
Multilingual Conversational Systems to Drive the Collection of Patient-Reported Outcomes and Integration into Clinical Workflows

 , , , and
, , , and 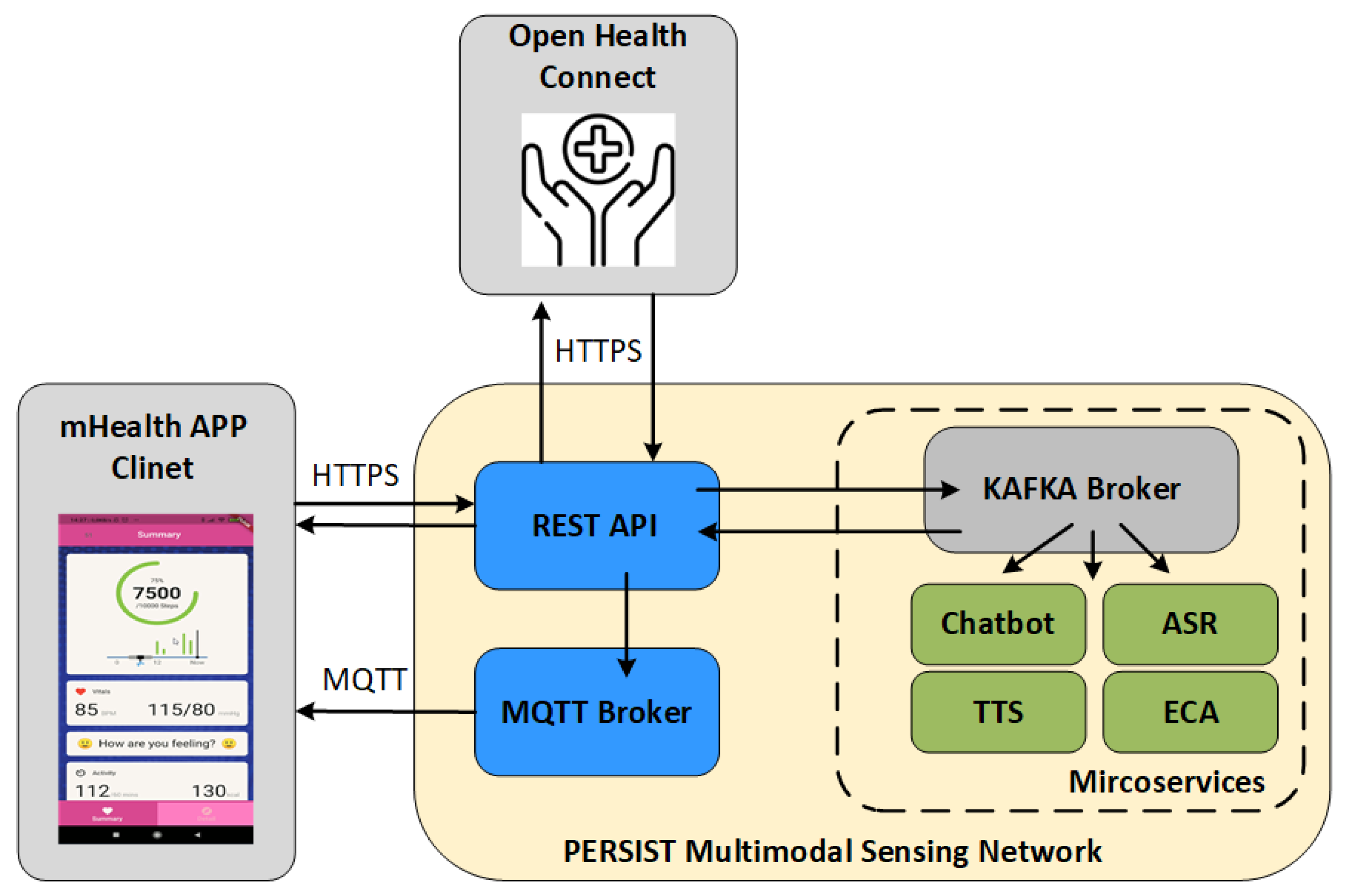{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Related Works
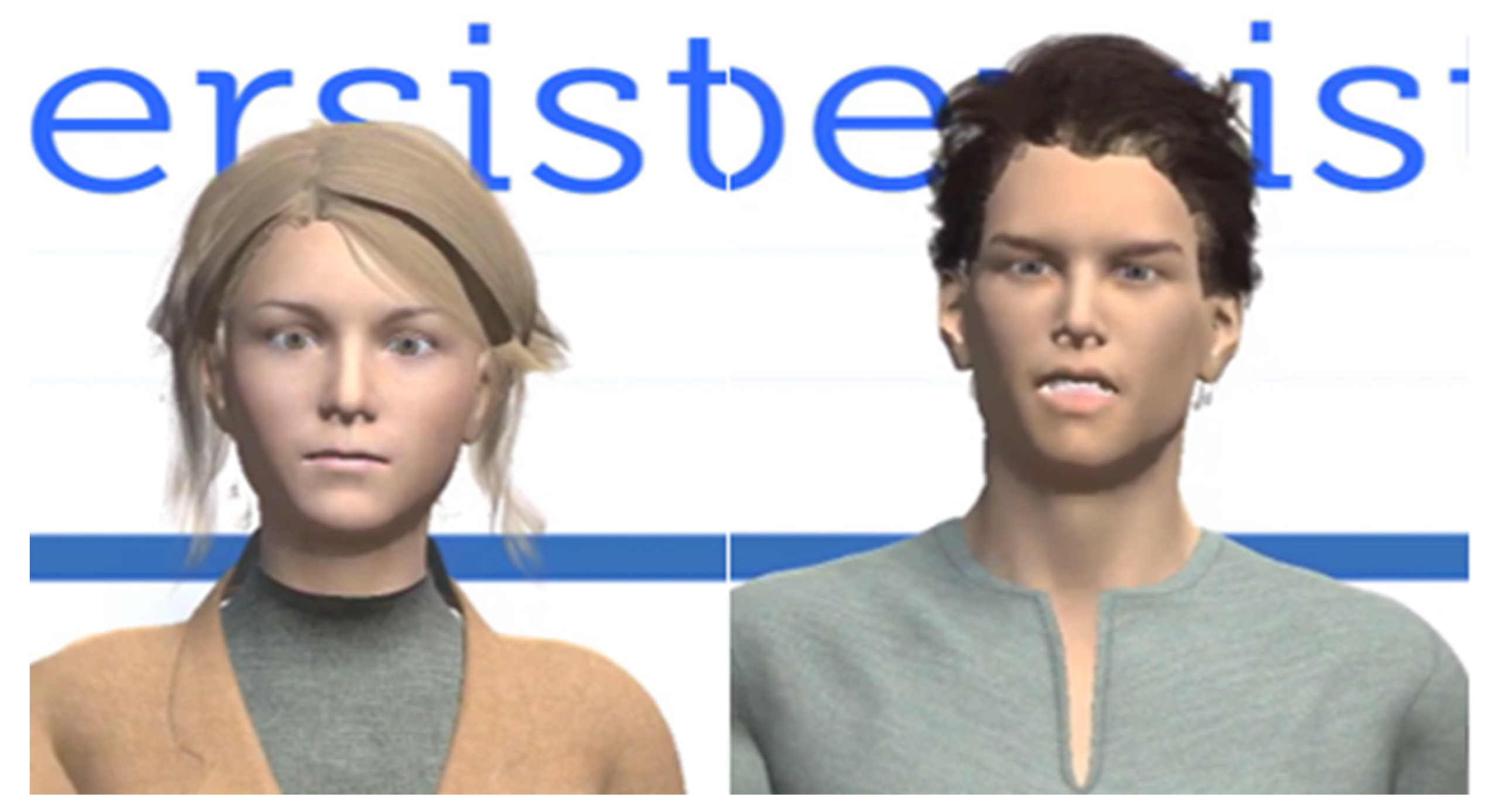
- A multilingual, fully articulated ECA implementing symmetric