
Quantifying Carotid Stenosis: History, Current Applications, Limitations, and Potential: How Imaging Is Changing the Scenario
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Models for Assessing the Degree of Carotid Stenosis
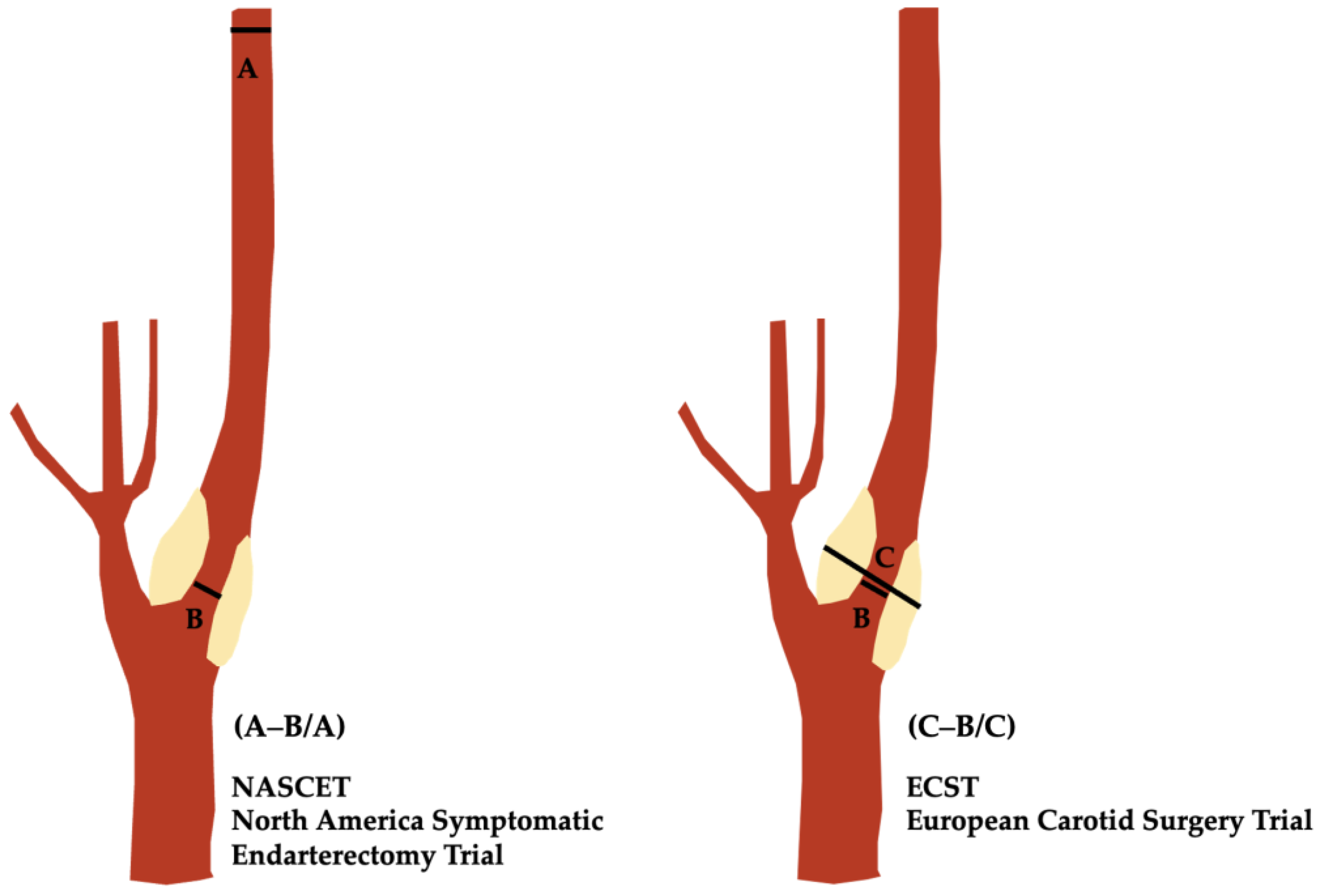
2.1. The NASCET
2.2. The ECST
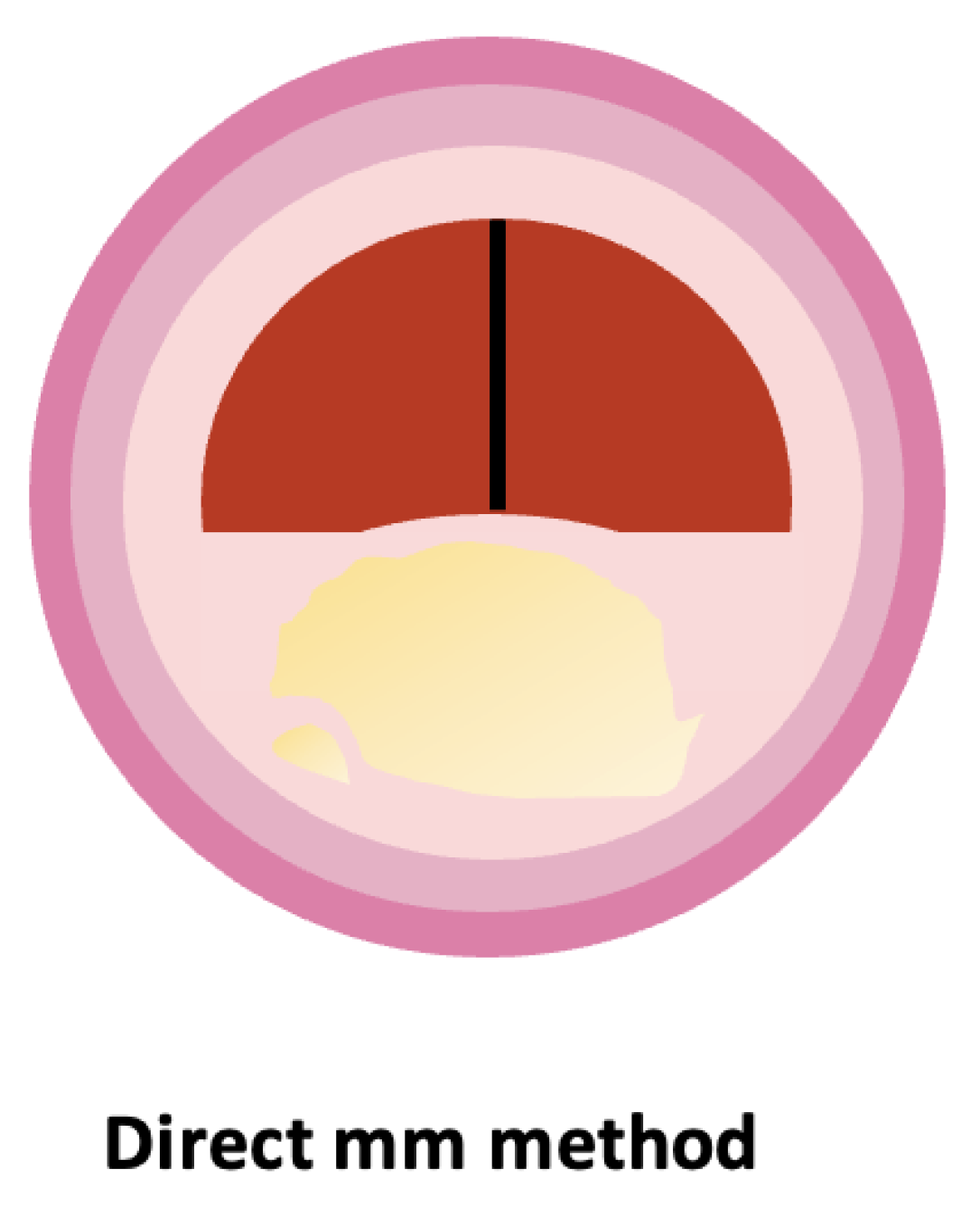
2.3. The Direct mm Measurement
3. Applications
3.1. The Guidelines and Use of NASCET: Endorsement from the Societies
3.2. Ultrasound Application
4. Current Limitations
4.1. Projectional Artifacts and Anatomy
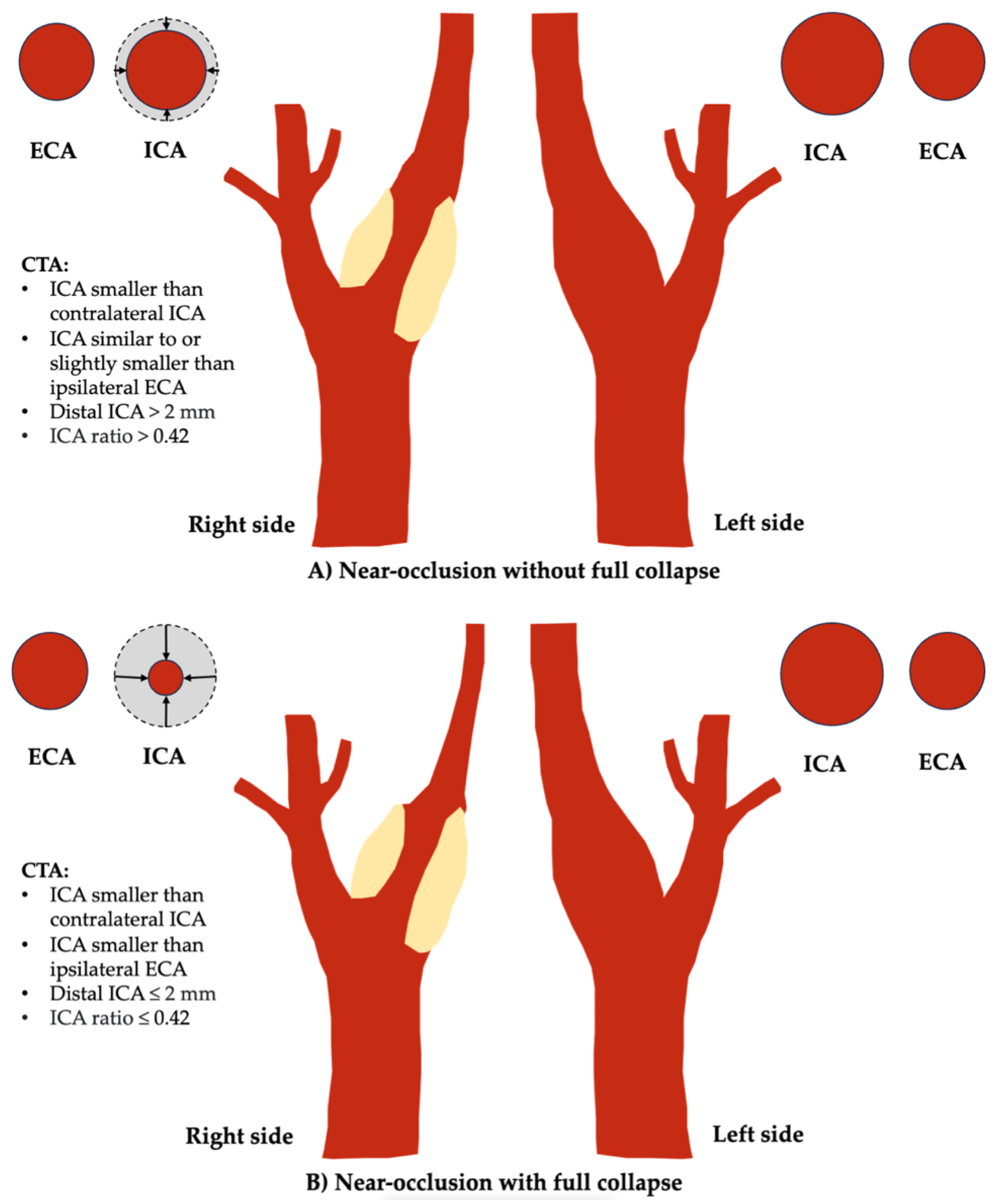
4.2. Near-Occlusion
4.3. The NASCET Pitfalls
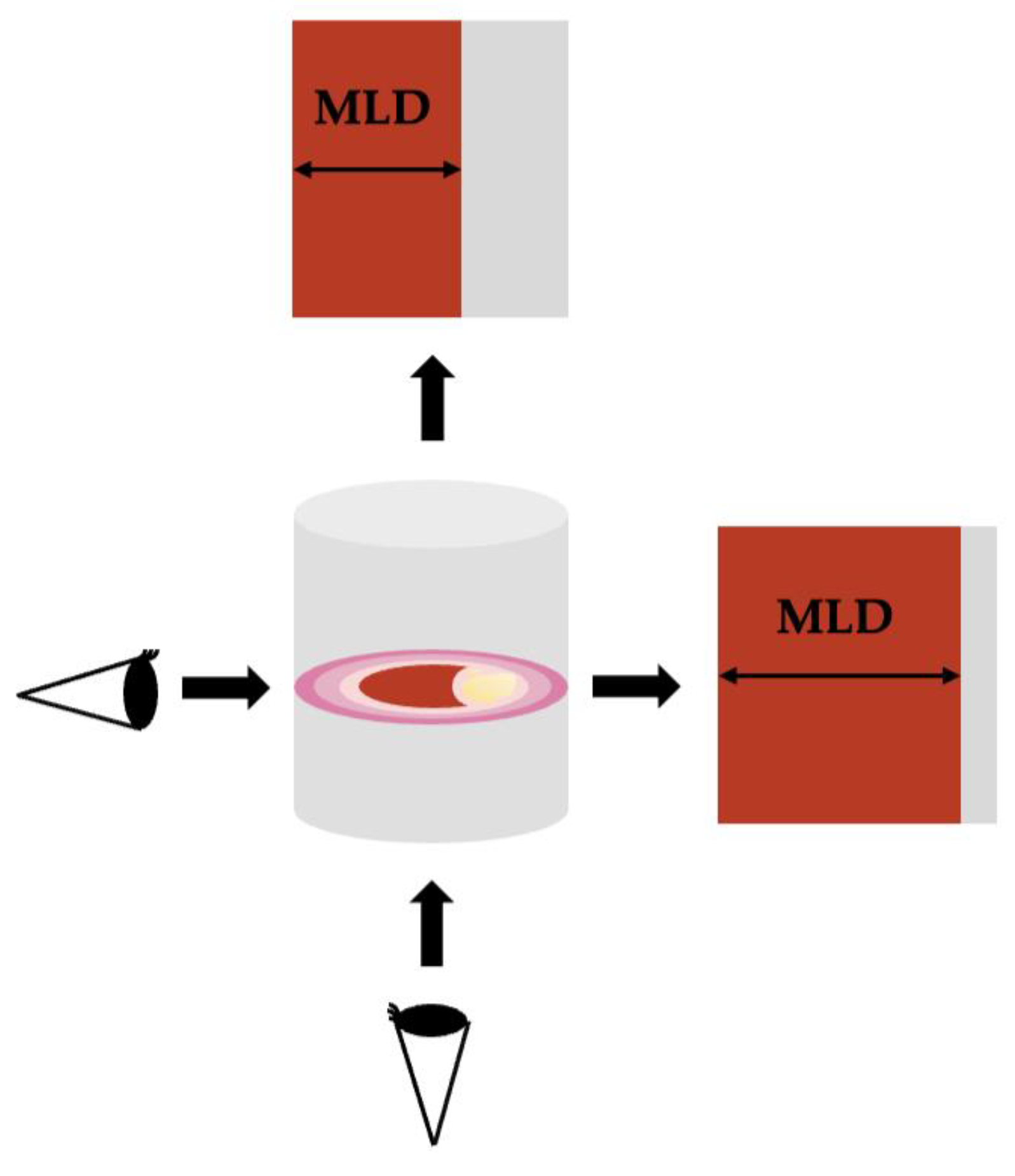
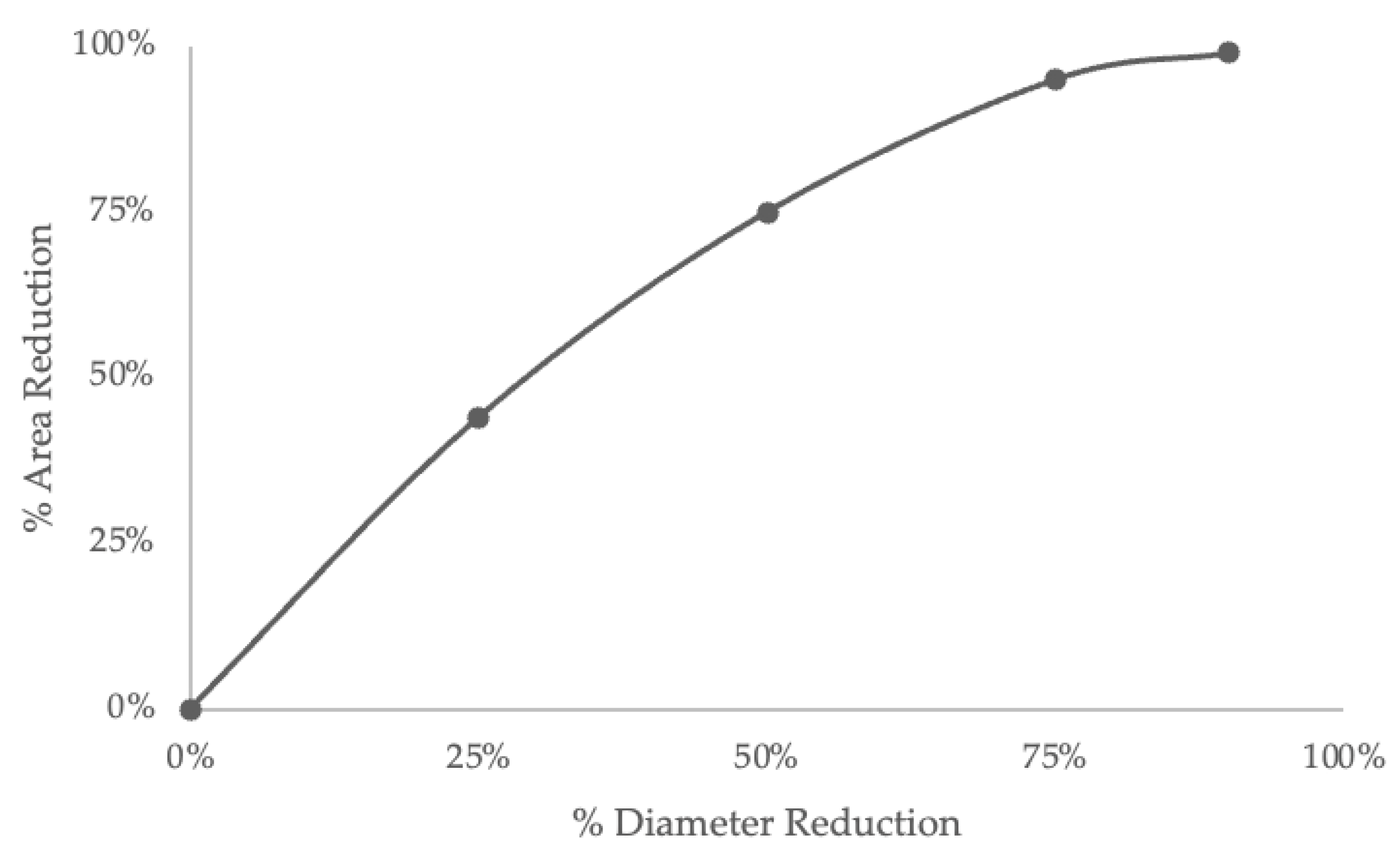
4.4. Diameter and Area
5. Discussion and Potential Future Directions
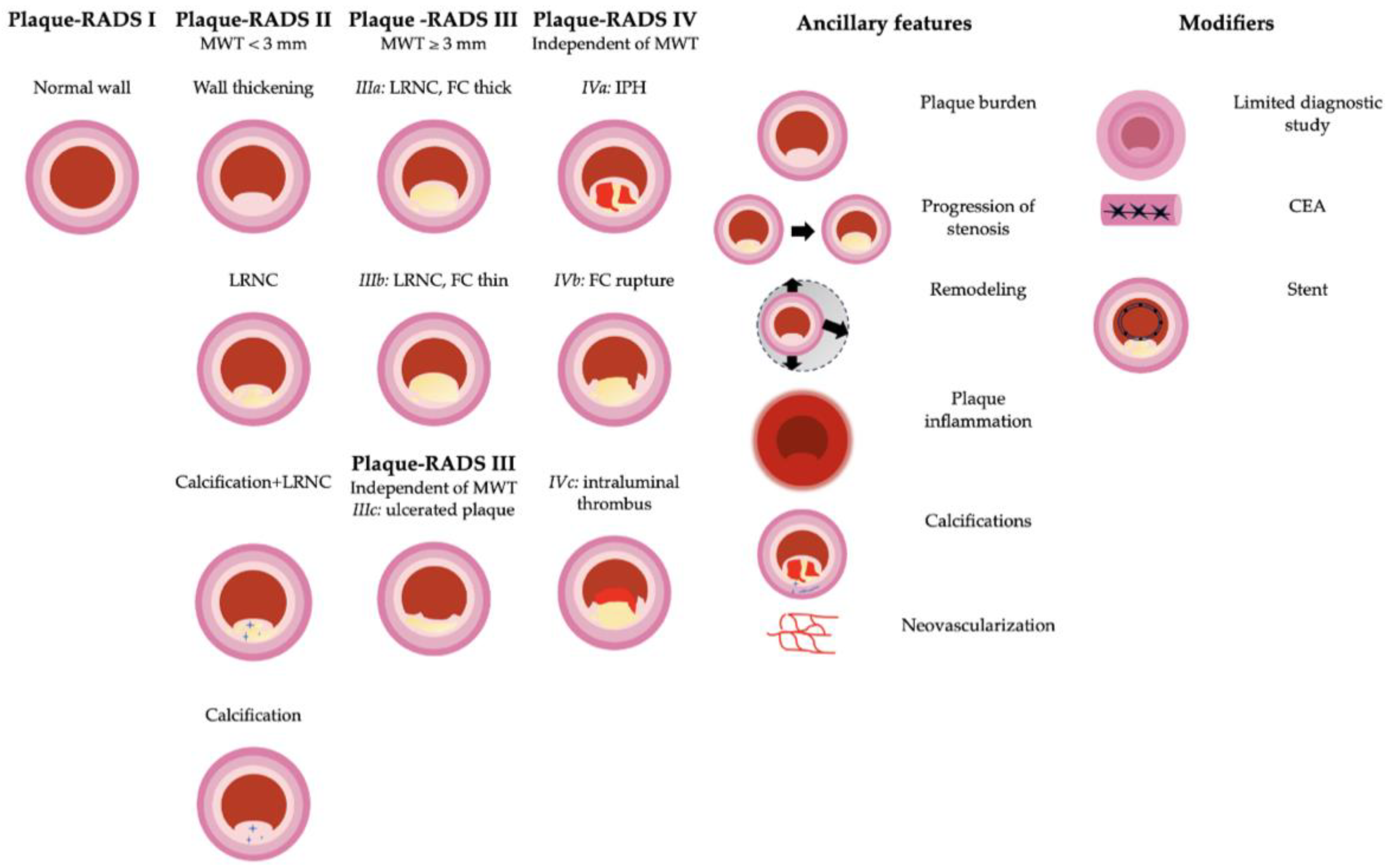
5.1. The Changing Landscape: The Carotid Vulnerable Plaque
- Imaging features: maximum wall thickness (MWT), lipid-rich necrotic core (LRNC), intraplaque hemorrhage (IPH), fibrous cap (FC) rupture, and intraluminal thrombus;
- Ancillary features: plaque inflammation and neovascularization, positive carotid remodeling, plaque burden, progression of stenosis, and carotid plaque calcifications;
- Modifiers: limited diagnostic study (L), stents, and previous CEA.
5.2. Photon-Counting CT (PCCT)
5.3. AI Impact
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hippocrates; Adams, F. The Genuine Works of Hippocrates; William Wood & Co.: New York, NY, USA, 1886. [Google Scholar]
- Robicsek, F.; Roush, T.S.; Cook, J.W.; Reames, M.K. From Hippocrates to Palmaz-Schatz, The History of Carotid Surgery. Eur. J. Vasc. Endovasc. Surg. 2004, 27, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Munster, A.B.; Thapar, A.; Davies, A.H. History of Carotid Stroke. Stroke 2016, 47, e66–e69. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M. Occlusion of the internal carotid artery. Arch. Neurol. Psychiatry 1951, 65, 346. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M. Occlusion of the carotid arteries: Further Experiences. AMA Arch. Neurol. Psychiatry 1954, 72, 187. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.G. The First Carotid Endarterectomy. J. Vasc. Surg. 2014, 60, 1703–1708.e4. [Google Scholar] [CrossRef]
- Pavlicek, W.; Weinstein, M.A.; Modic, M.T.; Buonocore, E.; Duchesneau, P.M. Patient Doses during Digital Subtraction Angiography of the Carotid Arteries: Comparison with Conventional Angiography. Radiology 1982, 145, 683–685. [Google Scholar] [CrossRef]
- Crummy, A.B.; Strother, C.M.; Mistretta, C.A. The History of Digital Subtraction Angiography. J. Vasc. Interv. Radiol. 2018, 29, 1138–1141. [Google Scholar] [CrossRef]
- North American Symptomatic Carotid Endarterectomy Trial Collaborators; Barnett, H.J.M.; Taylor, D.W.; Haynes, R.B.; Sackett, D.L.; Peerless, S.J.; Ferguson, G.G.; Fox, A.J.; Rankin, R.N.; Hachinski, V.C.; et al. Beneficial Effect of Carotid Endarterectomy in Symptomatic Patients with High-Grade Carotid Stenosis. N. Engl. J. Med. 1991, 325, 445–453. [Google Scholar] [CrossRef]
- Ferguson, G.G.; Eliasziw, M.; Barr, H.W.K.; Clagett, G.P.; Barnes, R.W.; Wallace, M.C.; Taylor, D.W.; Haynes, R.B.; Finan, J.W.; Hachinski, V.C.; et al. The North American Symptomatic Carotid Endarterectomy Trial: Surgical Results in 1415 Patients. Stroke 1999, 30, 1751–1758. [Google Scholar] [CrossRef]
- Warlow, C. MRC European Carotid Surgery Trial: Interim Results for Symptomatic Patients with Severe (70–99%) or with Mild (0–29%) Carotid Stenosis. Lancet 1991, 337, 1235–1243. [Google Scholar] [CrossRef]
- Randomised Trial of Endarterectomy for Recently Symptomatic Carotid Stenosis: Final Results of the MRC European Carotid Surgery Trial (ECST). Lancet 1998, 351, 1379–1387. [CrossRef]
- Fields, W.S.; Lemak, N.A. Joint Study of Extracranial Arterial Occlusion. X. Internal Carotid Artery Occlusion. JAMA 1976, 235, 2734–2738. [Google Scholar] [CrossRef] [PubMed]
- Naylor, A.R.; Rothwell, P.M.; Bell, P.R.F. Overview of the Principal Results and Secondary Analyses from the European and North American Randomised Trials of Endarterectomy for Symptomatic Carotid Stenosis. Eur. J. Vasc. Endovasc. Surg. 2003, 26, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Barnett, H.J.M.; Taylor, D.W.; Eliasziw, M.; Fox, A.J.; Ferguson, G.G.; Haynes, R.B.; Rankin, R.N.; Clagett, G.P.; Hachinski, V.C.; Sackett, D.L.; et al. Benefit of Carotid Endarterectomy in Patients with Symptomatic Moderate or Severe Stenosis. N. Engl. J. Med. 1998, 339, 1415–1425. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, P.M.; Gibson, R.J.; Slattery, J.; Warlow, C.P. Prognostic Value and Reproducibility of Measurements of Carotid Stenosis. A Comparison of Three Methods on 1001 Angiograms. European Carotid Surgery Trialists’ Collaborative Group. Stroke 1994, 25, 2440–2444. [Google Scholar] [CrossRef] [PubMed]
- Lell, M.M.; Anders, K.; Uder, M.; Klotz, E.; Ditt, H.; Vega-Higuera, F.; Boskamp, T.; Bautz, W.A.; Tomandl, B.F. New Techniques in CT Angiography. RadioGraphics 2006, 26, S45–S62. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, E.S.; Walters, T.D.; Symons, S.P.; Fox, A.J. Quantification of Carotid Stenosis on CT Angiography. AJNR Am. J. Neuroradiol. 2006, 27, 13–19. [Google Scholar]
