
Design of a 3D-Printed Hand Exoskeleton Based on Force-Myography Control for Assistance and Rehabilitation

 ,
,  ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design Requirements
- As many pieces as possible should be made with 3D printing to allow simple low-cost reproduction, affordable maintenance and easier customization/modification.
- The exoskeletal structure should contact the back of the hand, in order to free the palm and fingers so as to preserve a more natural grip of objects [36]. In this way, the mechanical system is strongly underactuated [46], but it still provides a comfortable grasp, without the need for complex controls [36].
- The torque exerted by the actuator should be capable of extending a paretic hand, which generally tends to be clenched due to muscle spasticity [10].
- The user should be able to activate both the flexion and extension of the hand by using a force-myography control system [47].
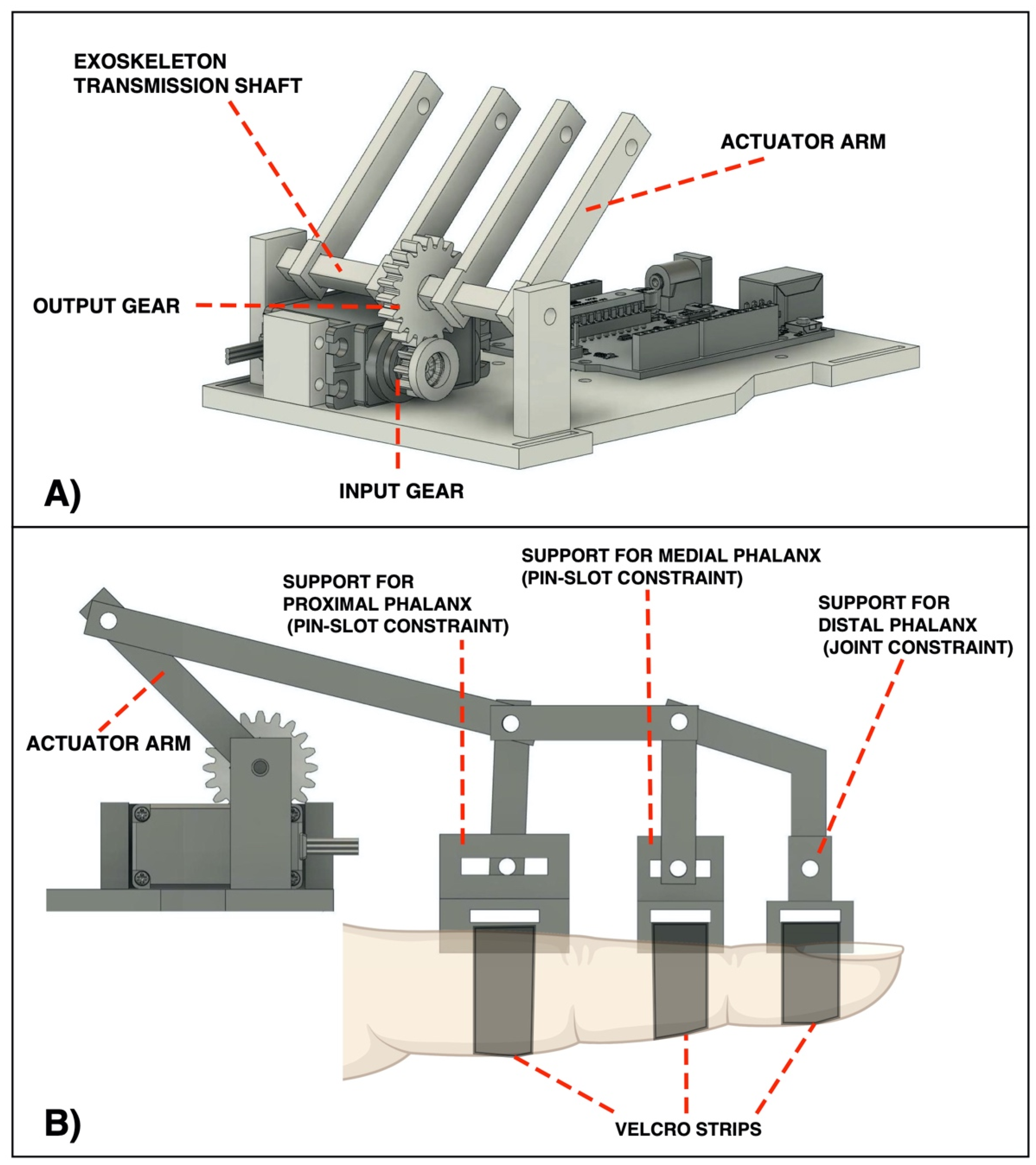
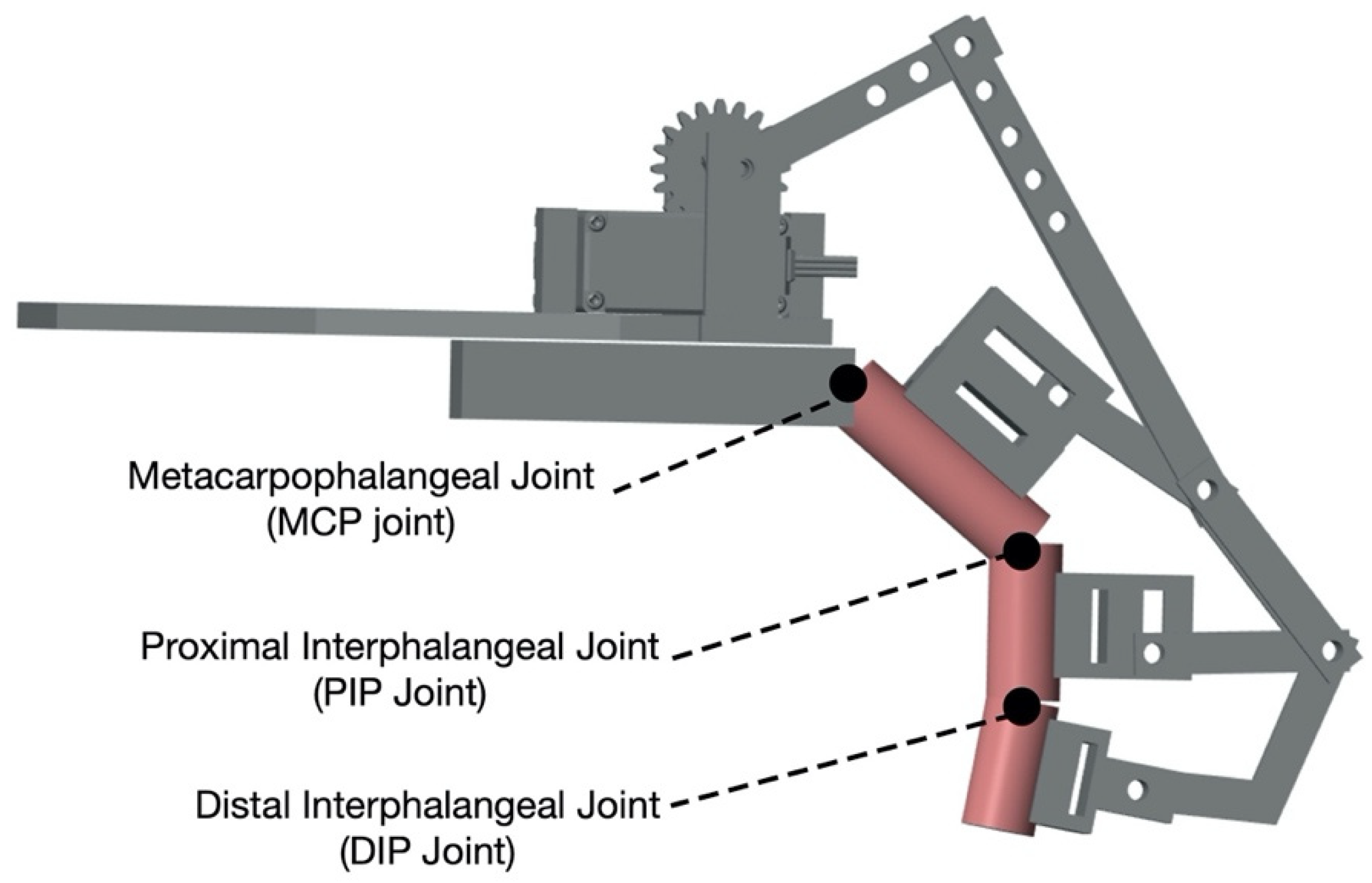
2.2. Hand Exoskeleton Design
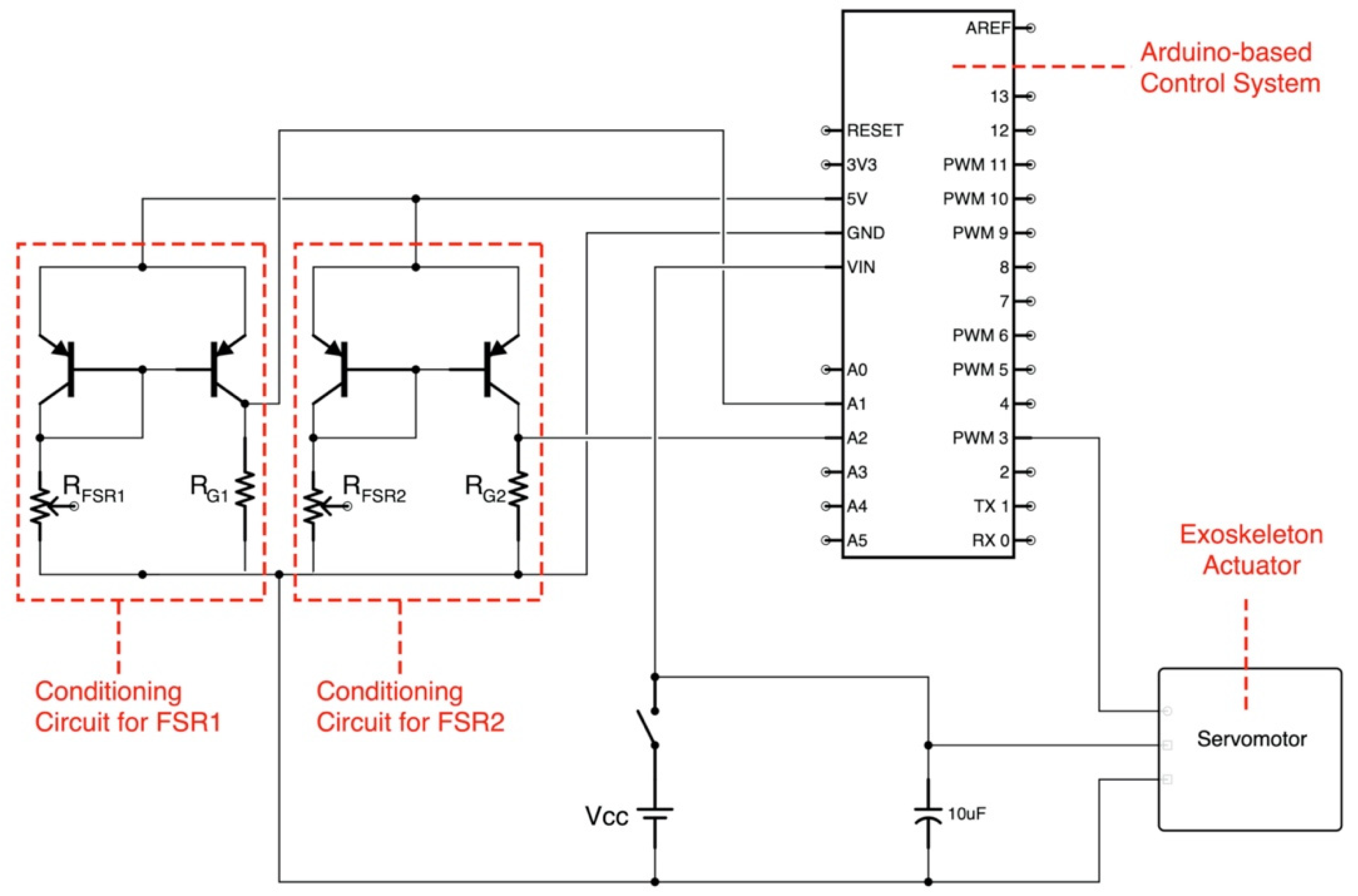
2.3. Control System Based on Force-Myography
2.4. Hand Exoskeleton Setup in the Simulation Environment
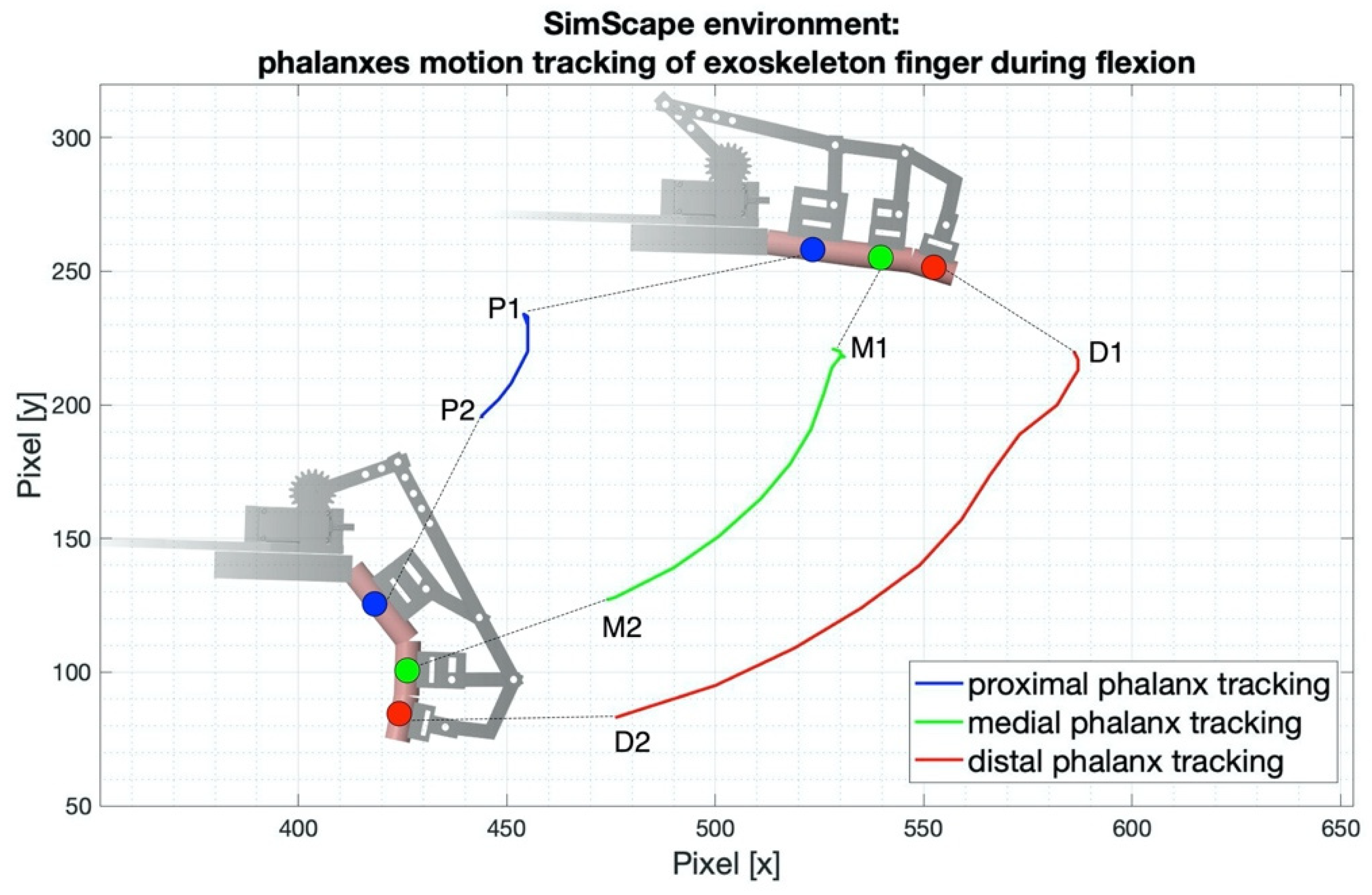
2.5. Kinematics Evaluation
2.6. Power Grasp Force Test
3. Results
3.1. Hand Exoskeleton Behavior in the Simulation Environment
3.2. Kinematics Evaluation Results
3.3. Power Grasp Test Results
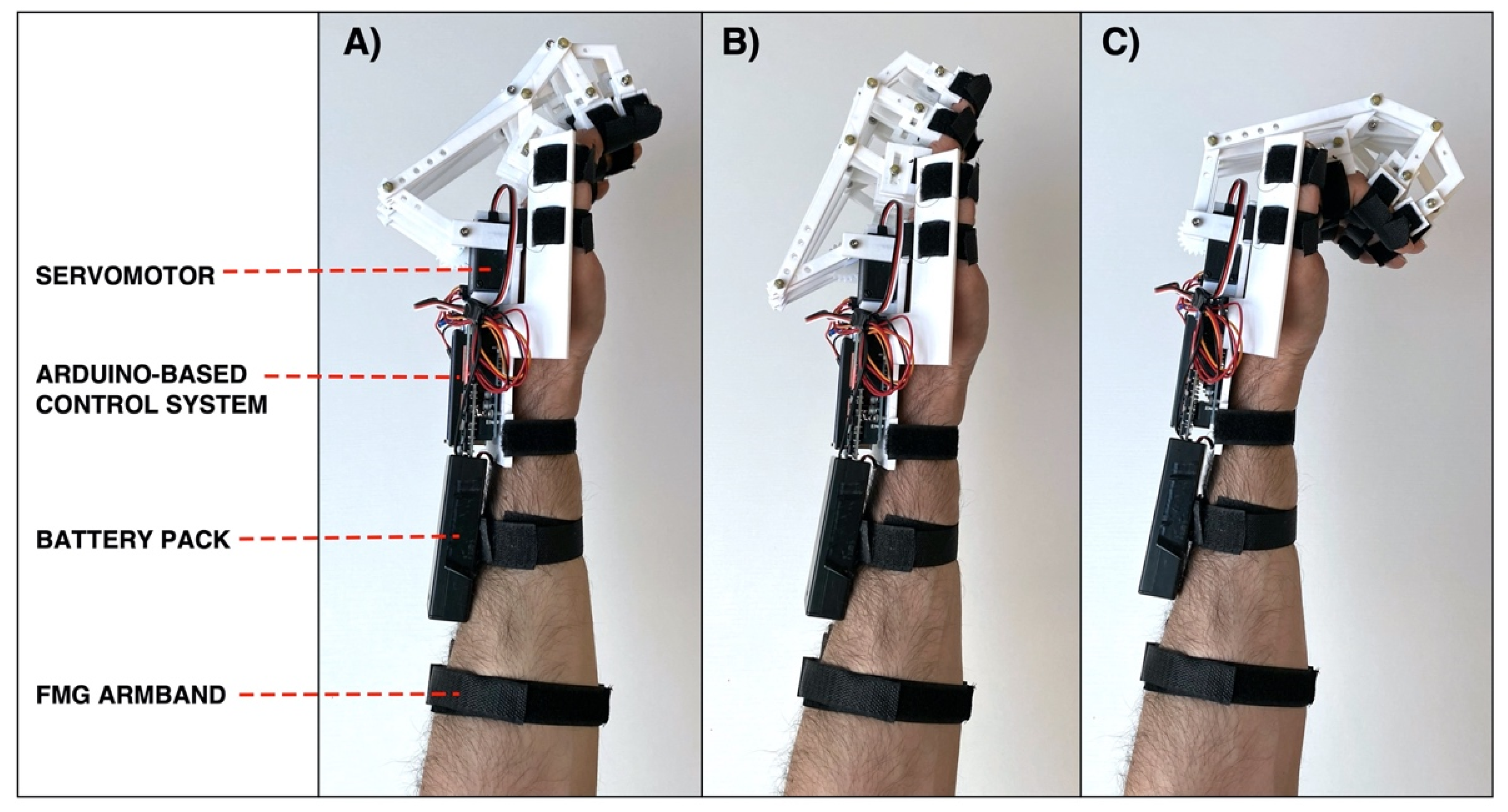
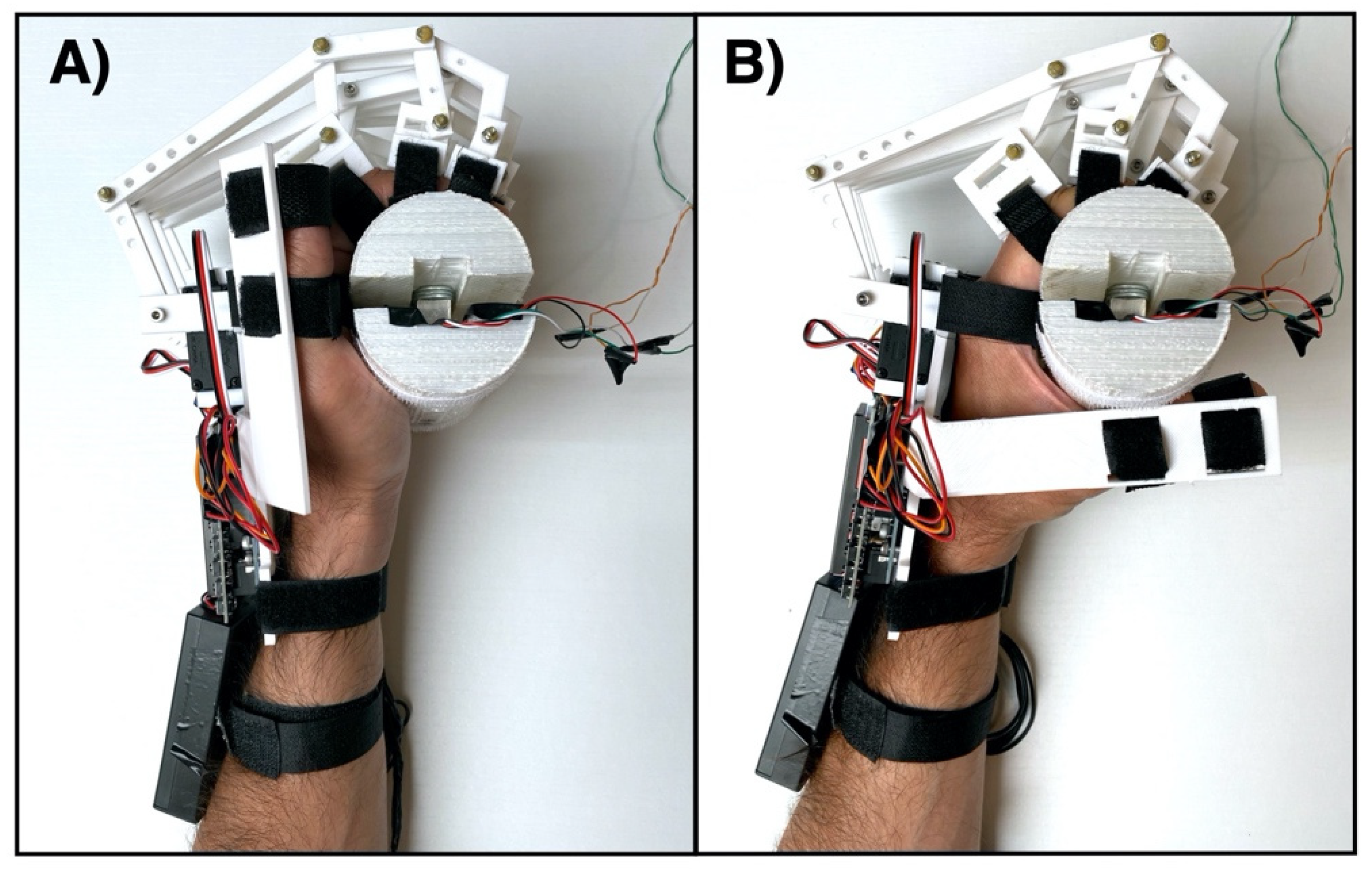
3.4. Current Realization of the Hand Exoskeleton
4. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tjahyono, A.P.; Aw, K.C.; Devaraj, H.; Surendra, W.; Haemmerle, E.; Travas-Sejdic, J. A Five-fingered Hand Exoskeleton Driven by Pneumatic Artificial Muscles with Novel Polypyrrole Sensors. Ind. Robot. Int. J. 2013, 40, 251–260. [Google Scholar] [CrossRef]
