
The Occurrence of Nephrolithiasis in Gout Patients: A Longitudinal Follow-Up Study Using a National Health Screening Cohort

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
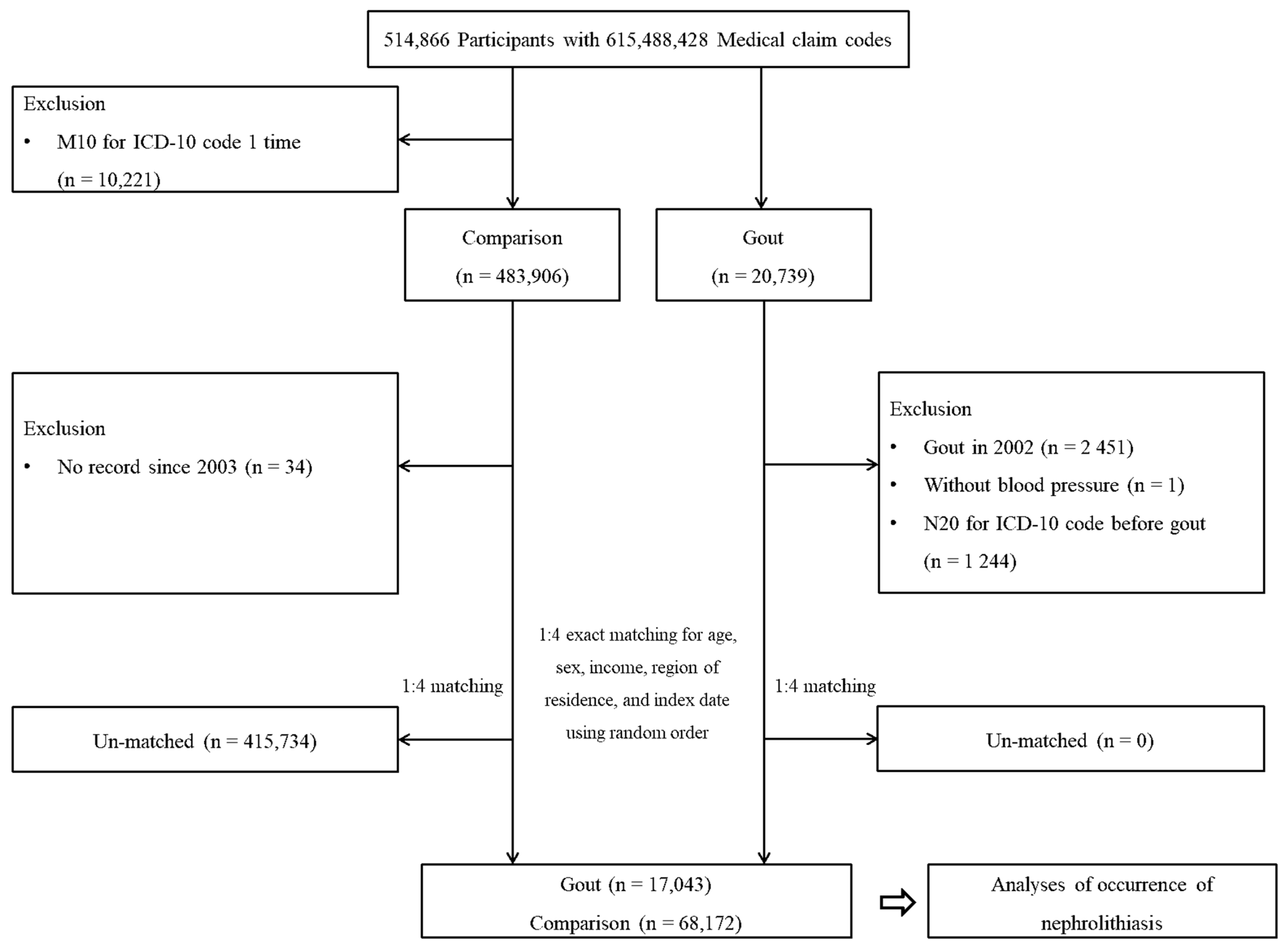
2.1. Study Population
2.2. Participant Selection
2.3. Definition of Gout (Independent Variable)
2.4. Definition of Nephrolithiasis (Dependent Variable)
2.5. Covariates
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scales, C.D., Jr.; Smith, A.C.; .Hanley, J.M.; Saigal, C.S.; Urologic Diseases in America Project. Prevalence of kidney stones in the United States. Eur. Urol. 2012, 62, 160–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziemba, J.B.; Matlaga, B.R. Epidemiology and economics of nephrolithiasis. Investig. Clin. Urol. 2017, 58, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Cicerello, E.; Mangano, M.S.; Cova, G.; Ciaccia, M. Changing in gender prevalence of nephrolithiasis. Urologia 2021, 88, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Moe, O.W. Kidney stones: Pathophysiology and medical management. Lancet 2006, 367, 333–344. [Google Scholar] [CrossRef]
- Lange, J.N.; Mufarrij, P.W.; Wood, K.D.; Holmes, R.P.; Assimos, D.G. The association of cardiovascular disease and metabolic syndrome with nephrolithiasis. Curr. Opin. Urol. 2012, 22, 154–159. [Google Scholar] [CrossRef]
- George, C.; Minter, D.A. Hyperuricemia; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Singh, J.A.; Gaffo, A. Gout epidemiology and comorbidities. Semin. Arthritis. Rheum. 2020, 50, S11–S16. [Google Scholar] [CrossRef]
- Pascual, E.; Sivera, F.; Andres, M. Managing Gout in the Patient with Renal Impairment. Drugs Aging 2018, 35, 263–273. [Google Scholar] [CrossRef]
- Dalbeth, N.; Merriman, T.R.; Stamp, L.K. Gout. Lancet 2016, 388, 2039–2052. [Google Scholar] [CrossRef]
- Dehlin, M.; Jacobsson, L.; Roddy, E. Global epidemiology of gout: Prevalence, incidence, treatment patterns and risk factors. Nat. Rev. Rheumatol. 2020, 16, 380–390. [Google Scholar] [CrossRef]
- Saito, Y.; Tanaka, A.; Node, K.; Kobayashi, Y. Uric acid and cardiovascular disease: A clinical review. J. Cardiol. 2021, 78, 51–57. [Google Scholar] [CrossRef]
- Roughley, M.J.; Belcher, J.; Mallen, C.D.; Roddy, E. Gout and risk of chronic kidney disease and nephrolithiasis: Meta-analysis of observational studies. Arthritis Res. Ther. 2015, 17, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoff, L.S.; Goldenstein-Schainberg, C.; Fuller, R. Nephrolithiasis in gout: Prevalence and characteristics of Brazilian patients. Adv. Rheumatol. 