- Bartlett, E.S.; Walters, T.D.; Symons, S.P.; Fox, A.J. Carotid Stenosis Index Revisited With Direct CT Angiography Measurement of Carotid Arteries to Quantify Carotid Stenosis. Stroke 2007, 38, 286–291. [Google Scholar] [CrossRef]
- Bartlett, E.S.; Symons, S.P.; Fox, A.J. Correlation of Carotid Stenosis Diameter and Cross-Sectional Areas with CT Angiography. AJNR Am. J. Neuroradiol. 2006, 27, 638–642. [Google Scholar]
- Rothwell, P.M.; Eliasziw, M.; Gutnikov, S.A.; Fox, A.J.; Taylor, D.W.; Mayberg, M.R.; Warlow, C.P.; Barnett, H.J.M. Analysis of Pooled Data from the Randomised Controlled Trials of Endarterectomy for Symptomatic Carotid Stenosis. Lancet 2003, 361, 107–116. [Google Scholar] [CrossRef]
- Staikov, I.N.; Arnold, M.; Mattle, H.; Remonda, L.; Sturzenegger, M.; Baumgartner, R.W.; Schroth, G. Comparison of the ECST, CC, and NASCET Grading Methods and Ultrasound for Assessing Carotid Stenosis. J. Neurol. 2000, 247, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Carnicelli, A.P.; Stone, J.J.; Doyle, A.; Chowdhry, A.K.; Mix, D.; Ellis, J.; Gillespie, D.L.; Chandra, A. Cross-Sectional Area for the Calculation of Carotid Artery Stenosis on Computed Tomographic Angiography. J. Vasc. Surg. 2013, 58, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Abbott, A.L.; Paraskevas, K.I.; Kakkos, S.K.; Golledge, J.; Eckstein, H.-H.; Diaz-Sandoval, L.J.; Cao, L.; Fu, Q.; Wijeratne, T.; Leung, T.W.; et al. Systematic Review of Guidelines for the Management of Asymptomatic and Symptomatic Carotid Stenosis. Stroke 2015, 46, 3288–3301. [Google Scholar] [CrossRef] [PubMed]
- Saba, L.; Loewe, C.; Weikert, T.; Williams, M.C.; Galea, N.; Budde, R.P.J.; Vliegenthart, R.; Velthuis, B.K.; Francone, M.; Bremerich, J.; et al. State-of-the-Art CT and MR Imaging and Assessment of Atherosclerotic Carotid Artery Disease: The Reporting—A Consensus Document by the European Society of Cardiovascular Radiology (ESCR). Eur. Radiol. 2022, 33, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Tekieli, L.; Mazurek, A.; Dzierwa, K.; Stefaniak, J.; Kablak-Ziembicka, A.; Knapik, M.; Moczulski, Z.; Banys, R.P.; Urbanczyk-Zawadzka, M.; Dabrowski, W.; et al. Misclassification of Carotid Stenosis Severity with Area Stenosis-Based Evaluation by Computed Tomography Angiography: Impact on Erroneous Indication to Revascularization or Patient (Lesion) Migration to a Higher Guideline Recommendation Class as per ESC/ESVS/ESO/SVS and CMS-FDA Thresholds. Adv. Interv. Cardiol. 2022, 18, 500–513. [Google Scholar] [CrossRef]
- Carpenter, J.P.; Lexa, F.J.; Davis, J.T. Determination of Duplex Doppler Ultrasound Criteria Appropriate to the North American Symptomatic Carotid Endarterectomy Trial. Stroke 1996, 27, 695–699. [Google Scholar] [CrossRef]
- Beebe, H.G.; Salles-Cunha, S.X.; Scissons, R.P.; Dosick, S.M.; Whalen, R.C.; Gale, S.S.; Seiwert, A.J. Carotid Arterial Ultrasound Scan Imaging: A Direct Approach to Stenosis Measurement. J. Vasc. Surg. 1999, 29, 838–844. [Google Scholar] [CrossRef]
- Ota, H.; Takase, K.; Rikimaru, H.; Tsuboi, M.; Yamada, T.; Sato, A.; Higano, S.; Ishibashi, T.; Takahashi, S. Quantitative Vascular Measurements in Arterial Occlusive Disease. RadioGraphics 2005, 25, 1141–1158. [Google Scholar] [CrossRef]
- Grant, E.G.; Benson, C.B.; Moneta, G.L.; Alexandrov, A.V.; Baker, J.D.; Bluth, E.I.; Carroll, B.A.; Eliasziw, M.; Gocke, J.; Hertzberg, B.S.; et al. Carotid Artery Stenosis: Gray-Scale and Doppler US Diagnosis—Society of Radiologists in Ultrasound Consensus Conference. Radiology 2003, 229, 340–346. [Google Scholar] [CrossRef]
- Widder, B.; von Reutern, G.M.; Neuerburg-Heusler, D. Morphologic and Doppler sonographic criteria for determining the degree of stenosis of the internal carotid artery. Ultraschall Med. 1986, 7, 70–75. [Google Scholar] [CrossRef]
- Arning, C.; Widder, B.; von Reutern, G.M.; Stiegler, H.; Görtler, M. Revision of DEGUM ultrasound criteria for grading internal carotid artery stenoses and transfer to NASCET measurement. Ultraschall Med. 2010, 31, 251–257. [Google Scholar] [CrossRef] [PubMed]
- von Reutern, G.-M.; Goertler, M.-W.; Bornstein, N.M.; Del Sette, M.; Evans, D.H.; Hetzel, A.; Kaps, M.; Perren, F.; Razumovky, A.; von Reutern, M.; et al. Grading Carotid Stenosis Using Ultrasonic Methods. Stroke 2012, 43, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Mozzini, C.; Roscia, G.; Casadei, A.; Cominacini, L. Searching the Perfect Ultrasonic Classification in Assessing Carotid Artery Stenosis: Comparison and Remarks upon the Existing Ultrasound Criteria. J. Ultrasound 2016, 19, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Moneta, G.L.; Edwards, J.M.; Chitwood, R.W.; Taylor, L.M.; Lee, R.W.; Cummings, C.A.; Porter, J.M. Correlation of North American Symptomatic Carotid Endarterectomy Trial (NASCET) Angiographic Definition of 70% to 99% Internal Carotid Artery Stenosis with Duplex Scanning. J. Vasc. Surg. 1993, 17, 152–157, discussion 157–159. [Google Scholar] [CrossRef] [PubMed]