- Bi, Q.; Yang, C. Human-Machine Interaction Force Control: Using a Model-Referenced Adaptive Impedance Device to Control an Index Finger Exoskeleton. J. Zhejiang Univ. Sci. C 2014, 15, 275–283. [Google Scholar] [CrossRef]
- Burton, T.M.W.; Vaidyanathan, R.; Burgess, S.C.; Turton, A.J.; Melhuish, C. Development of a Parametric Kinematic Model of the Human Hand and a Novel Robotic Exoskeleton. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–7. [Google Scholar]
- Kuswanto, D.; Iskandriawan, B.; Mahardhika, P.S. Power Grip Exoskeleton Design as Rehabilitation Devices for Post-Stroke Survivors. In Proceedings of the 2018 1st International Conference on Bioinformatics, Biotechnology, and Biomedical Engineering—Bioinformatics and Biomedical Engineering, Yogyakarta, Indonesia, 19–20 October 2018. [Google Scholar] [CrossRef]
- Hatem, S.M.; Saussez, G.; della Faille, M.; Prist, V.; Zhang, X.; Dispa, D.; Bleyenheuft, Y. Rehabilitation of Motor Function after Stroke: A Multiple Systematic Review Focused on Techniques to Stimulate Upper Extremity Recovery. Front. Hum. Neurosci. 2016, 10, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mawase, F.; Cherry-Allen, K.; Xu, J.; Anaya, M.; Uehara, S.; Celnik, P. Pushing the Rehabilitation Boundaries: Hand Motor Impairment Can Be Reduced in Chronic Stroke. Neurorehabil. Neural. Repair. 2020, 34, 733–745. [Google Scholar] [CrossRef] [PubMed]
- Cordo, P.; Wolf, S.; Lou, J.-S.; Bogey, R.; Stevenson, M.; Hayes, J.; Roth, E. Treatment of Severe Hand Impairment Following Stroke by Combining Assisted Movement, Muscle Vibration, and Biofeedback. J. Neurol. Phys. Ther. 2013, 37, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Kamper, D.G.; Fischer, H.C.; Cruz, E.G.; Rymer, W.Z. Weakness Is the Primary Contributor to Finger Impairment in Chronic Stroke. Arch. Phys. Med. Rehabil. 2006, 87, 1262–1269. [Google Scholar] [CrossRef] [PubMed]
- Ates, S.; Haarman, C.J.W.; Stienen, A.H.A. SCRIPT Passive Orthosis: Design of Interactive Hand and Wrist Exoskeleton for Rehabilitation at Home after Stroke. Auton. Robot 2017, 41, 711–723. [Google Scholar] [CrossRef] [Green Version]
