
Circulating miRNA-195-5p and -451a in Patients with Acute Hemorrhagic Stroke in Emergency Department

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Participants
2.2. Interventions
2.3. miRNA Isolation and Real-Time Reverse Transcription (qRT-PCR)
2.4. Serum VEGF-A ELISA Assay
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Study Subjects
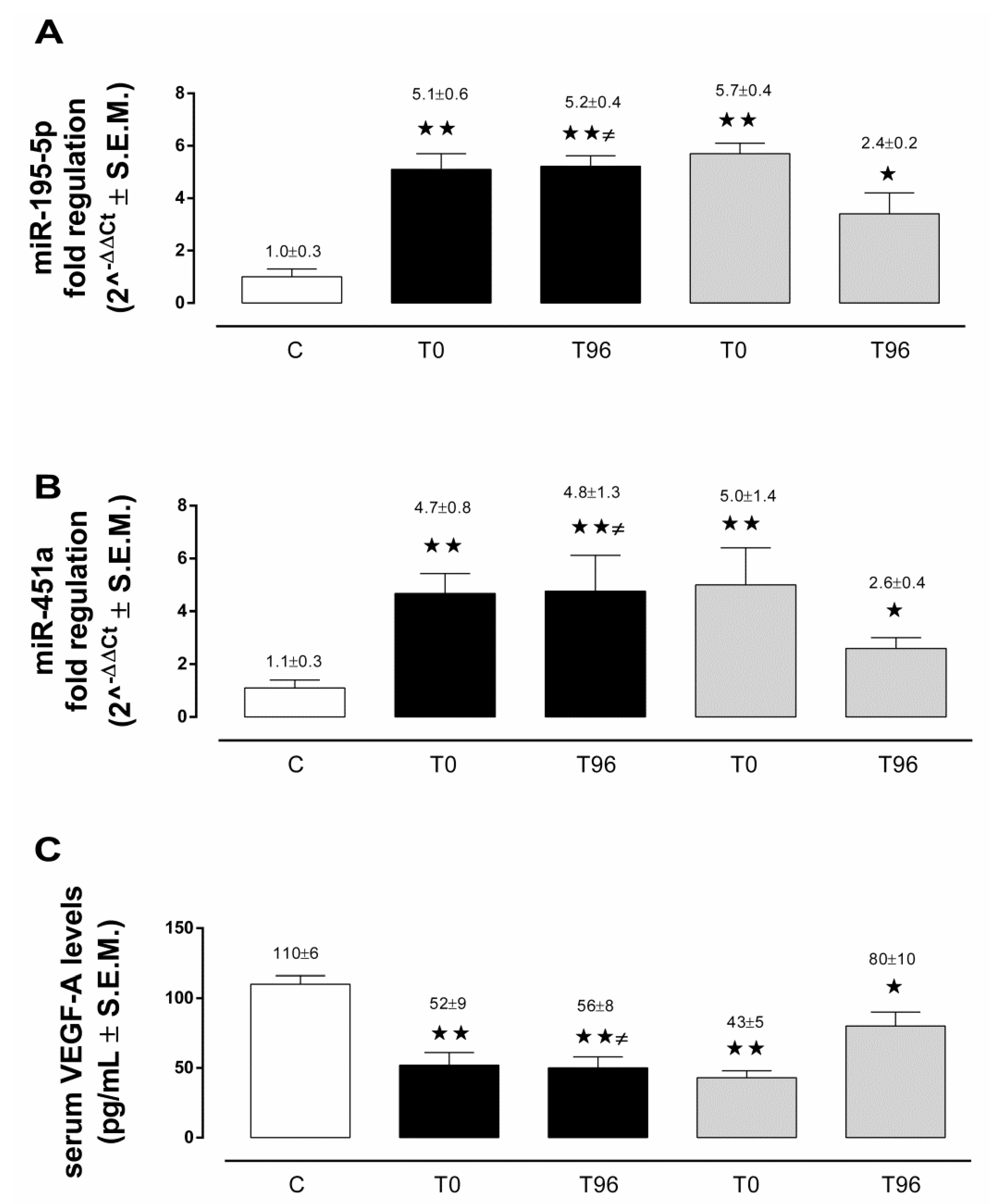
3.2. Circulating miRNA-195-5p in ICH and AIS Patients
3.3. Circulating miRNA-451a in ICH and AIS Patients
3.4. Serum VEGF-A in ICH and AIS Patients
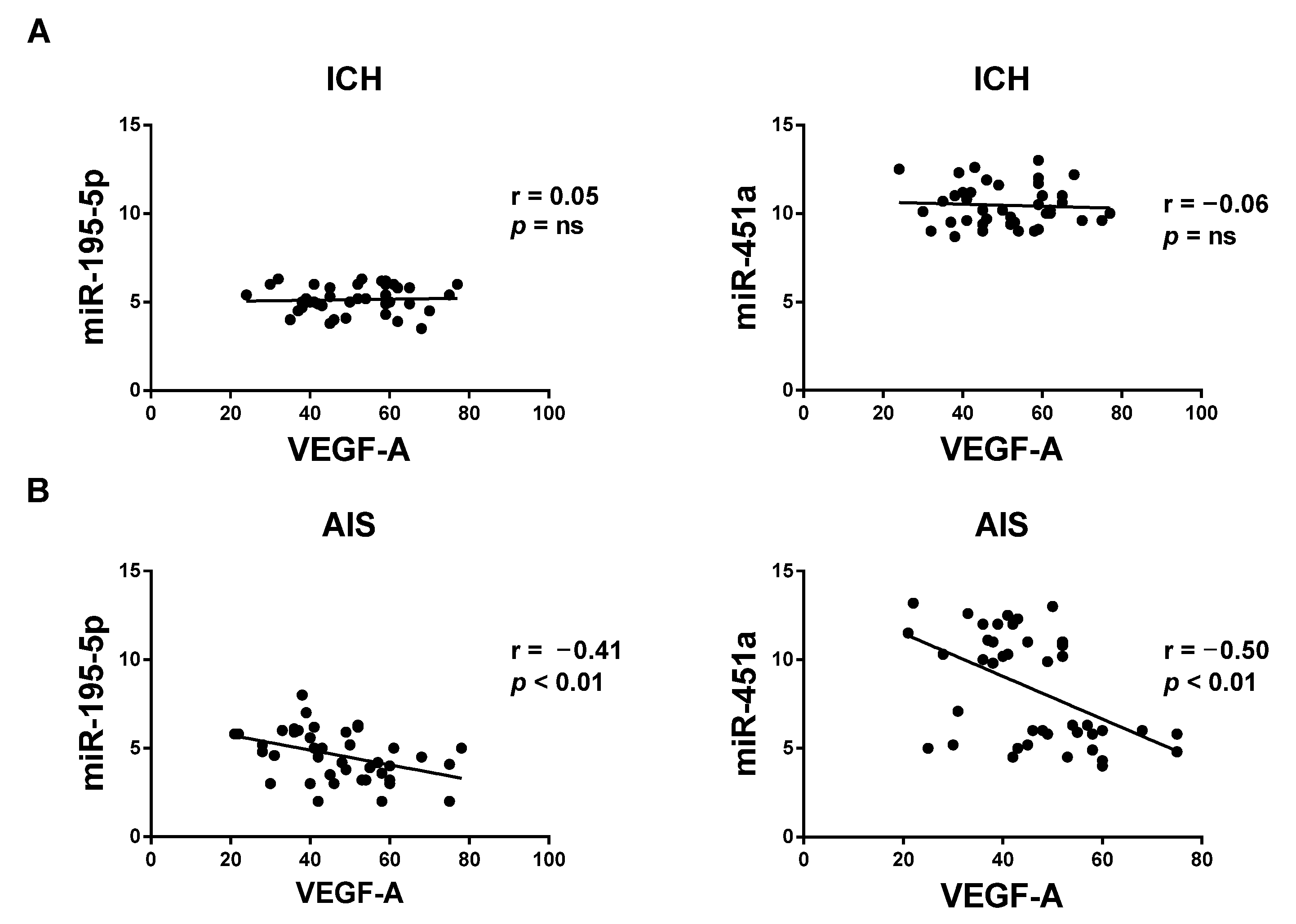
3.5. Correlation between Circulating miRNAs and VEGF-A Serum Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McGurgan, I.J.; Ziai, W.C.; Werring, D.J.; Al-Shahi Salman, R.; Parry-Jones, A.R. Acute Intracerebral Haemorrhage: Diagnosis and Management. Pract. Neurol. 2021, 21, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Hemphill, J.C.; Bonovich, D.C.; Besmertis, L.; Manley, G.T.; Johnston, S.C. The ICH Score: A Simple, Reliable Grading Scale for Intracerebral Hemorrhage. Stroke 2001, 32, 891–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Asch, C.J.; Luitse, M.J.; Rinkel, G.J.; van der Tweel, I.; Algra, A.; Klijn, C.J. Incidence, Case Fatality, and Functional Outcome of Intracerebral Haemorrhage over Time, According to Age, Sex, and Ethnic Origin: A Systematic Review and Meta-Analysis. Lancet Neurol. 2010, 9, 167–176. [Google Scholar] [CrossRef]
- Krishnamurthi, R.V.; Ikeda, T.; Feigin, V.L. Global, Regional and Country-Specific Burden of Ischaemic Stroke, Intracerebral Haemorrhage and Subarachnoid Haemorrhage: A Systematic Analysis of the Global Burden of Disease Study 2017. Neuroepidemiology 2020, 54, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Balami, J.S.; Buchan, A.M. Complications of Intracerebral Haemorrhage. Lancet Neurol. 2012, 11, 101–118. [Google Scholar] [CrossRef]
- Zeng, Y.; Cheng, H.; Cheng, L.; Huang, G.; Chen, Y.; Tang, W.; He, J. Comparison of Poststroke Depression between Acute Ischemic and Hemorrhagic Stroke Patients. Int. J. Geriatr. Psychiatry 2021, 36, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Morotti, A.; Goldstein, J.N. Diagnosis and Management of Acute Intracerebral Hemorrhage. Emerg. Med. Clin. N. Am. 2016, 34, 883–899. [Google Scholar] [CrossRef] [Green Version]
- Manners, J.; Steinberg, A.; Shutter, L. Early Management of Acute Cerebrovascular Accident. Curr. Opin. Crit. Care 2017, 23, 556–560. [Google Scholar] [CrossRef]
