
Patient Selection and Clinical Indication for Chronic Total Occlusion Revascularization—A Workflow Focusing on Non-Invasive Cardiac Imaging
 ,
,  ,
,  ,
,
Abstract
:1. Introduction to Chronic Total Occlusion and Revascularization Recommendations
2. Which Patient May Benefit from CTO PCI?
2.1. Viability
2.2. Ischemia
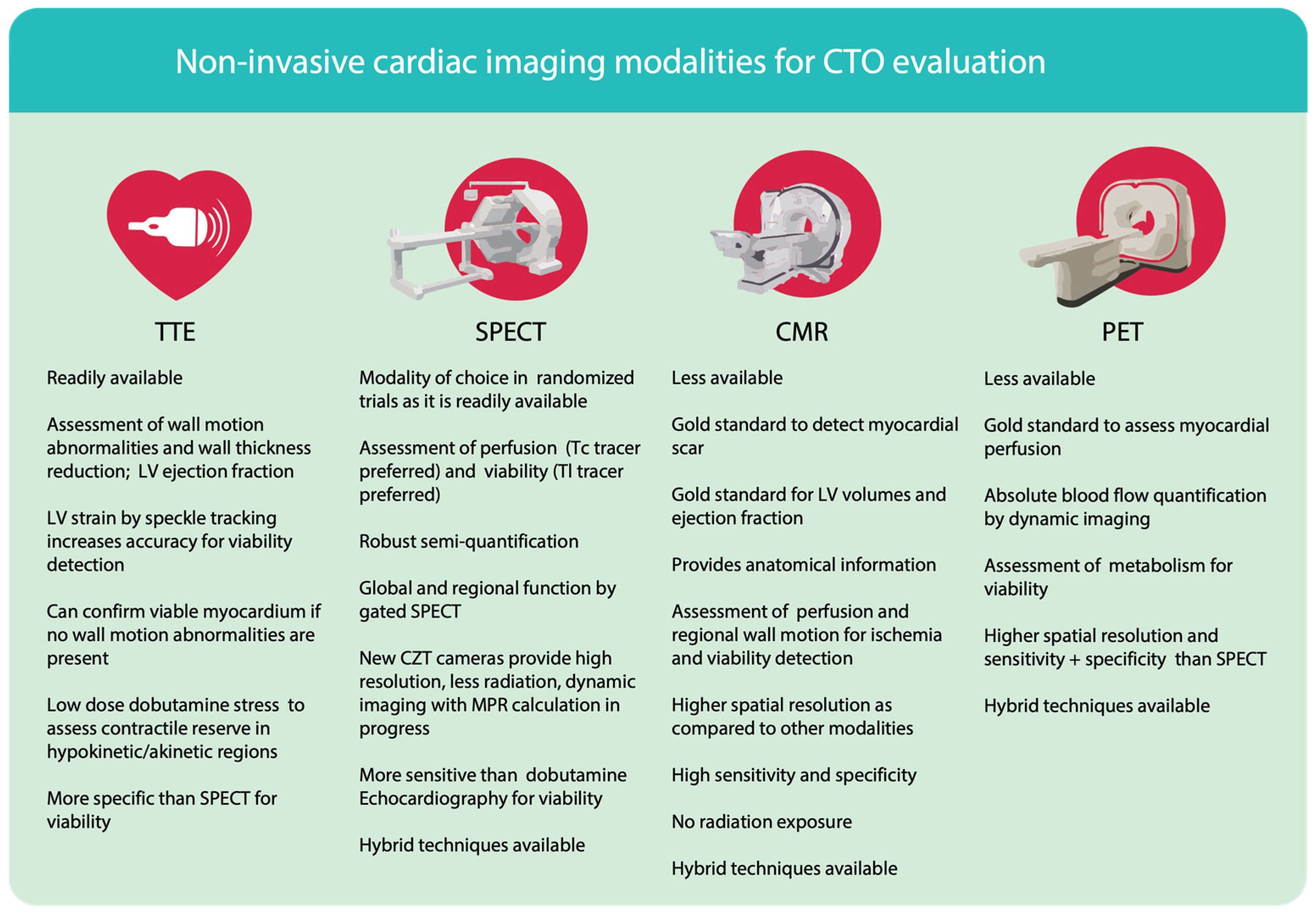
3. Non-Invasive Tools for Assessment of Viability and Ischemia
3.1. Transthoracic Echocardiography (TTE)
3.2. Single Photon Emission Computer Tomography (SPECT)
3.3. Positron Emission Tomography (PET)
3.4. Cardiac Magnetic Resonance Tomography (CMR)
4. Concluding Interpretations and Proposed Workflow
4.1. Choice and Interpretations of Non-Invasive Imaging Modalities
4.2. Proposed Workflow

Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Brilakis, E.S.; Mashayekhi, K.; Burke, M.N. How DECISION-CTO Can Help Guide the Decision to Perform Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation 2019, 139, 1684–1687. [Google Scholar] [CrossRef] [PubMed]
- Seiler, C.; Stoller, M.; Pitt, B.; Meier, P. The human coronary collateral circulation: Development and clinical importance. Eur. Heart J. 2013, 34, 2674–2682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brilakis, E.S.; Mashayekhi, K.; Tsuchikane, E.; Rafeh, N.A.; Alaswad, K.; Araya, M.; Avran, A.; Azzalini, L.; Babunashvili, A.M.; Bayani, B.; et al. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation 2019, 140, 420–433. [Google Scholar] [CrossRef]
- Henriques, J.P.; Hoebers, L.P.; Råmunddal, T.; Laanmets, P.; Eriksen, E.; Bax, M.; Ioanes, D.; Suttorp, M.J.; Strauss, B.H.; Barbato, E.; et al. Percutaneous Intervention for Concurrent Chronic Total Occlusions in Patients with STEMI. J. Am. Coll. Cardiol. 2016, 68, 1622–1632. [Google Scholar] [CrossRef] [PubMed]
- Werner, G.S.; Martin-Yuste, V.; Hildick-Smith, D.; Boudou, N.; Sianos, G.; Gelev, V.; Rumoroso, J.R.; Erglis, A.; Christiansen, E.H.; Escaned, J.; et al. A randomized multicentre trial to compare revascularization with optimal medical therapy for the treatment of chronic total coronary occlusions. Eur. Heart J. 2018, 39, 2484–2493. [Google Scholar] [CrossRef] [Green Version]
- Mashayekhi, K.; Nührenberg, T.G.; Toma, A.; Gick, M.; Ferenc, M.; Hochholzer, W.; Comberg, T.; Rothe, J.; Valina, C.M.; Löffelhardt, N.; et al. A Randomized Trial to Assess Regional Left Ventricular Function After Stent Implantation in Chronic Total Occlusion. JACC Cardiovasc. Interv. 2018, 11, 1982–1991. [Google Scholar] [CrossRef]
- Lee, S.-W.; Lee, P.H.; Ahn, J.-M.; Park, D.-W.; Yun, S.-C.; Han, S.; Kang, H.; Kang, S.-J.; Kim, Y.-H.; Lee, C.W.; et al. Randomized Trial Evaluating Percutaneous Coronary Intervention for the Treatment of Chronic Total Occlusion. Circulation 2019, 139, 1674–1683. [Google Scholar] [CrossRef]
- Tajti, P.; Burke, M.N.; Karmpaliotis, D.; Alaswad, K.; Werner, G.S.; Azzalini, L.; Carlino, M.; Patel, M.; Mashayekhi, K.; Egred, M.; et al. Update in the Percutaneous Management of Coronary Chronic Total Occlusions. JACC Cardiovasc. Interv. 2018, 11, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Mashayekhi, K.; Neuser, H.; Kraus, A.; Zimmer, M.; Dalibor, J.; Akin, I.; Werner, G.; Aurel, T.; Neumann, F.-J.; Behnes, M. Successful Percutaneous Coronary Intervention Improves Cardiopulmonary Exercise Capacity in Patients with Chronic Total Occlusions. J. Am. Coll. Cardiol. 2017, 69, 1095–1096. [Google Scholar] [CrossRef]
- Sapontis, J.; Salisbury, A.C.; Yeh, R.W.; Cohen, D.J.; Hirai, T.; Lombardi, W.; McCabe, J.M.; Karmpaliotis, D.; Moses, J.; Nicholson, W.J.; et al. Early Procedural and Health Status Outcomes After Chronic Total Occlusion Angioplasty. JACC Cardiovasc. Interv. 2017, 10, 1523–1534. [Google Scholar] [CrossRef]
