
Surgical-Orthodontic Diagnosis and Treatment Planning in an Asymmetric Skeletal Class III Patient—A Case Report

 ,
, 
Abstract
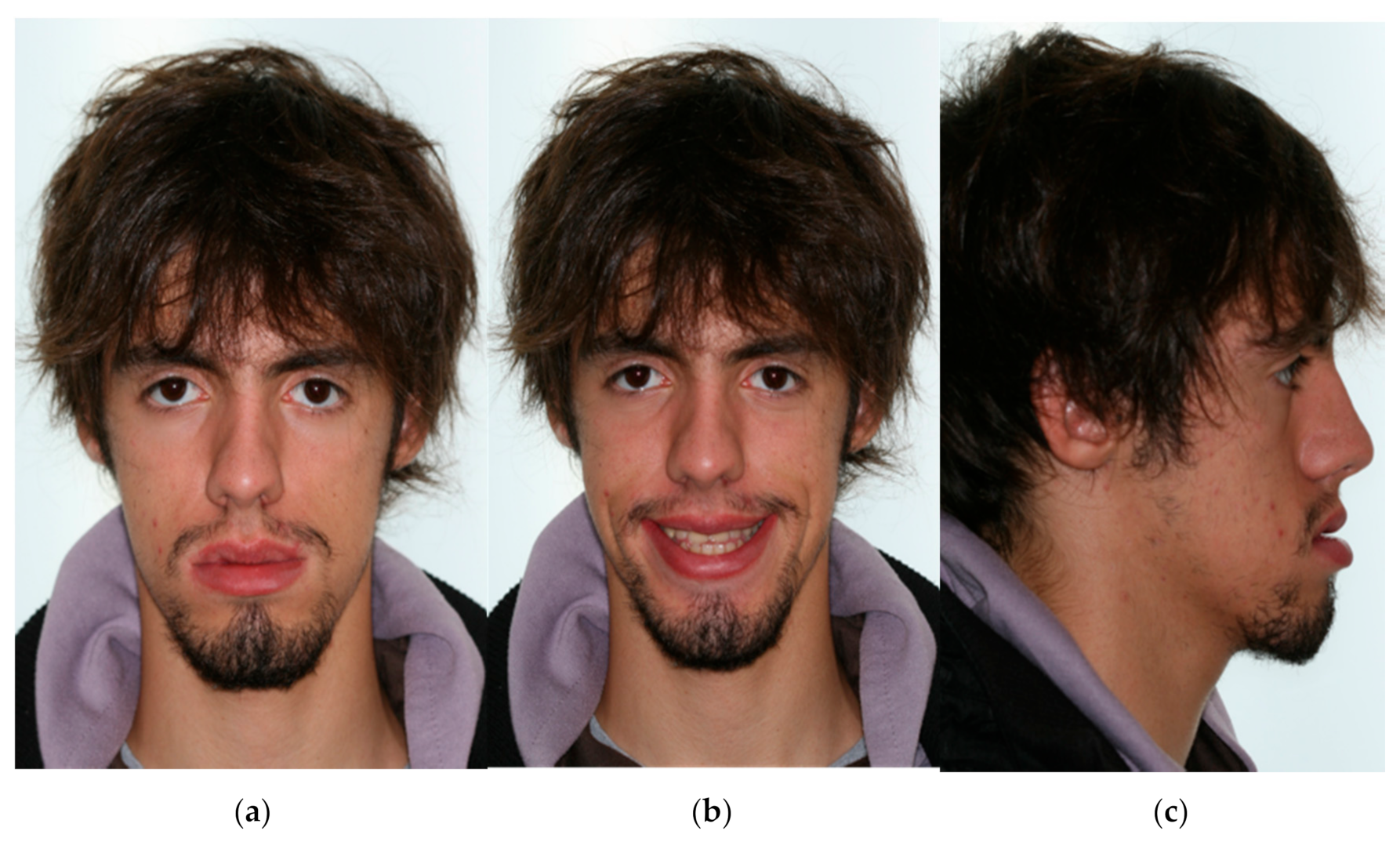
:1. Introduction
2. Materials and Methods
3. Results
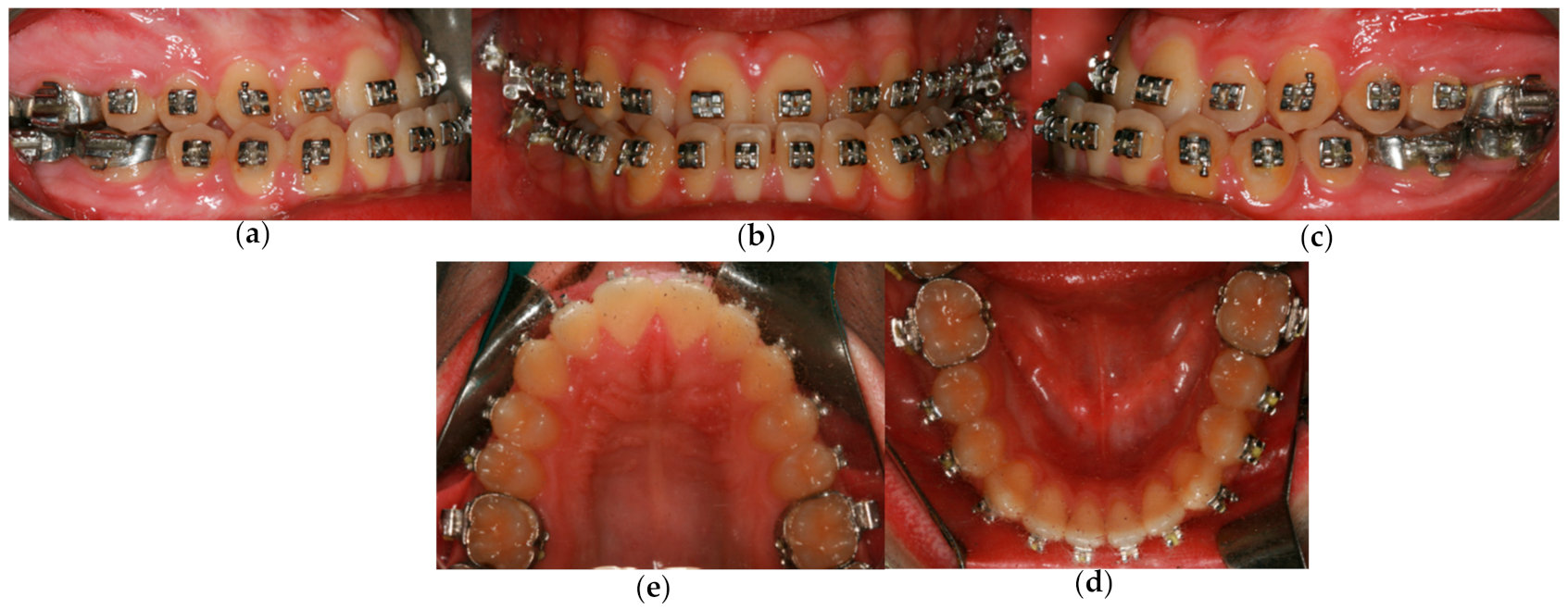
3.1. The Presurgical Orthodontic Treatment
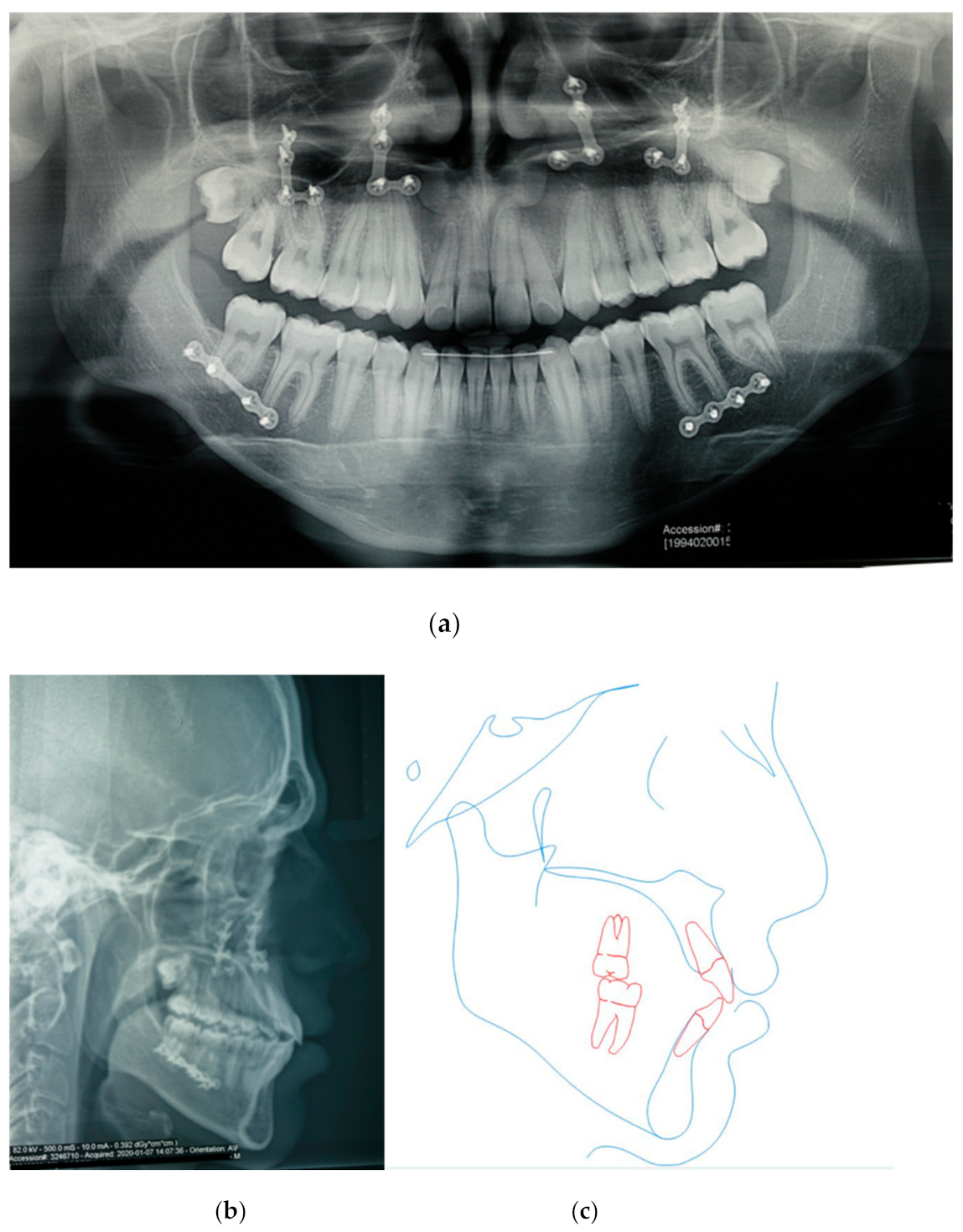
3.2. Orthognathic Surgery
3.3. Postsurgical Orthodontic Treatment
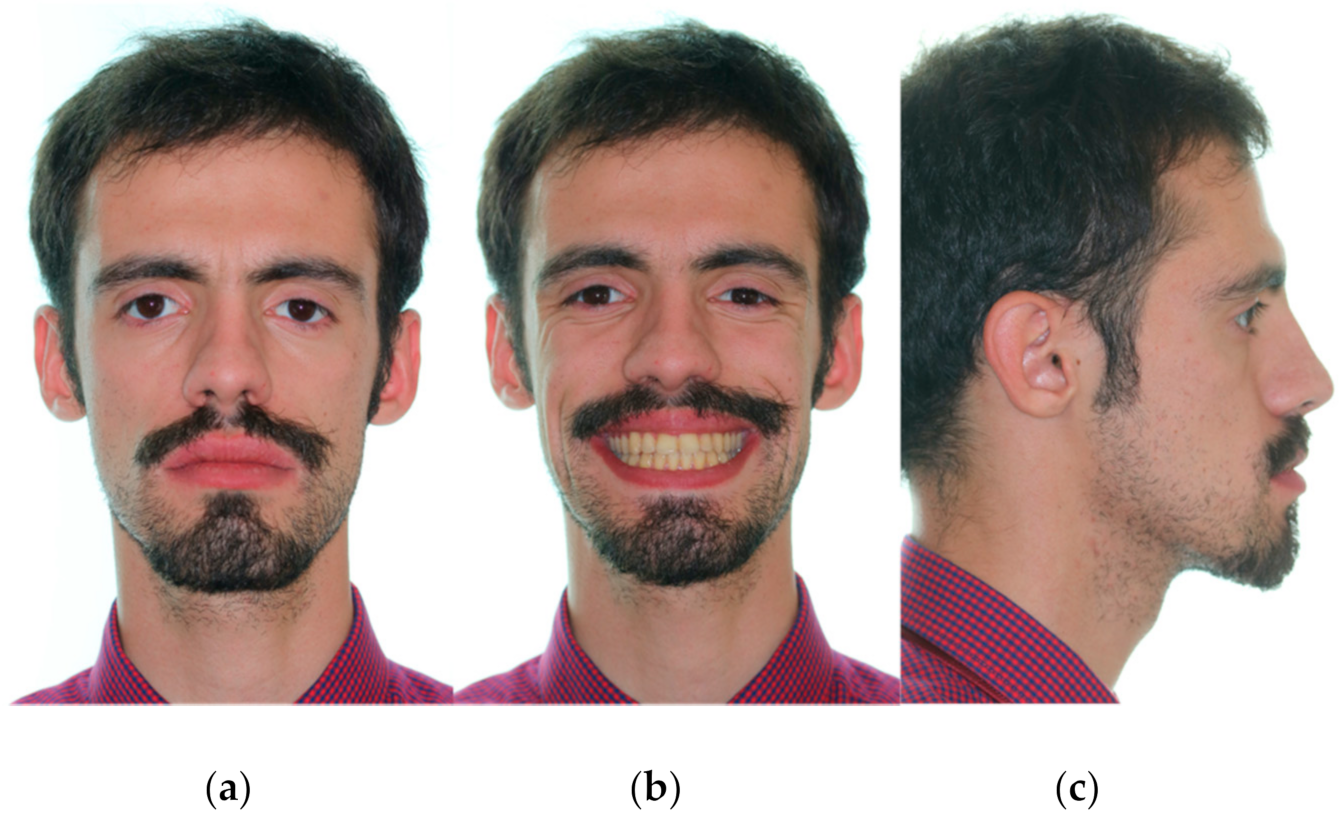
3.4. Treatment Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Da Pozzo, F.; Gibelli, D.; Beltramini, G.A.; Dolci, C.; Giannì, A.B.; Sforza, C. The Effect of Orthognathic Surgery on Soft-Tissue Facial Asymmetry: A Longitudinal Three-Dimensional Analysis. J. Craniofac. Surg. 2020, 31, 1578–1582. [Google Scholar] [CrossRef] [PubMed]
- Xue, Z.; Wu, L.; Qiu, T.; Li, Z.; Wang, X.; Liu, X. Three-Dimensional Dynamic Analysis of the Facial Movement Symmetry of Skeletal Class III Patients With Facial Asymmetry. J. Oral Maxillofac. Surg. 2020, 78, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Sfondrini, M.F.; Zampetti, P.; Luscher, G.; Gandini, P.; Gandía-Franco, J.L.; Scribante, A. Orthodontic Treatment and Healthcare Goals: Evaluation of Multibrackets Treatment Results Using PAR Index (Peer Assessment Rating). Healthcare 2020, 8, 473. [Google Scholar] [CrossRef] [PubMed]
- Thiesen, G.; Gribel, B.F.; Kim, K.B.; Pereira, K.C.R.; Freitas, M.P.M. Prevalence and Associated Factors of Mandibular Asymmetry in an Adult Population. J. Craniofac. Surg. 2017, 28, e199–e203. [Google Scholar] [CrossRef]
