
Physiotherapeutic Methods in the Treatment of Cervical Discopathy and Degenerative Cervical Myelopathy: A Prospective Study

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
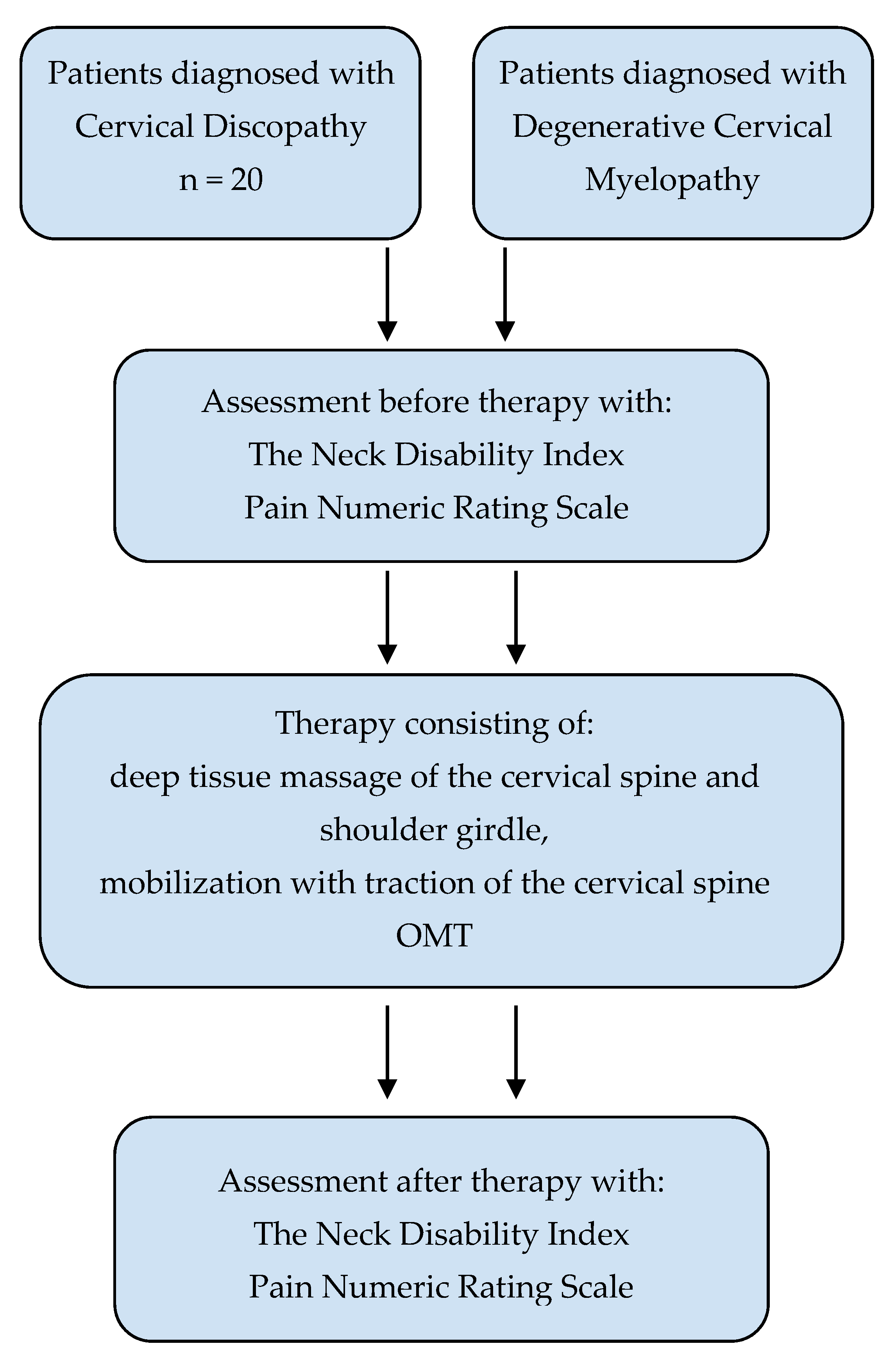
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Interventions
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Clinical Implication
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kushchayev, S.V.; Glushko, T.; Jarraya, M.; Schuleri, K.H.; Preul, M.C.; Brooks, M.L.; Teytelboym, O.M. ABCs of the degenerative spine. Insights Imaging 2018, 9, 253–274. [Google Scholar] [CrossRef] [Green Version]
- Ansari, S.; Amanullah, M.F.; Rauniyar, R.; Ahmad, K. Pott′s spine: Diagnostic imaging modalities and technology advancements. N. Am. J. Med. Sci. 2013, 5, 404. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.-U.; Chang, M.C.; Kim, T.U.; Lee, G.W. Diagnostic Modality in Spine Disease: A Review. Asian Spine J. 2020, 14, 910–920. [Google Scholar] [CrossRef]
- Bogduk, N. Functional Anatomy of the Spine. Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Machino, M.; Yukawa, Y.; Imagama, S.; Ito, K.; Katayama, Y.; Matsumoto, T.; Inoue, T.; Ouchida, J.; Tomita, K.; Ishiguro, N.; et al. Age-Related and Degenerative Changes in the Osseous Anatomy, Alignment, and Range of Motion of the Cervical Spine. Spine 2016, 41, 476–482. [Google Scholar] [CrossRef]
- Mańko, G.; Pieniążek, M.; Tim, S.; Jekiełek, M. The Effect of Frankel’s Stabilization Exercises and Stabilometric Platform in the Balance in Elderly Patients: A Randomized Clinical Trial. Medicina 2019, 55, 583. [Google Scholar] [CrossRef] [Green Version]
- Woods, B.I.; Hilibrand, A.S. Cervical Radiculopathy. J. Spinal Disord. Tech. 2015, 28, E251–E259. [Google Scholar] [CrossRef]
- Nouri, A.; Tetreault, L.; Singh, A.; Karadimas, S.K.; Fehlings, M.G. Degenerative Cervical Myelopathy. Spine 2015, 40, E675–E693. [Google Scholar] [CrossRef]
- Tetreault, L.; Goldstein, C.L.; Arnold, P.; Harrop, J.; Hilibrand, A.; Nouri, A.; Fehlings, M.G. Degenerative Cervical Myelopathy. Neurosurgery 2015, 77, S51–S67. [Google Scholar] [CrossRef] [Green Version]
- Badhiwala, J.H.; Ahuja, C.S.; Akbar, M.A.; Witiw, C.D.; Nassiri, F.; Furlan, J.C.; Curt, A.; Wilson, J.R.; Fehlings, M.G. Degenerative cervical myelopathy—Update and future directions. Nat. Rev. Neurol. 2020, 16, 108–124. [Google Scholar] [CrossRef]
- Kato, S.; Fehlings, M. Degenerative cervical myelopathy. Curr. Rev. Musculoskelet. Med. 2016, 9, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Nouri, A.; Cheng, J.S.; Davies, B.; Kotter, M.; Schaller, K.; Tessitore, E. Degenerative Cervical Myelopathy: A Brief Review of Past Perspectives, Present Developments, and Future Directions. J. Clin. Med. 2020, 9, 535. [Google Scholar] [CrossRef] [Green Version]