2019, 60, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.X.; Jiao, G.L.; Zhou, S.M.; Cheng, Z.Y.; Bashir, S.; Zhou, Y. Evaluation of the chemical composition of nephrolithiasis using dual-energy CT in Southern Chinese gout patients. BMC Nephrol. 2019, 20, 273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, H.M.; Curhan, G. The association between gout and nephrolithiasis: The National Health and Nutrition Examination Survey III, 1988–1994. Am. J. Kidney Dis. 2002, 40, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Min, C.; Yoo, D.M.; Chang, J.; Lee, H.J.; Park, B.; Choi, H.G. Hearing Impairment Increases Economic Inequality. Clin. Exp. Otorhinolaryngol. 2021, 14, 278–286. [Google Scholar] [CrossRef]
- Seong, S.C.; Kim, Y.Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.J.; Do, C.H.; Song, J.S.; Lee, E.J.; et al. Cohort profile: The National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.W.; Kwak, S.G.; Lee, H.; Kim, S.K.; Choe, J.Y.; Park, S.H. Prevalence and incidence of gout in Korea: Data from the national health claims database 2007–2015. Rheumatol. Int. 2017, 37, 1499–1506. [Google Scholar] [CrossRef]
- Kim, S.Y.; Bang, W.J.; Min, C.; Choi, H.G. Association of nephrolithiasis with the risk of cardiovascular diseases: A longitudinal follow-up study using a national health screening cohort. BMJ Open 2020, 10, e040034. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Bidirectional Association Between GERD and Asthma: Two Longitudinal Follow-Up Studies Using a National Sample Cohort. J. Allergy Clin. Immunol. Pract. 2020, 8, 1005–1013.e9. [Google Scholar] [CrossRef]
- Kim, S.Y.; Oh, D.J.; Park, B.; Choi, H.G. Bell’s palsy and obesity, alcohol consumption and smoking: A nested case-control study using a national health screening cohort. Sci. Rep. 2020, 10, 4248. [Google Scholar] [CrossRef]
- Alvarez-Nemegyei, J.; Medina-Escobedo, M.; Villanueva-Jorge, S.; Vazquez-Mellado, J. Prevalence and risk factors for urolithiasis in primary gout: Is a reappraisal needed? J. Rheumatol. 2005, 32, 2189–2191. [Google Scholar] [PubMed]
- Tee, M.; Lustre Ii, C.; Abrilla, A.; Afos, I.E.; Canal, J.P. Prevalence of Urolithiasis by Ultrasonography Among Patients with Gout: A Cross-Sectional Study from the UP-Philippine General Hospital. Res. Rep. Urol. 2020, 12, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Liebman, S.E.; Taylor, J.G.; Bushinsky, D.A. Uric acid nephrolithiasis. Curr. Rheumatol. Rep. 2007, 9, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Gutman, A.B. Uric acid nephrolithiasis in gout. Predisposing factors. Ann. Intern. Med. 1967, 67, 1133–1148. [Google Scholar] [CrossRef]