- Yu, J.; Hu, Y.; Huang, M.; Chen, J.; Ding, X.; Zheng, L. A three-dimensional analysis of skeletal and dental characteristics in skeletal class III patients with facial asymmetry. J. X-ray Sci. Technol. 2018, 26, 449–462. [Google Scholar] [CrossRef]
- Thiesen, G.; Gribel, B.F.; Kim, K.B.; Freitas, M.P.M. Maxillofacial Features Related to Mandibular Asymmetries in Skeletal Class III Patients. J. Oral Maxillofac. Surg. 2017, 75, 1015–1025. [Google Scholar] [CrossRef]
- Chen, Y.-J.; Yao, C.-C.; Chang, Z.-C.; Lai, H.-H.; Yeh, K.-J.; Kok, S.-H. Characterization of facial asymmetry in skeletal Class III malocclusion and its implications for treatment. Int. J. Oral Maxillofac. Surg. 2019, 48, 1533–1541. [Google Scholar] [CrossRef]
- Haraguchi, S.; Takada, K.; Yasuda, Y. Facial asymmetry in subjects with skeletal Class III deformity. Angle Orthod. 2002, 72, 28–35. [Google Scholar]
- Severt, T.R.; Proffit, W.R. The prevalence of facial asymmetry in the dentofacial deformities population at the University of North Carolina. Int. J. Adult Orthodon. Orthognath. Surg. 1997, 12, 171–176. [Google Scholar]
- Lin, C.-W.; Wang, Y.-C.; Chen, Y.-H.; Ko, E.W.-C. Dentoskeletal parameters related to visual perception of facial asymmetry in patients with skeletal class III malocclusion after orthognathic surgery. Int. J. Oral Maxillofac. Surg. 2018, 47, 48–56. [Google Scholar] [CrossRef]
- Kurabe, K.; Kojima, T.; Kato, Y.; Saito, I.; Kobayashi, T. Impact of orthognathic surgery on oral health-related quality of life in patients with jaw deformities. Int. J. Oral Maxillofac. Surg. 2016, 45, 1513–1519. [Google Scholar] [CrossRef]
