
High Risk for Attention-Deficit Hyperactive Disorder in Children with Strabismus: A Nationwide Cohort Study from the National Health Insurance Research Database


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
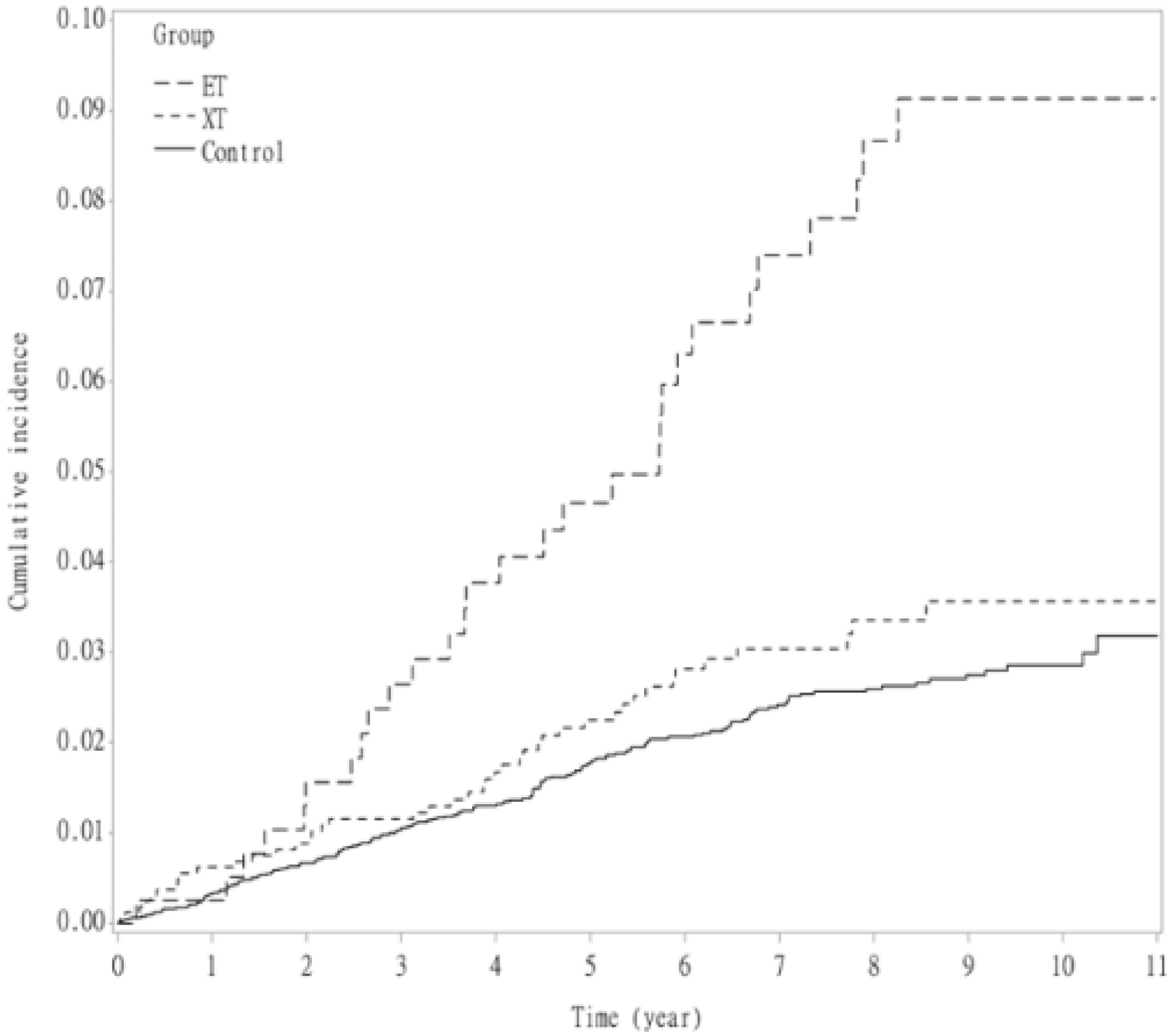
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mohney, B.G.; Greenberg, A.E.; Diehl, N.N. Age at Strabismus Diagnosis in an Incidence Cohort of Children. Am. J. Ophthalmol. 2007, 144, 467–469. [Google Scholar] [CrossRef]
- McKean-Cowdin, R.; Cotter, S.A.; Tarczy-Hornoch, K.; Wen, G.; Kim, J.; Borchert, M.; Varma, R.; Multi-Ethnic Pediatric Eye Disease Study Group. Prevalence of Amblyopia or Strabismus in Asian and Non-Hispanic White Preschool Children: Multi-Ethnic Pediatric Eye Disease Study. Ophthalmology 2013, 120, 2117–2124. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.C.; Quah, B.L.; Balakrishnan, V.; Lim, H.C.; Tay, V.; Emmanuel, S.C. Vision Screening of 4-Year-Old Children in Singapore. Singap. Med. J. 2000, 41, 271–278. [Google Scholar]
- Ip, J.M.; Robaei, D.; Kifley, A.; Wang, J.J.; Rose, K.A.; Mitchell, P. Prevalence of hyperopia and associations with eye findings in 6- and 12-year-olds. Ophthalmology 2008, 115, 678–685. [Google Scholar] [CrossRef]
- Yu, C.B.; Fan, D.S.; Wong, V.W.; Wong, C.Y.; Lam, D.S. Changing Patterns of Strabismus: A Decade of Experience in Hong Kong. Br. J. Ophthalmol. 2002, 86, 854–856. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Hunter, D.G. Amblyopia: Diagnostic and Therapeutic Options. Am. J. Ophthalmol. 2006, 141, 175–184. [Google Scholar] [CrossRef]
- Fox, R.; Aslin, R.N.; Shea, S.L.; Dumais, S.T. Stereopsis in Human Infants. Science 1980, 207, 323–324. [Google Scholar] [CrossRef]
- Sim, B.; Yap, G.H.; Chia, A. Functional and Psychosocial Impact of Strabismus on Singaporean Children. J. AAPOS 2014, 18, 178–182. [Google Scholar] [CrossRef]
- Hatt, S.R.; Leske, D.A.; Castañeda, Y.S.; Wernimont, S.M.; Liebermann, L.; Cheng-Patel, C.S.; Birch, E.E.; Holmes, J.M. Association of Strabismus with Functional Vision and Eye-Related Quality of Life in Children. JAMA Ophthalmol. 2020, 138, 528–535. [Google Scholar] [CrossRef]
- Schuster, A.K.; Elflein, H.M.; Pokora, R.; Schlaud, M.; Baumgarten, F.; Urschitz, M.S. Health-Related Quality of Life and Mental Health in Children and Adolescents With Strabismus—Results of the Representative Population-Based Survey KiGGS. Health Qual. Life Outcomes 2019, 17, 81. [Google Scholar] [CrossRef] [Green Version]