- Ayub, A.A.; Anwar, H.A. Cervical myelopathy. Orthop. Trauma 2015, 29, 399–407. [Google Scholar] [CrossRef]
- Grodzinski, N.; Grodzinski, B.; Davies, B.M. Can co-authorship networks be used to predict author research impact? A machine-learning based analysis within the field of degenerative cervical myelopathy research. PLoS ONE 2021, 16, e0256997. [Google Scholar] [CrossRef]
- Côté, P.; Wong, J.J.; Sutton, D.; Shearer, H.M.; Mior, S.; Randhawa, K.; Ameis, A.; Carroll, L.J.; Nordin, M.; Yu, H.; et al. Management of neck pain and associated disorders: A clinical practice guideline from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur. Spine J. 2016, 25, 2000–2022. [Google Scholar] [CrossRef]
- Davies, B.M.; Francis, J.J.; Butler, M.B.; Mowforth, O.; Goacher, E.; Starkey, M.; Kolias, A.; Wynne-Jones, G.; Hutton, M.; Selvanathan, S.; et al. Current surgical practice for multi-level degenerative cervical myelopathy: Findings from an international survey of spinal surgeons. J. Clin. Neurosci. 2021, 87, 84–88. [Google Scholar] [CrossRef]
- Davies, B.M.; Mowforth, O.D.; Smith, E.K.; Kotter, M.R. Degenerative cervical myelopathy. BMJ 2018, 360, k186. [Google Scholar] [CrossRef] [Green Version]
- Milligan, J.; Ryan, K.; Fehlings, M.; Bauman, C. Degenerative cervical myelopathy: Diagnosis and management in primary care. Can. Fam. Physician 2019, 65, 619–624. [Google Scholar]
- Wiedenhöfer, B.; Nacke, J.; Stephan, M.; Richter, W.; Carstens, C.; Eichler, M. Is Total Disk Replacement a Cost-effective Treatment for Cervical Degenerative Disk Disease? Clin. Spine Surg. A Spine Publ. 2017, 30, E530–E534. [Google Scholar] [CrossRef]
- Boisson, M.; Lefèvre-Colau, M.-M.; Rannou, F.; Nguyen, C. Active discopathy: A clinical reality. RMD Open 2018, 4, e000660. [Google Scholar] [CrossRef]
- de Rooij, J.D.; Gadjradj, P.S.; Huygen, F.J.; Luijsterburg, P.A.J.; Harhangi, B.S. Management of Symptomatic Cervical Disk Herniation. Spine 2017, 42, 311–317. [Google Scholar] [CrossRef]
- Masala, S.; Salimei, F.; Lacchè, A.; Marcia, S.; Massari, F. Overview on Percutaneous Therapies of Disc Diseases. Medicina 2019, 55, 471. [Google Scholar] [CrossRef] [Green Version]
- Rubio-Ochoa, J.; Benítez-Martínez, J.; Lluch, E.; Santacruz-Zaragozá, S.; Gómez-Contreras, P.; Cook, C.E. Physical examination tests for screening and diagnosis of cervicogenic headache: A systematic review. Man. Ther. 2016, 21, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Neuwirth, E. Headaches and Facial Pains in Cervical Discopathy. Ann. Intern. Med. 1952, 37, 75. [Google Scholar] [CrossRef] [Green Version]
- Alimoğulları, M.; Buluş, H. Existence of Cervical Discopathy in Non-Cyclic Mastodynia. Breast Care 2020, 15, 178–181. [Google Scholar] [CrossRef]