- Akan, S.; Kocaderelı, I.; Tuncbılek, G. Long-term stability of surgical-orthodontic treatment for skeletal Class III malocclusion with mild asymmetry. J. Oral Sci. 2017, 59, 161–164. [Google Scholar] [CrossRef] [Green Version]
- Zere, E.; Chaudhari, P.K.; Saran, J.; Dhingra, K.; Tiwari, N. Developing Class III malocclusions: Challenges and solutions. Clin. Cosmet. Investig. Dent. 2018, 10, 99–116. [Google Scholar] [CrossRef] [Green Version]
- Doraczynska-Kowalik, A.; Nelke, K.H.; Pawlak, W.; Sasiadek, M.M.; Gerber, H. Genetic Factors Involved in Mandibular Prognathism. J. Craniofac. Surg. 2017, 28, e422–e431. [Google Scholar] [CrossRef]
- Rizzatto, S.M.D.; Macedo de Menezes, L.; da Cunha Filho, J.J.; Allgayer, S. Conventional surgical-orthodontic approach with double-jaw surgery for a patient with a skeletal Class III malocclusion: Stability of results 10 years posttreatment. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 128–139. [Google Scholar] [CrossRef]
- Dehesa-Santos, A.; Iber-Diaz, P.; Iglesias-Linares, A. Genetic factors contributing to skeletal class III malocclusion: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 1587–1612. [Google Scholar] [CrossRef]
- Martinez, P.; Bellot-Arcís, C.; Llamas, J.M.; Cibrian, R.; Gandia, J.L.; Paredes-Gallardo, V. Orthodontic camouflage versus orthognathic surgery for class III deformity: Comparative cephalometric analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 490–495. [Google Scholar] [CrossRef]