- Ehrenreich, H.; Kästner, A.; Weissenborn, K.; Streeter, J.; Sperling, S.; Wang, K.K.; Worthmann, H.; Hayes, R.L.; von Ahsen, N.; Kastrup, A.; et al. Circulating Damage Marker Profiles Support a Neuroprotective Effect of Erythropoietin in Ischemic Stroke Patients. Mol. Med. 2011, 17, 1306–1310. [Google Scholar] [CrossRef]
- Whiteley, W.; Jackson, C.; Lewis, S.; Lowe, G.; Rumley, A.; Sandercock, P.; Wardlaw, J.; Dennis, M.; Sudlow, C. Association of Circulating Inflammatory Markers With Recurrent Vascular Events After Stroke: A Prospective Cohort Study. Stroke 2011, 42, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Faura, J.; Bustamante, A.; Reverté, S.; García-Berrocoso, T.; Millán, M.; Castellanos, M.; Lara-Rodríguez, B.; Zaragoza, J.; Ventura, O.; Hernández-Pérez, M.; et al. Blood Biomarker Panels for the Early Prediction of Stroke-Associated Complications. JAHA 2021, 10, e018946. [Google Scholar] [CrossRef] [PubMed]
- Bustamante, A.; López-Cancio, E.; Pich, S.; Penalba, A.; Giralt, D.; García-Berrocoso, T.; Ferrer-Costa, C.; Gasull, T.; Hernández-Pérez, M.; Millan, M.; et al. Blood Biomarkers for the Early Diagnosis of Stroke: The Stroke-Chip Study. Stroke 2017, 48, 2419–2425. [Google Scholar] [CrossRef] [PubMed]
- Mojtabavi, H.; Shaka, Z.; Momtazmanesh, S.; Ajdari, A.; Rezaei, N. Circulating Brain-Derived Neurotrophic Factor as a Potential Biomarker in Stroke: A Systematic Review and Meta-Analysis. J. Transl. Med. 2022, 20, 126. [Google Scholar] [CrossRef] [PubMed]
- Åberg, N.D.; Wall, A.; Anger, O.; Jood, K.; Andreasson, U.; Blennow, K.; Zetterberg, H.; Isgaard, J.; Jern, C.; Svensson, J. Circulating Levels of Vascular Endothelial Growth Factor and Post-stroke Long-term Functional Outcome. Acta Neurol. Scand. 2020, 141, 405–414. [Google Scholar] [CrossRef]
- Toyoda, K.; Yoshimura, S.; Nakai, M.; Koga, M.; Sasahara, Y.; Sonoda, K.; Kamiyama, K.; Yazawa, Y.; Kawada, S.; Sasaki, M.; et al. Twenty-Year Change in Severity and Outcome of Ischemic and Hemorrhagic Strokes. JAMA Neurol. 2022, 79, 61. [Google Scholar] [CrossRef]
- Zhou, S.; Bao, J.; Wang, Y.; Pan, S. S100β as a Biomarker for Differential Diagnosis of Intracerebral Hemorrhage and Ischemic Stroke. Neurol. Res. 2016, 38, 327–332. [Google Scholar] [CrossRef]