- Cicerello, E. Uric acid nephrolithiasis: An update. Urologia 2018, 85, 93–98. [Google Scholar] [CrossRef]
- Thottam, G.E.; Krasnokutsky, S.; Pillinger, M.H. Gout and Metabolic Syndrome: A Tangled Web. Curr. Rheumatol. Rep. 2017, 19, 60. [Google Scholar] [CrossRef]
- Rendina, D.; De Filippo, G.; D'Elia, L.; Strazzullo, P. Metabolic syndrome and nephrolithiasis: A systematic review and meta-analysis of the scientific evidence. J. Nephrol. 2014, 27, 371–376. [Google Scholar] [CrossRef]
- So, A.K.; Martinon, F. Inflammation in gout: Mechanisms and therapeutic targets. Nat. Rev. Rheumatol. 2017, 13, 639–647. [Google Scholar] [CrossRef]
- Joshi, S.; Wang, W.; Peck, A.B.; Khan, S.R. Activation of the NLRP3 inflammasome in association with calcium oxalate crystal induced reactive oxygen species in kidneys. J. Urol. 2015, 193, 1684–1691. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Chang, Y.; Yun, K.E.; Jung, H.S.; Lee, S.J.; Shin, H.; Ryu, S. Development of Nephrolithiasis in Asymptomatic Hyperuricemia: A Cohort Study. Am. J. Kidney Dis. 2017, 70, 173–181. [Google Scholar] [CrossRef]
- Puig, J.G.; Michan, A.D.; Jimenez, M.L.; Perez de Ayala, C.; Mateos, F.A.; Capitan, C.F.; de Miguel, E.; Gijon, J.B. Female gout. Clinical spectrum and uric acid metabolism. Arch. Intern. Med. 1991, 151, 726–732. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total Participants | ||
|---|---|---|---|
| Gout (n = 17,043) | Comparison (n = 68,172) | Standardized Difference | |
| Age (years old, n, %) | 0.00 | ||
| 40–44 | 564 (3.3) | 2256 (3.3) | |
| 45–49 | 1951 (11.5) | 7804 (11.5) | |
| 50–54 | 3212 (18.9) | 12,848 (18.9) | |
| 55–59 | 3111 (18.3) | 12,444 (18.3) | |
| 60–64 | 2617 (15.4) | 10,468 (15.4) | |
| 65–69 | 2343 (13.8) | 9372 (13.8) | |
| 70–74 | 1753 (10.3) | 7012 (10.3) | |
| 75–79 | 1033 (6.1) | 4132 (6.1) | |
| 80–84 | 376 (2.2) | 1504 (2.2) | |
| ≥85 | 83 (0.5) | 332 (0.5) | |
| Sex (n, %) | 0.00 | ||
| Male | 13,567 (79.6) | 54,268 (79.6) | |
| Female | 3476 (20.4) | 13,904 (20.4) | |
| Income (n, %) | 0.00 | ||
| 1 (lowest) | 2398 (14.1) | 9592 (14.1) | |
| 2 | 2099 (12.3) | 8396 (12.3) | |
| 3 | 2593 (15.2) | 10,372 (15.2) | |
| 4 | 3602 (21.1) | 14,408 (21.1) | |
| 5 (highest) | 6351 (37.3) | 25,404 (37.3) | |
| Region of residence (n, %) | 0.00 | ||
| Urban | 7246 (42.5) | 28,984 (42.5) | |
| Rural | 9797 (57.5) | 39,188 (57.5) | |
| Total cholesterol level (mg/dL, mean, SD) | 200.2 (40.3) | 196.7 (37.5) | 0.09 |
| SBP (mmHg, mean, SD) | 130.0 (17.3) | 127.5 (16.6) | 0.14 |
| DBP (mmHg, mean, SD) | 80.8 (11.3) | 79.3 (10.7) | 0.14 |