interaction in 6 languages and with male and female representation
- A micro-service-based sensing network to collect patient information further supported by patient and clinician mHealth application
- A holistic approach towards interoperable and fully integrated PGHD
3. PERSIST Platform for Efficient Collection of PROs
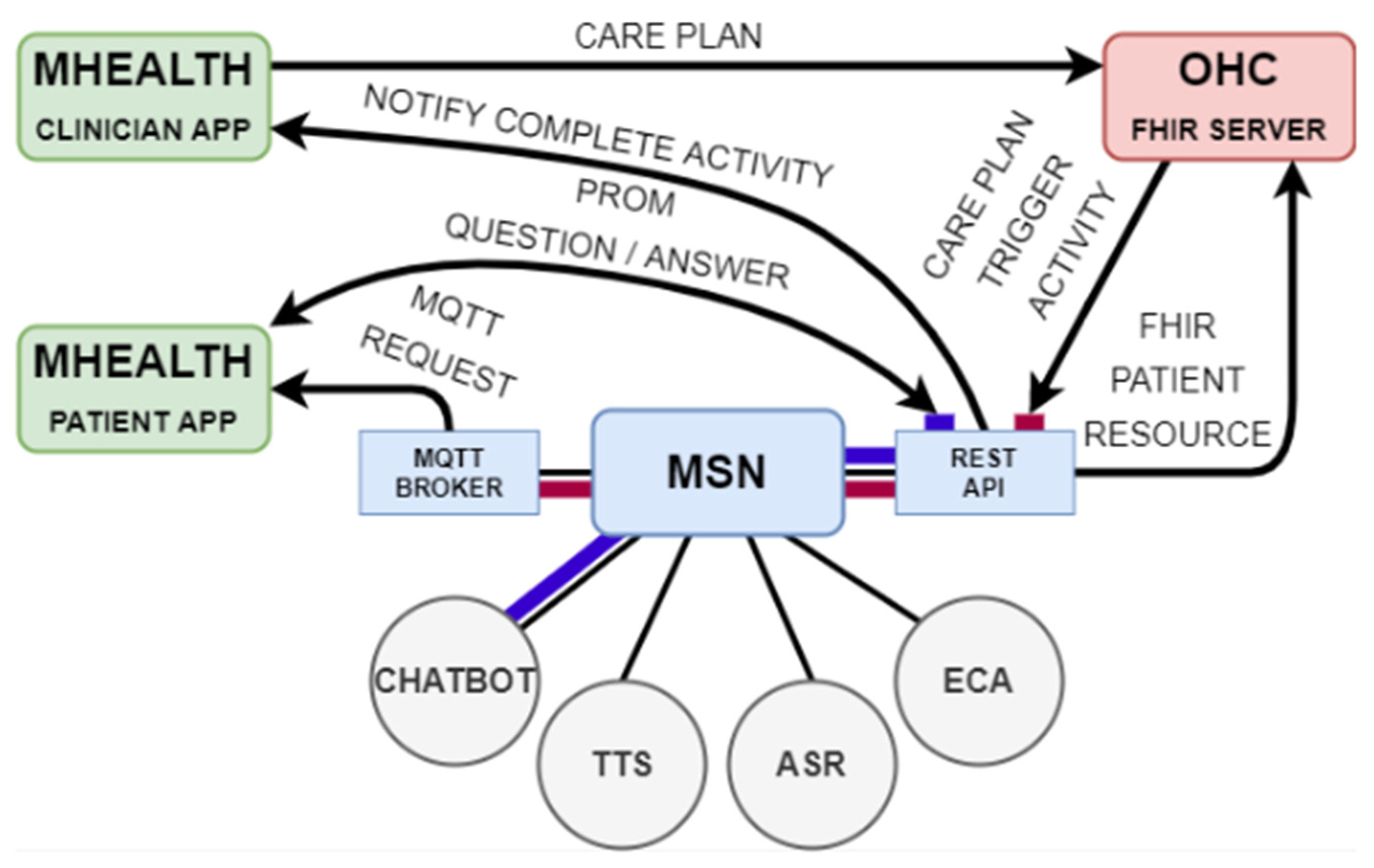