- Luger, S.; Jæger, H.S.; Dixon, J.; Bohmann, F.O.; Schaefer, J.; Richieri, S.P.; Larsen, K.; Hov, M.R.; Bache, K.G.; Foerch, C.; et al. Diagnostic Accuracy of Glial Fibrillary Acidic Protein and Ubiquitin Carboxy-Terminal Hydrolase-L1 Serum Concentrations for Differentiating Acute Intracerebral Hemorrhage from Ischemic Stroke. Neurocrit. Care 2020, 33, 39–48. [Google Scholar] [CrossRef]
- Foerch, C.; Niessner, M.; Back, T.; Bauerle, M.; De Marchis, G.M.; Ferbert, A.; Grehl, H.; Hamann, G.F.; Jacobs, A.; Kastrup, A.; et al. Diagnostic Accuracy of Plasma Glial Fibrillary Acidic Protein for Differentiating Intracerebral Hemorrhage and Cerebral Ischemia in Patients with Symptoms of Acute Stroke. Clin. Chem. 2012, 58, 237–245. [Google Scholar] [CrossRef] [Green Version]
- Llombart, V.; García-Berrocoso, T.; Bustamante, A.; Giralt, D.; Rodriguez-Luna, D.; Muchada, M.; Penalba, A.; Boada, C.; Hernández-Guillamon, M.; Montaner, J. Plasmatic Retinol-Binding Protein 4 and Glial Fibrillary Acidic Protein as Biomarkers to Differentiate Ischemic Stroke and Intracerebral Hemorrhage. J. Neurochem. 2016, 136, 416–424. [Google Scholar] [CrossRef]
- Montaner, J.; Mendioroz, M.; Delgado, P.; García-Berrocoso, T.; Giralt, D.; Merino, C.; Ribó, M.; Rosell, A.; Penalba, A.; Fernández-Cadenas, I.; et al. Differentiating Ischemic from Hemorrhagic Stroke Using Plasma Biomarkers: The S100B/RAGE Pathway. J. Proteom. 2012, 75, 4758–4765. [Google Scholar] [CrossRef]
- Dias, A.; Silva, I.; Pinto, I.M.; Maia, L.F. Timely and Blood-Based Multiplex Molecular Profiling of Acute Stroke. Life 2021, 11, 816. [Google Scholar] [CrossRef] [PubMed]
- Bejleri, J.; Jirström, E.; Donovan, P.; Williams, D.J.; Pfeiffer, S. Diagnostic and Prognostic Circulating MicroRNA in Acute Stroke: A Systematic and Bioinformatic Analysis of Current Evidence. J. Stroke 2021, 23, 162–182. [Google Scholar] [CrossRef] [PubMed]
- Giordano, M.; Ciarambino, T.; D’Amico, M.; Trotta, M.C.; Di Sette, A.M.; Marfella, R.; Malatino, L.; Paolisso, G.; Adinolfi, L.E. Circulating miRNA-195-5p and -451a in Transient and Acute Ischemic Stroke Patients in an Emergency Department. J. Clin. Med. 2019, 8, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giordano, M.; Trotta, M.C.; Ciarambino, T.; D’Amico, M.; Galdiero, M.; Schettini, F.; Paternosto, D.; Salzillo, M.; Alfano, R.; Andreone, V.; et al. Circulating miRNA-195-5p and -451a in Diabetic Patients with Transient and Acute Ischemic Stroke in the Emergency Department. Int. J. Mol. Sci. 2020, 21, 7615. [Google Scholar] [CrossRef] [PubMed]