| Fasting blood glucose level (mg/dL, mean, SD) | 101.5 (28.7) | 101.9 (30.6) | 0.01 |
| Obesity † (n, %) | 0.27 | ||
| Underweight | 236 (1.4) | 1718 (2.5) | |
| Normal | 4352 (25.5) | 23,836 (35.0) | |
| Overweight | 4699 (27.6) | 19,319 (28.3) | |
| Obese I | 7066 (41.5) | 21,670 (31.8) | |
| Obese II | 690 (4.1) | 1629 (2.4) | |
| Smoking status (n, %) | 0.07 | ||
| Nonsmoker | 9804 (57.5) | 38,271 (56.1) | |
| Past smoker | 3263 (19.2) | 12,027 (17.6) | |
| Current smoker | 3976 (23.3) | 17,874 (26.2) | |
| Alcohol consumption (n, %) | 0.10 | ||
| <1 time a week | 8920 (52.3) | 39,207 (57.5) | |
| ≥1 time a week | 8123 (47.7) | 28,965 (42.5) | |
| CCI score (score, n, %) | 0.05 | ||
| 0 | 10,603 (62.2) | 46,356 (68.0) | |
| 1 | 2633 (15.4) | 9348 (13.7) | |
| ≥2 | 3807 (22.3) | 12,468 (18.3) | |
| Nephrolithiasis (n, %) | 569 (3.3) | 1768 (2.6) | 0.04 |
| Characteristics | No. of Nephrolithiasis/No. of Participants | Follow-Up Duration, Person-Years | Incidence Rate, Per 1000 Person-Years | Hazard Ratios for Nephrolithiasis | |||
|---|---|---|---|---|---|---|---|
| Crude † | p-Value | Adjusted †,‡ | p-Value | ||||
| Total participants (n = 85,215) | |||||||
| Gout | 569/17,043 (3.3) | 99,082 | 5.7 | 1.29 (1.18–1.42) | <0.001 * | 1.23 (1.12–1.36) | <0.001 * |
| Comparison | 1768/68,172 (2.6) | 398,713 | 4.4 | 1 | 1 | ||
| Age < 60 years old (n = 44,190) | |||||||
| Gout | 387/8838 (4.4) | 59,125 | 6.5 | 1.33 (1.19–1.49) | <0.001 * | 1.26 (1.13–1.42) | <0.001 * |
| Comparison | 1174/35,352 (3.3) | 239,037 | 4.9 | 1 | 1 | ||
| Age ≥ 60 years old (n = 41,025) | |||||||
| Gout | 182/8205 (2.2) | 39,957 | 4.6 | 1.22 (1.03–1.44) | 0.019 * | 1.17 (0.99–1.38) | 0.075 |
| Comparison | 594/32,820 (1.8) | 159,676 | 3.7 | 1 | 1 | ||
| Males (n = 67,835) | |||||||
| Gout | 509/13,567 (3.8) | 79,748 | 6.4 | 1.35 (1.22–1.49) | <0.001 * | 1.27 (1.15–1.41) | <0.001 * |
| Comparison | 1517/54,268 (2.8) | 320,749 | 4.7 | 1 | 1 | ||
| Females (n = 17,380) | |||||||
| Gout | 60/3476 (1.7) | 19,334 | 3.1 | 0.96 (0.72–1.27) | 0.769 | 0.96 (0.72–1.27) | 0.752 |
| Comparison | 251/13,904 (1.8) | 77,964 | 3.2 | 1 | 1 | ||
| Low income (n = 35,450) | |||||||
| Gout | 221/7090 (3.1) | 39,824 | 5.5 | 1.37 (1.18–1.60) | <0.001 * | 1.32 (1.13–1.55) | <0.001 * |
| Comparison | 648/28,360 (2.3) | 160,604 | 4.0 | 1 | 1 | ||
| High income (n = 49,765) | |||||||
| Gout | 348/9953 (3.5) | 59,258 | 5.9 | 1.25 (1.11–1.41) | <0.001 * | 1.18 (1.04–1.33) | 0.009 * |
| Comparison | 1120/39,812 (2.8) | 238,109 | 4.7 | 1 | 1 | ||
| Urban (n = 36,230) | |||||||
| Gout | 235/7246 (3.2) | 42,795 | 5.5 | 1.25 (1.08–1.45) | 0.003 * | 1.21 (1.04–1.40) | 0.013 * |