- James, C.; Kathye, L.; Sangbum, K.; Mary, T.; Andrea, B. Chronic Motor Dysfunction After Stroke. Stroke 2000, 31, 1360–1364. [Google Scholar] [CrossRef]
- Schabowsky, C.N.; Godfrey, S.B.; Holley, R.J.; Lum, P.S. Development and Pilot Testing of HEXORR: Hand EXOskeleton Rehabilitation Robot. J. NeuroEngineering Rehabil. 2010, 7, 36. [Google Scholar] [CrossRef] [Green Version]
- McConnell, A.; Kong, X.; Vargas, P.A. A Novel Robotic Assistive Device for Stroke-Rehabilitation. In Proceedings of the 23rd IEEE International Symposium on Robot and Human Interactive Communication, Edinburgh, UK, 25–29 August 2014; pp. 917–923. [Google Scholar]
- Lee, S.W.; Landers, K.A.; Park, H.-S. Development of a Biomimetic Hand Exotendon Device (BiomHED) for Restoration of Functional Hand Movement Post-Stroke. IEEE Trans. Neural. Syst. Rehabil. Eng. 2014, 22, 886–898. [Google Scholar] [CrossRef] [Green Version]
- Lindberg, P.G.; Roche, N.; Robertson, J.; Roby-Brami, A.; Bussel, B.; Maier, M.A. Affected and Unaffected Quantitative Aspects of Grip Force Control in Hemiparetic Patients after Stroke. Brain Res. 2012, 1452, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Aqueveque, P.; Ortega, P.; Pino, E.; Saavedra, F.; Germany, E.; Gómez, B. After Stroke Movement Impairments: A Review of Current Technologies for Rehabilitation. In Disabilities—Therapeutic Implications; Under, T., Ed.; InTechOpen: London, UK, 2017; pp. 95–116. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.A.; Al-Jumaily, A. Design and Development of a Hand Exoskeleton for Rehabilitation Following Stroke. Procedia Eng. 2012, 41, 1028–1034. [Google Scholar] [CrossRef] [Green Version]
- Dobkin, B.H. Strategies for Stroke Rehabilitation. Lancet Neurol. 2004, 3, 528–536. [Google Scholar] [CrossRef] [Green Version]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke Rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Esposito, D.; Centracchio, J.; Andreozzi, E.; Gargiulo, G.D.; Naik, G.R.; Bifulco, P. Biosignal-Based Human–Machine Interfaces for Assistance and Rehabilitation: A Survey. Sensors 2021, 21, 6863. [Google Scholar] [CrossRef]