- Tiedt, S.; Prestel, M.; Malik, R.; Schieferdecker, N.; Duering, M.; Kautzky, V.; Stoycheva, I.; Böck, J.; Northoff, B.H.; Klein, M.; et al. RNA-Seq Identifies Circulating MiR-125a-5p, MiR-125b-5p, and MiR-143-3p as Potential Biomarkers for Acute Ischemic Stroke. Circ. Res. 2017, 121, 970–980. [Google Scholar] [CrossRef]
- Chen, Y.; Song, Y.; Huang, J.; Qu, M.; Zhang, Y.; Geng, J.; Zhang, Z.; Liu, J.; Yang, G.-Y. Increased Circulating Exosomal miRNA-223 Is Associated with Acute Ischemic Stroke. Front. Neurol. 2017, 8, 57. [Google Scholar] [CrossRef] [Green Version]
- Aldous, E.K.; Toor, S.M.; Parray, A.; Al-Sarraj, Y.; Diboun, I.; Abdelalim, E.M.; Arredouani, A.; El-Agnaf, O.; Thornalley, P.J.; Akhtar, N.; et al. Identification of Novel Circulating miRNAs in Patients with Acute Ischemic Stroke. Int. J. Mol. Sci. 2022, 23, 3387. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Y.; Huang, J.; Chen, X.; Gu, X.; Wang, Y.; Zeng, L.; Yang, G.-Y. Increase of Circulating MiR-223 and Insulin-like Growth Factor-1 Is Associated with the Pathogenesis of Acute Ischemic Stroke in Patients. BMC Neurol. 2014, 14, 77. [Google Scholar] [CrossRef] [Green Version]
- Jin, F.; Xing, J. Circulating MiR-126 and MiR-130a Levels Correlate with Lower Disease Risk, Disease Severity, and Reduced Inflammatory Cytokine Levels in Acute Ischemic Stroke Patients. Neurol. Sci. 2018, 39, 1757–1765. [Google Scholar] [CrossRef]
- Liu, P.; Han, Z.; Ma, Q.; Liu, T.; Wang, R.; Tao, Z.; Li, G.; Li, F.; Zhang, S.; Li, L.; et al. Upregulation of MicroRNA-128 in the Peripheral Blood of Acute Ischemic Stroke Patients Is Correlated with Stroke Severity Partially through Inhibition of Neuronal Cell Cycle Reentry. Cell Transpl. 2019, 28, 839–850. [Google Scholar] [CrossRef] [Green Version]
- Jia, L.; Hao, F.; Wang, W.; Qu, Y. Circulating MiR-145 Is Associated with Plasma High-Sensitivity C-Reactive Protein in Acute Ischemic Stroke Patients: Circulating MiR-145 in AIS. Cell Biochem. Funct. 2015, 33, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Kan, P.; Ma, Z.; Wang, Y.; Song, W.; Huang, C.; Zhang, B. Exploring the Potential Value of MiR-148b-3p, MiR-151b and MiR-27b-3p as Biomarkers in Acute Ischemic Stroke. Biosci. Rep. 2018, 38, BSR20181033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, B.; Zhu, Z.; Hao, J.; Wan, Z.; Guo, X. Decreased Plasma MiR-335 Expression in Patients with Acute Ischemic Stroke and Its Association with Calmodulin Expression. J. Int. Med. Res. 2016, 44, 1331–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sultan, W.; Machado, L.G.D.D.; Ali, M.G.; Tramontana, A.; Bayoumy, A.E.; Baxter, S.G.; Aly, M.R.A.; Bilotta, F. MicroRNAs as Biomarkers in Spontaneous Intracerebral Hemorrhage: A Systematic Review of Recent Clinical Evidence. Clin. Neurol. Neurosurg. 