
Altitude Effect on Cutaneous Melanoma Epidemiology in the Veneto Region (Northern Italy): A Pilot Study

 , , , , , , , ,
, , , , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Diagnosis
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Patients
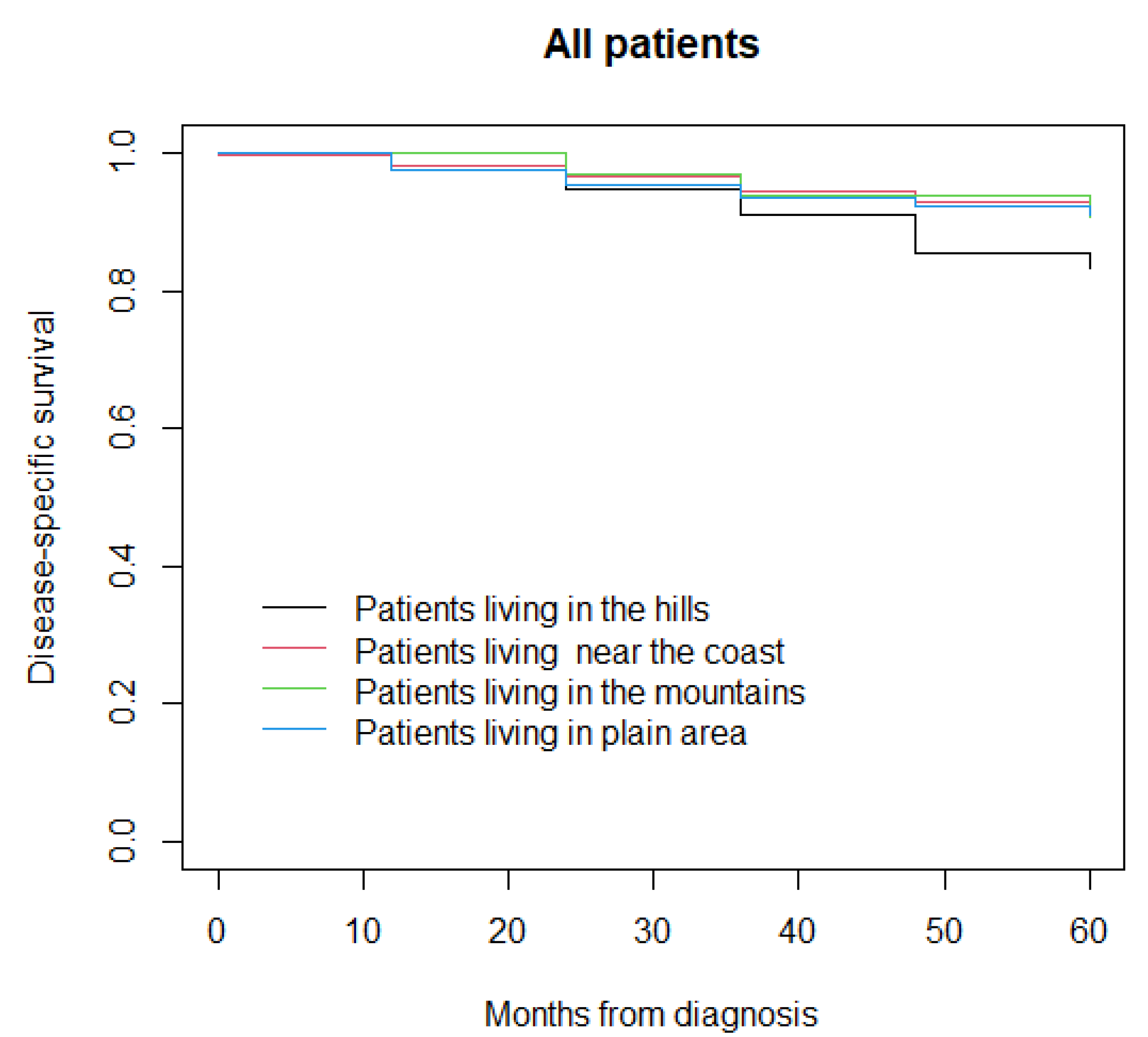
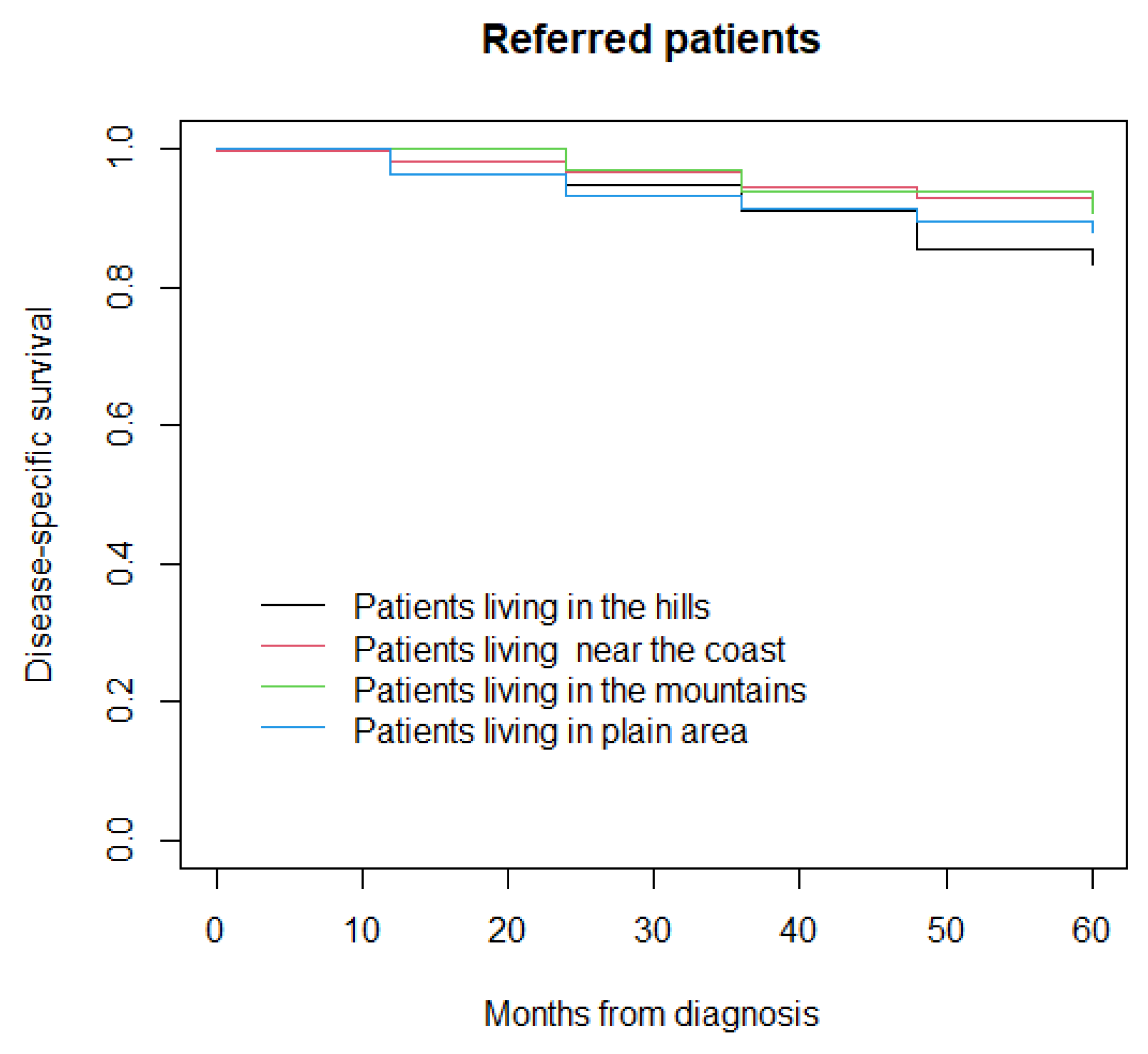
3.2. Disease-Specific Survival
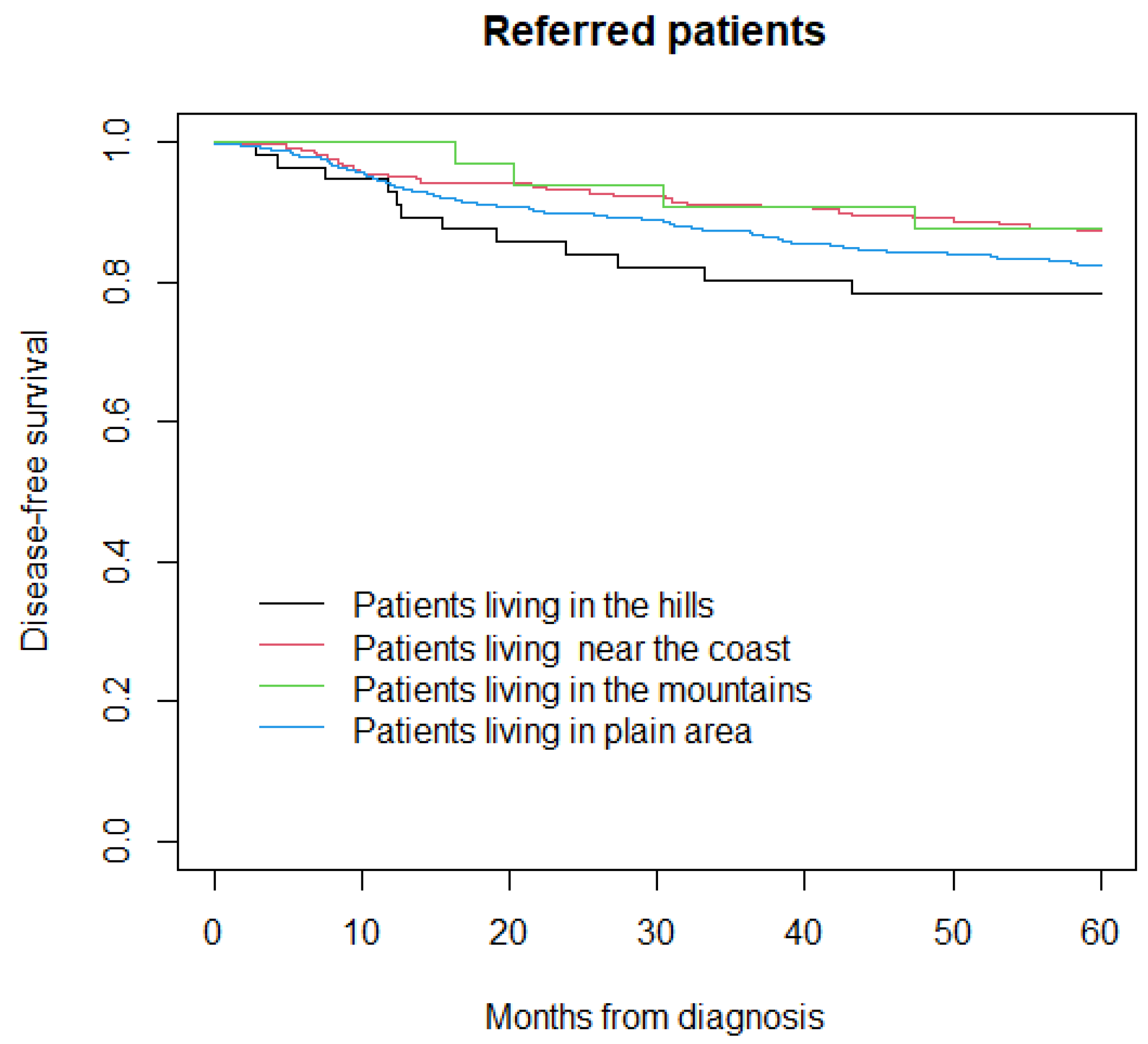
3.3. Disease-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Bishop, K.; Kosary, C.; Mariotto, A.; Cancer Statistics Review, 1975–2014—SEER Statistics. SEER Cancer Statistics Review—Bethesda (MD): National Cancer Institute. 2011. Available online: https://seer.cancer.gov/archive/csr/1975_2014/ (accessed on 2 May 2022).