- Hwang, C.-S.; Liao, K.-M.; Lee, J.-H.; Tegeler, C.H. Measurement of Carotid Stenosis: Comparisons Between Duplex and Different Angiographic Grading Methods. J. Neuroimaging 2003, 13, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Neale, M.L.; Chambers, J.L.; Kelly, A.T.; Connard, S.; Lawton, M.A.; Roche, J.; Appleberg, M. Reappraisal of Duplex Criteria to Assess Significant Carotid Stenosis with Special Reference to Reports from the North American Symptomatic Carotid Endarterectomy Trial and the European Carotid Surgery Trial. J. Vasc. Surg. 1994, 20, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Hathout, G.M.; Fink, J.R.; El-Saden, S.M.; Grant, E.G. Sonographic NASCET Index: A New Doppler Parameter for Assessment of Internal Carotid Artery Stenosis. AJNR Am. J. Neuroradiol. 2005, 26, 68–75. [Google Scholar]
- Henderson, R.D.; Steinman, D.A.; Eliasziw, M.; Barnett, H.J.M. Effect of Contralateral Carotid Artery Stenosis on Carotid Ultrasound Velocity Measurements. Stroke 2000, 31, 2636–2640. [Google Scholar] [CrossRef]
- Bluth, E.I.; Stavros, A.T.; Marich, K.W.; Wetzner, S.M.; Aufrichtig, D.; Baker, J.D. Carotid Duplex Sonography: A Multicenter Recommendation for Standardized Imaging and Doppler Criteria. Radiographics 1988, 8, 487–506. [Google Scholar] [CrossRef]
- Arnold, J.A.C.; Modaresi, K.B.; Thomas, N.; Taylor, P.R.; Padayachee, T.S. Carotid Plaque Characterization by Duplex Scanning: Observer Error May Undermine Current Clinical Trials. Stroke 1999, 30, 61–65. [Google Scholar] [CrossRef]
- Elgersma, O.E.H.; Buijs, P.C.; Wüst, A.F.J.; Van Der Graaf, Y.; Eikelboom, B.C.; Mali, W.P.T.M. Maximum Internal Carotid Arterial Stenosis: Assessment with Rotational Angiography versus Conventional Intraarterial Digital Subtraction Angiography. Radiology 1999, 213, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.M.; Saloner, D.; Reilly, L.M.; Bowersox, J.C.; Murray, S.P.; Anderson, C.M.; Gooding, G.A.W.; Rapp, J.H. Assessment of Carotid Artery Stenosis by Ultrasonography, Conventional Angiography, and Magnetic Resonance Angiography: Correlation with Ex Vivo Measurement of Plaque Stenosis. J. Vasc. Surg. 1995, 21, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Alexandrov, A.V.; Bladin, C.F.; Maggisano, R.; Norris, J.W. Measuring Carotid Stenosis. Time for a Reappraisal. Stroke 1993, 24, 1292–1296. [Google Scholar] [CrossRef] [PubMed]
- Bladin, C.F.; Alexandrov, A.V.; Murphy, J.; Maggisano, R.; Norris, J.W. Carotid Stenosis Index. A New Method of Measuring Internal Carotid Artery Stenosis. Stroke 1995, 26, 230–234. [Google Scholar] [CrossRef]
- Saba, L.; Loewe, C.; Weikert, T.; Williams, M.C.; Galea, N.; Budde, R.P.J.; Vliegenthart, R.; Velthuis, B.K.; Francone, M.; Bremerich, J.; et al. State-of-the-Art CT and MR Imaging and Assessment of Atherosclerotic Carotid Artery Disease: Standardization of Scanning Protocols and Measurements—A Consensus Document by the European Society of Cardiovascular Radiology (ESCR). Eur. Radiol. 2022, 33, 1063–1087. [Google Scholar] [CrossRef]
- Naylor, R.; Rantner, B.; Ancetti, S.; De Borst, G.J.; De Carlo, M.; Halliday, A.; Kakkos, S.K.; Markus, H.S.; McCabe, D.J.H.; Sillesen, H.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on the Management of Atherosclerotic Carotid and Vertebral Artery Disease. Eur. J. Vasc. Endovasc. Surg. 2023, 65, 7–111. [Google Scholar] [CrossRef]
- Fox, A.J.; Eliasziw, M.; Rothwell, P.M.; Schmidt, M.H.; Warlow, C.P.; Barnett, H.J.M. Identification, Prognosis, and Management of Patients with Carotid Artery near Occlusion. AJNR Am. J. Neuroradiol. 2005, 26, 2086–2094. [Google Scholar]
- Johansson, E.; Fox, A.J. Carotid Near-Occlusion: A Comprehensive Review, Part 1—Definition, Terminology, and Diagnosis. AJNR Am. J. Neuroradiol. 2016, 37, 2–10. [Google Scholar] [CrossRef]
- Johansson, E.; Fox, A.J. Carotid Near-Occlusion: A Comprehensive Review, Part 2—Prognosis and Treatment, Pathophysiology, Confusions, and Areas for Improvement. AJNR Am. J. Neuroradiol. 2016, 37, 200–204. [Google Scholar] [CrossRef]
- Holmgren, M.; Henze, A.; Wåhlin, A.; Eklund, A.; Fox, A.J.; Johansson, E. Diagnostic Separation of Conventional ≥50% Carotid Stenosis and Near-Occlusion with Phase-Contrast MRI. Eur. Stroke J. 2023; in press. [Google Scholar] [CrossRef]
- Meershoek, A.J.A.; Vries, E.E.; Veen, D.; Ruijter, H.M.; Borst, G.J.; Garcia-Pastor, A.; Gonzalez, A.; Johansson, E.; Matsuda, Y.; Ogata, T.; et al. Meta-Analysis of the Outcomes of Treatment of Internal Carotid Artery near Occlusion. Br. J. Surg. 2019, 106, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Johansson, E.; Gu, T.; Fox, A.J. Defining Carotid Near-Occlusion with Full Collapse: A Pooled Analysis. Neuroradiology 2022, 64, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Kellomäki, E.; Gu, T.; Fox, A.J.; Johansson, E. Symptomatic and Asymptomatic Carotid Near-Occlusions Have Very Similar Angiographic Appearance on CT-Angiography. Neuroradiology 2022, 64, 2203–2206. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, E.S.; Walters, T.D.; Symons, S.P.; Fox, A.J. Diagnosing Carotid Stenosis Near-Occlusion by Using CT Angiography. AJNR Am. J. Neuroradiol. 2006, 27, 632–637. [Google Scholar] [PubMed]