| Comparison | 752/28,984 (2.6) | 172,193 | 4.4 | 1 | 1 | ||
| Rural (n = 48,985) | |||||||
| Gout | 334/9797 (3.4) | 56,287 | 5.9 | 1.32 (1.17–1.50) | <0.001 * | 1.25 (1.10–1.42) | 0.001 * |
| Comparison | 1016/39,188 (2.6) | 226,520 | 4.5 | 1 | 1 | ||
| Characteristics | No. of Nephrolithiasis/No. of Participants | Follow-Up Duration, Person-Years | Incidence Rate, Per 1000 Person-Years | Hazard Ratios for Nephrolithiasis | |||
|---|---|---|---|---|---|---|---|
| Crude | p-Value | Adjusted † | p-Value | ||||
| Underweight (n = 1954) | |||||||
| Gout | 1/236 (0.4) | 1198 | 0.8 | 0.45 (0.06–3.37) | 0.434 | 0.44 (0.06–3.40) | 0.429 |
| Comparison | 16/1718 (0.9) | 8821 | 1.8 | 1 | 1 | ||
| Normal weight (n = 28,188) | |||||||
| Gout | 110/4352 (2.5) | 24,466 | 4.5 | 1.24 (1.01–1.52) | 0.043 * | 1.27 (1.03–1.56) | 0.026 * |
| Comparison | 499/23,836 (2.1) | 138,486 | 3.6 | 1 | 1 | ||
| Overweight (n = 24,018) | |||||||
| Gout | 121/4699 (2.6) | 27,436 | 4.4 | 0.95 (0.78–1.15) | 0.592 | 0.95 (0.78–1.15) | 0.585 |
| Comparison | 530/19,319 (2.7) | 114,083 | 4.6 | 1 | 1 | ||
| Obese (n = 31,055) | |||||||
| Gout | 337/7756 (4.4) | 45,982 | 7.3 | 1.39 (1.22–1.59) | <0.001 * | 1.38 (1.21–1.58) | <0.001 * |
| Comparison | 723/23,299 (3.1) | 137,323 | 5.3 | 1 | 1 | ||
| Nonsmoker (n = 48,075) | |||||||
| Gout | 324/9804 (3.3) | 58,807 | 5.5 | 1.24 (1.09–1.40) | 0.001 * | 1.18 (1.04–1.34) | 0.009 * |
| Comparison | 1022/38,271 (2.7) | 230,020 | 4.4 | 1 | 1 | ||
| Past or current smoker (n = 37,140) | |||||||
| Gout | 245/7239 (3.4) | 40,275 | 6.1 | 1.37 (1.19–1.58) | <0.001 * | 1.30 (1.13–1.51) | <0.001 * |
| Comparison | 746/29,901 (2.5) | 168,693 | 4.4 | 1 | 1 | ||
| Alcohol consumption < 1 time a week (n = 48,127) | |||||||
| Gout | 320/8920 (3.6) | 55,291 | 5.8 | 1.26 (1.11–1.43) | <0.001 * | 1.22 (1.07–1.38) | 0.002 * |
| Comparison | 1130/39,207 (2.9) | 247,079 | 4.6 | 1 | 1 | ||
| Alcohol consumption ≥ 1 time a week (n = 37,088) | |||||||
| Gout | 249/8123 (3.1) | 43,791 | 5.7 | 1.36 (1.17–1.57) | <0.001 * | 1.25 (1.08–1.45) | 0.003 * |
| Comparison | 638/28,965 (2.2) | 151,634 | 4.2 | 1 | 1 | ||
| Total cholesterol < 200 mg/dL (n = 46,981) | |||||||
| Gout | 273/8861 (3.1) | 49,401 | 5.5 | 1.26 (1.10–1.44) | 0.001 * | 1.22 (1.06–1.40) | 0.005 * |
| Comparison | 949/38,120 (2.5) | 217,932 | 4.4 | 1 | 1 | ||
| Total cholesterol ≥ 200 to < 240 mg/dL (n = 27,439) | |||||||
| Gout | 206/5631 (3.7) | 33,659 | 6.1 | 1.39 (1.19–1.63) | <0.001 * | 1.31 (1.11–1.54) | 0.001 * |
| Comparison | 574/21,808 (2.6) | 130,780 | 4.4 | 1 | 1 | ||