- Mohney, B.G.; McKenzie, J.A.; Capo, J.A.; Nusz, K.J.; Mrazek, D.; Diehl, N.N. Mental Illness in Young Adults Who Had Strabismus as Children. Pediatrics 2008, 122, 1033–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, M.Y.; Lee, K.M.; Hwang, J.M.; Choi, D.G.; Lee, D.S.; Park, K.H.; Yu, Y.S. Comparison Between Anisometropic and Strabismic Amblyopia Using Functional Magnetic Resonance Imaging. Br. J. Ophthalmol. 2001, 85, 1052–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Li, S.H.; Zhou, F.Q.; Zhang, Y.; Zhong, Y.L.; Cai, F.Q.; Shao, Y.; Zeng, X.J. Altered Intrinsic Regional Brain Spontaneous Activity in Patients With Comitant Strabismus: A Resting-State Functional MRI Study. Neuropsychiatr. Dis. Treat. 2016, 12, 1303–1308. [Google Scholar] [CrossRef] [Green Version]
- Thomas, R.; Sanders, S.; Doust, J.; Beller, E.; Glasziou, P. Prevalence of Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis. Pediatrics 2015, 135, e994–e1001. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, L.S.; Levitt, J.G.; O’Neill, J.; Alger, J.R.; Luders, E.; Phillips, O.R.; Caplan, R.; Toga, A.W.; McCracken, J.; Narr, K.L. Reduced White Matter Integrity in Attention-Deficit Hyperactivity Disorder. NeuroReport 2008, 19, 1705–1708. [Google Scholar]
- Loe, I.M.; Feldman, H.M. Academic and Educational Outcomes of Children With ADHD. J. Pediatr. Psychol. 2007, 32, 643–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merrell, C.; Tymms, P.B. Inattention, Hyperactivity and Impulsiveness: Their Impact on Academic Achievement and Progress. Br. J. Educ. Psychol. 2001, 71, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Eyre, O.; Riglin, L.; Leibenluft, E.; Stringaris, A.; Collishaw, S.; Thapar, A. Irritability in ADHD: Association With Later Depression Symptoms. Eur. Child Adolesc. Psychiatry 2019, 28, 1375–1384. [Google Scholar] [CrossRef] [Green Version]
- Dalsgaard, S. Attention-Deficit/Hyperactivity Disorder (ADHD). Eur. Child Adolesc. Psychiatry 2013, 22 (Suppl. 1), S43–S48. [Google Scholar] [CrossRef]
- Faraone, S.V.; Biederman, J. Neurobiology of Attention-Deficit Hyperactivity Disorder. Biol. Psychiatry 1998, 44, 951–958. [Google Scholar] [CrossRef]
- Leslie, L.K.; Weckerly, J.; Plemmons, D.; Landsverk, J.; Eastman, S. Implementing the American Academy of Pediatrics Attention-Deficit/Hyperactivity Disorder Diagnostic Guidelines in Primary Care Settings. Pediatrics 2004, 114, 129–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.; Congdon, N.; Yam, J.C.; Huang, Y.; Qiu, K.; Ma, D.; Chen, B.; Li, L.; Zhang, M. Alcohol Use and Positive Screening Results for Depression and Anxiety Are Highly Prevalent Among Chinese Children With Strabismus. Am. J. Ophthalmol. 