- Manrique-Zegarra, M.; García-Pastor, A.; Castro-Reyes, E.; Guzmán-De-Villoria, J.A.; Herrera, I.H.; Morro, I.G.; Diéguez, M.D.V.; Gil, F.F.; Cantero, J.G.; Lorente, J.S. CT Angiography for Diagnosis of Carotid Near-Occlusion: A Digital Subtraction Angiography Validation Study. Neuroradiology 2022, 64, 1729–1735. [Google Scholar] [CrossRef] [PubMed]
- Johansson, E.; Aviv, R.I.; Fox, A.J. Atherosclerotic ICA Stenosis Coinciding with ICA Asymmetry Associated with Circle of Willis Variations Can Mimic Near-Occlusion. Neuroradiology 2020, 62, 101–104. [Google Scholar] [CrossRef]
- Mansour, M.A.; Mattos, M.A.; Hood, D.B.; Hodgson, K.J.; Barkmeier, L.D.; Ramsey, D.E.; Sumner, D.S. Detection of Total Occlusion, String Sign, and Preocclusive Stenosis of the Internal Carotid Artery by Color-Flow Duplex Scanning. Am. J. Surg. 1995, 170, 154–158. [Google Scholar] [CrossRef]
- Hetzel, A.; Eckenweber, B.; Trummer, B.; Wernz, M.; Schumacher, M.; von Reutern, G. Colour-Coded Duplex Sonography of Preocclusive Carotid Stenoses. Eur. J. Ultrasound 1998, 8, 183–191. [Google Scholar] [CrossRef]
- El-Saden, S.M.; Grant, E.G.; Hathout, G.M.; Zimmerman, P.T.; Cohen, S.N.; Baker, J.D. Imaging of the Internal Carotid Artery: The Dilemma of Total versus near Total Occlusion. Radiology 2001, 221, 301–308. [Google Scholar] [CrossRef]
- Palacios-Mendoza, M.A.; García-Pastor, A.; Gil-Núñez, A.; Ramírez-Moreno, J.M.; González-Nafría, N.; Moniche, F.; Portilla-Cuenca, J.C.; Fuentes, B.; Gamero-García, M.A.; Alonso De Leciñana, M.; et al. Ultrasonographic and Hemodynamic Characteristics of Patients with Symptomatic Carotid Near-Occlusion: Results from a Multicenter Registry Study. Neuroradiology 2021, 63, 705–711. [Google Scholar] [CrossRef]
- Johansson, E.; Vanoli, D.; Bråten-Johansson, I.; Law, L.; Aviv, R.I.; Fox, A.J. Near-Occlusion Is Difficult to Diagnose with Common Carotid Ultrasound Methods. Neuroradiology 2021, 63, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Johansson, E.; Benhabib, H.; Herod, W.; Hopyan, J.; Machnowska, M.; Maggisano, R.; Aviv, R.; Fox, A.J. Carotid Near-Occlusion Can Be Identified with Ultrasound by Low Flow Velocity Distal to the Stenosis. Acta Radiol. 2019, 60, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Johansson, E.; Fox, A.J. Near-Occlusion Is a Common Variant of Carotid Stenosis: Study and Systematic Review. Can. J. Neurol. Sci. 2022, 49, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Johansson, E.; Gu, T.; Aviv, R.I.; Fox, A.J. Carotid Near-Occlusion Is Often Overlooked When CT Angiography Is Assessed in Routine Practice. Eur. Radiol. 2020, 30, 2543–2551. [Google Scholar] [CrossRef] [PubMed]
- Johansson, E.; Holmgren, M.; Henze, A.; Fox, A.J. Diagnosing Carotid Near-Occlusion Is a Difficult Task—But It Might Get Easier. Neuroradiology 2022, 64, 1709–1714. [Google Scholar] [CrossRef] [PubMed]
- Fox, A.J. How to Measure Carotid Stenosis. Radiology 1993, 186, 316–318. [Google Scholar] [CrossRef]
- Fox, A.J.; Symons, S.P.; Aviv, R.I.; Howard, P.; Yeung, R.; Bartlett, E.S. Falsely Claiming Use of NASCET Percentage Stenosis Method. Radiology 2009, 253, 574–575. [Google Scholar] [CrossRef]
- Eliasziw, M.; Smith, R.F.; Singh, N.; Holdsworth, D.W.; Fox, A.J.; Barnett, H.J. Further Comments on the Measurement of Carotid Stenosis from Angiograms. North American Symptomatic Carotid Endarterectomy Trial (NASCET) Group. Stroke 1994, 25, 2445–2449. [Google Scholar] [CrossRef]
- Gagne, P.J.; Matchett, J.; MacFarland, D.; Hauer-Jensen, M.; Barone, G.W.; Eidt, J.F.; Barnes, R.W. Can the NASCET Technique for Measuring Carotid Stenosis Be Reliably Applied Outside the Trial? J. Vasc. Surg. 1996, 24, 449–456. [Google Scholar] [CrossRef]
- Barnett, H.J.; Barnes, R.W.; Clagett, G.P.; Ferguson, G.G.; Robertson, J.T.; Walker, P.M. Symptomatic Carotid Artery Stenosis: A Solvable Problem. North American Symptomatic Carotid Endarterectomy Trial. Stroke 1992, 23, 1048–1053. [Google Scholar] [CrossRef]
- Ranval, T.J.; Bailey, T.; Solis, M.E.; MacDonald, C.; Wallace, B.; Harshfield, D.; Barnes, R.W. Overestimation of Carotid Stenosis: Implications for Carotid Endarterectomy (Abstract). Stroke 1992, 23, 142. [Google Scholar]
- LaMuraglia, G.M.; Brewster, D.C.; Moncure, A.C.; Dorer, D.J.; Stoner, M.C.; Trehan, S.K.; Drummond, E.C.; Abbott, W.M.; Cambria, R.P. Carotid Endarterectomy at the Millennium: What Interventional Therapy Must Match. Ann. Surg. 2004, 240, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Calvet, D.; Mas, J.-L. Recent Advances in Carotid Angioplasty and Stenting. Int. J. Stroke 2016, 11, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Bucek, R.A.; Puchner, S.; Haumer, M.; Reiter, M.; Minar, E.; Lammer, J. CTA Quantification of Internal Carotid Artery Stenosis: Application of Luminal Area vs. Luminal Diameter Measurements and Assessment of Inter-observer Variability. J. Neuroimaging 2007, 17, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Samarzija, K.; Milosevic, P.; Jurjevic, Z.; Erdeljac, E. Grading of Carotid Artery Stenosis with Computed Tomography Angiography: Whether to Use the Narrowest Diameter or the Cross-Sectional Area. Insights Imaging 2018, 9, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Qin, H.; Liu, J.; Wu, B.; Cheng, Z.; Jiang, Y.; Liu, L.; Jing, L.; Leng, X.; Jing, J.; et al. Characteristics of Wall Shear Stress and Pressure of Intracranial Atherosclerosis Analyzed by a Computational Fluid Dynamics Model: A Pilot Study. Front. Neurol. 2020, 10, 1372. [Google Scholar] [CrossRef] [PubMed]