- Lee, G.-C.; Yoo, J.-K.; Kim, S.-H.; Moon, C.-H. Lip line changes in Class III facial asymmetry patients after orthodontic camouflage treatment, one-jaw surgery, and two-jaw surgery: A preliminary study. Angle Orthod. 2017, 87, 239–245. [Google Scholar] [CrossRef] [Green Version]
- Bou Wadi, M.N.; Freitas, K.M.S.; Freitas, D.S.; Cançado, R.H.; de Oliveira, R.C.G.; de Oliveira, R.C.G.; Janson, G.; Valarelli, F.P. Comparison of Profile Attractiveness between Class III Orthodontic Camouflage and Predictive Tracing of Orthognathic Surgery. Int. J. Dent. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Eslami, S.; Faber, J.; Fateh, A.; Sheikholaemmeh, F.; Grassia, V.; Jamilian, A. Treatment decision in adult patients with class III malocclusion: Surgery versus orthodontics. Prog. Orthod. 2018, 19, 28. [Google Scholar] [CrossRef] [Green Version]
- Quast, A.; Santander, P.; Leding, J.; Klenke, D.; Moser, N.; Schliephake, H.; Meyer-Marcotty, P. Orthodontic incisor decompensation in orthognathic therapy—Success and efficiency in three dimensions. Clin. Oral Investig. 2021, 25, 4001–4010. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.-S.; Oh, M.-H.; Oh, H.-K.; Oh, H. Surgery-first approach in correcting skeletal Class III malocclusion with mandibular asymmetry. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Benyahia, H.; Azaroual, M.F.; Garcia, C.; Hamou, E.; Abouqal, R.; Zaoui, F. Treatment of skeletal class III malocclusions: Orthognathic surgery or orthodontic camouflage? How to decide. Int. Orthod. 2011, 9, 196–209. [Google Scholar] [CrossRef] [PubMed]