2014, 157, 894–900.e1. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.B.; Hodge, D.O.; Mohney, B.G. Prevalence of Mental Health Illness Among Patients with Adult-Onset Strabismus. Strabismus 2015, 23, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohney, B.G. Intermittent Exotropia and Mental Illness. Am. Orthopt. J. 2016, 66, 25–29. [Google Scholar] [CrossRef]
- Kilgore, K.P.; Barraza, R.A.; Hodge, D.O.; McKenzie, J.A.; Mohney, B.G. Surgical Correction of Childhood Intermittent Exotropia and the Risk of Developing Mental Illness. Am. J. Ophthalmol. 2014, 158, 788–792.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granet, D.B.; Gomi, C.F.; Ventura, R.; Miller-Scholte, A. The Relationship Between Convergence Insufficiency and ADHD. Strabismus 2005, 13, 163–168. [Google Scholar] [CrossRef] [PubMed]
- DeCarlo, D.K.; Bowman, E.; Monroe, C.; Kline, R.; McGwin, G., Jr.; Owsley, C. Prevalence of Attention-Deficit/Hyperactivity Disorder Among Children With Vision Impairment. J. AAPOS 2014, 18, 10–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reimelt, C.; Wolff, N.; Hölling, H.; Mogwitz, S.; Ehrlich, S.; Roessner, V. The Underestimated Role of Refractive Error (Hyperopia, Myopia, and Astigmatism) and Strabismus in Children With ADHD. J. Atten. Disord. 2021, 25, 235–244. [Google Scholar] [CrossRef] [PubMed]
- DeCarlo, D.K.; Swanson, M.; McGwin, G.; Visscher, K.; Owsley, C. ADHD and Vision Problems in the National Survey of Children’s Health. Optom. Vis. Sci. 2016, 93, 459–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chia, A.; Dirani, M.; Chan, Y.H.; Gazzard, G.; Au Eong, K.G.; Selvaraj, P.; Ling, Y.; Quah, B.L.; Young, T.L.; Mitchell, P.; et al. Prevalence of Amblyopia and Strabismus in Young Singaporean Chinese Children. Investig. Ophthalmol. Vis. Sci. 2010, 51, 3411–3417. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.W.; Zhu, H.; Yu, J.J.; Ding, H.; Bai, J.; Chen, J.; Yu, R.-B.; Liu, H. Epidemiology of Intermittent Exotropia in Preschool children in China. Optom. Vis. Sci. 2016, 93, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.H.; Wang, A.H.; Hu, F.R.; Tsai, T.H. Exploring the Divergence Range for Stereopsis Maintenance With a Computer-Simulated Troposcope in Patients With Intermittent Exotropia. Investig. Ophthalmol. Vis. Sci. 2016, 57, 4493–4497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, A.E.; Mohney, B.G.; Diehl, N.N.; Burke, J.P. Incidence and Types of Childhood Esotropia: A Population-Based Study. Ophthalmology 2007, 114, 170–174. [Google Scholar] [CrossRef]