- Strecker, C.; Krafft, A.J.; Kaufhold, L.; Hüllebrandt, M.; Treppner, M.; Ludwig, U.; Köber, G.; Hennemuth, A.; Hennig, J.; Harloff, A. Carotid Geometry and Wall Shear Stress Independently Predict Increased Wall Thickness—A Longitudinal 3D MRI Study in High-Risk Patients. Front. Cardiovasc. Med. 2021, 8, 723860. [Google Scholar] [CrossRef] [PubMed]
- Caro, C.G. Discovery of the Role of Wall Shear in Atherosclerosis. ATVB 2009, 29, 158–161. [Google Scholar] [CrossRef]
- Walker, M.D. Endarterectomy for Asymptomatic Carotid Artery Stenosis. JAMA 1995, 273, 1421. [Google Scholar] [CrossRef]
- Halliday, A.; Harrison, M.; Hayter, E.; Kong, X.; Mansfield, A.; Marro, J.; Pan, H.; Peto, R.; Potter, J.; Rahimi, K.; et al. 10-Year Stroke Prevention after Successful Carotid Endarterectomy for Asymptomatic Stenosis (ACST-1): A Multicentre Randomised Trial. Lancet 2010, 376, 1074–1084. [Google Scholar] [CrossRef]
- Brott, T.G.; Halperin, J.L.; Abbara, S.; Bacharach, J.M.; Barr, J.D.; Bush, R.L.; Cates, C.U.; Creager, M.A.; Fowler, S.B.; Friday, G.; et al. 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery. Circulation 2011, 124, 489–532. [Google Scholar] [CrossRef] [PubMed]
- Abbott, A.L. Extra-Cranial Carotid Artery Stenosis: An Objective Analysis of the Available Evidence. Front. Neurol. 2022, 13, 739999. [Google Scholar] [CrossRef] [PubMed]
- Shahidi, S.; Owen-Falkenberg, A.; Hjerpsted, U.; Rai, A.; Ellemann, K. Urgent Best Medical Therapy May Obviate the Need for Urgent Surgery in Patients With Symptomatic Carotid Stenosis. Stroke 2013, 44, 2220–2225. [Google Scholar] [CrossRef] [PubMed]
- Shahidi, S.; Owen-Falkenberg, A.; Gottschalksen, B.; Ellemann, K. Risk of Early Recurrent Stroke in Symptomatic Carotid Stenosis after Best Medical Therapy and before Endarterectomy. Int. J. Stroke 2016, 11, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Venermo, M.; Wang, G.; Sedrakyan, A.; Mao, J.; Eldrup, N.; DeMartino, R.; Mani, K.; Altreuther, M.; Beiles, B.; Menyhei, G.; et al. Editor’s Choice—Carotid Stenosis Treatment: Variation in International Practice Patterns. Eur. J. Vasc. Endovasc. Surg. 2017, 53, 511–519. [Google Scholar] [CrossRef]
- Fisch, U.; Von Felten, S.; Wiencierz, A.; Jansen, O.; Howard, G.; Hendrikse, J.; Halliday, A.; Fraedrich, G.; Eckstein, H.-H.; Calvet, D.; et al. Editor’s Choice—Risk of Stroke before Revascularisation in Patients with Symptomatic Carotid Stenosis: A Pooled Analysis of Randomised Controlled Trials. Eur. J. Vasc. Endovasc. Surg. 2021, 61, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Abbott, A.L. Medical (Nonsurgical) Intervention Alone Is Now Best for Prevention of Stroke Associated With Asymptomatic Severe Carotid Stenosis: Results of a Systematic Review and Analysis. Stroke 2009, 40, E573–E583. [Google Scholar] [CrossRef]
- Mott, M.; Koroshetz, W.; Wright, C.B. CREST-2: Identifying the Best Method of Stroke Prevention for Carotid Artery Stenosis: National Institute of Neurological Disorders and Stroke Organizational Update. Stroke 2017, 48, e130–e131. [Google Scholar] [CrossRef]
- Cheng, S.F.; Van Velzen, T.J.; Gregson, J.; Richards, T.; Jäger, H.R.; Simister, R.; Kooi, M.E.; De Borst, G.J.; Pizzini, F.B.; Nederkoorn, P.J.; et al. The 2nd European Carotid Surgery Trial (ECST-2): Rationale and Protocol for a Randomised Clinical Trial Comparing Immediate Revascularisation versus Optimised Medical Therapy Alone in Patients with Symptomatic and Asymptomatic Carotid Stenosis at Low to Intermediate Risk of Stroke. Trials 2022, 23, 606. [Google Scholar] [CrossRef]
- Kopczak, A.; Schindler, A.; Bayer-Karpinska, A.; Koch, M.L.; Sepp, D.; Zeller, J.; Strecker, C.; Hempel, J.-M.; Yuan, C.; Malik, R.; et al. Complicated Carotid Artery Plaques as a Cause of Cryptogenic Stroke. J. Am. Coll. Cardiol. 2020, 76, 2212–2222. [Google Scholar] [CrossRef]
- Kopczak, A.; Schindler, A.; Sepp, D.; Bayer-Karpinska, A.; Malik, R.; Koch, M.L.; Zeller, J.; Strecker, C.; Janowitz, D.; Wollenweber, F.A.; et al. Complicated Carotid Artery Plaques and Risk of Recurrent Ischemic Stroke or TIA. J. Am. Coll. Cardiol. 2022, 79, 2189–2199. [Google Scholar] [CrossRef] [PubMed]
- Kakkos, S.K.; Griffin, M.B.; Nicolaides, A.N.; Kyriacou, E.; Sabetai, M.M.; Tegos, T.; Makris, G.C.; Thomas, D.J.; Geroulakos, G. The Size of Juxtaluminal Hypoechoic Area in Ultrasound Images of Asymptomatic Carotid Plaques Predicts the Occurrence of Stroke. J. Vasc. Surg. 2013, 57, 609–618.e1. [Google Scholar] [CrossRef] [PubMed]
- Larson, A.; Nardi, V.; Brinjikji, W.; Benson, J.; Lanzino, G.; Savastano, L. Endarterectomy for Symptomatic Non-Stenotic Carotids: A Systematic Review and Descriptive Analysis. Stroke Vasc. Neurol. 2022, 7, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Puig, N.; Solé, A.; Aguilera-Simon, A.; Griñán, R.; Rotllan, N.; Camps-Renom, P.; Benitez, S. Novel Therapeutic Approaches to Prevent Atherothrombotic Ischemic Stroke in Patients with Carotid Atherosclerosis. IJMS 2023, 24, 14325. [Google Scholar] [CrossRef] [PubMed]