- du Plessis, T.; Djouani, K.; Oosthuizen, C. A Review of Active Hand Exoskeletons for Rehabilitation and Assistance. Robotics 2021, 10, 40. [Google Scholar] [CrossRef]
- Basmajian, J.V.; Luca, C.J. Muscles Alive: Their Functions Revealed by Electromyography. J. Med. Educ. 1962, 37, 802. [Google Scholar]
- Konrad, P. The ABC of EMG: A Practical Introduction to Kinesiological Electromyography, 1st ed.; Noraxon: Scottsdale, AZ, USA, 2005. [Google Scholar]
- Gargiulo, G.; Bifulco, P.; McEwan, A.; Nasehi Tehrani, J.; Calvo, R.A.; Romano, M.; Ruffo, M.; Shephard, R.; Cesarelli, M.; Jin, C.; et al. Dry Electrode Bio-Potential Recordings. Annu. Int. Conf. IEEE. Eng. Med. Biol. Soc. 2010, 2010, 6493–6496. [Google Scholar] [CrossRef] [Green Version]
- Esposito, D.; Andreozzi, E.; Fratini, A.; Gargiulo, G.D.; Savino, S.; Niola, V.; Bifulco, P. A Piezoresistive Sensor to Measure Muscle Contraction and Mechanomyography. Sensors 2018, 18, 2553. [Google Scholar] [CrossRef] [Green Version]
- Esposito, D.; Gargiulo, G.D.; Parajuli, N.; Cesarelli, G.; Andreozzi, E.; Bifulco, P. Measurement of Muscle Contraction Timing for Prosthesis Control: A Comparison between Electromyography and Force-Myography. In Proceedings of the 2020 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Bari, Italy, 1 June–1 July 2020; pp. 1–6. [Google Scholar]
- Esposito, D.; Savino, S.; Andreozzi, E.; Cosenza, C.; Niola, V.; Bifulco, P. The “Federica” Hand. Bioengineering 2021, 8, 128. [Google Scholar] [CrossRef]
- Esposito, D.; Cosenza, C.; Gargiulo, G.D.; Andreozzi, E.; Niola, V.; Fratini, A.; D’Addio, G.; Bifulco, P. Experimental Study to Improve “Federica” Prosthetic Hand and Its Control System. In Proceedings of the XV Mediterranean Conference on Medical and Biological Engineering and Computing—MEDICON 2019, Coimbra, Portugal, 26–28 September 2019; pp. 586–593. [Google Scholar]
