
Tracheal Repair with Human Umbilical Cord Mesenchymal Stem Cells Differentiated in Chondrocytes Grown on an Acellular Amniotic Membrane: A Pre-Clinical Approach

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Experimental Design
2.3. Isolation and Characterization of hucMSCs/Amniotic Membrane Decellularization
2.4. Flow Cytometry Analysis
2.5. Rabbit Tracheostomy Model and Membrane Implant
2.6. Computed Tomography Scanning Analysis
2.7. Euthanasia
2.8. Histopathological Analysis
2.9. Statistical Analysis
3. Results
3.1. Cell Adhesion and Proliferation
3.2. Computed Tomography Scanning Findings
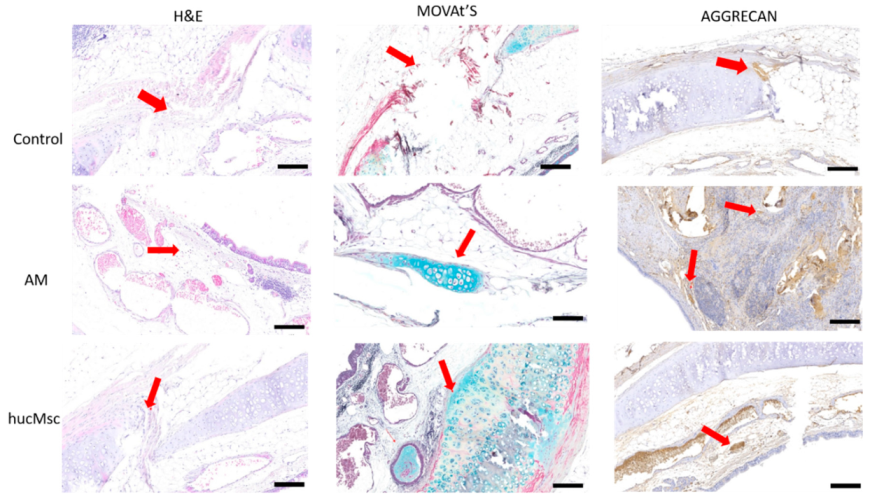
3.3. Histological Analyses
3.4. Collagen Level Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, Z.; Wei, P.; Gan, L.; Zeng, T.; Qin, C.; Liu, G. Role of Erythromycin-Regulated Histone Deacetylase-2 in Benign Tracheal Stenosis. Can. Respir. J. 2020, 2020, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Boswell, S.G.; Cole, B.J.; Sundman, E.A.; Karas, V.; Fortier, L.A. Platelet-Rich Plasma: A Milieu of Bioactive Factors. Arthrosc. J. Arthrosc. Relat. Surg. 2012, 28, 429–439. [Google Scholar] [CrossRef]
- Grillo, H.C. Tracheal replacement: A critical review. Ann Thorac Surg. 2002, 73, 1995–2004. [Google Scholar] [CrossRef]
- Elicora, A.; Liman, S.T.; Yegin, B.A.; Eroglu, H.; Yıldız, K.; Topcu, S.; Ozer, C.; AKGÜL, A.G. Effect of Locally Applied Transforming Growth Factor Beta3 on Wound Healing and Stenosis Development in Tracheal Surgery. Respir. Care 2013, 59, 1281–1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, S.J.; Park, M.-H.; Lee, T.-K.; Choi, S.H. Healing Effect of Platelet-rich Plasma on Decellularized Tracheal Allotransplantation in Rabbits. In Vivo 2018, 32, 1443–1447. [Google Scholar] [CrossRef] [Green Version]
- Etienne, H.; Fabre, D.; Caro, A.G.; Kolb, F.; Mussot, S.; Mercier, O.; Mitilian, D.; Stephan, F.; Fadel, E.; Dartevelle, P. Tracheal replacement. Eur. Respir. J. 2018, 51, 1702211. [Google Scholar] [CrossRef] [PubMed]
- Boys, A.J.; Barron, S.L.; Tilev, D.; Owens, R.M. Building Scaffolds for Tubular Tissue Engineering. Front. Bioeng. Biotechnol. 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Litwiniuk, M.; Grzela, T. Amniotic membrane: New concepts for an old dressing. Wound Repair Regen. 2014, 22, 451–456. [Google Scholar] [CrossRef]
- Nouri, M.; Ebrahimi, M.; Bagheri, T.; Fatemi, M.J.; Najafbeygi, A.; Araghi, S.; Molaee, M. Healing Effects of Dried and Acellular Human Amniotic Membrane and Mepitelas for Coverage of Skin Graft Donor Areas; A Randomized Clinical Trial. Bull. Emerg. Trauma 2018, 6, 195–200. [Google Scholar] [CrossRef] [Green Version]