2022, 213, 107130. [Google Scholar] [CrossRef]
- Wang, J.; Zhu, Y.; Jin, F.; Tang, L.; He, Z.; He, Z. Differential Expression of Circulating MicroRNAs in Blood and Haematoma Samples from Patients with Intracerebral Haemorrhage. J. Int. Med. Res. 2016, 44, 419–432. [Google Scholar] [CrossRef] [Green Version]
- Fu, X.; Niu, T.; Li, X. MicroRNA-126-3p Attenuates Intracerebral Hemorrhage-Induced Blood-Brain Barrier Disruption by Regulating VCAM-1 Expression. Front. Neurosci. 2019, 13, 866. [Google Scholar] [CrossRef] [Green Version]
- Leung, L.Y.; Chan, C.P.Y.; Leung, Y.K.; Jiang, H.L.; Abrigo, J.M.; Wang, D.F.; Chung, J.S.H.; Rainer, T.H.; Graham, C.A. Comparison of MiR-124-3p and MiR-16 for Early Diagnosis of Hemorrhagic and Ischemic Stroke. Clin. Chim. Acta 2014, 433, 139–144. [Google Scholar] [CrossRef]
- Martinez, B.; Peplow, P. Blood MicroRNAs as Potential Diagnostic Markers for Hemorrhagic Stroke. Neural Regen. Res. 2017, 12, 13. [Google Scholar] [CrossRef]
- Zhu, Y.; Wang, J.-L.; He, Z.-Y.; Jin, F.; Tang, L. Association of Altered Serum MicroRNAs with Perihematomal Edema after Acute Intracerebral Hemorrhage. PLoS ONE 2015, 10, e0133783. [Google Scholar] [CrossRef]
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.B.; Culebras, A.; Elkind, M.S.V.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An Updated Definition of Stroke for the 21st Century: A Statement for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef] [Green Version]
- Yin, K.-J.; Hamblin, M.; Chen, Y.E. Angiogenesis-Regulating MicroRNAs and Ischemic Stroke. Curr. Vasc. Pharmacol. 2015, 13, 352–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Morris-Blanco, K.C.; Lopez, M.S.; Yang, T.; Zhao, H.; Vemuganti, R.; Luo, Y. Impact of MicroRNAs on Ischemic Stroke: From Pre- to Post-Disease. Prog. Neurobiol. 2018, 163–164, 59–78. [Google Scholar] [CrossRef] [PubMed]
- Atif, H.; Hicks, S.D. A Review of MicroRNA Biomarkers in Traumatic Brain Injury. J. Exp. Neurosci. 2019, 13, 1179069519832286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, Y.; Zhang, Z.; Wang, Z.; Liu, J. miRNA-27b Regulates Angiogenesis by Targeting AMPK in Mouse Ischemic Stroke Model. Neuroscience 2019, 398, 12–22. [Google Scholar] [CrossRef]