- Esposito, D.; Savino, S.; Cosenza, C.; Gargiulo, G.D.; Fratini, A.; Cesarelli, G.; Bifulco, P. Study on the Activation Speed and the Energy Consumption of “Federica” Prosthetic Hand. In Proceedings of the XV Mediterranean Conference on Medical and Biological Engineering and Computing—MEDICON 2019, Coimbra, Portugal, 26–28 September 2019; pp. 594–603. [Google Scholar]
- Esposito, D.; Savino, S.; Cosenza, C.; Andreozzi, E.; Gargiulo, G.D.; Polley, C.; Cesarelli, G.; D’Addio, G.; Bifulco, P. Evaluation of Grip Force and Energy Efficiency of the “Federica” Hand. Machines 2021, 9, 25. [Google Scholar] [CrossRef]
- Esposito, D.; Andreozzi, E.; Gargiulo, G.D.; Fratini, A.; D’Addio, G.; Naik, G.R.; Bifulco, P. A Piezoresistive Array Armband With Reduced Number of Sensors for Hand Gesture Recognition. Front. Neurorobot. 2020, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, D.; Gargiulo, G.D.; Polley, C.; D’Addio, G.; Bifulco, P. Improvements of a Simple Piezoresistive Array Armband for Gesture Recognition. In Proceedings of the 2020 International Conference on e-Health and Bioengineering (EHB), Iasi, Romania, 29–30 October 2020; pp. 1–5. [Google Scholar]
- Andreozzi, E.; Centracchio, J.; Punzo, V.; Esposito, D.; Polley, C.; Gargiulo, G.D.; Bifulco, P. Respiration Monitoring via Forcecardiography Sensors. Sensors 2021, 21, 3996. [Google Scholar] [CrossRef] [PubMed]
- Andreozzi, E.; Fratini, A.; Esposito, D.; Naik, G.; Polley, C.; Gargiulo, G.D.; Bifulco, P. Forcecardiography: A Novel Technique to Measure Heart Mechanical Vibrations onto the Chest Wall. Sensors 2020, 20, 3885. [Google Scholar] [CrossRef] [PubMed]