- Claessen, B.E.; Dangas, G.D.; Weisz, G.; Witzenbichler, B.; Guagliumi, G.; Möckel, M.; Brener, S.J.; Xu, K.; Henriques, J.P.; Mehran, R.; et al. Prognostic impact of a chronic total occlusion in a non-infarct-related artery in patients with ST-segment elevation myocardial infarction: 3-year results from the HORIZONS-AMI trial. Eur. Heart J. 2012, 33, 768–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tajti, P.; Karmpaliotis, D.; Alaswad, K.; Jaffer, F.A.; Yeh, R.W.; Patel, M.; Mahmud, E.; Choi, J.W.; Burke, M.N.; Doing, A.H.; et al. The Hybrid Approach to Chronic Total Occlusion Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2018, 11, 1325–1335. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.M.; Walsh, S.J.; Yan, A.T.; Hanratty, C.G.; Bagnall, A.J.; Egred, M.; Smith, E.; Oldroyd, K.G.; McEntegart, M.; Irving, J.; et al. Hybrid approach improves success of chronic total occlusion angioplasty. Heart 2016, 102, 1486–1493. [Google Scholar] [CrossRef] [PubMed]
- Brilakis, E.S.; Banerjee, S.; Karmpaliotis, D.; Lombardi, W.L.; Tsai, T.T.; Shunk, K.A.; Kennedy, K.F.; Spertus, J.A.; Holmes, D.R.; Grantham, J.A. Procedural Outcomes of Chronic Total Occlusion Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2015, 8, 245–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, M.R.; Calhoon, J.H.; Dehmer, G.J.; Grantham, J.A.; Maddox, T.M.; Maron, D.J.; Smith, P.K. ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 Appropriate Use Criteria for Coronary Revascularization in Patients with Stable Ischemic Heart Disease. J. Am. Coll. Cardiol. 2017, 69, 2212–2241. [Google Scholar] [CrossRef]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [Green Version]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization. J. Am. Coll. Cardiol. 2022, 79, e21–e129. [Google Scholar] [CrossRef]
- Camici, P.G.; Prasad, S.K.; Rimoldi, O.E. Stunning, Hibernation, and Assessment of Myocardial Viability. Circulation 2008, 117, 103–114. [Google Scholar] [CrossRef] [Green Version]
- Al-Lamee, R.; Thompson, D.; Dehbi, H.-M.; Sen, S.; Tang, K.; Davies, J.; Keeble, T.; Mielewczik, M.; Kaprielian, R.; Malik, I.S.; et al. Percutaneous coronary intervention in stable angina (ORBITA): A double-blind, randomised controlled trial. Lancet 2018, 391, 31–40. [Google Scholar] [CrossRef] [Green Version]
- Windecker, S.; Stortecky, S.; Stefanini, G.; da Costa, B.R.; Rutjes, A.W.S.; Di Nisio, M.; Siletta, M.G.; Maione, A.; Alfonso, F.; Clemmensen, P.M.; et al. Revascularisation versus medical treatment in patients with stable coronary artery disease: Network meta-analysis. BMJ 2014, 348, g3859. [Google Scholar] [CrossRef]
- Allman, K.C.; Shaw, L.J.; Hachamovitch, R.; E Udelson, J. Myocardial viability testing and impact of revascularization on prognosis in patients with coronary artery disease and left ventricular dysfunction: A meta-analysis. J. Am. Coll. Cardiol. 2002, 39, 1151–1158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zannad, F.; Ferreira, J.P.; Pocock, S.J.; Anker, S.D.; Butler, J.; Filippatos, G.; Brueckmann, M.; Ofstad, A.P.; Pfarr, E.; Jamal, W.; et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: A meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet 2020, 396, 819–829. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.; Morgan, H.; Chiribiri, A.; Nagel, E.; Cleland, J.; Perera, D. Myocardial viability testing: All STICHed up, or about to be REVIVED? Eur. Heart J. 2022, 43, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Velazquez, E.J.; Lee, K.L.; Deja, M.A.; Jain, A.; Sopko, G.; Marchenko, A.; Ali, I.S.; Pohost, G.; Gradinac, S.; Abraham, W.T.; et al. Coronary-Artery Bypass Surgery in Patients with Left Ventricular Dysfunction. N. Engl. J. Med. 2011, 364, 1607–1616. [Google Scholar] [CrossRef] [Green Version]
- Howlett, J.G.; Stebbins, A.; Petrie, M.C.; Jhund, P.S.; Castelvecchio, S.; Cherniavsky, A.; Sueta, C.A.; Roy, A.; Piña, I.L.; Wurm, R.; et al. CABG Improves Outcomes in Patients with Ischemic Cardiomyopathy. JACC Heart Fail. 2019, 7, 878–887. [Google Scholar] [CrossRef]
