uemura, T.; Matsuo, K.; Masumoto, K.; Harada, Y.; Chuman, T.; Murata, T. The effect of different positions on lower limbs skin perfusion pressure. Indian J. Plast. Surg. 2013, 46, 508–512. [Google Scholar] [CrossRef]
- Egorova, N.; Vouyouka, A.G.; Quin, J.; Guillerme, S.; Moskowitz, A.; Marin, M.; Faries, P.L. Analysis of gender-related differences in lower extremity peripheral arterial disease. J. Vasc. Surg. 2010, 51, 372–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, S.A.E.; Muntner, P.; Woodward, M. Sex Differences in the Prevalence of, and Trends in, Cardiovascular Risk Factors, Treatment, and Control in the United States, 2001 to 2016. Circulation 2019, 139, 1025–1035. [Google Scholar] [CrossRef] [PubMed]
- Manevska, N.; Gjorceva, D.P.; Ahmeti, I.; Todorovska, L.; Stojanoski, S.; Kocovska, M.Z. Tissue-Muscle Perfusion Scintigraphy of the Lower Limbs in a Patient with Type 2 Diabetes Mellitus and Peripheral Arterial Disease. Mol. Imaging Radionucl. Ther. 2016, 25, 42–46. [Google Scholar] [CrossRef]
- De Ritter, R.; de Jong, M.; Vos, R.C.; van der Kallen, C.; Sep, S.; Woodward, M.; Stehouwer, C.; Bots, M.L.; Peters, S. Sex differences in the risk of vascular disease associated with diabetes. Biol. Sex Differ. 2020, 11, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Perfusion differences between dominant and contralateral (non-dominant) limbs obtained in each phase (baseline, challenge, and recovery) of the experimental protocols. Median blood perfusion values registered via LDF BP (blood perfusion) are shown by sex considering body position (supine or upright). Statistical differences were assessed by the Wilcoxon signed rank test; * p < 0.05.
Figure 1.
Perfusion differences between dominant and contralateral (non-dominant) limbs obtained in each phase (baseline, challenge, and recovery) of the experimental protocols. Median blood perfusion values registered via LDF BP (blood perfusion) are shown by sex considering body position (supine or upright). Statistical differences were assessed by the Wilcoxon signed rank test; * p < 0.05.

Figure 2.
Evolution of the perfusion asymmetry defined by the dominant/contralateral limb ratio in all male (a) and female (b) participants during the experimental supine and upright protocols course; * p < 0.05 (see text).
Figure 2.
Evolution of the perfusion asymmetry defined by the dominant/contralateral limb ratio in all male (a) and female (b) participants during the experimental supine and upright protocols course; * p < 0.05 (see text).

Figure 3.
Evolution of the perfusion asymmetry defined by the dominant/contralateral limb ratio during the supine experimental protocols course in younger (a) and aged (b) participants (see text).
Figure 3.
Evolution of the perfusion asymmetry defined by the dominant/contralateral limb ratio during the supine experimental protocols course in younger (a) and aged (b) participants (see text).

Figure 4.
Evolution of the perfusion asymmetry defined by the dominant/contralateral limb ratio during the upright experimental protocols course in younger (a) and aged (b) participants (see text).
Figure 4.
Evolution of the perfusion asymmetry defined by the dominant/contralateral limb ratio during the upright experimental protocols course in younger (a) and aged (b) participants (see text).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary of experimental settings of each study included in the present analysis. All studies included perfusion measurement in both feet.
Table 1.
Summary of experimental settings of each study included in the present analysis. All studies included perfusion measurement in both feet.