- Głowacki, M. Kinesiophobia in Pre-Operative Patients with Cervical Discopathy and Coexisting Degenerative Changes in Relation to Pain-Related Variables, Psychological State and Sports Activity. Med. Sci. Monit. 2015, 21, 181–194. [Google Scholar] [CrossRef] [Green Version]
- Lizis, P.; Kobza, W.; Manko, G.; Jaszczur-Nowicki, J.; Perlinski, J.; Para, B. Cryotherapy With Mobilization Versus Cryotherapy With Mobilization Reinforced With Home Stretching Exercises in Treatment of Chronic Neck Pain: A Randomized Trial. J. Manip. Physiol. Ther. 2020, 43, 197–205. [Google Scholar] [CrossRef]
- Northover, J.R.; Wild, J.B.; Braybrooke, J.; Blanco, J. The epidemiology of cervical spondylotic myelopathy. Skelet. Radiol. 2012, 41, 1543–1546. [Google Scholar] [CrossRef]
- Gibson, J.; Nouri, A.; Krueger, B.; Lakomkin, N.; Nasser, R.; Gimbel, D.; Cheng, J. Degenerative Cervical Myelopathy: A Clinical Review. Yale J. Biol. Med. 2018, 91, 43–48. [Google Scholar]
- Saltychev, M.; Mattie, R.; McCormick, Z.; Laimi, K. Psychometric properties of the neck disability index amongst patients with chronic neck pain using item response theory. Disabil. Rehabil. 2018, 40, 2116–2121. [Google Scholar] [CrossRef]
- Hattapoğlu, E.; Batmaz, İ.; Dilek, B.; Karakoç, M.; Em, S.; Çevik, R. Efficiency of pulsed electromagnetic fields on pain, disability, anxiety, depression, and quality of life in patients with cervical disc herniation: A randomized controlled study. Turk. J. Med. Sci. 2019, 49, 1095–1101. [Google Scholar] [CrossRef]
- Kose, N.; Otman, A.S. Comparison of the quality of life of patients with lumbar and cervical disc herniation. Pain Clin. 2004, 16, 281–286. [Google Scholar] [CrossRef]
- Kim, E.J.; Chotai, S.; Schneider, B.J.; Sivaganesan, A.; McGirt, M.J.; Devin, C.J. Effect of Depression on Patient-Reported Outcomes Following Cervical Epidural Steroid Injection for Degenerative Spine Disease. Pain Med. 2018, 19, 2371–2376. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.P.; Mitchell, M.D.; Hacker, R.J.; Riew, K.D.; Sasso, R.C. Single-Level Degenerative Cervical Disc Disease and Driving Disability: Results from a Prospective, Randomized Trial. Glob. Spine J. 2013, 3, 237–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nykänen, M.; Ylinen, J.; Häkkinen, A. Do cervical degenerative changes in women with chronic neck pain affect function? J. Rehabil. Med. 2007, 39, 363–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sipko, T.; Bieć, E.; Demczuk-Włodarczyk, E.; Ciesielska, B. Mobility of cervical spine and postural equilibrium in patients with spinal overload syndrome. Ortop. Traumatol. Rehabil. 2007, 9, 141–148. [Google Scholar]