- Fearon, W.F.; Zimmermann, F.M.; De Bruyne, B.; Piroth, Z.; van Straten, A.H.; Szekely, L.; Davidavičius, G.; Kalinauskas, G.; Mansour, S.; Kharbanda, R.; et al. Fractional Flow Reserve–Guided PCI as Compared with Coronary Bypass Surgery. N. Engl. J. Med. 2022, 386, 128–137. [Google Scholar] [CrossRef]
- Perera, D.; Clayton, T.; O’Kane, P.D.; Greenwood, J.P.; Weerackody, R.; Ryan, M.; Morgan, H.P.; Dodd, M.; Evans, R.; Canter, R.; et al. Percutaneous Revascularization for Ischemic Left Ventricular Dysfunction. N. Engl. J. Med. 2022, 387, 1351–1360. [Google Scholar] [CrossRef]
- Beanlands, R.S.; Nichol, G.; Huszti, E.; Humen, D.; Racine, N.; Freeman, M.; Gulenchyn, K.Y.; Garrard, L.; Dekemp, R.; Guo, A.; et al. F-18-Fluorodeoxyglucose Positron Emission Tomography Imaging-Assisted Management of Patients with Severe Left Ventricular Dysfunction and Suspected Coronary Disease: A Randomized, Controlled Trial (PARR-2). J. Am. Coll. Cardiol. 2007, 50, 2002–2012. [Google Scholar] [CrossRef] [Green Version]
- Gerber, B.L.; Rousseau, M.F.; Ahn, S.A.; Waroux, J.-B.L.P.D.; Pouleur, A.-C.; Phlips, T.; Vancraeynest, D.; Pasquet, A.; Vanoverschelde, J.-L.J. Prognostic Value of Myocardial Viability by Delayed-Enhanced Magnetic Resonance in Patients with Coronary Artery Disease and Low Ejection Fraction: Impact of Revascularization Therapy. J. Am. Coll. Cardiol. 2012, 59, 825–835. [Google Scholar] [CrossRef]
- Safley, D.M.; Koshy, S.; Grantham, J.A.; Bybee, K.A.; House, J.A.; Ms, K.F.K.; Rutherford, B.D. Changes in myocardial ischemic burden following percutaneous coronary intervention of chronic total occlusions. Catheter. Cardiovasc. Interv. 2011, 78, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Ling, L.F.; Marwick, T.H.; Flores, D.R.; Jaber, W.A.; Brunken, R.C.; Cerqueira, M.D.; Hachamovitch, R. Identification of Therapeutic Benefit from Revascularization in Patients with Left Ventricular Systolic Dysfunction. Circ. Cardiovasc. Imaging 2013, 6, 363–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frangogiannis, N.G. The pathological basis of myocardial hibernation. Histol. Histopathol. 2003, 18, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.P.; Mc Ardle, B.A.; Beanlands, R.S.; Hessian, R.C. Myocardial Viability: It is Still Alive. Semin. Nucl. Med. 2014, 44, 358–374. [Google Scholar] [CrossRef] [PubMed]
- Roes, S.D.; Mollema, S.A.; Lamb, H.J.; van der Wall, E.E.; de Roos, A.; Bax, J.J. Validation of Echocardiographic Two-Dimensional Speckle Tracking Longitudinal Strain Imaging for Viability Assessment in Patients with Chronic Ischemic Left Ventricular Dysfunction and Comparison with Contrast-Enhanced Magnetic Resonance Imaging. Am. J. Cardiol. 2009, 104, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.; Pennell, D.; Ray, S.; Coats, A.; Macfarlane, P.; Murray, G.; Mule, J.D.; Vered, Z.; Lahiri, A. Myocardial viability as a determinant of the ejection fraction response to carvedilol in patients with heart failure (CHRISTMAS trial): Randomised controlled trial. Lancet 2003, 362, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Hachamovitch, R.; Rozanski, A.; Shaw, L.J.; Stone, G.W.; Thomson, L.E.J.; Friedman, J.D.; Hayes, S.W.; Cohen, I.; Germano, G.; Berman, D.S. Impact of ischaemia and scar on the therapeutic benefit derived from myocardial revascularization vs. medical therapy among patients undergoing stress-rest myocardial perfusion scintigraphy. Eur. Heart J. 2011, 32, 1012–1024. [Google Scholar] [CrossRef] [PubMed]
- Boden, W.E.; O’Rourke, R.A.; Teo, K.K.; Hartigan, P.M.; Maron, D.J.; Kostuk, W.J.; Knudtson, M.; Dada, M.; Casperson, P.; Harris, C.L.; et al. Optimal Medical Therapy with or without PCI for Stable Coronary Disease. N. Engl. J. Med. 2007, 356, 1503–1516. [Google Scholar] [CrossRef] [Green Version]