- Stary, H.C.; Chandler, A.B.; Dinsmore, R.E.; Fuster, V.; Glagov, S.; Insull, W.; Rosenfeld, M.E.; Schwartz, C.J.; Wagner, W.D.; Wissler, R.W. A Definition of Advanced Types of Atherosclerotic Lesions and a Histological Classification of Atherosclerosis. A Report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Circulation 1995, 92, 1355–1374. [Google Scholar] [CrossRef] [PubMed]
- Virmani, R.; Kolodgie, F.D.; Burke, A.P.; Farb, A.; Schwartz, S.M. Lessons from Sudden Coronary Death: A Comprehensive Morphological Classification Scheme for Atherosclerotic Lesions. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1262–1275. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.-M.; Hatsukami, T.S.; Ferguson, M.S.; Small, R.; Polissar, N.L.; Yuan, C. Classification of Human Carotid Atherosclerotic Lesions With In Vivo Multicontrast Magnetic Resonance Imaging. Circulation 2002, 106, 1368–1373. [Google Scholar] [CrossRef]
- Saba, L.; Cau, R.; Murgia, A.; Nicolaides, A.N.; Wintermark, M.; Castillo, M.; Staub, D.; Kakkos, S.; Yang, Q.; Paraskevas, K.I.; et al. Carotid Plaque-RADS, a Novel Stroke Risk Classification System. JACC Cardiovasc. Imaging 2023, S1936-878X(23)00431-X. [Google Scholar] [CrossRef]
- McNally, J.S.; McLaughlin, M.S.; Hinckley, P.J.; Treiman, S.M.; Stoddard, G.J.; Parker, D.L.; Treiman, G.S. Intraluminal Thrombus, Intraplaque Hemorrhage, Plaque Thickness, and Current Smoking Optimally Predict Carotid Stroke. Stroke 2015, 46, 84–90. [Google Scholar] [CrossRef]
- Gupta, A.; Baradaran, H.; Schweitzer, A.D.; Kamel, H.; Pandya, A.; Delgado, D.; Dunning, A.; Mushlin, A.I.; Sanelli, P.C. Carotid Plaque MRI and Stroke Risk: A Systematic Review and Meta-Analysis. Stroke 2013, 44, 3071–3077. [Google Scholar] [CrossRef]
- Moody, A.R.; Allder, S.; Lennox, G.; Gladman, J.; Fentem, P. Direct Magnetic Resonance Imaging of Carotid Artery Thrombus in Acute Stroke. Lancet 1999, 353, 122–123. [Google Scholar] [CrossRef] [PubMed]
- Moody, A.R.; Murphy, R.E.; Morgan, P.S.; Martel, A.L.; Delay, G.S.; Allder, S.; MacSweeney, S.T.; Tennant, W.G.; Gladman, J.; Lowe, J.; et al. Characterization of Complicated Carotid Plaque With Magnetic Resonance Direct Thrombus Imaging in Patients With Cerebral Ischemia. Circulation 2003, 107, 3047–3052. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Mitsumori, L.M.; Ferguson, M.S.; Polissar, N.L.; Echelard, D.; Ortiz, G.; Small, R.; Davies, J.W.; Kerwin, W.S.; Hatsukami, T.S. In Vivo Accuracy of Multispectral Magnetic Resonance Imaging for Identifying Lipid-Rich Necrotic Cores and Intraplaque Hemorrhage in Advanced Human Carotid Plaques. Circulation 2001, 104, 2051–2056. [Google Scholar] [CrossRef] [PubMed]
- Van Dam-Nolen, D.H.K.; Truijman, M.T.B.; Van Der Kolk, A.G.; Liem, M.I.; Schreuder, F.H.B.M.; Boersma, E.; Daemen, M.J.A.P.; Mess, W.H.; Van Oostenbrugge, R.J.; Van Der Steen, A.F.W.; et al. Carotid Plaque Characteristics Predict Recurrent Ischemic Stroke and TIA. JACC Cardiovasc. Imaging 2022, 15, 1715–1726. [Google Scholar] [CrossRef] [PubMed]
- Carr, S.; Farb, A.; Pearce, W.H.; Virmani, R.; Yao, J.S.T. Atherosclerotic Plaque Rupture in Symptomatic Carotid Artery Stenosis. J. Vasc. Surg. 1996, 23, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Eesa, M.; Hill, M.D.; Al-Khathaami, A.; Al-Zawahmah, M.; Sharma, P.; Menon, B.K.; Tymchuk, S.; Demchuk, A.M.; Goyal, M. Role of CT Angiographic Plaque Morphologic Characteristics in Addition to Stenosis in Predicting the Symptomatic Side in Carotid Artery Disease. AJNR Am. J. Neuroradiol. 2010, 31, 1254–1260. [Google Scholar] [CrossRef] [PubMed]
- Paraskevas, K.I.; Veith, F.J.; Spence, J.D. How to Identify Which Patients with Asymptomatic Carotid Stenosis Could Benefit from Endarterectomy or Stenting. Stroke Vasc. Neurol. 2018, 3, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Markus, H.S.; King, A.; Shipley, M.; Topakian, R.; Cullinane, M.; Reihill, S.; Bornstein, N.M.; Schaafsma, A. Asymptomatic Embolisation for Prediction of Stroke in the Asymptomatic Carotid Emboli Study (ACES): A Prospective Observational Study. Lancet Neurol. 2010, 9, 663–671. [Google Scholar] [CrossRef]
- Baradaran, H.; Myneni, P.K.; Patel, P.; Askin, G.; Gialdini, G.; Al-Dasuqi, K.; Kamel, H.; Gupta, A. Association Between Carotid Artery Perivascular Fat Density and Cerebrovascular Ischemic Events. JAHA 2018, 7, e010383. [Google Scholar] [CrossRef]
- Saba, L.; Zucca, S.; Gupta, A.; Micheletti, G.; Suri, J.S.; Balestrieri, A.; Porcu, M.; Crivelli, P.; Lanzino, G.; Qi, Y.; et al. Perivascular Fat Density and Contrast Plaque Enhancement: Does a Correlation Exist? AJNR Am. J. Neuroradiol. 2020, 41, 1460–1465. [Google Scholar] [CrossRef]
- Miura, T.; Matsukawa, N.; Sakurai, K.; Katano, H.; Ueki, Y.; Okita, K.; Yamada, K.; Ojika, K. Plaque Vulnerability in Internal Carotid Arteries with Positive Remodeling. Cerebrovasc. Dis. Extra 2011, 1, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Watase, H.; Sun, J.; Hippe, D.S.; Balu, N.; Li, F.; Zhao, X.; Mani, V.; Fayad, Z.A.; Fuster, V.; Hatsukami, T.S.; et al. Carotid Artery Remodeling Is Segment Specific: An In Vivo Study by Vessel Wall Magnetic Resonance Imaging. ATVB 2018, 38, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, A.N.; Panayiotou, A.G.; Griffin, M.; Tyllis, T.; Bond, D.; Georgiou, N.; Kyriacou, E.; Avraamides, C.; Martin, R.M. Arterial Ultrasound Testing to Predict Atherosclerotic Cardiovascular Events. J. Am. Coll. Cardiol. 2022, 79, 1969–1982. [Google Scholar] [CrossRef] [PubMed]