- Atkinson, J.; Braddick, O. Visual Development. Handb. Clin. Neurol. 2020, 173, 121–142. [Google Scholar] [CrossRef] [PubMed]
- Hakim, R.B.; Tielsch, J.M. Maternal cigarette smoking during pregnancy: A risk factor for childhood strabismus. Arch. Ophthalmol. 1992, 110, 1459–1462. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.L., 3rd; Hung, L.F.; Arumugam, B.; Wensveen, J.M.; Chino, Y.M.; Harwerth, R.S. Observations on the Relationship Between Anisometropia, Amblyopia and Strabismus. Vis. Res. 2017, 134, 26–42. [Google Scholar] [CrossRef] [PubMed]
- Su, C.C.; Tsai, C.Y.; Tsai, T.H.; Tsai, I.J. Incidence and Risk of Attention-Deficit Hyperactivity Disorder in Children With Amblyopia: A Nationwide Cohort Study. Clin. Exp. Ophthalmol. 2019, 47, 259–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konrad, K.; Eickhoff, S.B. Is the ADHD Brain Wired Differently? A Review on Structural and Functional Connectivity in Attention Deficit Hyperactivity Disorder. Hum. Brain Mapp. 2010, 31, 904–916. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.; Norcia, A.M.; Yeatman, J.D.; Mezer, A. The Structural Properties of Major White Matter Tracts in Strabismic Amblyopia. Investig. Ophthalmol. Vis. Sci. 2015, 56, 5152–5160. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, F.X.; Margulies, D.S.; Kelly, C.; Uddin, L.Q.; Ghaffari, M.; Kirsch, A.; Shaw, D.; Shehzad, Z.; Di Martino, A.; Biswal, B.; et al. Cingulate-Precuneus Interactions: A New Locus of Dysfunction in Adult Attention-Deficit/Hyperactivity Disorder. Biol. Psychiatry 2008, 63, 332–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogt, B.A. Cingulate Impairments in ADHD: Comorbidities, Connections, and Treatment. Handb. Clin. Neurol. 2019, 166, 297–314. [Google Scholar]
- Ten Tusscher, M.P.M.; Houtman, A.C.; De Mey, J.; Van Schuerbeek, P. Cortical Visual Connections via the Corpus Callosum Are Asymmetrical in Human Infantile Esotropia. Strabismus 2018, 26, 22–27. [Google Scholar] [CrossRef]
- Cao, Q.; Sun, L.; Gong, G.; Lv, Y.; Cao, X.; Shuai, L.; Zhu, C.; Zang, Y.; Wang, Y. The Macrostructural and Microstructural Abnormalities of Corpus Callosum in Children With Attention Deficit/Hyperactivity Disorder: A Combined Morphometric and Diffusion Tensor MRI Study. Brain Res. 2010, 1310, 172–180. [Google Scholar] [CrossRef]