- Soverina, D.; Gasparini, G.; Pelo, S.; Doneddu, P.; Todaro, M.; Boniello, R.; Azzuni, C.; Grippaudo, C.; Saponaro, G.; D’Amato, G.; et al. Skeletal stability in orthognathic surgery with the surgery first approach: A systematic review. Int. J. Oral Maxillofac. Surg. 2019, 48, 930–940. [Google Scholar] [CrossRef]
- Seifi, M.; Matini, N.-S.; Motabar, A.-R.; Motabar, M. Dentoskeletal Stability in Conventional Orthognathic Surgery, Presurgical Orthodontic Treatment and Surgery-First Approach in Class-III Patients. WORLD J. Plast. Surg. 2018, 7, 283–293. [Google Scholar] [CrossRef] [Green Version]
- Ming, Y.; Hu, Y.; Wang, T.; Zhang, J.; Li, Y.; Xu, W.; Tan, H.; Ye, H.; Zheng, L. Three-dimensional evaluation of skeletal and dental changes in patients with skeletal class III malocclusion and facial asymmetry after surgical-orthodontic treatment. J. X-ray Sci. Technol. 2020, 28, 783–798. [Google Scholar] [CrossRef]
- Dietrich, L.; Costa, M.; Ferreira, N.; Andrade, C.; Martins, V.; Mesquita, A. Planejamento E Tratamento Ortodôntico Para cirurgia ortognática. Rev. Odontol. Contemp. 2021, 2, 10–20. [Google Scholar]
- Park, J.H.; Emamy, M.; Lee, S.H. Adult skeletal Class III correction with camouflage orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 858–869. [Google Scholar] [CrossRef]
- Philippe, F.; Mona, S. Surgical Treatment of a Borderline Skeletal Class III Patient: An Interdisciplinary Approach. Med. Arch. 2021, 75, 69. [Google Scholar] [CrossRef]
