
Electrocardiogram Quality Assessment with a Generalized Deep Learning Model Assisted by Conditional Generative Adversarial Networks


Abstract
:1. Introduction
2. Materials and Methods
2.1. Datasets Introduction and Construction
2.2. Methods
2.2.1. Data Augmentation
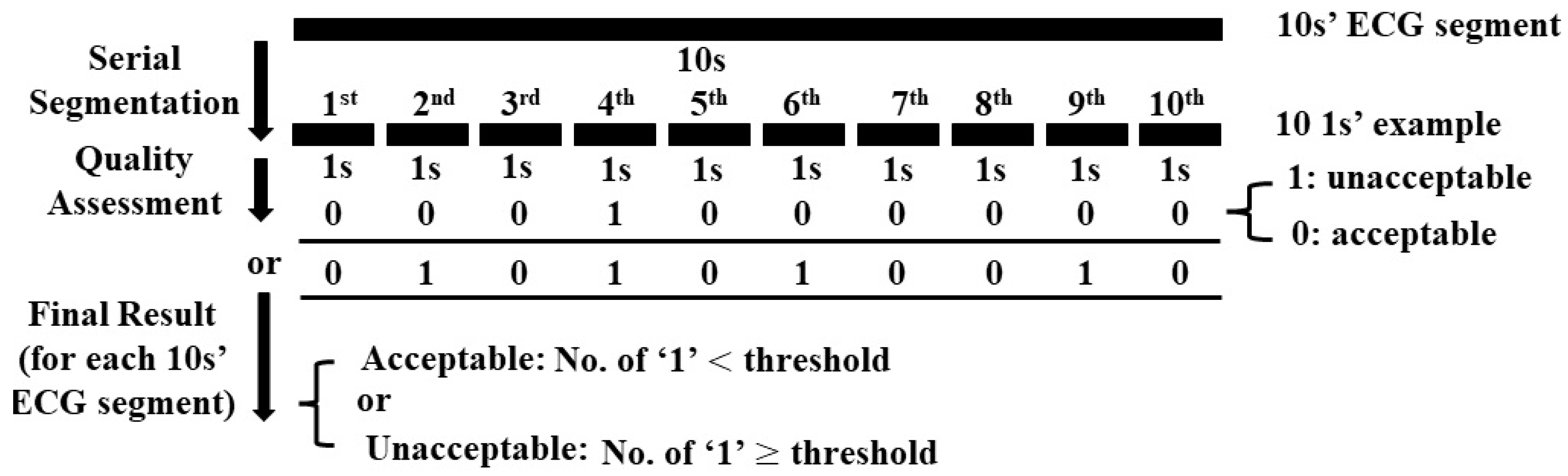
2.2.2. Quality Assessment
3. Results
3.1. Data Augmentation
3.2. Quality Assessment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Augmentation | Performance of Quality Assessment | Remark | ||
|---|---|---|---|---|
| Model | Duration of Generated ECG | COMD | RECD | |
| CGANs | 10 s | acc: 97.1%; sen: 98.6%; spe: 96.4% | acc: 96.4%; sen: 99.1%; spe: 95.0% | Proposed method |
| CGANs | 1 s | acc: 95.5%; sen: 94.5%; spe: 96.0% | - | - |
| GANs | 10 s | - | - | GANs: convergence failed |
| GANs | 1 s | acc: 95.4%; sen: 99.3%; spe: 93.4% | - | - |
| CGANs | 10 s | acc: 84.1%; sen: 75.8%; spe: 88.2% | - | Directly using 10 s ECG segments for assessment model development, and adding L2 regularization in CNN, LSTM, and Dense layers, but the model still performs overfitting; acc: 95.8% vs. 84.1% (trainng set vs. testing set); sen: 91.2% vs. 75.8%; spe: 98.0% vs. 88.2% |
| - | - | acc: 94.1%; sen: 96.5%; spe: 92.9% | acc: 94.0%; sen: 98.1%; spe: 91.9% | Without data augmentation, but segment each 10 s ECG segment to 10 examples with 1 s duration to naturally increase the number of examples. |
| - | - | acc: 95.8%; sen: 96.5%; spe: 95.5% | acc: 93.8%; sen: 89.0%; spe: 96.2% | Using shallow model and downsampled ECG segments, which is similar to the previous work [35], to avoid overfitting. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baig, M.M.; Gholamhosseini, H.; Connolly, M.J. A comprehensive survey of wearable and wireless ECG monitoring systems for older adults. Med. Biol. Eng. Comput. 2013, 51, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Rosiek, A.; Leksowski, K. The risk factors and prevention of cardiovascular disease: The importance of electrocardiogram in the diagnosis and treatment of acute coronary syndrome. Ther. Clin. Risk Manag. 2016, 12, 1223–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaffer, F.; Ginsberg, J.P. An overview of heart rate variability metrics and norms. Front. Public Health 2017, 5, 285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maršánová, L.; Ronzhina, M.; Smíšek, R.; Vítek, M.; Němcová, A.; Smital, L.; Nováková, M. ECG features and methods for automatic classification of ventricular premature and ischemic heartbeats: A comprehensive experimental study. Sci. Rep. 2017, 7, 1–11. [Google Scholar]