- D’Egidio, G.; Nichol, G.; Williams, K.A.; Guo, A.; Garrard, L.; Dekemp, R.; Ruddy, T.D.; DaSilva, J.; Humen, D.; Gulenchyn, K.Y.; et al. Increasing Benefit From Revascularization Is Associated with Increasing Amounts of Myocardial Hibernation: A Substudy of the PARR-2 Trial. JACC Cardiovasc. Imaging 2009, 2, 1060–1068. [Google Scholar] [CrossRef] [Green Version]
- van Nunen, L.X.; Zimmermann, F.M.; Tonino, P.A.L.; Barbato, E.; Baumbach, A.; Engstrøm, T.; Klauss, V.; A MacCarthy, P.; Manoharan, G.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet 2015, 386, 1853–1860. [Google Scholar] [CrossRef]
- Johnson, N.P.; Gould, K.L. Physiological Basis for Angina and ST-Segment Change: PET-Verified Thresholds of Quantitative Stress Myocardial Perfusion and Coronary Flow Reserve. JACC Cardiovasc. Imaging 2011, 4, 990–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werner, G.S.; Surber, R.; Ferrari, M.; Fritzenwanger, M.; Figulla, H.R. The functional reserve of collaterals supplying long-term chronic total coronary occlusions in patients without prior myocardial infarction. Eur. Heart J. 2006, 27, 2406–2412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obedinskiy, A.A.; Kretov, E.I.; Boukhris, M.; Kurbatov, V.P.; Osiev, A.G.; Ibn Elhadj, Z.; Obedinskaya, N.R.; Kasbaoui, S.; Grazhdankin, I.O.; Prokhorikhin, A.A.; et al. The IMPACTOR-CTO Trial. JACC Cardiovasc. Interv. 2018, 11, 1309–1311. [Google Scholar] [CrossRef] [PubMed]
- Flotats, A.; Knuuti, J.; Gutberlet, M.; Marcassa, C.; Bengel, F.; Kaufmann, P.A.; Rees, M.R.; Hesse, B. Hybrid cardiac imaging: SPECT/CT and PET/CT. A joint position statement by the European Association of Nuclear Medicine (EANM), the European Society of Cardiac Radiology (ESCR) and the European Council of Nuclear Cardiology (ECNC). Eur. J. Pediatr. 2011, 38, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Bax, J.J.; Delgado, V. Detection of viable myocardium and scar tissue: Table 1. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1062–1064. [Google Scholar] [CrossRef] [Green Version]
- Neglia, D.; Rovai, D.; Caselli, C.; Pietila, M.; Teresinska, A.; Aguadé-Bruix, S.; Pizzi, M.N.; Todiere, G.; Gimelli, A.; Schroeder, S.; et al. Detection of Significant Coronary Artery Disease by Noninvasive Anatomical and Functional Imaging. Circ. Cardiovasc. Imaging 2015, 8, e002179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, D.J.; Kim, H.W.; James, O.; Parker, M.; Wu, E.; Bonow, R.O.; Judd, R.M.; Kim, R.J. Prevalence of Regional Myocardial Thinning and Relationship with Myocardial Scarring in Patients with Coronary Artery Disease. JAMA 2013, 309, 909–918. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, R.; Agrawal, M.; Flynn, S.E.; Werner, G.S.; Uretsky, B.F. The myocardium supplied by a chronic total occlusion is a persistently ischemic zone. Catheter. Cardiovasc. Interv. 2014, 83, 9–16. [Google Scholar] [CrossRef]
- Cornel, J.H.; Bax, J.J.; Elhendy, A.; Maat, A.P.; Kimman, G.-J.P.; Geleijnse, M.L.; Rambaldi, R.; Boersma, E.; Fioretti, P.M. Biphasic Response to Dobutamine Predicts Improvement of Global Left Ventricular Function After Surgical Revascularization in Patients with Stable Coronary Artery Disease: Implications of Time Course of Recovery on Diagnostic Accuracy. J. Am. Coll. Cardiol. 1998, 31, 1002–1010. [Google Scholar] [CrossRef] [Green Version]
- Pellikka, P.A.; Arruda-Olson, A.; Chaudhry, F.A.; Chen, M.H.; Marshall, J.E.; Porter, T.R.; Sawada, S.G. Guidelines for Performance, Interpretation, and Application of Stress Echocardiography in Ischemic Heart Disease: From the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2020, 33, 1–41.e8. [Google Scholar] [CrossRef]