- Gilliam, M.; Stockman, M.; Malek, M.; Sharp, W.; Greenstein, D.; Lalonde, F.; Clasen, L.; Giedd, J.; Rapoport, J.; Shaw, P. Developmental Trajectories of the Corpus Callosum in Attention-Deficit/Hyperactivity Disorder. Biol. Psychiatry 2011, 69, 839–846. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.Y.; Warren-Gash, C.; Smeeth, L.; Chen, P.C. Data Resource Profile: The National Health Insurance Research Database (NHIRD). Epidemiol. Health 2018, 40, e2018062. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total | Strabismus Group | Esotropia | Exotropia | Non-Strabismus Group | p-Value * |
|---|---|---|---|---|---|---|
| n = 44330 | n = 2049 | n = 404 | n = 1645 | n = 8196 | ||
| Age, no. (%) | ||||||
| ≤7 | 3197 (31.2) | 650 (31.7) | 233 (57.7) | 417 (25.3) | 2547 (31.1) | 0.7168 |
| 7– ≤ 12 | 4180 (40.8) | 820 (40.0) | 100 (24.8) | 720 (43.8) | 3360 (41.0) | |
| 12– ≤ 18 | 2868 (28.0) | 579 (28.3) | 71 (17.6) | 508 (30.9) | 2289 (27.9) | |
| Mean (SD) | 9.2 (4.2) | 9.2 (4.2) | 6.9 (4.7) | 9.8 (3.8) | 9.2 (4.2) | 0.9987 |
| Female | 5440 (53.1) | 1088 (53.1) | 219 (54.2) | 869 (52.8) | 4352 (53.1) | 1.0000 |
| Duration of follow-up (year) | ||||||
| Mean (SD) | 6.5 (2.9) | 6.5 (2.9) | 7.2 (3.0) | 6.4 (2.9) | 6.5 (2.9) | 0.7877 |
| Median (interquartile range) | 6.9 (4.4, 9.1) | 6.9 (4.3, 9.1) | 8.1 (5.1, 9.8) | 6.7 (4.2, 8.9) | 6.9 (4.4, 9.1) | |
| Comorbiditities **, no. (%) | ||||||
| Autism spectrum disorder | 7 (0.1) | 7 (0.3) | 1 (0.2) | 6 (0.4) | 0 (0.0) | <0.0001 |
| Tourette syndrome (Tics) | 3 (0.0) | 2 (0.1) | 0 (0.0) | 2 (0.1) | 1 (0.0) | 0.1040 |
| oppositional defiant disorder | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| depression | 4 (0.0) | 3 (0.1) | 1 (0.2) | 2 (0.1) | 1 (0.0) | 0.0272 |
| Delayed development | 48 (0.5) | 37 (1.8) | 12 (3.0) | 25 (1.5) | 11 (0.1) | <0.0001 |
| Intellectual disability | 10 (0.1) | 7 (0.3) | 1 (0.2) | 6 (0.4) | 3 (0.0) | 0.0009 |
| Stuttering | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.0) | |
| Obsessive compulsive disorder | 1 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.0) | 0.6171 |
| Conduct disorder | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.0) | |
| Encopresis | 6 (0.1) | 4 (0.2) | 0 (0.0) | 4 (0.2) | 2 (0.0) | 0.0043 |
| Feeding and eating disorder | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Prematurity, low birth weight | 7 (0.1) | 6 (0.3) | 2 (0.5) | 4 (0.2) | 1 (0.0) | 0.0004 |
| Perinatal infection | 5 (0.0) | 5 (0.2) | 5 (1.2) | 0 (0.0) | 0 (0.0) | 0.0003 |
| Fetal and newborn respiratory condition | 1 (0.0) | 1 (0.0) | 0 (0.0) | 1 (0.1) | 0 (0.0) | 0.2000 |