- Takaya, N.; Cai, J.; Ferguson Mt, M.S.; Yarnykh, V.L.; Chu, B.; Saam, T.; Polissar, N.L.; Sherwood, J.; Cury, R.C.; Anders, R.J.; et al. Intra- and Interreader Reproducibility of Magnetic Resonance Imaging for Quantifying the Lipid-rich Necrotic Core Is Improved with Gadolinium Contrast Enhancement. Magn. Reson. Imaging 2006, 24, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Kakkos, S.K.; Nicolaides, A.N.; Charalambous, I.; Thomas, D.; Giannopoulos, A.; Naylor, A.R.; Geroulakos, G.; Abbott, A.L. Predictors and Clinical Significance of Progression or Regression of Asymptomatic Carotid Stenosis. J. Vasc. Surg. 2014, 59, 956–967.e1. [Google Scholar] [CrossRef] [PubMed]
- Benson, J.C.; Nardi, V.; Madhavan, A.A.; Bois, M.C.; Saba, L.; Savastano, L.; Lerman, A.; Lanzino, G. Reassessing the Carotid Artery Plaque “Rim Sign” on CTA: A New Analysis with Histopathologic Confirmation. AJNR Am. J. Neuroradiol. 2022, 43, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Saba, L.; Chen, H.; Cau, R.; Rubeis, G.D.; Zhu, G.; Pisu, F.; Jang, B.; Lanzino, G.; Suri, J.S.; Qi, Y.; et al. Impact Analysis of Different CT Configurations of Carotid Artery Plaque Calcifications on Cerebrovascular Events. AJNR Am. J. Neuroradiol. 2022, 43, 272–279. [Google Scholar] [CrossRef]
- Saba, L.; Nardi, V.; Cau, R.; Gupta, A.; Kamel, H.; Suri, J.S.; Balestrieri, A.; Congiu, T.; Butler, A.P.H.; Gieseg, S.; et al. Carotid Artery Plaque Calcifications: Lessons From Histopathology to Diagnostic Imaging. Stroke 2022, 53, 290–297. [Google Scholar] [CrossRef]
- Cury, R.C.; Leipsic, J.; Abbara, S.; Achenbach, S.; Berman, D.; Bittencourt, M.; Budoff, M.; Chinnaiyan, K.; Choi, A.D.; Ghoshhajra, B.; et al. CAD-RADSTM 2.0—2022 Coronary Artery Disease—Reporting and Data System An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Cardiology (ACC), the American College of Radiology (ACR) and the North America Society of Cardiovascular Imaging (NASCI). Radiol. Cardiothorac. Imaging 2022, 4, e220183. [Google Scholar] [CrossRef]
- Giannoukas, A.D.; Chabok, M.; Spanos, K.; Nicolaides, A. Screening for Asymptomatic Carotid Plaques with Ultrasound. Eur. J. Vasc. Endovasc. Surg. 2016, 52, 309–312. [Google Scholar] [CrossRef]
- Nambi, V.; Chambless, L.; Folsom, A.R.; He, M.; Hu, Y.; Mosley, T.; Volcik, K.; Boerwinkle, E.; Ballantyne, C.M. Carotid Intima-Media Thickness and Presence or Absence of Plaque Improves Prediction of Coronary Heart Disease Risk in the Atherosclerosis Risk in Communities (ARIC) Study. J. Am. Coll. Cardiol. 2010, 55, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Landry, A.; Spence, J.D.; Fenster, A. Measurement of Carotid Plaque Volume by 3-Dimensional Ultrasound. Stroke 2004, 35, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Hippe, D.S.; Li, R.; Canton, G.M.; Sui, B.; Song, Y.; Li, F.; Xue, Y.; Sun, J.; Yamada, K.; et al. Prevalence and Characteristics of Carotid Artery High-Risk Atherosclerotic Plaques in Chinese Patients with Cerebrovascular Symptoms: A Chinese Atherosclerosis Risk Evaluation II Study. J. Am. Heart Assoc. 2017, 6, e005831. [Google Scholar] [CrossRef] [PubMed]
- Underhill, H.R.; Kerwin, W.S.; Hatsukami, T.S.; Yuan, C. Automated Measurement of Mean Wall Thickness in the Common Carotid Artery by MRI: A Comparison to Intima-Media Thickness by B-Mode Ultrasound. J. Magn. Reson. Imaging 2006, 24, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Devuyst, G.; Karapanayiotides, T.; Ruchat, P.; Pusztaszeri, M.; Lobrinus, J.-A.; Jonasson, L.; Cuisinaire, O.; Kalangos, A.; Despland, P.-A.; Thiran, J.-P.; et al. Ultrasound Measurement of the Fibrous Cap in Symptomatic and Asymptomatic Atheromatous Carotid Plaques. Circulation 2005, 111, 2776–2782. [Google Scholar] [CrossRef] [PubMed]
- Sztajzel, R.; Momjian, S.; Momjian-Mayor, I.; Murith, N.; Djebaili, K.; Boissard, G.; Comelli, M.; Pizolatto, G. Stratified Gray-Scale Median Analysis and Color Mapping of the Carotid Plaque: Correlation With Endarterectomy Specimen Histology of 28 Patients. Stroke 2005, 36, 741–745. [Google Scholar] [CrossRef]
- Mitchell, C.C.; Stein, J.H.; Cook, T.D.; Salamat, S.; Wang, X.; Varghese, T.; Jackson, D.C.; Sandoval Garcia, C.; Wilbrand, S.M.; Dempsey, R.J. Histopathologic Validation of Grayscale Carotid Plaque Characteristics Related to Plaque Vulnerability. Ultrasound Med. Biol. 2017, 43, 129–137. [Google Scholar] [CrossRef]
- McNally, J.S.; Kim, S.-E.; Mendes, J.; Hadley, J.R.; Sakata, A.; De Havenon, A.H.; Treiman, G.S.; Parker, D.L. Magnetic Resonance Imaging Detection of Intraplaque Hemorrhage. Magn. Reson. Insights 2017, 10, 1178623x17694150. [Google Scholar] [CrossRef]
- Saba, L.; Saam, T.; Jäger, H.R.; Yuan, C.; Hatsukami, T.S.; Saloner, D.; Wasserman, B.A.; Bonati, L.H.; Wintermark, M. Imaging Biomarkers of Vulnerable Carotid Plaques for Stroke Risk Prediction and Their Potential Clinical Implications. Lancet Neurol. 2019, 18, 559–572. [Google Scholar] [CrossRef]