- Hickman, M.; Chelliah, R.; Burden, L.; Senior, R. Resting myocardial blood flow, coronary flow reserve, and contractile reserve in hibernating myocardium: Implications for using resting myocardial contrast echocardiography vs. dobutamine echocardiography for the detection of hibernating myocardium. Eur. J. Echocardiogr. 2010, 11, 756–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sicari, R.; Nihoyannopoulos, P.; Evangelista, A.; Kasprzak, J.; Lancellotti, P.; Poldermans, D.; Voigt, J.-U.; Zamorano, J.L. On behalf of the European Association of Echocardiography Stress echocardiography expert consensus statement: European Association of Echocardiography (EAE) (a registered branch of the ESC). Eur. J. Echocardiogr. 2008, 9, 415–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortigiani, L.; Urluescu, M.-L.; Coltelli, M.; Carpeggiani, C.; Bovenzi, F.; Picano, E. Apparent Declining Prognostic Value of a Negative Stress Echocardiography Based on Regional Wall Motion Abnormalities in Patients with Normal Resting Left Ventricular Function Due to the Changing Referral Profile of the Population Under Study. Circ. Cardiovasc. Imaging 2019, 12, e008564. [Google Scholar] [CrossRef] [PubMed]
- Kayden, D.S.; Sigal, S.; Soufer, R.; Mattera, J.; Zaret, B.L.; Wackers, F.J.T. Thallium-201 for assessment of myocardial viability: Quantitative comparison of 24-hour redistribution imaging with imaging after reinjection at rest. J. Am. Coll. Cardiol. 1991, 18, 1480–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gewirtz, H.; A Beller, G.; Strauss, H.W.; E Dinsmore, R.; Zir, L.M.; A McKusick, K.; Pohost, G.M. Transient defects of resting thallium scans in patients with coronary artery disease. Circulation 1979, 59, 707–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Udelson, J.E.; Coleman, P.S.; Metherall, J.; Pandian, N.G.; Gomez, A.R.; Griffith, J.L.; Shea, N.L.; Oates, E.; A Konstam, M. Predicting recovery of severe regional ventricular dysfunction. Comparison of resting scintigraphy with 201Tl and 99mTc-sestamibi. Circulation 1994, 89, 2552–2561. [Google Scholar] [CrossRef]
- Maes, A.F.; Borgers, M.; Flameng, W.; Nuyts, J.L.; van de Werf, F.; Ausma, J.J.; Sergeant, P.; A Mortelmans, L. Assessment of Myocardial Viability in Chronic Coronary Artery Disease Using Technetium-99m Sestamibi SPECT: Correlation with Histologic and Positron Emission Tomographic Studies and Functional Follow-Up. J. Am. Coll. Cardiol. 1997, 29, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Taillefer, R.; Amyot, R.; Turpin, S.; Lambert, R.; Pilon, C.; Jarry, M. Comparison between dipyridamole and adenosine as pharmacologic coronary vasodilators in detection of coronary artery disease with thallium 201 imaging. J. Nucl. Cardiol. 1996, 3, 204–211. [Google Scholar] [CrossRef]
- Loong, C.Y.; Anagnostopoulos, C. Diagnosis of coronary artery disease by radionuclide myocardial perfusion imaging. Heart 2004, 90, v2–v9. [Google Scholar] [CrossRef]
- Gimelli, A.; Liga, R.; Pasanisi, E.M.; Giorgetti, A.; Marras, G.; Favilli, B.; Marzullo, P. Evaluation of left ventricular diastolic function with a dedicated cadmium-zinc-telluride cardiac camera: Comparison with Doppler echocardiography. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 972–979. [Google Scholar] [CrossRef]
- Hachamovitch, R.; Hayes, S.W.; Friedman, J.D.; Cohen, I.; Berman, D.S. Comparison of the Short-Term Survival Benefit Associated with Revascularization Compared with Medical Therapy in Patients with No Prior Coronary Artery Disease Undergoing Stress Myocardial Perfusion Single Photon Emission Computed Tomography. Circulation 2003, 107, 2900–2907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, T.; Yang, L.-F.; Zhai, J.-L.; Li, J.; Wang, Q.-M.; Zhang, R.-J.; Wang, S.; Peng, Z.-H.; Li, M.; Sun, G. SPECT myocardial perfusion versus fractional flow reserve for evaluation of functional ischemia: A meta analysis. Eur. J. Radiol. 2014, 83, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Burrell, S.; MacDonald, A. Artifacts and pitfalls in myocardial perfusion imaging. J. Nucl. Med. Technol. 2006, 34, 193–211. [Google Scholar]