- Andreozzi, E.; Gargiulo, G.D.; Esposito, D.; Bifulco, P. A Novel Broadband Forcecardiography Sensor for Simultaneous Monitoring of Respiration, Infrasonic Cardiac Vibrations and Heart Sounds. Front. Physiol. 2021, 12, 1988. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.R.U.; Waris, A.; Kamavuako, E.N.; Bai, S. A Comparative Study of Motion Detection with FMG and SEMG Methods for Assistive Applications. J. Rehabil. Assist. Technol. Eng. 2020, 7, 2055668320938588. [Google Scholar] [CrossRef] [PubMed]
- Randazzo, L.; Iturrate, I.; Perdikis, S.; Millán, J.d.R. Mano: A Wearable Hand Exoskeleton for Activities of Daily Living and Neurorehabilitation. IEEE Robot Autom. Lett. 2018, 3, 500–507. [Google Scholar] [CrossRef] [Green Version]
- Araujo, R.S.; Silva, C.R.; Netto, S.P.N.; Morya, E.; Brasil, F.L. Development of a Low-Cost EEG-Controlled Hand Exoskeleton 3D Printed on Textiles. Front. Neurosci. 2021, 15, 661569. [Google Scholar] [CrossRef]
- Wege, A.; Zimmermann, A. Electromyography Sensor Based Control for a Hand Exoskeleton. In Proceedings of the 2007 IEEE International Conference on Robotics and Biomimetics (ROBIO), Sanya, China, 15–18 December 2007. [Google Scholar] [CrossRef]
- Ho, N.S.K.; Tong, K.Y.; Hu, X.L.; Fung, K.L.; Wei, X.J.; Rong, W.; Susanto, E.A. An EMG-Driven Exoskeleton Hand Robotic Training Device on Chronic Stroke Subjects: Task Training System for Stroke Rehabilitation. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–5. [Google Scholar]
- Dwivedi, A.; Gerez, L.; Hasan, W.; Yang, C.-H.; Liarokapis, M. A Soft Exoglove Equipped With a Wearable Muscle-Machine Interface Based on Forcemyography and Electromyography. IEEE Robot. Autom. Lett. 2019, 4, 3240–3246. [Google Scholar] [CrossRef]
- Carson, R.G. Neural Pathways Mediating Bilateral Interactions between the Upper Limbs. Brain Res. Rev. 2005, 49, 641–662. [Google Scholar] [CrossRef]
- Summers, J.J.; Kagerer, F.A.; Garry, M.I.; Hiraga, C.Y.; Loftus, A.; Cauraugh, J.H. Bilateral and Unilateral Movement Training on Upper Limb Function in Chronic Stroke Patients: A TMS Study. J. Neurol. Sci. 2007, 252, 76–82. [Google Scholar] [CrossRef]