- Rabie, A.-B.M.; Wong, R.W.K.; Min, G.U. Treatment in Borderline Class III Malocclusion: Orthodontic Camouflage (Extraction) Versus Orthognathic Surgery. Open Dent. J. 2008, 2, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Troy, B.A.; Shanker, S.; Fields, H.W.; Vig, K.; Johnston, W. Comparison of incisor inclination in patients with Class III malocclusion treated with orthognathic surgery or orthodontic camouflage. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 146.e1–146.e9. [Google Scholar] [CrossRef]
- Sándor, G.K.B.; McGuire, T.P.; Ylikontiola, L.P.; Serlo, W.S.; Pirttiniemi, P.M. Management of Facial Asymmetry. Oral Maxillofac. Surg. Clin. N. Am. 2007, 19, 395–422. [Google Scholar] [CrossRef]
- Hwang, H.-S.; Hwang, C.H.; Lee, K.-H.; Kang, B.-C. Maxillofacial 3-dimensional image analysis for the diagnosis of facial asymmetry. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 779–785. [Google Scholar] [CrossRef]
- Vaida, L.L.; Bud, E.S.; Halitchi, L.G.; Cavalu, S.; Todor, B.I.; Negrutiu, B.M.; Moca, A.E.; Bodog, F.D. The Behavior of Two Types of Upper Removable Retainers—Our Clinical Experience. Children 2020, 7, 295. [Google Scholar] [CrossRef]
- Kim, C.-H.; Joh, B.; Lim, H.J.; Park, J.H.; Kook, Y.-A.; Kim, Y. A conservative approach for an adult patient with a fractured tooth and crowding: Autotransplantation at the fracture site. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 234–245. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Norm | Pretreatment | Post-Treatment |