- Acampa, W.; Gaemperli, O.; Gimelli, A.; Knaapen, P.; Schindler, T.H.; Verberne, H.J.; Zellweger, M.J.; Reviewers, D.; Kaufmann, P.A.; Rosenhek, R.; et al. Role of risk stratification by SPECT, PET, and hybrid imaging in guiding management of stable patients with ischaemic heart disease: Expert panel of the EANM cardiovascular committee and EACVI. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1289–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gould, K.L.; Johnson, N.P.; Bateman, T.M.; Beanlands, R.S.; Bengel, F.M.; Bober, R.; Camici, P.G.; Cerqueira, M.D.; Chow, B.J.; Di Carli, M.F.; et al. Anatomic Versus Physiologic Assessment of Coronary Artery Disease. J. Am. Coll. Cardiol. 2013, 62, 1639–1653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrin, M.; Djaballah, W.; Moulin, F.; Claudin, M.; Veran, N.; Imbert, L.; Poussier, S.; Morel, O.; Besseau, C.; Verger, A.; et al. Stress-first protocol for myocardial perfusion SPECT imaging with semiconductor cameras: High diagnostic performances with significant reduction in patient radiation doses. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Einstein, A.J.; Pascual, T.N.B.; Mercuri, M.; Karthikeyan, G.; Vitola, J.V.; Mahmarian, J.J.; Better, N.; Bouyoucef, S.E.; Bom, H.H.-S.; Lele, V.; et al. Current worldwide nuclear cardiology practices and radiation exposure: Results from the 65 country IAEA Nuclear Cardiology Protocols Cross-Sectional Study (INCAPS). Eur. Heart J. 2015, 36, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- Ben-Haim, S.; Murthy, V.; Breault, C.; Allie, R.; Sitek, A.; Roth, N.; Fantony, J.; Moore, S.C.; Park, M.-A.; Kijewski, M.; et al. Quantification of Myocardial Perfusion Reserve Using Dynamic SPECT Imaging in Humans: A Feasibility Study. J. Nucl. Med. 2013, 54, 873–879. [Google Scholar] [CrossRef] [Green Version]
- Garcia, E.V. Are SPECT measurements of myocardial blood flow and flow reserve ready for clinical use? Eur. J. Pediatr. 2014, 41, 2291–2293. [Google Scholar] [CrossRef] [Green Version]
- Gimelli, A.; Bottai, M.; Giorgetti, A.; Genovesi, D.; Kusch, A.; Ripoli, A.; Marzullo, P. Comparison Between Ultrafast and Standard Single-Photon Emission CT in Patients with Coronary Artery Disease. Circ. Cardiovasc. Imaging 2011, 4, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Nakae, I.; Matsuo, S.; Tsutamoto, T.; Matsumoto, T.; Mitsunami, K.; Horie, M. Assessment of cardiac function in patients with heart disease by quantitative gated myocardial perfusion SPECT. Ann. Nucl. Med. 2007, 21, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Dilsizian, V.; Bacharach, S.L.; Beanlands, R.S.; Bergmann, S.R.; Delbeke, D.; Dorbala, S.; Gropler, R.J.; Knuuti, J.; Schelbert, H.R.; Travin, M.I. ASNC imaging guidelines/SNMMI procedure standard for positron emission tomography (PET) nuclear cardiology procedures. J. Nucl. Cardiol. 2016, 23, 1187–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anavekar, N.S.; Chareonthaitawee, P.; Narula, J.; Gersh, B.J. Revascularization in Patients with Severe Left Ventricular Dysfunction. J. Am. Coll. Cardiol. 2016, 67, 2874–2887. [Google Scholar] [CrossRef] [PubMed]
- Taqueti, V.R.; Hachamovitch, R.; Murthy, V.; Naya, M.; Foster, C.R.; Hainer, J.; Dorbala, S.; Blankstein, R.; Di Carli, M.F. Global Coronary Flow Reserve Is Associated with Adverse Cardiovascular Events Independently of Luminal Angiographic Severity and Modifies the Effect of Early Revascularization. Circulation 2015, 131, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziadi, M.C.; Dekemp, R.A.; Williams, K.; Guo, A.; Renaud, J.; Chow, B.; Klein, R.; Ruddy, T.D.; Aung, M.; Garrard, L.; et al. Does quantification of myocardial flow reserve using rubidium-82 positron emission tomography facilitate detection of multivessel coronary artery disease? J. Nucl. Cardiol. 2012, 19, 670–680. [Google Scholar] [CrossRef]