- Gugliandolo, A.; Silvestro, S.; Sindona, C.; Bramanti, P.; Mazzon, E. miRNA: Involvement of the MAPK Pathway in Ischemic Stroke. A Promising Therapeutic Target. Medicina 2021, 57, 1053. [Google Scholar] [CrossRef]
- Pignataro, G. Emerging Role of MicroRNAs in Stroke Protection Elicited by Remote Postconditioning. Front. Neurol. 2021, 12, 748709. [Google Scholar] [CrossRef]
- Saif, J.; Emanueli, C. miRNAs in Post-Ischaemic Angiogenesis and Vascular Remodelling. Biochem. Soc. Trans. 2014, 42, 1629–1636. [Google Scholar] [CrossRef]
- Dewdney, B.; Trollope, A.; Moxon, J.; Thomas Manapurathe, D.; Biros, E.; Golledge, J. Circulating MicroRNAs as Biomarkers for Acute Ischemic Stroke: A Systematic Review. J. Stroke Cerebrovasc. Dis. 2018, 27, 522–530. [Google Scholar] [CrossRef]
- Sun, S.; Li, L.; Dong, L.; Cheng, J.; Zhao, C.; Bao, C.; Wang, H. Circulating MRNA and MicroRNA Profiling Analysis in Patients with Ischemic Stroke. Mol. Med. Rep. 2020, 22, 792–802. [Google Scholar] [CrossRef]
- Liu, H.M. Neovasculature and Blood-Brain Barrier in Ischemic Brain Infarct. Acta Neuropathol. 1988, 75, 422–426. [Google Scholar] [CrossRef]
- Chen, H.H.; Chien, C.H.; Liu, H.M. Correlation between Angiogenesis and Basic Fibroblast Growth Factor Expression in Experimental Brain Infarct. Stroke 1994, 25, 1651–1657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krupinski, J.; Kaluza, J.; Kumar, P.; Kumar, S.; Wang, J.M. Role of Angiogenesis in Patients with Cerebral Ischemic Stroke. Stroke 1994, 25, 1794–1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.Y.; Ju, W.K.; Cha, J.H.; Son, B.C.; Chun, M.H.; Kang, J.K.; Park, C.K. Expression of Vascular Endothelial Growth Factor MRNA Following Transient Forebrain Ischemia in Rats. Neurosci. Lett. 1999, 265, 107–110. [Google Scholar] [CrossRef]
- Jin, K.L.; Mao, X.O.; Nagayama, T.; Goldsmith, P.C.; Greenberg, D.A. Induction of Vascular Endothelial Growth Factor and Hypoxia-Inducible Factor-1alpha by Global Ischemia in Rat Brain. Neuroscience 2000, 99, 577–585. [Google Scholar] [CrossRef]
- Gu, W.; Brännström, T.; Jiang, W.; Bergh, A.; Wester, P. Vascular Endothelial Growth Factor-A and -C Protein up-Regulation and Early Angiogenesis in a Rat Photothrombotic Ring Stroke Model with Spontaneous Reperfusion. Acta Neuropathol. 2001, 102, 216–226. [Google Scholar] [CrossRef]