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Registro Tumori Veneto. Available online: https://www.registrotumoriveneto.it/it/pubblicazioni/monografie/per-sede (accessed on 11 April 2022).
- Crocetti, E.; Buzzoni, C.; Chiarugi, A.; Nardini, P.; Pimpinelli, N. Relationship between Latitude and Melanoma in Italy. ISRN Oncol. 2012, 2012, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Registro Tumori Veneto. Available online: https://gecoopendata.registrotumoriveneto.it/incidenza.php?sede=melanoma_cutaneo/ (accessed on 11 April 2022).
- Berwick, M.; Buller, D.B.; Cust, A.; Gallagher, R.; Lee, T.K.; Meyskens, F.; Pandey, S.; Thomas, N.E.; Veierød, M.B.; Ward, S. Melanoma Epidemiology and Prevention. Cancer Treat. Res. 2015, 167, 17–49. [Google Scholar] [CrossRef] [Green Version]
- Narayanan, D.L.; Saladi, R.N.; Fox, J.L. Review: Ultraviolet radiation and skin cancer. Int. J. Dermatol. 2010, 49, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Aceituno-Madera, P.; Buendía-Eisman, A.; Olmo, F.; Jimenez-Moleon, J.J.; Serrano-Ortega, S. Melanoma, altitud y radiación UVB [Melanoma, altitude, and UV-B radiation]. Actas Dermo-Sifiliogr. 2011, 102, 199–205. [Google Scholar] [CrossRef]
- Keim, U.; Gandini, S.; Amaral, T.; Katalinic, A.; Holleczek, B.; Flatz, L.; Leiter, U.; Whiteman, D.; Garbe, C. Cutaneous melanoma attributable to UVR exposure in Denmark and Germany. Eur. J. Cancer 2021, 159, 98–104. [Google Scholar] [CrossRef]
- Khan, A.Q.; Travers, J.B.; Kemp, M.G. Roles of UVA radiation and DNA damage responses in melanoma pathogenesis. Environ. Mol. Mutagen. 2018, 59, 438–460. [Google Scholar] [CrossRef]
- Chalada, M.; Ramlogan-Steel, C.; Dhungel, B.; Layton, C.; Steel, J. The Impact of Ultraviolet Radiation on the Aetiology and Development of Uveal Melanoma. Cancers 2021, 13, 1700. [Google Scholar] [CrossRef]
- Regione del Veneto. Available online: https://idt2.regione.veneto.it/ (accessed on 11 April 2022).
- Elder, D.E.; Massi, D.; Scolyer, R.A.; Willemze, R. World Health Organization Classification of Skin Tumours; International Agency for Research on Cancer: Lyon, France, 2018. [Google Scholar]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2017. [Google Scholar]
- ISTAT. Available online: https://www.istat.it/it/informazioni-territoriali-e-cartografiche (accessed on 11 April 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Moan, J.; Porojnicu, A.C.; Dahlback, A. Ultraviolet Radiation and Malignant Melanoma. Adv. Exp. Med. Biol. 2008, 624, 104–116. [Google Scholar] [CrossRef]
- Buja, A.; Rugge, M.; de Luca, G.; Bovo, E.; Zorzi, M.; de Toni, C.; Cozzolino, C.; Vecchiato, A.; Del Fiore, P.; Spina, R.; et al. Cutaneous Melanoma in Alpine Population: Incidence Trends and Clinicopathological Profile. Curr. Oncol. 2022, 29, 30175. [Google Scholar] [CrossRef]