| Total cholesterol ≥ 240 mg/dL (n = 10,795) | |||||||
| Gout | 90/2551 (3.5) | 16,022 | 5.6 | 1.15 (0.90–1.47) | 0.254 | 1.11 (0.87–1.42) | 0.408 |
| Comparison | 245/8244 (3.0) | 50,001 | 4.9 | 1 | 1 | ||
| SBP < 140 mmHg and DBP < 90 mmHg (n = 60,148) | |||||||
| Gout | 345/11,228 (3.1) | 61,471 | 5.6 | 1.24 (1.10–1.40) | <0.001 * | 1.19 (1.06–1.34) | 0.005 * |
| Comparison | 1237/48,920 (2.5) | 275,056 | 4.5 | 1 | 1 | ||
| SBP ≥ 140 mmHg or DBP ≥ 90 mmHg (n = 25,067) | |||||||
| Gout | 224/5815 (3.9) | 37,611 | 6.0 | 1.39 (1.19–1.62) | <0.001 * | 1.30 (1.11–1.53) | 0.001 * |
| Comparison | 531/19,252 (2.8) | 123,657 | 4.3 | 1 | 1 | ||
| Fasting blood glucose < 100 mg/dL (n = 51,333) | |||||||
| Gout | 341/10,028 (3.4) | 60,803 | 5.6 | 1.37 (1.21–1.54) | <0.001 * | 1.28 (1.13–1.45) | <0.001 * |
| Comparison | 1037/41,305 (2.5) | 252,771 | 4.1 | 1 | 1 | ||
| Fasting blood glucose ≥ 100 mg/dL (n = 33,882) | |||||||
| Gout | 228/7015 (3.3) | 38,279 | 6.0 | 1.19 (1.02–1.38) | 0.024 * | 1.15 (0.99–1.34) | 0.062 |
| Comparison | 731/26,867 (2.7) | 145,942 | 5.0 | 1 | 1 | ||
| 0 CCI score (n = 56,959) | |||||||
| Gout | 360/10,603 (3.4) | 61,758 | 5.8 | 1.37 (1.22–1.54) | <0.001 * | 1.31 (1.16–1.48) | <0.001 * |
| Comparison | 1169/46,356 (2.5) | 275,735 | 4.2 | 1 | 1 | ||
| 1 CCI score (n = 11,981) | |||||||
| Gout | 96/2633 (3.6) | 15,412 | 6.2 | 1.25 (0.99–1.58) | 0.057 | 1.17 (0.92–1.48) | 0.200 |
| Comparison | 271/9348 (2.9) | 54,603 | 5.0 | 1 | 1 | ||
| ≥ 2 CCI score (n = 16,275) | |||||||
| Gout | 113/3807 (3.0) | 21,912 | 5.2 | 1.08 (0.87–1.34) | 0.477 | 1.03 (0.83–1.27) | 0.821 |
| Comparison | 328 12,468 (2.6) | 68,375 | 4.8 | 1 | 1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.Y.; Yoo, D.M.; Kim, J.H.; Kwon, M.J.; Kim, J.-H.; Lee, J.W.; Bang, W.J.; Choi, H.G. The Occurrence of Nephrolithiasis in Gout Patients: A Longitudinal Follow-Up Study Using a National Health Screening Cohort. Life 2022, 12, 653. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050653
Kim SY, Yoo DM, Kim JH, Kwon MJ, Kim J-H, Lee JW, Bang WJ, Choi HG. The Occurrence of Nephrolithiasis in Gout Patients: A Longitudinal Follow-Up Study Using a National Health Screening Cohort. Life. 2022; 12(5):653. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050653
Chicago/Turabian StyleKim, So Young, Dae Myoung Yoo, Ji Hee Kim, Mi Jung Kwon, Joo-Hee Kim, Jung Woo Lee, Woo Jin Bang, and Hyo Geun Choi. 2022. "The Occurrence of Nephrolithiasis in Gout Patients: A Longitudinal Follow-Up Study Using a National Health Screening Cohort" Life 12, no. 5: 653. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050653