- Xiong, Y.; Mahmood, A.; Chopp, M. Angiogenesis, Neurogenesis and Brain Recovery of Function Following Injury. Curr. Opin. Investig. Drugs 2010, 11, 298–308. [Google Scholar]
- Ergul, A.; Alhusban, A.; Fagan, S.C. Angiogenesis: A Harmonized Target for Recovery after Stroke. Stroke 2012, 43, 2270–2274. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, D.A.; Jin, K. Vascular Endothelial Growth Factors (VEGFs) and Stroke. Cell. Mol. Life Sci. 2013, 70, 1753–1761. [Google Scholar] [CrossRef]
- Liu, J.; Wang, Y.; Akamatsu, Y.; Lee, C.C.; Stetler, R.A.; Lawton, M.T.; Yang, G.-Y. Vascular Remodeling after Ischemic Stroke: Mechanisms and Therapeutic Potentials. Prog. Neurobiol. 2014, 115, 138–156. [Google Scholar] [CrossRef] [Green Version]
- Cosky, E.E.P.; Ding, Y. The Role of Vascular Endothelial Growth Factor in Angiogenesis and Brain Circulation after Stroke. Brain Circ. 2018, 4, 73–75. [Google Scholar] [CrossRef]
- Beck, H.; Plate, K.H. Angiogenesis after Cerebral Ischemia. Acta Neuropathol. 2009, 117, 481–496. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Lawes, C.M.M.; Bennett, D.A.; Barker-Collo, S.L.; Parag, V. Worldwide Stroke Incidence and Early Case Fatality Reported in 56 Population-Based Studies: A Systematic Review. Lancet Neurol. 2009, 8, 355–369. [Google Scholar] [CrossRef]
- Hemphill, J.C.; Greenberg, S.M.; Anderson, C.S.; Becker, K.; Bendok, B.R.; Cushman, M.; Fung, G.L.; Goldstein, J.N.; Macdonald, R.L.; Mitchell, P.H.; et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2015, 46, 2032–2060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toyoda, K.; Koga, M.; Iguchi, Y.; Itabashi, R.; Inoue, M.; Okada, Y.; Ogasawara, K.; Tsujino, A.; Hasegawa, Y.; Hatano, T.; et al. Guidelines for Intravenous Thrombolysis (Recombinant Tissue-Type Plasminogen Activator), the Third Edition, March 2019: A Guideline from the Japan Stroke Society. Neurol. Med. Chir. 2019, 59, 449–491. [Google Scholar] [CrossRef] [Green Version]
- Broderick, J.P.; Adeoye, O.; Elm, J. Evolution of the Modified Rankin Scale and Its Use in Future Stroke Trials. Stroke 2017, 48, 2007–2012. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e110. [Google Scholar] [CrossRef]
- Cheng, H.-Y.; Wang, Y.-S.; Hsu, P.-Y.; Chen, C.-Y.; Liao, Y.-C.; Juo, S.-H.H. MiR-195 Has a Potential to Treat Ischemic and Hemorrhagic Stroke through Neurovascular Protection and Neurogenesis. Mol. Ther. Methods Clin. Dev. 2019, 13, 121–132. [Google Scholar] [CrossRef] [Green Version]