- Muntyanu, A.; Savin, E.; Ghazawi, F.M.; Alakel, A.; Zubarev, A.; Litvinov, I.V. Geographic Variations in Cutaneous Melanoma Distribution in the Russian Federation. Dermatology 2020, 236, 500–507. [Google Scholar] [CrossRef]
- Shipman, A.R.; Clark, A.B.; Levell, N.J. Sunnier European countries have lower melanoma mortality. Clin. Exp. Dermatol. 2011, 36, 544–547. [Google Scholar] [CrossRef]
- Cicarma, E.; Juzeniene, A.; Porojnicu, A.C.; Bruland, S.; Moan, J. Latitude gradient for melanoma incidence by anatomic site and gender in Norway 1966–2007. J. Photochem. Photobiol. B Biol. 2010, 101, 174–178. [Google Scholar] [CrossRef] [Green Version]
- Eklund, G.; Malec, E. Sunlight and Incidence of Cutaneous Malignant Melanoma: Effect of Latitude and Domicile in Sweden. Scand. J. Plast. Reconstr. Surg. 1978, 12, 231–241. [Google Scholar] [CrossRef]
- Eide, M.J.; Weinstock, M.A. Association of UV Index, Latitude, and Melanoma Incidence in Nonwhite Populations—US Surveillance, Epidemiology, and End Results (SEER) Program, 1992 to 2001. Arch. Dermatol. 2005, 141, 477–481. [Google Scholar] [CrossRef]
- Bulliard, J.-L. Site-specific risk of cutaneous malignant melanoma and pattern of Sun exposure in New Zealand. Int. J. Cancer 2000, 85, 627–632. [Google Scholar] [CrossRef]
- Grant, W.B. An ecologic study of cancer mortality rates in Spain with respect to indices of solar UVB irradiance and smoking. Int. J. Cancer 2006, 120, 1123–1128. [Google Scholar] [CrossRef]
- Lindegård, B. Mortality and fatality of cutaneous malignant melanoma in Sweden, 1982–1986. Biomed. Pharmacother. 1990, 44, 495–501. [Google Scholar] [CrossRef]
- Lee, J.A.H. Declining effect of latitude on melanoma mortality rates in the United States. A preliminary study. Am. J. Epidemiol. 1997, 146, 413–417. [Google Scholar] [CrossRef] [Green Version]
- Arpa Veneto. Available online: http://geomap.arpa.veneto.it/maps/51#license-more-above (accessed on 2 May 2022).
- Arpa Veneto. Available online: https://www.arpa.veneto.it/temi-ambientali/agenti-fisici/radiazioni-uv/dati-in-diretta (accessed on 2 May 2022).
- Wyatt, C.; Lucas, R.; Hurst, C.; Kimlin, M. Vitamin D Deficiency at Melanoma Diagnosis Is Associated with Higher Breslow Thickness. PLoS ONE 2015, 10, e0126394. [Google Scholar] [CrossRef] [Green Version]
- Moreno-Arrones, O.M.; Zegeer, J.; Gerbo, M.; Manrique-Silva, E.; Requena, C.; Traves, V.; Nagore, E. Decreased vitamin D serum levels at melanoma diagnosis are associated with tumor ulceration and high tumor mitotic rate. Melanoma Res. 2019, 29, 664–667. [Google Scholar] [CrossRef]