3.1. The PERSIST Sensing Network
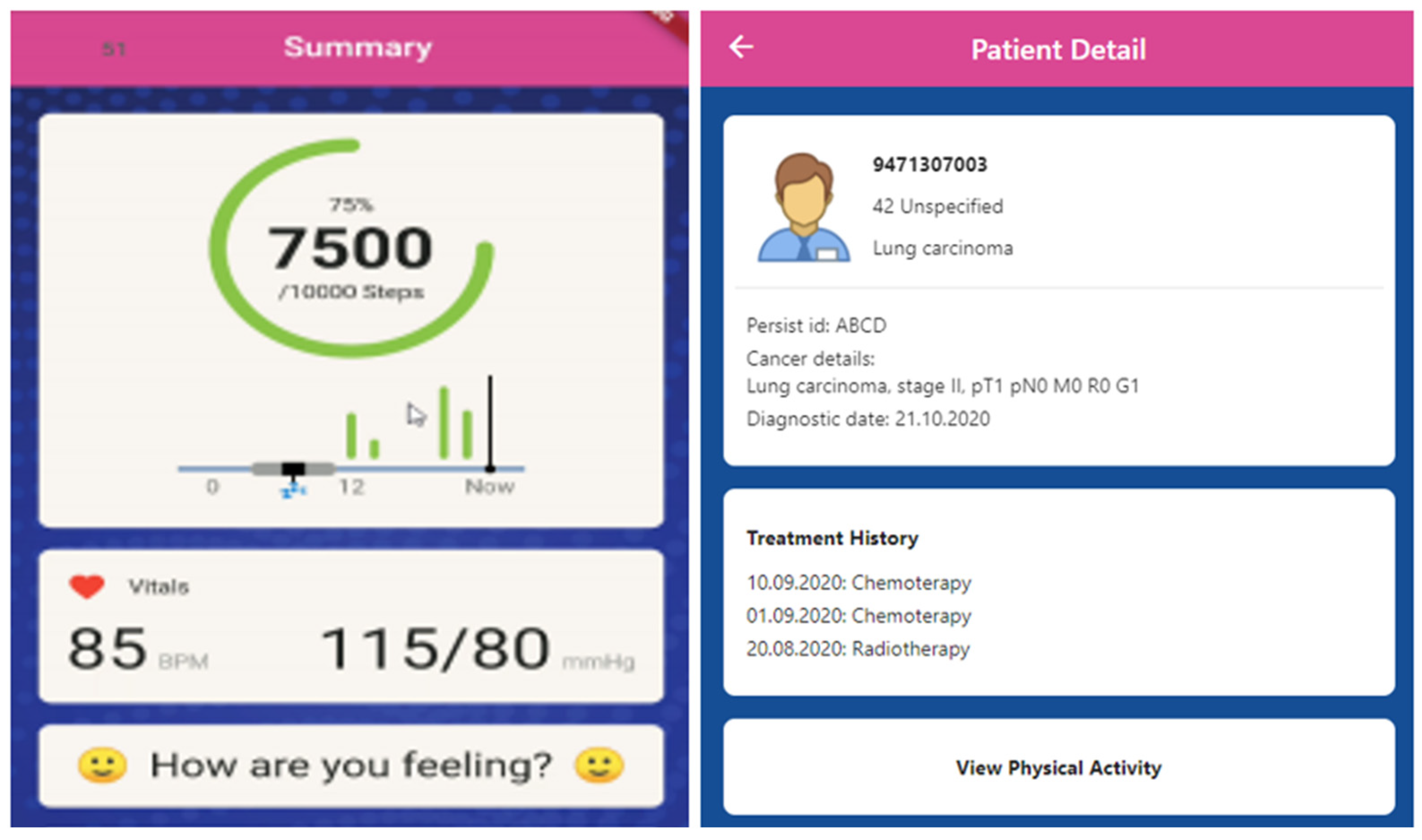
3.2. mHealth Application
3.3. OHC FHIR Server
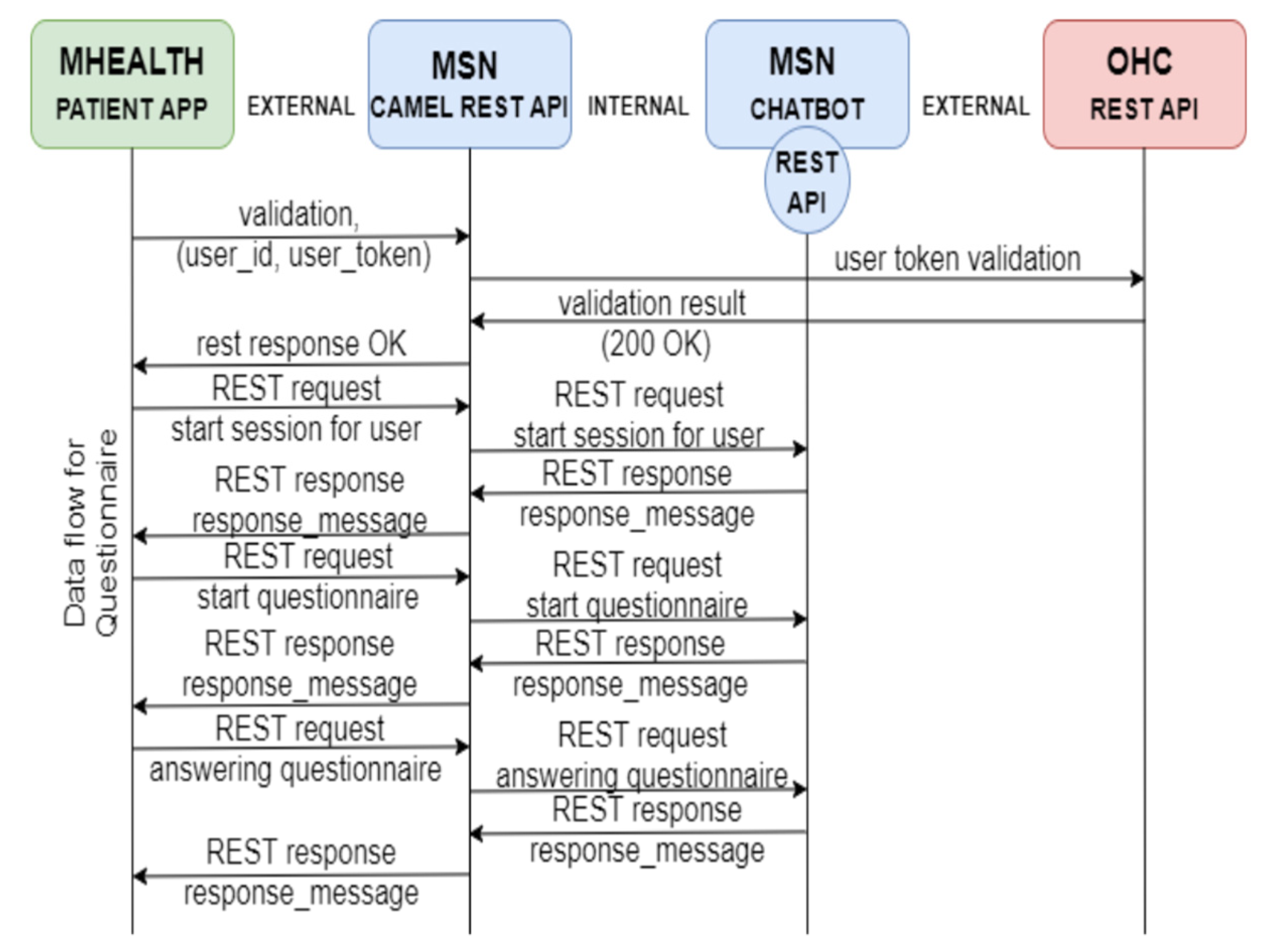
4. Microservices to Support Fully Symmetric Interaction Model
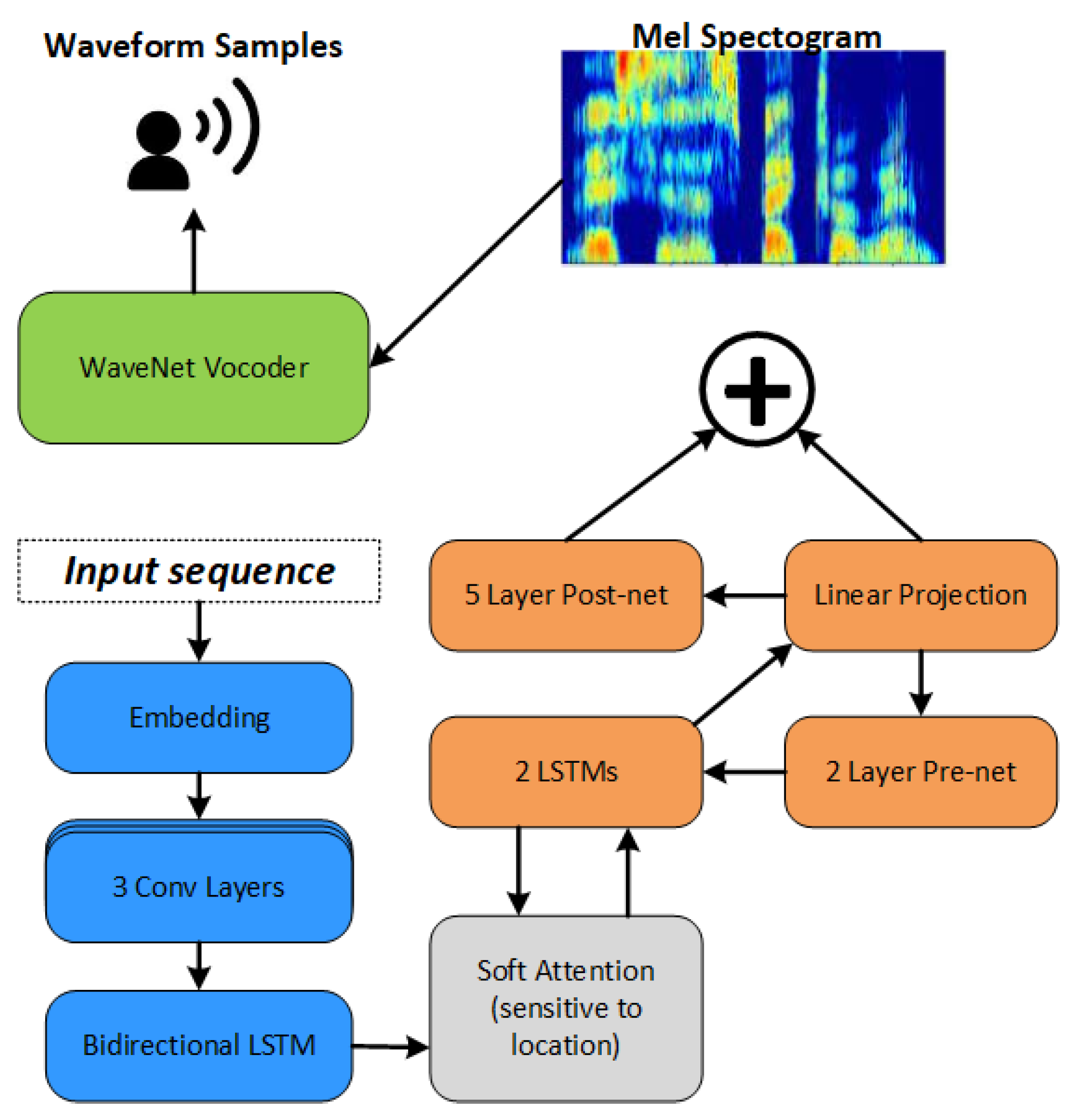
4.1. End-to-End Multilingual Text-To-Speech Synthesis
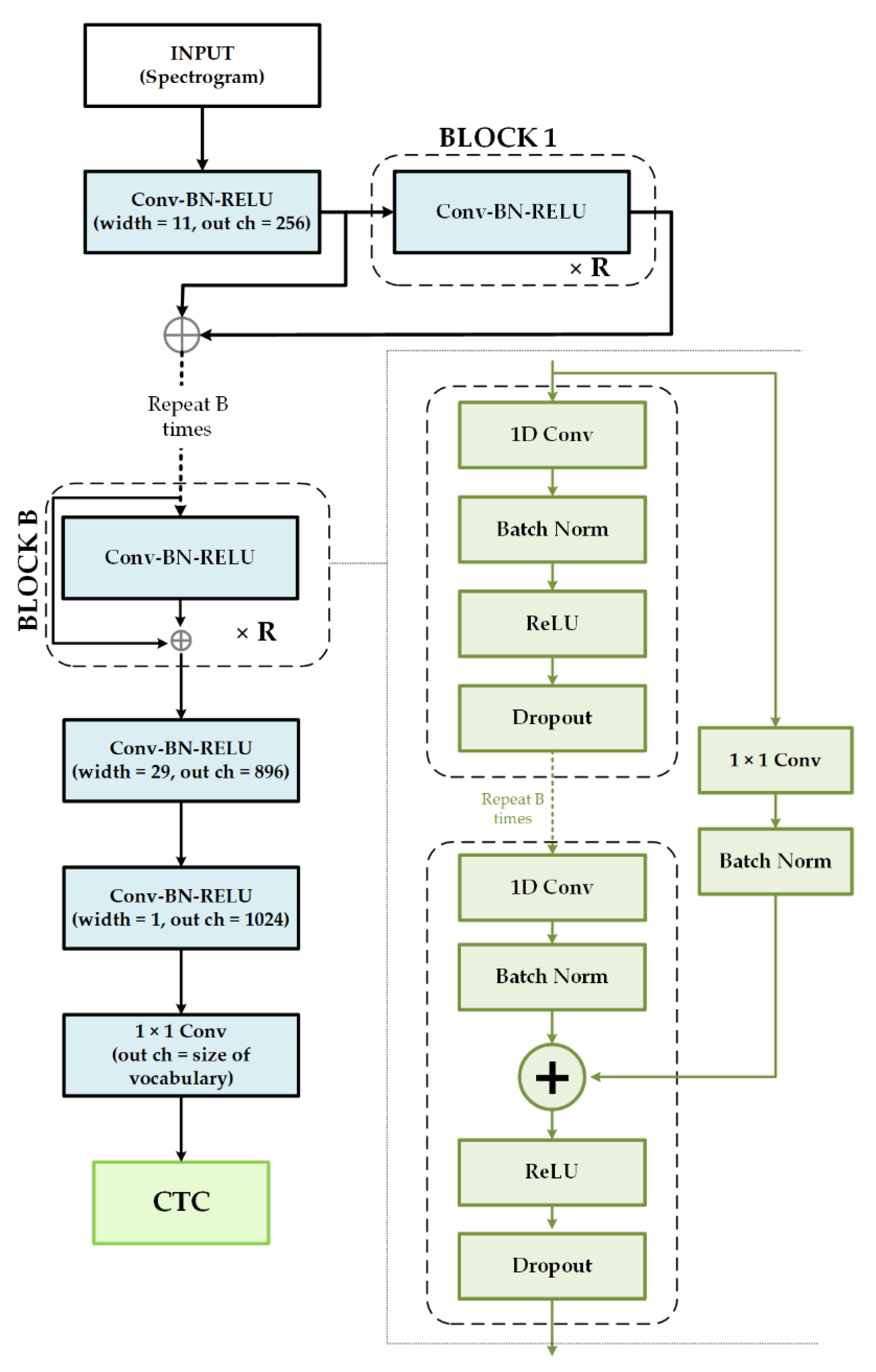