- Benders, K.E.M.; Van Weeren, P.R.; Badylak, S.F.; Saris, D.B.F.; Dhert, W.J.A.; Malda, J. Extracellular matrix scaffolds for cartilage and bone regeneration. Trends Biotechnol. 2013, 31, 169–176. [Google Scholar] [CrossRef]
- Zhang, Y.; Ding, J.; Ren, S.; Wang, W.; Yang, Y.; Li, S.; Meng, M.; Wu, T.; Liu, D.; Tian, S.; et al. Intravenous infusion of human umbilical cord Wharton’s jelly-derived mesenchymal stem cells as a potential treatment for patients with COVID-19 pneumonia. Stem Cell Res. Ther. 2020, 11, 1–6. [Google Scholar] [CrossRef]
- Chen, Y.; Yu, Y.; Chen, L.; Ye, L.; Cui, J.; Sun, Q.; Li, K.; Li, Z.; Liu, L. Human Umbilical Cord Mesenchymal Stem Cells: A New Therapeutic Option for Tooth Regeneration. Stem Cells Int. 2015, 2015, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving Bioscience Research Reporting: The ARRIVE Guidelines for Reporting Animal Research. Animals 2014, 4, 35–44. [Google Scholar] [CrossRef] [Green Version]
- Hopper, R.A.; Woodhouse, K.; Semple, J.L. Acellularization of Human Placenta with Preservation of the Basement Membrane. Ann. Plast. Surg. 2003, 51, 598–602. [Google Scholar] [CrossRef]
- Jorge, L.F.; Francisco, J.C.; Bergonse, N.; Baena, C.P.; De Carvalho, K.A.T.; Abdelwahid, E.; Neto, J.R.F.; Moreira, L.F.P.; Guarita-Souza, L.C. Tracheal repair with acellular human amniotic membrane in a rabbit model. J. Tissue Eng. Regen. Med. 2017, 12, e1525–e1530. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liu, Z.; Li, Y.; You, Q.; Yang, J.; Jin, Y.; Zou, G.; Tang, J.; Ge, Z.; Liu, Y. FGF-2-Induced Human Amniotic Mesenchymal Stem Cells Seeded on a Human Acellular Amniotic Membrane Scaffold Accelerated Tendon-to-Bone Healing in a Rabbit Extra-Articular Model. Stem Cells Int. 2020, 2020, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, X.; Ma, Y.; Lu, X.; Li, W.; Xia, E.; Li, T.-C.; Zhang, H.; Huang, X. Transplantation of Human Adipose Stem Cells Using Acellular Human Amniotic Membrane Improves Angiogenesis in Injured Endometrial Tissue in a Rat Intrauterine Adhesion Model. Cell Transplant. 2020, 29. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Liu, X.; Yuan, D.; Zhao, J. Human acellular amniotic membrane is adopted to treat venous ulcers. Exp. Ther. Med. 2018, 16, 1285–1289. [Google Scholar] [CrossRef] [Green Version]
- Chun, S.Y.; Lim, G.J.; Kwon, T.G.; Kwak, E.K.; Kim, B.W.; Atala, A.; Yoo, J.J. Identification and characterization of bioactive factors in bladder submucosa matrix. Biomaterials 2007, 28, 4251–4256. [Google Scholar] [CrossRef]
- Du, X.F.; Kwon, S.K.; Song, J.-J.; Cho, C.G.; Park, S.-W. Tracheal reconstruction by mesenchymal stem cells with small intestine submucosa in rabbits. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 345–351. [Google Scholar] [CrossRef]