- De Smedt, J.; van Kelst, S.; Janssen, L.; Marasigan, V.; Boecxstaens, V.; Stas, M.; Vanderschueren, D.; Guler, I.; Bogaerts, K.; Vandenberghe, K.; et al. Determinants of 25-hydroxyvitamin D Status in a Cutaneous Melanoma Population. Acta Derm. Venereol. 2022, 102, adv00692. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, M.; Vigezzi, A.; Ietto, G.; Franchi, C.; Iori, V.; Masci, F.; Scorza, A.; Macchi, S.; Iovino, D.; Parise, C.; et al. Role of vitamin D serum levels in prevention of primary and recurrent melanoma. Sci. Rep. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- De Martino, E.; Brunetti, D.; Canzonieri, V.; Conforti, C.; Eisendle, K.; Mazzoleni, G.; Nobile, C.; Rao, F.; Zschocke, J.; Jukic, E.; et al. The Association of Residential Altitude on the Molecular Profile and Survival of Melanoma: Results of an Interreg Study. Cancers 2020, 12, 2796. [Google Scholar] [CrossRef] [PubMed]
- Gencia, I.; Baderca, F.; Avram, S.; Gogulescu, A.; Marcu, A.; Seclaman, E.; Marian, C.; Solovan, C. A preliminary study of microRNA expression in different types of primary melanoma. Bosn. J. Basic Med. Sci. 2019, 20, 197–208. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hills (n = 56) | Coast (n = 262) | Mountains (n = 34) | Plain Area (n = 2400) | p-Value | |
|---|---|---|---|---|---|
| Age, years: | |||||
| Median (IQR) | 46 (39–63) | 53 (39–63) | 46 (38–64) | 51 (39–64) | 0.61 |
| Males: n (%) | 29 (51.8%) | 127 (48.5%) | 21 (61.8%) | 1133 (47.2%) | 0.34 |
| Primary site: n (%): | <0.0001 | ||||
| Hand and foot | 5 (8.9%) | 13 (5.0%) | 3 (8.8%) | 134 (5.6%) | |
| Head/neck | 17 (30.4%) | 23 (8.8%) | 4 (11.8%) | 140 (5.8%) | |
| Upper limb | 6 (10.7%) | 35 (13.4%) | 4 (11.8%) | 346 (14.4%) | |
| Trunk | 17 (30.4%) | 120 (45.8%) | 14 (41.2%) | 1161 (48.4%) | |
| Lower limb | 11 (19.6%) | 71 (27.0%) | 9 (26.4%) | 619 (25.8%) | |
| Breslow, mm: | <0.0001 | ||||
| Median (IQR) | 2.0 (1.1–4.4) | 0.7 (0.5–1.8) | 1.6 (0.5–2.3) | 0.7 (0.4–1.5) | |
| Data not available | 3 (5.3%) | 8 (3.0%) | 1 (2.9%) | 58 (2.4%) | |
| Ulceration, n (%): | 0.03 | ||||
| Absent | 33 (59.0%) | 206 (78.6%) | 27 (79.4%) | 1859 (77.4%) | |
| Present | 19 (33.9%) | 46 (17.6%) | 7 (20.6%) | 479 (20.0%) | |
| Data not available | 4 (7.1%) | 10 (3.8%) | - | 62 (2.6%) | |
| Mitoses per mm2: | <0.0001 | ||||
| Median (IQR) | 4 (2–8) | 1 (0–3) | 2 (0–3) | 1 (0–4) | |
| Data not available | 1 (1.7%) | 1 (0.4%) | - | 13 (0.5%) | |
| pTNM, n (%): | <0.0001 | ||||
| I | 23 (41.1%) | 175 (66.8%) | 18 (52.9%) | 1696 (70.7%) | |
| II | 21 (37.5%) | 48 (18.3%) | 8 (23.6%) | 334 (13.9%) | |
| III | 12 (21.4%) | 39 (14.9%) | 7 (20.6%) | 369 (15.4%) | |
| IV | 0 (0.0%) | 0 (0.0%) | 1 (2.9%) | 1 (0.0%) | |
| Subtype, n (%): | 0.09 | ||||
| ALM | 2 (3.6%) | 3 (1.1%) | 0 (0.0%) | 75 (3.1%) | |