4.2. End-to-End Multilingual Speech Recognition
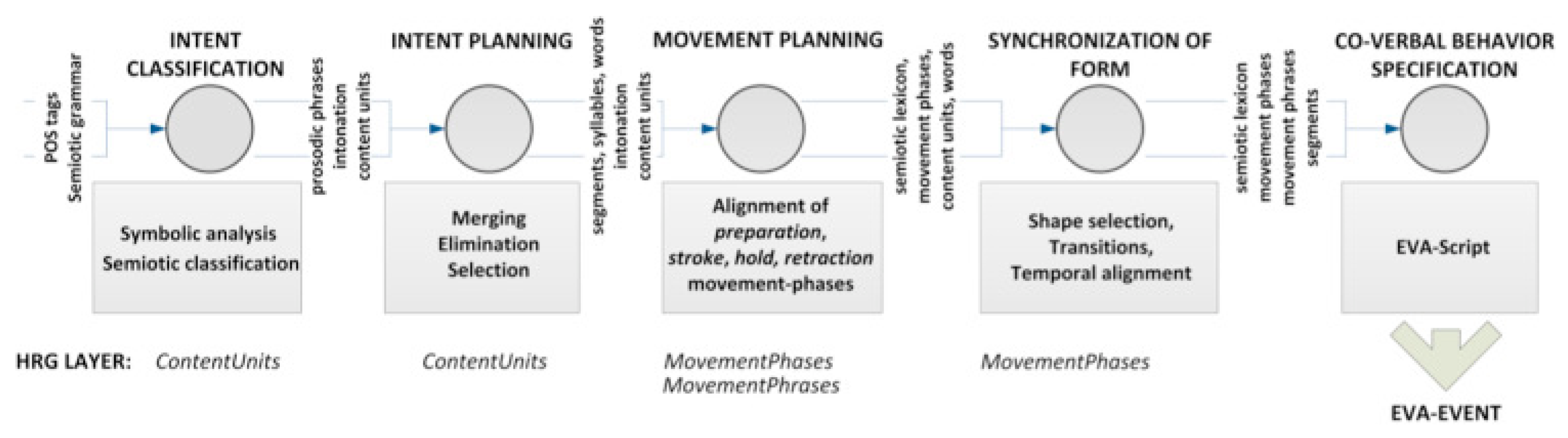
4.3. Embodied Conversational System and Embodied Conversational Agent
5. Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Health Council. What are Clinician-Reported Outcomes (ClinROs)? National Health Council, 2019; Available online: https://nationalhealthcouncil.org/coa-series-what-are-clinician-reported-outcomes-clinros/ (accessed on 19 June 2021).
- Health IT, Office of the National Coordinator for Health Information Technology (ONC), US Department of Health Human Services. What Are Patient-Generated Health Data? Available online: Healthit.gov/topic/otherhot-topics/what-are-patient-generated-health-data (accessed on 15 October 2019).