- Loconsole, C.; Leonardis, D.; Barsotti, M.; Solazzi, M.; Frisoli, A.; Bergamasco, M.; Troncossi, M.; Foumashi, M.M.; Mazzotti, C.; Castelli, V.P. An Emg-Based Robotic Hand Exoskeleton for Bilateral Training of Grasp. In Proceedings of the 2013 World Haptics Conference (WHC), Daejeon, Korea, 14–17 April 2013; pp. 537–542. [Google Scholar]
- Ueki, S.; Kawasaki, H.; Ito, S.; Nishimoto, Y.; Abe, M.; Aoki, T.; Ishigure, Y.; Ojika, T.; Mouri, T. Development of a Hand-Assist Robot With Multi-Degrees-of-Freedom for Rehabilitation Therapy. IEEE/ASME Trans. Mechatron. 2012, 17, 136–146. [Google Scholar] [CrossRef]
- Cortese, M.; Cempini, M.; de Almeida Ribeiro, P.R.; Soekadar, S.R.; Carrozza, M.C.; Vitiello, N. A Mechatronic System for Robot-Mediated Hand Telerehabilitation. IEEE/ASME Trans. Mechatron. 2015, 20, 1753–1764. [Google Scholar] [CrossRef]
- Liu, Y.; Yu, H. A Survey of Underactuated Mechanical Systems. IET Control. Theory Appl. 2013, 7, 921–935. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Z.G.; Menon, C. A Review of Force Myography Research and Development. Sensors 2019, 19, 4557. [Google Scholar] [CrossRef] [Green Version]
- Fusion 360|3D CAD, CAM, CAE & PCB Cloud-Based Software|Autodesk. Available online: https://www.autodesk.com/products/fusion-360/overview (accessed on 22 June 2021).
- Arduino Uno Rev3|Arduino Official Store. Available online: https://store.arduino.cc/arduino-uno-rev3 (accessed on 18 November 2020).
- Simscape Multibody. Available online: https://it.mathworks.com/products/simscape-multibody.html (accessed on 22 June 2021).
- Boissy, P.; Bourbonnais, D.; Carlotti, M.M.; Gravel, D.; Arsenault, B.A. Maximal Grip Force in Chronic Stroke Subjects and Its Relationship to Global Upper Extremity Function. Clin. Rehabil. 1999, 13, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Kinovea. Available online: https://www.kinovea.org/ (accessed on 4 September 2021).