| LMM | 2 (3.6%) | 5 (1.9%) | 0 (0.0%) | 32 (1.3%) | |
| NM | 13 (23.2%) | 44 (16.8%) | 6 (17.6%) | 355 (14.8%) | |
| SSM | 32 (57.1%) | 192 (73.3%) | 26 (76.5%) | 1813 (75.5%) | |
| Other | 5 (8.9%) | 11 (4.2%) | 2 (5.9%) | 78 (3.3%) | |
| Data not available | 2 (3.6%) | 7 (2.7%) | - | 47 (2.0%) |
| Hills (n = 56) | Coast (n = 262) | Mountains (n = 34) | Plain Area (n = 766) | p-Value | |
|---|---|---|---|---|---|
| Age, years: | |||||
| Median (IQR) | 46 (39–63) | 53 (39–63) | 46 (38–64) | 49 (38–62) | 0.43 |
| Males, n (%) | 29 (51.8%) | 127 (48.5%) | 21 (61.8%) | 357 (46.6%) | 0.32 |
| Primary site, n (%): | 0.005 | ||||
| Hand and foot | 5 (8.9%) | 13 (5.0%) | 3 (8.8%) | 58 (7.6%) | |
| Head/neck | 17 (30.4%) | 23 (8.8%) | 4 (11.8%) | 76 (9.9%) | |
| Upper limb | 6 (10.7%) | 35 (13.4%) | 4 (11.8%) | 187 (24.4%) | |
| Trunk | 17 (30.4%) | 120 (45.8%) | 14 (41.2%) | 336 (43.9%) | |
| Lower limb | 11 (19.6%) | 71 (27.0%) | 9 (26.4%) | 109 (14.2%) | |
| Breslow, mm: | <0.0001 | ||||
| Median (IQR) | 2.0 (1.1–4.4) | 0.7 (0.5–1.8) | 1.6 (0.5–2.3) | 1.0 (0.5–2.5) | |
| Data not available | 3 (5.3%) | 8 (3.0%) | 1 (2.9%) | 42 (5.4%) | |
| Ulceration, n (%): | 0.009 | ||||
| Absent | 33 (59.0%) | 206 (78.6%) | 27 (79.4%) | 539 (70.4%) | |
| Present | 19 (33.9%) | 46 (17.6%) | 7 (20.6%) | 199 (26.0%) | |
| Data not available | 4 (7.1%) | 10 (3.8%) | - | 28 (3.6%) | |
| Mitoses per mm2: | <0.0001 | ||||
| Median (IQR) | 4 (2–8) | 1 (0–3) | 2 (0–3) | 2 (0–4) | |
| Data not available | 1 (1.7%) | 1 (0.4%) | - | 9 (1.1%) | |
| pTNM, n (%): | <0.0001 | ||||
| I | 23 (41.1%) | 175 (66.8%) | 18 (52.9%) | 435 (56.8%) | |
| II | 21 (37.5%) | 48 (18.3%) | 8 (23.6%) | 153 (20.0%) | |
| III | 12 (21.4%) | 39 (14.9%) | 7 (20.6%) | 177 (23.1%) | |
| IV | 0 (0.0%) | 0 (0.0%) | 1 (2.9%) | 1 (0.1%) | |
| Subtype, n (%): | 0.25 | ||||
| ALM | 2 (3.6%) | 3 (1.1%) | 0 (0.0%) | 26 (3.4%) | |
| LMM | 2 (3.6%) | 5 (1.9%) | 0 (0.0%) | 14 (1.7%) | |
| NM | 13 (23.2%) | 44 (16.8%) | 6 (17.6%) | 165 (21.5%) | |
| SSM | 32 (57.1%) | 192 (73.3%) | 26 (76.5%) | 495 (64.6%) | |
| Other | 5 (8.9%) | 11 (4.2%) | 2 (5.9%) | 32 (4.2%) | |
| Data not available | 2 (3.6%) | 7 (2.7%) | - | 35 (4.6%) |
| All Patients | Referred Patients | |||
|---|---|---|---|---|
| p-Value | ||||
| Hazard Ratio (95% Confidence Interval) | p-Value | Hazard Ratio (95% Confidence Interval) | p-Value | |
| Geographical area: | ||||
| Hills | 0.95 (0.52 to 1.72) | 0.86 | 1.23 (0.66 to 2.29) | 0.51 |
| Coast | 1.09 (0.73 to 1.62) | 0.68 | 1.09 (0.73 to 1.62) | 0.89 |
| Mountains | 0.65 (0.21 to 2.04) | 0.46 | 0.65 (0.21 to 2.04) | 0.54 |
| Plain area | Reference | Reference | ||
| Primary site: | ||||
| Head/neck | 1.46 (0.98 to 2.17) | 0.06 | 1.68 (0.38 to 1.19) | 0.18 |