- Fauzana, N.; Gulcharan, B.I.; Azhar, M.A.; Daud, H.; Mohd, N.N.; Taib, I. Integrating Emerging Network Technologies to Heart Rate Monitoring System to Investigate Transmission Stability and Accuracy: Preliminary Results. Int. J. Electr. Eng. Comput. Sci. (EEACS) 2021, 3, 21–22. [Google Scholar]
- Sawssen, B.; Okba, T.; Noureeddine, L. A Mammographic Images Classification Technique via the Gaussian Radial Basis Kernel ELM and KPCA. Int. J. Appl. Math. Comput. Sci. Syst. Eng. 2020, 2, 92–98. [Google Scholar]
- Zheng, Q.; Yang, L.; Zeng, B.; Li, J.; Guo, K.; Liang, Y.; Liao, G. Artificial intelligence performance in detecting tumor metastasis from medical radiology imaging: A systematic review and meta-analysis. EClinicalMedicine 2021, 31, 100669. [Google Scholar] [CrossRef]
- Inès, A.; Zgaya, H.; Slim, H. Workflow tool to Model and simulate patients paths in Pediatric Emergency Department. Int. J. Electr. Eng. Comput. Sci. 2020, 2, 73–78. [Google Scholar]
- Abdelnabi, M.L.R.; Jasim, M.W.; El-Bakry, H.M.; Taha, M.H.N.; Khalifa, N.E.M.; Loey, M. Breast and Colon Cancer Classification from Gene Expression Profiles Using Data Mining Techniques. Symmetry 2020, 12, 408. [Google Scholar] [CrossRef] [Green Version]
- Austin, E.; LeRouge, C.; Hartzler, A.L.; Segal, C.; Lavallee, D.C. Capturing the patient voice: Implementing patient-reported outcomes across the health system. Qual. Life Res. 2020, 29, 347–355. [Google Scholar] [CrossRef] [Green Version]
- Groccia, M.C.; Guido, R.; Conforti, D. Multi-Classifier Approaches for Supporting Clinical Decision Making. Symmetry 2020, 12, 699. [Google Scholar] [CrossRef]
- Ellwood, P.M. Outcomes Management. N. Engl. J. Med. 1988, 318, 1549–1556. [Google Scholar] [CrossRef]
- Tarlov, A.R.; Ware, J.E.; Greenfield, S.; Nelson, E.C.; Perrin, E.; Zubkoff, M. The Medical Outcomes Study: An application of methods for monitoring the results of medical care. JAMA 1989, 262, 925–930. [Google Scholar] [CrossRef]
- Bielli, E.; Carminati, F.; La Capra, S.; Lina, M.; Brunelli, C.; Tamburini, M. A Wireless Health Outcomes Moni-toring System (WHOMS): Development and field testing with cancer patients using mobile phones. BMC Med. Inform. Decis. Mak. 2004, 4, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Tran, C.; Dicker, A.; Leiby, B.; Gressen, E.; Williams, N.; Jim, H. Utilizing digital health to collect electronic pa-tient-reported outcomes in prostate cancer: Single-arm pilot trial. J. Med. Internet Res. 2020, 22, e12689. [Google Scholar] [CrossRef]
- Wright, A.A.; Raman, N.; Staples, P.; Schonholz, S.; Cronin, A.; Carlson, K.; Keating, N.L.; Onnela, J.-P. The HOPE Pilot Study: Harnessing Patient-Reported Outcomes and Biometric Data to Enhance Cancer Care. JCO Clin. Cancer Inform. 2018, 2, 1–12. [Google Scholar] [CrossRef]
- Rajguru, P.; Ryan, S.; McLaurin, E.; Wirta, D.; Grieco, J. A novel method for collecting patient reported outcomes (PROs): Developing and validating electronic PROs on a mobile smartphone platform. Invest. Ophthalmol. Vis. Sci. 2020, 7, 110. [Google Scholar]
- Van Egdom, L.S.E.; Pusic, A.; Verhoef, C.; Hazelzet, J.A.; Koppert, L.B. Machine learning with PROs in breast cancer surgery; caution: Collecting PROs at baseline is crucial. Breast J. 2020, 26, 1213–1215. [Google Scholar] [CrossRef]
- Kramer, L.L.; Ter Stal, S.; Mulder, B.; De Vet, E.; Van Velsen, L. Developing Embodied Conversational Agents for Coaching People in a Healthy Lifestyle: Scoping Review. J. Med. Internet Res. 2020, 22, e14058. [Google Scholar] [CrossRef]
- Queirós, A.; Dias, A.; Silva, A.G.; Rocha, N.P. Ambient assisted living and health-related out-comes-A systematic literature review. Informatics 2014, 4, 19. [Google Scholar] [CrossRef] [Green Version]
- Alosaimi, W.; Ansari, T.J.; Alharbi, A.; Alyami, H.; Seh, A.; Pandey, A.; Agrawal, A.; Khan, R. Evaluating the Impact of Different Symmetrical Models of Ambient Assisted Living Systems. Symmetry 2021, 13, 450. [Google Scholar] [CrossRef]
- Laranjo, L.; Dunn, A.; Tong, H.L.; Kocaballi, A.B.; Chen, J.; Bashir, R.; Surian, D.; Gallego, B.; Magrabi, F.; Lau, A.Y.; et al. Conversational agents in healthcare: A systematic review. J. Am. Med. Inform. Assoc. 2018, 25, 1248–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jim, H.S.L.; Hoogland, A.; Brownstein, N.C.; Barata, A.; Dicker, A.P.; Knoop, H.; Gonzalez, B.D.; Perkins, R.; Rollison, D.; Gilbert, S.M.; et al. Innovations in research and clinical care using patient-generated health data. CA Cancer J. Clin. 2020, 70, 182–199. [Google Scholar] [CrossRef]
- Rehman, A.; Naz, S.; Razzak, I. Leveraging big data analytics in healthcare enhancement: Trends, challenges and opportunities. Multimedia Syst. 2021, 1–33. [Google Scholar] [CrossRef]
- Resourcelist—FHIR v4.0.1. Available online: http://hl7.org/fhir/resourcelist.html (accessed on 1 April 2021).