- Hutchins, G.D.; Schwaiger, M.; Rosenspire, K.C.; Krivokapich, J.; Schelbert, H.; Kuhl, D.E. Noninvasive quantification of regional blood flow in the human heart using N-13 ammonia and dynamic positron emission tomographic imaging. J. Am. Coll. Cardiol. 1990, 15, 1032–1042. [Google Scholar] [CrossRef] [Green Version]
- Cerqueira, M.D.; Weissman, N.J.; Dilsizian, V.; Jacobs, A.K.; Kaul, S.; Laskey, W.K.; Pennell, D.J.; Rumberger, J.A.; Ryan, T.; Verani, M.S. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart: A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation 2002, 105, 539–542. [Google Scholar] [CrossRef] [Green Version]
- Danad, I.; Uusitalo, V.; Kero, T.; Saraste, A.; Raijmakers, P.G.; Lammertsma, A.; Heymans, M.; Kajander, S.A.; Pietilä, M.; James, S.; et al. Quantitative Assessment of Myocardial Perfusion in the Detection of Significant Coronary Artery Disease. J. Am. Coll. Cardiol. 2014, 64, 1464–1475. [Google Scholar] [CrossRef] [Green Version]
- Parker, M.W.; Iskandar, A.; Limone, B.; Perugini, A.; Kim, H.; Jones, C.; Calamari, B.; Coleman, C.I.; Heller, G.V. Diagnostic accuracy of cardiac positron emission tomography versus single photon emission computed tomography for coronary artery disease: A bivariate meta-analysis. Circ. Cardiovasc. Imaging 2012, 5, 700–707. [Google Scholar] [CrossRef] [Green Version]
- Wolk, M.J.; Bailey, S.R.; Doherty, J.U.; Douglas, P.S.; Hendel, R.C.; Kramer, C.M.; Min, J.K.; Patel, M.R.; Rosenbaum, L.; Shaw, L.J.; et al. ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 Multimodality Appropriate Use Criteria for the Detection and Risk Assessment of Stable Ischemic Heart Disease. J. Am. Coll. Cardiol. 2014, 63, 380–406. [Google Scholar] [CrossRef] [Green Version]
- Pegg, T.J.; Selvanayagam, J.B.; Jennifer, J.; Francis, J.M.; Karamitsos, T.D.; Dall’Armellina, E.; Smith, K.L.; Taggart, D.P.; Neubauer, S. Prediction of global left ventricular functional recovery in patients with heart failure undergoing surgical revascularisation, based on late gadolinium enhancement Cardiovascular Magnetic Resonance. J. Cardiovasc. Magn. Reson. 2010, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Schuster, A.; Morton, G.; Chiribiri, A.; Perera, D.; Vanoverschelde, J.-L.; Nagel, E. Imaging in the Management of Ischemic Cardiomyopathy: Special Focus on Magnetic Resonance. J. Am. Coll. Cardiol. 2012, 59, 359–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, R.J.; Wu, E.; Rafael, A.; Chen, E.-L.; Parker, M.A.; Simonetti, O.; Klocke, F.J.; Bonow, R.O.; Judd, R.M. The Use of Contrast-Enhanced Magnetic Resonance Imaging to Identify Reversible Myocardial Dysfunction. N. Engl. J. Med. 2000, 343, 1445–1453. [Google Scholar] [CrossRef] [PubMed]
- Karamitsos, T.D.; Ab Ntusi, N.; Francis, J.M.; Holloway, C.J.; Myerson, S.G.; Neubauer, S. Feasibility and safety of high-dose adenosine perfusion cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2010, 12, 66–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jogiya, R.; Kozerke, S.; Morton, G.; De Silva, K.; Redwood, S.; Perera, D.; Nagel, E.; Plein, S. Validation of Dynamic 3-Dimensional Whole Heart Magnetic Resonance Myocardial Perfusion Imaging Against Fractional Flow Reserve for the Detection of Significant Coronary Artery Disease. J. Am. Coll. Cardiol. 2012, 60, 756–765. [Google Scholar] [CrossRef] [Green Version]
- Shin, T.; Hu, H.H.; Pohost, G.M.; Nayak, K.S. Three dimensional first-pass myocardial perfusion imaging at 3T: Feasibility study. J. Cardiovasc. Magn. Reson. 2008, 10, 57. [Google Scholar] [CrossRef] [Green Version]
- Greenwood, J.P.; Maredia, N.; Younger, J.; Brown, J.M.; Nixon, J.; Everett, C.C.; Bijsterveld, P.; Ridgway, J.P.; Radjenovic, A.; Dickinson, C.J.; et al. Cardiovascular magnetic resonance and single-photon emission computed tomography for diagnosis of coronary heart disease (CE-MARC): A prospective trial. Lancet 2012, 379, 453–460. [Google Scholar] [CrossRef] [Green Version]