| Birth condition | 2 (0.0) | 1 (0.0) | 0 (0.0) | 1 (0.1) | 1 (0.0) | 0.3600 |
| Birth trauma | 1 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.0) | 1.0000 |
| Intrauterine hypoxia and birth asphyxia | 1 (0.0) | 1 (0.0) | 1 (0.2) | 0 (0.0) | 0 (0.0) | 0.2000 |
| Lower respiratory tract infection | 1846 (18.0) | 597 (29.1) | 159 (39.4) | 438 (26.6) | 1249 (15.2) | <0.0001 |
| Paralysis | 29 (0.3) | 26 (1.3) | 4 (1.0) | 22 (1.3) | 3 (0.0) | <0.0001 |
| Headaches | 74 (0.7) | 40 (2.0) | 8 (2.0) | 32 (1.9) | 34 (0.4) | <0.0001 |
| Epilepsy | 28 (0.3) | 16 (0.8) | 0 (0.0) | 16 (1.0) | 12 (0.1) | <0.0001 |
| Rheumatic disease | 2 (0.0) | 2 (0.1) | 0 (0.0) | 2 (0.1) | 0 (0.0) | 0.0400 |
| Chronic pulmonary disease | 376 (3.7) | 112 (5.5) | 23 (5.7) | 89 (5.4) | 264 (3.2) | <0.0001 |
| asthma | 289 (2.8) | 90 (4.4) | 18 (4.5) | 72 (4.4) | 199 (2.4) | <0.0001 |
| allergic rhinitis | 606 (5.9) | 245 (12.0) | 49 (12.1) | 196 (11.9) | 361 (4.4) | <0.0001 |
| allergic conjunctivitis | 191 (1.9) | 91 (4.4) | 8 (2.0) | 83 (5.0) | 100 (1.2) | <0.0001 |
| Deficiency anemias | 6 (0.1) | 4 (0.2) | 0 (0.0) | 4 (0.2) | 2 (0.0) | 0.0169 |
| ADHD Events | PY | Incidence † | Hazard Ratio (95% C.I.) | ||
|---|---|---|---|---|---|
| Crude | Adjusted | ||||
| Comparison group | 173 | 53615 | 3.23 | 1 (reference) | 1 (reference) |
| All patients | 72 | 13370 | 5.39 | 1.67 (1.27, 2.20) ** | 1.64 (1.23, 2.17) ** |
| Patients with ET | 29 | 2920 | 9.93 | 3.14 (2.12, 4.65) ** | 2.04 (1.36, 3.06) ** |
| Patients with XT | 43 | 10450 | 4.11 | 1.27 (0.91, 1.77) | 1.44 (1.03, 2.03) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, C.-Y.; Su, C.-C.; Liu, Y.-L.; Tsai, I.-J.; Tsai, T.-H. High Risk for Attention-Deficit Hyperactive Disorder in Children with Strabismus: A Nationwide Cohort Study from the National Health Insurance Research Database. Life 2021, 11, 1139. https://0-doi-org.brum.beds.ac.uk/10.3390/life11111139
Tsai C-Y, Su C-C, Liu Y-L, Tsai I-J, Tsai T-H. High Risk for Attention-Deficit Hyperactive Disorder in Children with Strabismus: A Nationwide Cohort Study from the National Health Insurance Research Database. Life. 2021; 11(11):1139. https://0-doi-org.brum.beds.ac.uk/10.3390/life11111139
Chicago/Turabian StyleTsai, Chia-Ying, Chien-Chia Su, Yao-Lin Liu, I-Ju Tsai, and Tzu-Hsun Tsai. 2021. "High Risk for Attention-Deficit Hyperactive Disorder in Children with Strabismus: A Nationwide Cohort Study from the National Health Insurance Research Database" Life 11, no. 11: 1139. https://0-doi-org.brum.beds.ac.uk/10.3390/life11111139