- Wald, J.S.; Sands, D.Z. Transforming Health Care Delivery Through Consumer Engagement, Health Data Transparency, and Patient-Generated Health Information. Yearb. Med. Inform. 2014, 23, 170–176. [Google Scholar] [CrossRef] [Green Version]
- Shawar, B.; Atwell, E. Chatbots: Are they Really Useful? LDV Forum 2007, 22, 29–49. [Google Scholar]
- Weizenbaum, J. ELIZA—A computer program for the study of natural language communication between man and machine. Commun. ACM 1966, 9, 36–45. [Google Scholar] [CrossRef]
- Sharma, R.K.; Center, N.I. An Analytical Study and Review of open source Chatbot framework, Rasa. Int. J. Eng. Res. 2020, 9, 060723. [Google Scholar] [CrossRef]
- Palanica, A.; Flaschner, P.; Thommandram, A.; Li, M.; Fossat, Y. Physicians’ Perceptions of Chatbots in Health Care: Cross-Sectional Web-Based Survey. J. Med. Internet Res. 2019, 21, e12887. [Google Scholar] [CrossRef] [PubMed]
- Bibault, J.-E.; Chaix, B.; Nectoux, P.; Pienkowski, A.; Guillemasé, A.; Brouard, B. Healthcare ex Machina: Are conversational agents ready for prime time in oncology? Clin. Transl. Radiat. Oncol. 2019, 16, 55–59. [Google Scholar] [CrossRef] [Green Version]
- Owens, O.L.; Felder, T.; Tavakoli, A.S.; Revels, A.A.; Friedman, D.B.; Hughes-Halbert, C.; Hébert, J.R. Evaluation of a Computer-Based Decision Aid for Promoting Informed Prostate Cancer Screening Decisions Among African American Men: iDecide. Am. J. Health Promot. 2019, 33, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, K.K.; Darcy, A.; Vierhile, M. Delivering Cognitive Behavior Therapy to Young Adults with Symptoms of Depression and Anxiety Using a Fully Automated Conversational Agent (Woebot): A Randomized Controlled Trial. JMIR Ment. Health 2017, 4, e19. [Google Scholar] [CrossRef]
- Inkster, B.; Sarda, S.; Subramanian, V. An Empathy-Driven, Conversational Artificial Intelligence Agent (Wysa) for Digital Mental Well-Being: Real-World Data Evaluation Mixed-Methods Study. JMIR mHealth uHealth 2018, 6, e12106. [Google Scholar] [CrossRef] [Green Version]
- Ly, K.H.; Ly, A.-M.; Andersson, G. A fully automated conversational agent for promoting mental well-being: A pilot RCT using mixed methods. Internet Interv. 2017, 10, 39–46. [Google Scholar] [CrossRef]
- Gardiner, P.M.; McCue, K.D.; Negash, L.M.; Cheng, T.; White, L.F.; Yinusa-Nyahkoon, L.; Jack, B.W.; Bickmore, T.W. Engaging women with an embodied conversational agent to deliver mindfulness and lifestyle recommendations: A feasibility randomized control trial. Patient Educ. Couns. 2017, 100, 1720–1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girgi, A.; Durcinoska, I.; Levesque, J.V.; Gerges, M.; Sandell, T.; Arnold, A.; Delaney, G.P. The PROMPT-Care Program Group eHealth System for Collecting and Utilizing Patient Reported Outcome Measures for Personalized Treatment and Care (PROMPT-Care) Among Cancer Patients: Mixed Methods Approach to Evaluate Feasibility and Acceptability. J. Med. Internet Res. 2017, 19, e330. [Google Scholar] [CrossRef] [PubMed]
- Kneuertz, P.J.; Jagadesh, N.; Perkins, A.; Fitzgerald, M.; Moffatt-Bruce, S.D.; Merritt, R.E.; D’Souza, D.M. Improving patient engagement, adherence, and satisfaction in lung cancer surgery with implementation of a mobile device platform for patient reported outcomes. J. Thorac. Dis. 2020, 12, 6883–6891. [Google Scholar] [CrossRef] [PubMed]
- Tellols, D.; Lopez-Sanchez, M.; Rodríguez, I.; Almajano, P.; Puig, A. Enhancing sentient embodied conversational agents with machine learning. Pattern Recognit. Lett. 2020, 129, 317–323. [Google Scholar] [CrossRef]
- Martin, L.R.; Williams, S.L.; Haskard, K.B.; DiMatteo, M.R. The challenge of patient adherence. Ther. Clin. Risk Manag. 2005, 1, 189–199. [Google Scholar] [PubMed]
- Isbister, K.; Doyle, P. The blind men and the elephant revisited evaluating interdisciplinary ECA research. In From Brows to Trust Evaluating Embodied Conversational Agents; Ruttkay, Z., Pelachaud, C., Eds.; Springer: Dordrecht, The Netherlands, 2004; pp. 3–26. [Google Scholar]
- Bickmore, T.; Gruber, A.; Picard, R. Establishing the computer–patient working alliance in automated health behavior change interventions. Patient Educ. Couns. 2005, 59, 21–30. [Google Scholar] [CrossRef]
- Klaassen, R.; Bul, K.C.M.; Akker, R.O.D.; Van Der Burg, G.J.; Kato, P.M.; Di Bitonto, P. Design and Evaluation of a Pervasive Coaching and Gamification Platform for Young Diabetes Patients. Sensors 2018, 18, 402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Provoost, S.; Lau, H.M.; Ruwaard, J.; Riper, H. Embodied Conversational Agents in Clinical Psychology: A Scoping Review. J. Med. Internet Res. 2017, 19, e151. [Google Scholar] [CrossRef] [Green Version]
- Rojc, M.; Kačič, Z.; Mlakar, I. Advanced Content and Interface Personalization through Conversational Behavior and Affective Embodied Conversational Agents. In Artificial Intelligence Emerging Trends and Applications; Fernandez, M.A.A., Ed.; IntechOpen: London, UK, 2018. [Google Scholar] [CrossRef] [Green Version]
- Brinkman, W.P. Virtual health agents for behavior change: Research perspectives and directions. In Proceedings of the Workshop on Graphical and Robotic Embodied Agents for Therapeutic Systems, Institute for Creative Technologies, USC, Los Angeles, CA, USA, 20 September 2016. [Google Scholar]
- Stal, S.; Kramer, L.L.; Tabak, M.; Akker, H.O.D.; Hermens, H. Design Features of Embodied Conversational Agents in eHealth: A Literature Review. Int. J. Hum. Comput. Stud. 2020, 138, 102409. [Google Scholar] [CrossRef]
- Friederichs, S.; Bolman, C.; Oenema, A.; Guyaux, J.; Lechner, L. Motivational Interviewing in a Web-Based Physical Activity Intervention with an Avatar: Randomized Controlled Trial. J. Med. Internet Res. 2014, 16, e48. [Google Scholar] [CrossRef]
- Bickmore, T.W.; Caruso, L.; Clough-Gorr, K.; Heeren, T. ’It’s just like you talk to a friend’ relational agents for older adults. Interact. Comput. 2005, 17, 711–735. [Google Scholar] [CrossRef]
- Ellis, T.; Latham, N.K.; DeAngelis, T.R.; Thomas, C.A.; Saint-Hilaire, M.; Bickmore, T.W. Feasibility of a Virtual Exercise Coach to Promote Walking in Community-Dwelling Persons with Parkinson Disease. Am. J. Phys. Med. Rehabil. 2013, 92, 472–485. [Google Scholar] [CrossRef] [Green Version]
- Henkemans, B.O.A.; van der Boog, P.J.; Lindenberg, J.; van der Mast, C.A.; Neerincx, M.A.; Zwetsloot-Schonk, B.J. An online lifestyle diary with a persuasive computer assistant providing feedback on self-management. Technol. Health Care 2009, 17, 253–267. [Google Scholar] [CrossRef] [PubMed]
- Bickmore, T.W.; Schulman, D.; Sidner, C. Automated interventions for multiple health behaviors using conversational agents. Patient Educ. Couns. 2013, 92, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Sillice, A.M.; Morokoff, P.J.; Ferszt, G.; Bickmore, T.; Bock, B.C.; Lantini, R.; Velicer, W.F. Using Relational Agents to Promote Exercise and Sun Protection: Assessment of Participants’ Experiences with Two Interventions. J. Med. Internet Res. 2018, 20, e48. [Google Scholar] [CrossRef] [Green Version]
- Benze, G.; Nauck, F.; Alt-Epping, B.; Gianni, G.; Bauknecht, T.; Ettl, J.; Munte, A.; Kretzschmar, L.; Gaertner, J. PROutine: A feasibility study assessing surveillance of electronic patient reported outcomes and adherence via smartphone app in advanced cancer. Ann. Palliat. Med. 2019, 8, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Sayeed, R.; Gottlieb, D.; Mandl, K.D. SMART Markers: Collecting patient-generated health data as a standardized property of health information technology. NPJ Digit. Med. 2020, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Versions—FHIR v4.0.1. Available online: https://www.hl7.org/fhir/versions.html (accessed on 1 April 2021).