- Satija, U.; Ramkumar, B.; Manikandan, M.S. A review of signal processing techniques for electrocardiogram signal quality assessment. IEEE Rev. Biomed. Eng. 2018, 11, 36–52. [Google Scholar] [CrossRef] [PubMed]
- Improving the Quality of ECGs Collected Using Mobile Phones—The PhysioNet Computing in Cardiology Challenge 2011. Available online: https://www.physionet.org/content/challenge-2011/1.0.0/ (accessed on 3 August 2021).
- Moody, G.B.; Muldrow, W.; Mark, R.G. A noise stress test for arrhythmia detectors. Comput. Cardiol. 1984, 11, 381–384. [Google Scholar]
- Tsien, C.L.; Fackler, J.C. Poor prognosis for existing monitors in the intensive care unit. Crit. Care Med. 1997, 25, 614–619. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef] [Green Version]
- Quesnel, P.X.; Chan, A.D.; Yang, H. Real-time biosignal quality analysis of ambulatory ECG for detection of myocardial ischemia. In Proceedings of the 2013 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Gatineau, QC, Canada, 4–5 May 2013. [Google Scholar]
- Redmond, S.J.; Xie, Y.; Chang, D.; Basilakis, J.; Lovell, N.H. Electrocardiogram signal quality measures for unsupervised telehealth environments. Physiol. Meas. 2012, 33, 1517–1533. [Google Scholar] [CrossRef]
- Shahriari, Y.; Fidler, R.; Pelter, M.M.; Bai, Y.; Villaroman, A.; Hu, X. Electrocardiogram signal quality assessment based on structural image similarity metric. IEEE Trans. Biomed. Eng. 2017, 65, 745–753. [Google Scholar] [CrossRef]
- Zhao, Z.; Zhang, Y. SQI quality evaluation mechanism of single-lead ECG signal based on simple heuristic fusion and fuzzy comprehensive evaluation. Front. Physiol. 2018, 9, 727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moeyersons, J.; Smets, E.; Morales, J.; Villa, A.; De Raedt, W.; Testelmans, D.; Buyse, B.; Van Hoof, C.; Willems, R.; Van Huffel, S.; et al. Artefact detection and quality assessment of ambulatory ECG signals. Comput. Methods Programs Biomed. 2019, 182, 105050. [Google Scholar] [CrossRef]
- Fu, F.; Xiang, W.; An, Y.; Liu, B.; Chen, X.; Zhu, S.; Li, J. Comparison of Machine Learning Algorithms for the Quality Assessment of Wearable ECG Signals Via Lenovo H3 Devices. J. Med. Biol. Eng. 2021, 41, 231–240. [Google Scholar] [CrossRef]
- MATLAB R2019b. Available online: https://www.tensorflow.org/learn (accessed on 11 December 2020).