|---|---|---|---|
| Skeletal | |||
| SNA (°) | 82 | 77.5 | 82.2 |
| SNB (°) | 80 | 82.5 | 82.2 |
| ANB (°) | 2 | −5 | 0 |
| Wits appraisal (mm) | −1 | −9.4 | −3.4 |
| Dental | |||
| Interincisal Angle (U1–L1) (°) | 130 | 124.9 | 112.8 |
| U1–NA (°) | 22 | 30.7 | 36.6 |
| U1–NA (mm) | 4 | 8.4 | 9.9 |
| U1–Mx Base (°) | 110 | 115.8 | 126.8 |
| L1–NB (°) | 25 | 29.4 | 30.5 |
| L1–NB (mm) | 4 | 7.6 | 6.1 |
| L1–GoGn (°) | 92 | 90.3 | 99.1 |
| Soft tissue | |||
| Maxillary lip to E-line (mm) | −2 | −4.3 | −2.5 |
| Mandibular lip to E-line (mm) | 0 | 4.7 | 1.6 |
| Holdaway angle (NB to H-line) (°) | 4.9 | 10.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vale, F.; Nunes, C.; Guimarães, A.; Paula, A.B.; Francisco, I. Surgical-Orthodontic Diagnosis and Treatment Planning in an Asymmetric Skeletal Class III Patient—A Case Report. Symmetry 2021, 13, 1150. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13071150
Vale F, Nunes C, Guimarães A, Paula AB, Francisco I. Surgical-Orthodontic Diagnosis and Treatment Planning in an Asymmetric Skeletal Class III Patient—A Case Report. Symmetry. 2021; 13(7):1150. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13071150
Chicago/Turabian StyleVale, Francisco, Catarina Nunes, Adriana Guimarães, Anabela Baptista Paula, and Inês Francisco. 2021. "Surgical-Orthodontic Diagnosis and Treatment Planning in an Asymmetric Skeletal Class III Patient—A Case Report" Symmetry 13, no. 7: 1150. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13071150