| References | Participant Profile | Reference Measuring Technology | Measurement Sites | Protocol Duration (Three Phases) | Challenge (Ph2) |
|---|---|---|---|---|---|
| Gregorio et al. [31] | Healthy, young, both sexes | LDF | 2nd toe, plantar, both feet | Ph1—10 min Ph2—5 min Ph3—10 min | Massage |
| Rocha et al. [33] | Healthy, aged, both sexes | LDF | 2nd toe, plantar, both feet | Ph1—10 min Ph2—5 min Ph3—10 min | Massage |
| Rocha et al. [34] | Healthy, young, both sexes | LDF | 2nd toe, plantar, both feet | Ph1—10 min Ph2—5 min Ph3—10 min | Massage |
| Rodrigues et al. [35] | Healthy, young, both sexes | LDF | 2nd toe, plantar, both feet | Ph1—10 min Ph2—5 min Ph3—10 min | Massage |
| Florindo et al. [37] | Healthy, aged, both sexes | LDF | Dorsal, 1st metatarsal, both feet | Ph1—10 min Ph2—1 min Ph3—5 min | Plantar flexion |
| Nuno et al. [38] | Healthy, young, both sexes | LDF | Dorsal, 2nd–3rd toe root, both feet | Ph1—10 min Ph2—5 min Ph3—10 min | Hemi-squat; squat |
| Florindo et al. [39] | Healthy, young and aged, both sexes | LDF | Dorsal, 1st metatarsal, both feet | Ph1—10 min Ph2—5 min Ph3—10 min | Walking |
Table 2.
Participants’ characteristics and their differences (parametric one-way ANOVA test, with post-hoc Tukey’s HSD for pairwise comparison of multiple samples was used when normality of the data was confirmed by Shapiro–Wilk test; ⸸—non-parametric Kruskal–Wallis test was used if the data were not normally distributed; * p < 0.05).
Table 2.
Participants’ characteristics and their differences (parametric one-way ANOVA test, with post-hoc Tukey’s HSD for pairwise comparison of multiple samples was used when normality of the data was confirmed by Shapiro–Wilk test; ⸸—non-parametric Kruskal–Wallis test was used if the data were not normally distributed; * p < 0.05).
| MEN | Massage | Plantar Flexion | Step-in-Place | Hemi-Squat | Squat | Walking | p |
|---|---|---|---|---|---|---|---|
| N (%) | 28 (40.6) | 9 (13.0) | 12 (17.4) | 4 (5.8) | 4 (5.8) | 12 (17.4) | - |
| Median Age, years (min—max) | 20.5 (18.0–66.0) | 30.0 (21.0–55.0) | 22.5 (18.0–32.0) | 31.5 (20.0–32.0) | 31.5 (20.0–32.0) | 31.5 (19.0–58.0) | 0.563 |
| Mean Weight, kg (SD) | 76.1 (10.0) | 75.9 (15.3) | 77.1 (6.3) | 68.0 (6.7) | 68.0 (6.7) | 75.5 (6.6) | 0.398 |
| Mean Height, meters (SD) | 1.8 (0.1) | 1.8 (0.1) | 1.8 (0.1) | 1.7 (0.0) | 1.7 (0.0) | 1.7 (0.1) | 0.211 |
| Mean BMI, kg/m2 (SD) | 23.9 (2.9) | 24.6 (4.1) | 24.7 (1.2) | 22.8 (1.8) | 22.8 (1.8) | 25.0 (1.4) | 0.446 |
| Mean SYS (SD) | 118.2 (11.8) | 116.0 (14.6) | 123.0 (13.6) | 124.0 (7.4) | 124.0 (7.4) | 124.2 (17.7) | 0.570 |
| Mean DIA (SD) | 74.4 (9.2) | 75.1 (9.0) | 71.5 (8.2) | 67.0 (6.7) | 67.0 (6.7) | 71.4 (7.3) | 0.324 |
| Median ABI (min—max) | 1.1 (1.0–1.3) | 1.2 (1.1–1.8) | 1.1 (1.0–1.2) | 1.0 (1.0–1.1) | 1.0 (1.0–1.1) | 1.1 (1.0–1.2) | 0.008 * |
| WOMEN | |||||||
| N (%) | 28 (40.0) | 9 (12.9) | 11 (15.7) | 4 (5.7) | 4 (5.7) | 14 (20.0) | - |
| Median Age, years (min—max) | 23.0 (18.0–62.0) | 26.0 (21.0–59.0) | 23.0 (20.0–31.0) | 22.0 (21.0–22.0) | 22.0 (21.0–22.0) | 22.5 (19.0–44.0) | 0.463 |