- TensorFlow. Available online: https://jp.mathworks.com/products/new_products/release2019b.html (accessed on 7 January 2021).
- AF Classification from a Short Single Lead ECG Recording—The PhysioNet Computing in Cardiology Challenge 2017. Available online: https://physionet.org/content/challenge-2017/1.0.0/ (accessed on 1 December 2020).
- Khamis, H.; Weiss, R.; Xie, Y.; Chang, C.W.; Lovell, N.H.; Redmond, S.J. TELE ECG Database: 250 Telehealth ECG Records (Collected Using Dry Metal Electrodes) with Annotated QRS and Artifact Masks, and MATLAB Code for the UNSW Artifact Detection and UNSW QRS Detection Algorithms. Harvard Dataverse, V3. Available online: https://dataverse.harvard.edu/dataset.xhtml?persistentId=doi:10.7910/DVN/QTG0EP (accessed on 1 December 2020).
- Moody, G.B.; Mark, R.G. The impact of the MIT-BIH arrhythmia database. IEEE Eng. Med. Biol. Mag. 2001, 20, 45–50. [Google Scholar] [CrossRef] [PubMed]
- MIT-BIH Normal Sinus Rhythm Database. Available online: https://physionet.org/content/nsrdb/1.0.0/ (accessed on 1 December 2020).
- Khamis, H.; Weiss, R.; Xie, Y.; Chang, C.W.; Lovell, N.H.; Redmond, S.J. QRS detection algorithm for telehealth electrocardiogram recordings. IEEE Trans. Biomed. Eng. 2016, 63, 1377–1388. [Google Scholar] [CrossRef] [PubMed]
- The WFDB Software Package. Available online: https://archive.physionet.org/physiotools/wfdb.shtml (accessed on 1 December 2020).
- Dong, Q.; Gong, S.; Zhu, X. Imbalanced deep learning by minority class incremental rectification. IEEE Trans. Pattern Anal. Mach. Intelligence. 2018, 41, 1367–1381. [Google Scholar] [CrossRef] [Green Version]
- Japkowicz, N.; Stephen, S. The class imbalance problem: A systematic study. Intell. Data Anal. 2002, 6, 429–449. [Google Scholar] [CrossRef]
- Wulan, N.; Wang, W.; Sun, K.; Xia, Y.; Zhang, H. Generating electrocardiogram signals by deep learning. Neurocomputing 2020, 404, 122–136. [Google Scholar] [CrossRef]
- Goodfellow, I.J.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial nets. Adv. Neural Inf. Process. Syst. 2014, 2014, 2672–2680. [Google Scholar]
- Zhu, F.; Ye, F.; Fu, Y.; Liu, Q.; Shen, B. Electrocardiogram generation with a bidirectional LSTM-CNN generative adversarial network. Sci. Rep. 2019, 9, 6734. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Hou, B.; Shao, S.; Yan, R. ECG arrhythmias detection using auxiliary classifier generative adversarial network and residual network. IEEE Access 2019, 7, 100910–100922. [Google Scholar] [CrossRef]
- Ye, F.; Zhu, F.; Fu, Y.; Shen, B. ECG generation with sequence generative adversarial nets optimized by policy gradient. IEEE Access 2019, 7, 159369–159378. [Google Scholar] [CrossRef]
- Hazra, D.; Byun, Y. SynSigGAN: Generative Adversarial Networks for Synthetic Biomedical Signal Generation. Biology 2020, 9, 441. [Google Scholar] [CrossRef] [PubMed]
- Mirza, M.; Osindero, S. Conditional generative adversarial nets. arXiv 2014, arXiv:1411.1784. [Google Scholar]
- Maaten, L.V.D.; Hinton, G. Visualizing data using t-SNE. J. Mach Learn Res. 2008, 9, 2579–2605. [Google Scholar]