| Trunk | Reference | Reference | ||
| Limbs | 0.95 (0.74 to 1.22) | 0.71 | 0.75 (0.52 to 1.07) | 0.11 |
| Breslow, mm | 1.07 (1.05 to 1.09) | <0.0001 | 1.13 (1.10 to 1.16) | <0.0001 |
| Ulceration: | 0.0006 | |||
| Absent | Reference | Reference | ||
| Present | 2.96 (2.25 to 3.89) | <0.0001 | 1.95 (1.33 to 2.85) | |
| Mitoses per mm2 | 1.08 (1.06 to 1.09) | <0.0001 | 1.06 (1.02 to 1.09) | 0.0006 |
| pTNM: | ||||
| I-II | Reference | Reference | ||
| III-IV | 2.68 (2.06 to 3.48) | <0.0001 | 2.39 (1.65 to 3.46) | <0.0001 |
| All Patients | Referred Patients | |||
|---|---|---|---|---|
| p-Value | ||||
| Hazard Ratio (95% Confidence Interval) | p-Value | Hazard Ratio (95% Confidence Interval) | p-Value | |
| Geographical area: | ||||
| Hills | 0.97 (0.56 to 1.68) | 0.91 | 0.98 (0.55 to 1.73) | 0.94 |
| Coast | 1.12 (0.78 to 1.60) | 0.54 | 0.95 (0.65 to 1.39) | 0.8 |
| Mountains | 0.68 (0.25 to 1.84) | 0.45 | 0.62 (0.23 to 1.68) | 0.35 |
| Plain area | Reference | Reference | ||
| Primary site: | ||||
| Head/neck | 2.03 (1.42 to 2.90) | <0.0001 | 1.56 (0.99 to 2.47) | 0.05 |
| Trunk | Reference | Reference | ||
| Limbs | 1.22 (0.97 to 1.53) | 0.09 | 1.23 (0.89 to 1.70) | 0.21 |
| Breslow, mm | 1.06 (1.04 to 1.08) | <0.0001 | 1.10 (1.07 to 1.13) | <0.0001 |
| Ulceration: | 0.004 | |||
| Absent | Reference | Reference | ||
| Present | 2.28 (1.78 to 2.91) | <0.0001 | 1.63 (1.17 to 2.26) | |
| Mitoses per mm2 | 1.07 (1.05 to 1.08) | <0.0001 | 1.06 (1.03 to 1.09) | <0.0001 |
| pTNM: | ||||
| I-II | Reference | Reference | ||
| III-IV | 3.50 (2.75 to 4.45) | <0.0001 | 3.20 (2.32 to 4.1) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Del Fiore, P.; Russo, I.; Dal Monico, A.; Tartaglia, J.; Ferrazzi, B.; Mazza, M.; Cavallin, F.; Tropea, S.; Buja, A.; Cappellesso, R.; et al. Altitude Effect on Cutaneous Melanoma Epidemiology in the Veneto Region (Northern Italy): A Pilot Study. Life 2022, 12, 745. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050745
Del Fiore P, Russo I, Dal Monico A, Tartaglia J, Ferrazzi B, Mazza M, Cavallin F, Tropea S, Buja A, Cappellesso R, et al. Altitude Effect on Cutaneous Melanoma Epidemiology in the Veneto Region (Northern Italy): A Pilot Study. Life. 2022; 12(5):745. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050745
Chicago/Turabian StyleDel Fiore, Paolo, Irene Russo, Alessandro Dal Monico, Jacopo Tartaglia, Beatrice Ferrazzi, Marcodomenico Mazza, Francesco Cavallin, Saveria Tropea, Alessandra Buja, Rocco Cappellesso, and et al. 2022. "Altitude Effect on Cutaneous Melanoma Epidemiology in the Veneto Region (Northern Italy): A Pilot Study" Life 12, no. 5: 745. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050745