- Stylli, S.S.; Adamides, A.A.; Koldej, R.M.; Luwor, R.B.; Ritchie, D.S.; Ziogas, J.; Kaye, A.H. miRNA Expression Profiling of Cerebrospinal Fluid in Patients with Aneurysmal Subarachnoid Hemorrhage. J. Neurosurg. 2017, 126, 1131–1139. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Zhang, A.; Xiang, J.; Lv, Y.; Zhang, X. MiR-451 Acts as a Suppressor of Angiogenesis in Hepatocellular Carcinoma by Targeting the IL-6R-STAT3 Pathway. Oncol. Rep. 2016, 36, 1385–1392. [Google Scholar] [CrossRef]
- Zhao, W.-J.; Zhang, H.-F.; Su, J.-Y. Downregulation of MicroRNA-195 Promotes Angiogenesis Induced by Cerebral Infarction via Targeting VEGFA. Mol. Med. Rep. 2017, 16, 5434–5440. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| C | ICH | AIS | p Value | |
|---|---|---|---|---|
| N (M) | 21 (10) | 21 (11) | 20 (9) | ns |
| Age (years) | 69 ± 2 | 68 ± 3 | 73 ± 5 | ns |
| BMI (kg/m2) | 27 ± 2 | 25 ± 5 | 26 ± 4 | ns |
| SBP (mmHg) | 142 ± 6 | 141 ± 7 | 139 ± 5 | ns |
| DBP (mmHg) | 81 ± 2 | 85 ± 5 | 82 ± 3 | ns |
| Hypertension (%) | 9 (43) | 11 (52) | 9 (45) | ns |
| Smoking (%) | (25) | (35) | (35) | ns |
| Hyperlipidemia (%) | (40) | (45) | (50) | ns |
| NIHSS score | - | 15 ± 1.4 | 16 ± 1.6 | ns * |
| Modified Rankin scale | - | 3.7 ± 0.4 | 3.5 ± 0.3 | ns * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giordano, M.; Trotta, M.C.; Ciarambino, T.; D’Amico, M.; Schettini, F.; Sisto, A.D.; D’Auria, V.; Voza, A.; Malatino, L.S.; Biolo, G.; et al. Circulating miRNA-195-5p and -451a in Patients with Acute Hemorrhagic Stroke in Emergency Department. Life 2022, 12, 763. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050763
Giordano M, Trotta MC, Ciarambino T, D’Amico M, Schettini F, Sisto AD, D’Auria V, Voza A, Malatino LS, Biolo G, et al. Circulating miRNA-195-5p and -451a in Patients with Acute Hemorrhagic Stroke in Emergency Department. Life. 2022; 12(5):763. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050763
Chicago/Turabian StyleGiordano, Mauro, Maria Consiglia Trotta, Tiziana Ciarambino, Michele D’Amico, Federico Schettini, Angela Di Sisto, Valentina D’Auria, Antonio Voza, Lorenzo Salvatore Malatino, Gianni Biolo, and et al. 2022. "Circulating miRNA-195-5p and -451a in Patients with Acute Hemorrhagic Stroke in Emergency Department" Life 12, no. 5: 763. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050763