{kind=link}
| Points | Group D | Group M | ||||||
|---|---|---|---|---|---|---|---|---|
| Median | IQR | Min | Max | Median | IQR | Min | Max | |
| NDI | 24 | 16.25 | 9 | 36 | 35 | 13 | 16 | 45 |
| PNRS | 4.5 | 1.25 | 3 | 6 | 4.67 | 1.58 | 3 | 8.67 |
| Group D | Group M | |||
|---|---|---|---|---|
| Disability | n | % | n | % |
| No disability | 0 | 0 | 0 | 0 |
| Mild disability | 5 | 25 | 0 | 0 |
| Moderate disability | 6 | 30 | 4 | 20 |
| Severe disability | 8 | 40 | 6 | 30 |
| Complete disability | 1 | 5 | 10 | 50 |
| Points | Group D | Group M | ||||||
|---|---|---|---|---|---|---|---|---|
| Median | IQR | Min | Max | Median | IQR | Min | Max | |
| NDI | 4.5 | 5 | 0 | 9 | 10 | 17 | 1 | 18 |
| PNRS | 2 | 0.67 | 1 | 3.33 | 2.33 | 1.25 | 1.33 | 3.67 |
| Distribution of Patients in Groups D and M in Individual Disability Groups after Completing Therapy | Group D | Group M | ||
|---|---|---|---|---|
| Disability | n | % | n | % |
| No disability | 10 | 50 | 4 | 20 |
| Mild disability | 10 | 50 | 12 | 60 |
| Moderate disability | 0 | 0 | 4 | 20 |
| Points | Group D | Group M | ||||||
|---|---|---|---|---|---|---|---|---|
| Median | IQR | Min | Max | Median | IQR | Min | Max | |
| NDI | 20 | 11 | 9 | 31 | 25.5 | 9 | 14 | 32 |
| PNRS | 2.67 | 0.92 | 1.67 | 3.33 | 2.33 | 0.92 | 1.33 | 5.67 |
| Group D | Group M | |||||||
|---|---|---|---|---|---|---|---|---|
| Question | Median | IQR | Min | Max | Median | IQR | Min | Max |
| 1 | 3 | 1.75 | 1 | 4 | 3 | 2 | 2 | 4 |
| 2 | 3 | 2 | 1 | 4 | 3 | 2 | 2 | 4 |
| 3 | 4 | 2 | 1 | 4 | 3 | 2 | 1 | 4 |
| 4 | 1 | 1 | 0 | 4 | 4 | 2 | 1 | 5 |
| 5 | 2 | 2 | 1 | 4 | 4 | 2 | 1 | 5 |
| 6 | 1 | 2 | 0 | 4 | 4 | 1 | 1 | 5 |
| 7 | 2 | 2 | 1 | 4 | 3.5 | 1 | 1 | 5 |
| 8 | 2.5 | 3 | 1 | 4 | 4 | 1 | 1 | 5 |
| 9 | 2.5 | 2 | 0 | 4 | 3 | 2.5 | 0 | 4 |
| 10 | 2 | 2 | 1 | 4 | 4 | 2.5 | 1 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mańko, G.; Jekiełek, M.; Ambroży, T.; Rydzik, Ł.; Jaszczur-Nowicki, J. Physiotherapeutic Methods in the Treatment of Cervical Discopathy and Degenerative Cervical Myelopathy: A Prospective Study. Life 2022, 12, 513. https://0-doi-org.brum.beds.ac.uk/10.3390/life12040513
Mańko G, Jekiełek M, Ambroży T, Rydzik Ł, Jaszczur-Nowicki J. Physiotherapeutic Methods in the Treatment of Cervical Discopathy and Degenerative Cervical Myelopathy: A Prospective Study. Life. 2022; 12(4):513. https://0-doi-org.brum.beds.ac.uk/10.3390/life12040513
Chicago/Turabian StyleMańko, Grzegorz, Małgorzata Jekiełek, Tadeusz Ambroży, Łukasz Rydzik, and Jarosław Jaszczur-Nowicki. 2022. "Physiotherapeutic Methods in the Treatment of Cervical Discopathy and Degenerative Cervical Myelopathy: A Prospective Study" Life 12, no. 4: 513. https://0-doi-org.brum.beds.ac.uk/10.3390/life12040513