- Nagel, E.; Greenwood, J.P.; McCann, G.P.; Bettencourt, N.; Shah, A.M.; Hussain, S.T.; Perera, D.; Plein, S.; Bucciarelli-Ducci, C.; Paul, M.; et al. Magnetic Resonance Perfusion or Fractional Flow Reserve in Coronary Disease. N. Engl. J. Med. 2019, 380, 2418–2428. [Google Scholar] [CrossRef]
- Pica, S.; Di Giovine, G.; Bollati, M.; Testa, L.; Bedogni, F.; Camporeale, A.; Pontone, G.; Andreini, D.; Monti, L.; Gasparini, G.; et al. Cardiac magnetic resonance for ischaemia and viability detection. Guiding patient selection to revascularization in coronary chronic total occlusions: The CARISMA_CTO study design. Int. J. Cardiol. 2018, 272, 356–362. [Google Scholar] [CrossRef]
- Christakopoulos, G.E.; Christopoulos, G.; Carlino, M.; Jeroudi, O.M.; Roesle, M.; Rangan, B.V.; Abdullah, S.; Grodin, J.; Kumbhani, D.J.; Vo, M.; et al. Meta-Analysis of Clinical Outcomes of Patients Who Underwent Percutaneous Coronary Interventions for Chronic Total Occlusions. Am. J. Cardiol. 2015, 115, 1367–1375. [Google Scholar] [CrossRef] [PubMed]
- Nkoulou, R.; Fuchs, T.A.; Pazhenkottil, A.P.; Kuest, S.M.; Ghadri, J.R.; Stehli, J.; Fiechter, M.; Herzog, B.A.; Gaemperli, O.; Buechel, R.R.; et al. Absolute Myocardial Blood Flow and Flow Reserve Assessed by Gated SPECT with Cadmium–Zinc–Telluride Detectors Using 99mTc-Tetrofosmin: Head-to-Head Comparison with 13N-Ammonia PET. J. Nucl. Med. 2016, 57, 1887–1892. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.P.; Kirkeeide, R.L.; Gould, K.L. Coronary Steal: Mechanisms of a Misnomer. J. Am. Heart Assoc. 2021, 10, e021000. [Google Scholar] [CrossRef] [PubMed]
- De Winter, R.W.; Schumacher, S.S.; Diemen, P.v.D.v.; Jukema, R.J.; Somsen, Y.S.; Stuijfzand, W.S.; Driessen, R.D.; Bom, M.B.; Everaars, H.; Rossum, A.v.R.v.; et al. Impact of percutaneous coronary intervention of chronic total occlusions on absolute perfusion in remote myocardium. EuroIntervention 2022, 18, e314–e323. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. American Thoracic Society. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Time | Number of Patients | Success Rate | Follow-Up (Median) | Findings |
|---|---|---|---|---|---|
| DECISION-CTO | 2010–2016 | 834 (1:1) | 90.6% | 4 years |
|
| EURO-CTO | 2012–2015 | 396 (2:1) | 86.6% | 1 year |
|
| EXPLORE | 2007–2015 | 304 (1:1) | 77% | 4 months |
|
| REVASC | 2007–2015 | 205 (1:1) | 86% at first attempt (99% overall) | 1 year |
|
| IMPACTOR (RCA CTO) | 2010–2014 | 94 (1:1) | 83% | 1 year |
|
| Gudielines | Class of Recommendation | Level of Evidence | Recommendation |
|---|---|---|---|
| European 2018 | II-a | B | “Percutaneous revascularization of CTOs should be considered in patients with angina resistant to medical therapy or with a large area of documented ischaemia in the territory of the occluded vessel” |
| American 2021 | II-b | B | “In patients with suitable anatomy who have refractory angina on medical therapy, after treatment of non-CTO lesions, the benefit of PCI of a CTO to improve symptoms is uncertain” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamzaraj, K.; Kammerlander, A.; Gyöngyösi, M.; Frey, B.; Distelmaier, K.; Graf, S. Patient Selection and Clinical Indication for Chronic Total Occlusion Revascularization—A Workflow Focusing on Non-Invasive Cardiac Imaging. Life 2023, 13, 4. https://0-doi-org.brum.beds.ac.uk/10.3390/life13010004
Hamzaraj K, Kammerlander A, Gyöngyösi M, Frey B, Distelmaier K, Graf S. Patient Selection and Clinical Indication for Chronic Total Occlusion Revascularization—A Workflow Focusing on Non-Invasive Cardiac Imaging. Life. 2023; 13(1):4. https://0-doi-org.brum.beds.ac.uk/10.3390/life13010004
Chicago/Turabian StyleHamzaraj, Kevin, Andreas Kammerlander, Mariann Gyöngyösi, Bernhard Frey, Klaus Distelmaier, and Senta Graf. 2023. "Patient Selection and Clinical Indication for Chronic Total Occlusion Revascularization—A Workflow Focusing on Non-Invasive Cardiac Imaging" Life 13, no. 1: 4. https://0-doi-org.brum.beds.ac.uk/10.3390/life13010004