| Mean Weight, kg (SD) | 60.5 (9.1) | 72.9 (15.5) | 57.8 (8.7) | 61.3 (10.7) | 61.3 (10.7) | 60.7 (10.2) | 0.043 * |
| Mean Height, meters (SD) | 1.6 (0.1) | 1.6 (0.1) | 1.6 (0.1) | 1.7 (0.1) | 1.7 (0.1) | 1.6 (0.1) | 0.597 |
| Mean BMI, kg/m2 (SD) | 22.9 (3.3) | 27.7 (6.4) | 21.4 (2.8) | 21.8 (2.1) | 21.8 (2.1) | 22.8 (3.0) | 0.007 * |
| Mean SYS (SD) | 113.0 (13.8) | 123.7 (11.0) | 115.9 (8.2) | 122.0 (7.6) | 122.0 (7.6) | 114.5 (14.4) | 0.218 |
| Mean DIA (SD) | 74.1 (7.2) | 83.2 (8.5) | 72.1 (11.2) | 63.0 (7.9) | 63.0 (7.9) | 68.5 (6.6) | <0.001 * |
| Median ABI (min—max) | 1.1 (1.0–1.3) | 1.2 ⸸ (1.0–1.4) | 1.1 (0.9–1.2) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 1.0 (0.9–1.2) | 0.001 * |
Note: BMI—body mass index; SYS—systolic pressure; DIA—diastolic pressure; ABI—ankle–brachial index.
Table 3.
Association of individuals’ perfusion, at baseline and recovery phases of experimental protocols, with the independent variables of interest.
Table 3.
Association of individuals’ perfusion, at baseline and recovery phases of experimental protocols, with the independent variables of interest.
| Perfusion at Baseline (4th Quartile) | Perfusion at Recovery (4th Quartile) | |||
|---|---|---|---|---|
| OR [95% CI] (p-Value) | aOR [95% CI] (p-Value) | OR [95% CI] (p-Value) | aOR [95% CI] (p-Value) | |
| SEX | ||||
| Men | 2.4 [1.1–5.4] (0.030) | 2.6 [1.1–6.3] (0.032) | 1.8 [0.8–3.8] (0.159) | 1.6 [0.7–3.8] (0.281) |
| Women | 1 | 1 | 1 | 1 |
| BMI, kg/m2 | ||||
| less than 25 | 0.4 [0.2–0.8] (0.013) | 0.5 [0.2–1.3] (0.173) | 0.4 [0.2–0.8] (0.013) | 0.6 [0.2–1.4] (0.198) |
| more than 25 | 1 | 1 | 1 | 1 |
| AGE, years | ||||
| less than 30 | 0.4 [0.2–0.8] (0.010) | 0.4 [0.2–1.0] (0.064) | 0.2 [0.1–0.5] (<0.001) | 0.3 [0.1–0.6] (0.003) |
| more than 30 | 1 | 1 | 1 | 1 |
Notes: OR: unadjusted odds ratio; aOR: for sex, adjusted odds ratio with age, BMI, PSYS, PDIAS, body position; for BMI group, adjusted odds ratio with age, sex, PSYS, PDIAS, body position; for age group, adjusted odds ratio with sex, BMI, PSYS, PDIA, body position. (BMI—body mass index; SYS—systolic pressure; DIA—diastolic pressure; ABI—ankle–brachial index.)
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Rodrigues, L.M.; Rocha, C.G.; Florindo, M.E.; Gregório, J. Lower Limb Perfusion Asymmetries in Humans at Rest and Following Activity—A Collective View. Symmetry 2021, 13, 2348. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13122348
AMA Style
Rodrigues LM, Rocha CG, Florindo ME, Gregório J. Lower Limb Perfusion Asymmetries in Humans at Rest and Following Activity—A Collective View. Symmetry. 2021; 13(12):2348. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13122348
Chicago/Turabian StyleRodrigues, Luis Monteiro, Clemente Gomes Rocha, Margarida Esteves Florindo, and João Gregório. 2021. "Lower Limb Perfusion Asymmetries in Humans at Rest and Following Activity—A Collective View" Symmetry 13, no. 12: 2348. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13122348
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.