- Bae, S.-W.; Lee, K.-W.; Park, J.-H.; Lee, J.; Jung, C.-R.; Yu, J.; Kim, H.-Y.; Kim, D.-H. 3D Bioprinted Artificial Trachea with Epithelial Cells and Chondrogenic-Differentiated Bone Marrow-Derived Mesenchymal Stem Cells. Int. J. Mol. Sci. 2018, 19, 1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klin, B.; Weinberg, M.; Vinograd, I.; Sandbank, J.; Siman-Tov, Y.; Astachov, L.; Ayalon, O.; Rochkind, S.; Shahar, A.; Nevo, Z. Experimental Repair of Tracheal Defects Using a New Biodegradable Membrane. J. Laparoendosc. Adv. Surg. Tech. 2007, 17, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.S.; Gabra, N.; Baig, A.; Manoukian, J.J.; Daniel, S.J. Bridging the gap: Using 3D printed polycaprolactone implants to reconstruct circumferential tracheal defects in rabbits. Laryngoscope 2019, 130. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tomography Analysis | |||||
|---|---|---|---|---|---|
| Global Mean | |||||
| Variable | Group | Value (mm2) | Min; Max; Median (mm2) | p Value | Test |
| Lesion Area | C {n = 10) | 18.71 | 11.37; 33.5; 13.1 | 0.211 | ANOVA-Oneway |
| AM {n = 10) | 14.15 | 11.2; 16.1; 14.3 | |||
| AM + hucMSCs {n = 10) | 25.44 | 14.7; 47.4; 18.4 | |||
| Area without Lesion | C {n = 10) | 25.10 | 19.1; 35; 24.2 | 0.811 | Kruskal-Wallis |
| AM {n = 10) | 23.87 | 22.5; 26.2; 23.4 | |||
| AM + hucMSCs {n = 10) | 26.96 | 18.9; 47.9; 19.8 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baggio Simeoni, P.R.; Simeoni, R.B.; Bispo Machado Júnior, P.A.; de Almeida, M.B.; Dziedzic, D.S.M.; da Rosa, N.N.; Ferreira Stricker, P.E.; dos Santos Miggiolaro, A.F.R.; Naves, G.; Neto, N.B.; et al. Tracheal Repair with Human Umbilical Cord Mesenchymal Stem Cells Differentiated in Chondrocytes Grown on an Acellular Amniotic Membrane: A Pre-Clinical Approach. Life 2021, 11, 879. https://0-doi-org.brum.beds.ac.uk/10.3390/life11090879
Baggio Simeoni PR, Simeoni RB, Bispo Machado Júnior PA, de Almeida MB, Dziedzic DSM, da Rosa NN, Ferreira Stricker PE, dos Santos Miggiolaro AFR, Naves G, Neto NB, et al. Tracheal Repair with Human Umbilical Cord Mesenchymal Stem Cells Differentiated in Chondrocytes Grown on an Acellular Amniotic Membrane: A Pre-Clinical Approach. Life. 2021; 11(9):879. https://0-doi-org.brum.beds.ac.uk/10.3390/life11090879
Chicago/Turabian StyleBaggio Simeoni, Paulo Ricardo, Rossana Baggio Simeoni, Paulo André Bispo Machado Júnior, Meila Bastos de Almeida, Dilcele Silva Moreira Dziedzic, Nádia Nascimento da Rosa, Priscila E. Ferreira Stricker, Anna Flávia Ribeiro dos Santos Miggiolaro, Guilherme Naves, Nelson Bergonse Neto, and et al. 2021. "Tracheal Repair with Human Umbilical Cord Mesenchymal Stem Cells Differentiated in Chondrocytes Grown on an Acellular Amniotic Membrane: A Pre-Clinical Approach" Life 11, no. 9: 879. https://0-doi-org.brum.beds.ac.uk/10.3390/life11090879