- Shen, J.; Pang, R.; Weiss, R.J.; Schuster, M.; Jaitly, N.; Yang, Z.; Wu, Y. Natural tts synthesis by condi-tioning wavenet on mel spectrogram predictions. In Proceedings of the 2018 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Calgary, AB, Canada, 15–20 April 2018; pp. 4779–4783. [Google Scholar]
- Oord, A.V.D.; Dieleman, S.; Zen, H.; Simonyan, K.; Vinyals, O.; Graves, A.; Kavukcuoglu, K. Wavenet: A generative model for raw audio. arXiv 2016, arXiv:1609.03499. [Google Scholar]
- Li, J.; Lavrukhin, V.; Ginsburg, B.; Leary, R.; Kuchaiev, O.; Cohen, J.M.; Nguyen, H.; Gadde, R.T. Jasper: An End-to-End Convolutional Neural Acoustic Model. arXiv 2019, arXiv:1904.03288. [Google Scholar]
- Graves, A.; Jaitly, N. Towards end-to-end speech recognition with recurrent neural networks. In Proceedings of the International Conference on Machine Learning (ICML 2014), Beijing, China, 21–26 June 2014; pp. 1764–1772. [Google Scholar]
- Chorowski, J.; Bahdanau, D.; Cho, K.; Bengio, Y. End-to-end continuous speech recognition using attention-based recurrent nn: First results. arXiv 2014, arXiv:1412.1602. [Google Scholar]
- Bocklisch, T.; Faulkner, J.; Pawlowski, N.; Nichol, A. Rasa: Open source language understanding and dialogue management. arXiv 2017, arXiv:1712.05181. [Google Scholar]
- Rojc, M.; Mlakar, I.; Kačič, Z. The TTS-driven affective embodied conversational agent EVA, based on a novel conversational-behavior generation algorithm. Eng. Appl. Artif. Intell. 2017, 57, 80–104. [Google Scholar] [CrossRef]
- Mlakar, I.; Smrke, U. Clinical Study to Assess the Outcomes of a Patient-Centred Survivorship Care Plan Enhanced with Big Data and Artificial Intelligence Technologies 2021. Available online: https://www.isrctn.com/ISRCTN97617326 (accessed on 19 June 2021).
- Schoeffler, M.; Bartoschek, S.; Stöter, F.R.; Roess, M.; Westphal, S.; Edler, B.; Herre, J. Web MUSHRA—A comprehensive framework for web-based listening tests. J. Open Res. Softw. 2016, 6. [Google Scholar] [CrossRef] [Green Version]
- H2020 Project PERSIST. Available online: https://projectpersist.com/ (accessed on 31 May 2020).
- Sofer, C.; Dotsch, R.; Wigboldus, D.H.; Todorov, A. What is typical is good: The influence of face typicality on perceived trustworthiness. Psychol. Sci. 2015, 26, 39–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, A.; Ramasubramanian, K.; Shivam, S. Introduction to Microsoft Bot, RASA, and Google Dialogflow. In Building an Enterprise Chatbot: Work with Protected Enterprise Data Using Open Source Frameworks; Apress: Berkeley, CA, USA, 2019; pp. 281–302. [Google Scholar] [CrossRef]
- Ciechanowski, L.; Przegalinska, A.; Magnuski, M.; Gloor, P. In the shades of the uncanny valley: An experimental study of human–chatbot interaction. Future Gener. Comput. Syst. 2018, 92, 539–548. [Google Scholar] [CrossRef]












Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mlakar, I.; Šafran, V.; Hari, D.; Rojc, M.; Alankuş, G.; Pérez Luna, R.; Ariöz, U. Multilingual Conversational Systems to Drive the Collection of Patient-Reported Outcomes and Integration into Clinical Workflows. Symmetry 2021, 13, 1187. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13071187
Mlakar I, Šafran V, Hari D, Rojc M, Alankuş G, Pérez Luna R, Ariöz U. Multilingual Conversational Systems to Drive the Collection of Patient-Reported Outcomes and Integration into Clinical Workflows. Symmetry. 2021; 13(7):1187. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13071187
Chicago/Turabian StyleMlakar, Izidor, Valentino Šafran, Daniel Hari, Matej Rojc, Gazihan Alankuş, Rafael Pérez Luna, and Umut Ariöz. 2021. "Multilingual Conversational Systems to Drive the Collection of Patient-Reported Outcomes and Integration into Clinical Workflows" Symmetry 13, no. 7: 1187. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13071187