- Dollar, A.M. Classifying Human Hand Use and the Activities of Daily Living. In The Human Hand as an Inspiration for Robot Hand Development; Balasubramanian, R., Santos, V.J., Eds.; Springer International Publishing: Cham, Switzerland, 2014; pp. 201–216. ISBN 978-3-319-03017-3. [Google Scholar]
- Mat Rosly, M.; Mat Rosly, H.; Davis Oam, G.M.; Husain, R.; Hasnan, N. Exergaming for Individuals with Neurological Disability: A Systematic Review. Disabil. Rehabil. 2017, 39, 727–735. [Google Scholar] [CrossRef]
- Pong. Wikipedia 2021. Available online: https://en.wikipedia.org/wiki/Pong (accessed on 8 September 2021).














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Specification |
|---|---|
| size | suitable for an adult man |
| weight | 380 g (500 g including the battery pack) |
| modularity | Yes |
| actuator | 1 servomotor (25 kg/cm) |
| degrees of freedom (DOF) | 11 |
| hand closing time (from trigger to complete closure) | ≈0.9 s |
| hand opening time (from trigger to complete opening) | ≈0.9 s |
| power grasp force | 94.61 N (SD: 1.92 N) |
| energy power | 2 × 3.7 V batteries (3000 mAh) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esposito, D.; Centracchio, J.; Andreozzi, E.; Savino, S.; Gargiulo, G.D.; Naik, G.R.; Bifulco, P. Design of a 3D-Printed Hand Exoskeleton Based on Force-Myography Control for Assistance and Rehabilitation. Machines 2022, 10, 57. https://0-doi-org.brum.beds.ac.uk/10.3390/machines10010057
Esposito D, Centracchio J, Andreozzi E, Savino S, Gargiulo GD, Naik GR, Bifulco P. Design of a 3D-Printed Hand Exoskeleton Based on Force-Myography Control for Assistance and Rehabilitation. Machines. 2022; 10(1):57. https://0-doi-org.brum.beds.ac.uk/10.3390/machines10010057
Chicago/Turabian StyleEsposito, Daniele, Jessica Centracchio, Emilio Andreozzi, Sergio Savino, Gaetano D. Gargiulo, Ganesh R. Naik, and Paolo Bifulco. 2022. "Design of a 3D-Printed Hand Exoskeleton Based on Force-Myography Control for Assistance and Rehabilitation" Machines 10, no. 1: 57. https://0-doi-org.brum.beds.ac.uk/10.3390/machines10010057