- Jeon, E.; Oh, K.; Kwon, S.; Son, H.; Yun, Y.; Jung, E.S.; Kim, M.S. A Lightweight Deep Learning Model for Fast Electrocardiographic Beats Classification With a Wearable Cardiac Monitor: Development and Validation Study. JMIR Med. Inform. 2020, 8, e17037. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Zhu, X.; Nakamura, K.; Noro, M. ECG quality assessment using 1D-convolutional neural network. In Proceedings of the 2018 14th IEEE International Conference on Signal Processing (ICSP), Beijing, China, 12–16 August 2018; pp. 780–784. [Google Scholar]
- McSharry, P.E.; Clifford, G.D.; Tarassenko, L.; Smith, L.A. A dynamical model for generating synthetic electrocardiogram signals. IEEE Trans. Biomed. Eng. 2003, 50, 289–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roonizi, E.K.; Sameni, R. Morphological modeling of cardiac signals based on signal decomposition. Comput. Biol. Med. 2013, 43, 1453–1461. [Google Scholar] [CrossRef]








| Noise Type | MIT-BIHA | MIT-BIHNSR |
|---|---|---|
| bw | - | “19093”, “19140”, “19830” |
| em | - | All 17 recordings |
| ma | “101_V1”, “106_V1”, “112_V1”, “113_V1”, “114_V5”, “115_V1”, “122_V1”, “200_V1”, “205_V1”, “209_V1”, “215_V1”, “220_V1”, “221_V1”, “222_MLII” | All 17 recordings |
| bw, g | - | Recordings expect “19093”, “19140”, “19830” (Total 14 recordings) |
| bw, p | - | Recordings expect “19093”, “19140”, “19830” (Total 14 recordings) |
| em, g | “101_V1”, “106_V1”, “112_V1”, “113_V1”, “114_V5”, “115_V1”, “122_V1”, “200_V1”, “205_V1”, “209_V1”, “215_V1”, “220_V1”, “221_V1”, “222_MLII” | - |
| ma, bw | “112”, “113”, “114”, “115”, “116”, “117”, “118”, “119”, “121”, “122”, “123” | - |
| ma, em | “124”, “200”, “201”, “202”, “203”, “205”, “207”, “208”, “209”, “210”, “213”, “214”, “215” | All 17 recordings |
| bw, g, p | “101_V1”, “106_V1”, “112_V1”, “113_V1”, “114_V5”, “115_V1”, “122_V1”, “200_V1”, “205_V1”, “209_V1”, “215_V1”, “220_V1”, “221_V1”, “222_MLII” | - |
| em, bw, g | “212”, “217”, “219”, “220”, “221”, “228”, “230”, “231”, “232”, “233”, “234” | - |
| ma, em, bw | “100”, “101”, “102”, “103”, “104”, “105”, “106”, “107”, “108”, “109”, “111” | - |
| g | first 5 min of each recording | first 5 min of each recording |
| p | first 5 min of each recording | first 5 min of each recording |
| Usage | COMD | Generated Unacceptable ECG | RECD | |||
|---|---|---|---|---|---|---|
| Training Set | Testing Set | Parts of Acceptable ECG | Training Set | Testing Set | ||
| Train CGANs | √ | - | - | |||
| Pretrain Assessment Model | - | √ | √ | - | ||
| Finetune Assessment Model | √ | - | - | - | √ | - |
| Test Assessment Model | - | √ | - | - | - | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, X.; Zhu, X.; Nakamura, K.; Noro, M. Electrocardiogram Quality Assessment with a Generalized Deep Learning Model Assisted by Conditional Generative Adversarial Networks. Life 2021, 11, 1013. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101013
Zhou X, Zhu X, Nakamura K, Noro M. Electrocardiogram Quality Assessment with a Generalized Deep Learning Model Assisted by Conditional Generative Adversarial Networks. Life. 2021; 11(10):1013. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101013
Chicago/Turabian StyleZhou, Xue, Xin Zhu, Keijiro Nakamura, and Mahito Noro. 2021. "Electrocardiogram Quality Assessment with a Generalized Deep Learning Model Assisted by Conditional Generative Adversarial Networks" Life 11, no. 10: 1013. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101013