- Cau, R.; Gupta, A.; Kooi, M.E.; Saba, L. Pearls and Pitfalls of Carotid Artery Imaging: Ultrasound, Computed Tomography Angiography, and MR Imaging. Radiol. Clin. N. Am. 2023, 61, 405–413. [Google Scholar] [CrossRef]
- Saba, L.; Agarwal, N.; Cau, R.; Gerosa, C.; Sanfilippo, R.; Porcu, M.; Montisci, R.; Cerrone, G.; Qi, Y.; Balestrieri, A.; et al. Review of Imaging Biomarkers for the Vulnerable Carotid Plaque. JVS-Vasc. Sci. 2021, 2, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gialdini, G.; Lerario, M.P.; Baradaran, H.; Giambrone, A.; Navi, B.B.; Marshall, R.S.; Iadecola, C.; Kamel, H. Magnetic Resonance Angiography Detection of Abnormal Carotid Artery Plaque in Patients With Cryptogenic Stroke. JAHA 2015, 4, e002012. [Google Scholar] [CrossRef] [PubMed]
- Cademartiri, F.; Meloni, A.; Pistoia, L.; Degiorgi, G.; Clemente, A.; De Gori, C.; Positano, V.; Celi, S.; Berti, S.; Emdin, M.; et al. Dual Source Photon-Counting Computed Tomography—Part II: Clinical Overview of Neurovascular Applications. JCM 2023, 12, 3626. [Google Scholar] [CrossRef] [PubMed]
- Dahal, S.; Raja, A.Y.; Searle, E.; Colgan, F.E.; Crighton, J.S.; Roake, J.; Saba, L.; Gieseg, S.; Butler, A.P.H. Components of Carotid Atherosclerotic Plaque in Spectral Photon-Counting CT with Histopathologic Comparison. Eur. Radiol. 2023, 33, 1612–1619. [Google Scholar] [CrossRef] [PubMed]
- Boussel, L.; Coulon, P.; Thran, A.; Roessl, E.; Martens, G.; Sigovan, M.; Douek, P. Photon Counting Spectral CT Component Analysis of Coronary Artery Atherosclerotic Plaque Samples. BJR 2014, 87, 20130798. [Google Scholar] [CrossRef] [PubMed]
- Cademartiri, F.; Meloni, A.; Pistoia, L.; Degiorgi, G.; Clemente, A.; Gori, C.D.; Positano, V.; Celi, S.; Berti, S.; Emdin, M.; et al. Dual-Source Photon-Counting Computed Tomography—Part I: Clinical Overview of Cardiac CT and Coronary CT Angiography Applications. JCM 2023, 12, 3627. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.J.; Tison, G.H.; Delling, F.N. Artificial Intelligence in Cardiovascular Imaging. Methodist. Debakey Cardiovasc. J. 2020, 16, 138–145. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Volpato, V.; Cau, R.; Chiesa, M.; Saba, L.; Guglielmo, M.; Senatieri, A.; Chierchia, G.; Pontone, G.; Dell’Aversana, S.; et al. Application of AI in Cardiovascular Multimodality Imaging. Heliyon 2022, 8, e10872. [Google Scholar] [CrossRef]
- Paraskevas, K.I.; Saba, L.; Suri, J.S. Applications of Artificial Intelligence in Vascular Diseases. Angiology 2022, 73, 597–598. [Google Scholar] [CrossRef]
- Cau, R.; Pisu, F.; Muscogiuri, G.; Mannelli, L.; Suri, J.S.; Saba, L. Applications of Artificial Intelligence-Based Models in Vulnerable Carotid Plaque. Vessel. Plus 2023, 7, 20. [Google Scholar] [CrossRef]
- Menchón-Lara, R.-M.; Bastida-Jumilla, M.-C.; Morales-Sánchez, J.; Sancho-Gómez, J.-L. Automatic Detection of the Intima-Media Thickness in Ultrasound Images of the Common Carotid Artery Using Neural Networks. Med. Biol. Eng. Comput. 2014, 52, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Caetano Dos Santos, F.L.; Kolasa, M.; Terada, M.; Salenius, J.; Eskola, H.; Paci, M. VASIM: An Automated Tool for the Quantification of Carotid Atherosclerosis by Computed Tomography Angiography. Int. J. Cardiovasc. Imaging 2019, 35, 1149–1159. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, M.; Alfraeus, J.; Bustamante, M.; Good, E.; Engvall, J.; De Muinck, E.; Dyverfeldt, P. Automated Segmentation of the Individual Branches of the Carotid Arteries in Contrast-Enhanced MR Angiography Using DeepMedic. BMC Med. Imaging 2021, 21, 38. [Google Scholar] [CrossRef] [PubMed]
- Latha, S.; Samiappan, D.; Muthu, P.; Kumar, R. Fully Automated Integrated Segmentation of Carotid Artery Ultrasound Images Using DBSCAN and Affinity Propagation. J. Med. Biol. Eng. 2021, 41, 260–271. [Google Scholar] [CrossRef]
- Zhang, R.; Zhang, Q.; Ji, A.; Lv, P.; Zhang, J.; Fu, C.; Lin, J. Identification of High-Risk Carotid Plaque with MRI-Based Radiomics and Machine Learning. Eur. Radiol. 2021, 31, 3116–3126. [Google Scholar] [CrossRef] [PubMed]
- Cilla, S.; Macchia, G.; Lenkowicz, J.; Tran, E.H.; Pierro, A.; Petrella, L.; Fanelli, M.; Sardu, C.; Re, A.; Boldrini, L.; et al. CT Angiography-Based Radiomics as a Tool for Carotid Plaque Characterization: A Pilot Study. Radiol. Med. 2022, 127, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Saba, L.; Sanagala, S.S.; Gupta, S.K.; Koppula, V.K.; Laird, J.R.; Viswanathan, V.; Sanches, M.J.; Kitas, G.D.; Johri, A.M.; Sharma, N.; et al. A Multicenter Study on Carotid Ultrasound Plaque Tissue Characterization and Classification Using Six Deep Artificial Intelligence Models: A Stroke Application. IEEE Trans. Instrum. Meas. 2021, 70, 2505312. [Google Scholar] [CrossRef]
- Gharahi, H.; Zambrano, B.A.; Zhu, D.C.; DeMarco, J.K.; Baek, S. Computational Fluid Dynamic Simulation of Human Carotid Artery Bifurcation Based on Anatomy and Volumetric Blood Flow Rate Measured with Magnetic Resonance Imaging. Int. J. Adv. Eng. Sci. Appl. Math. 2016, 8, 46–60. [Google Scholar] [CrossRef]
- Wang, S.; Wu, D.; Li, G.; Zhang, Z.; Xiao, W.; Li, R.; Qiao, A.; Jin, L.; Liu, H. Deep Learning-Based Hemodynamic Prediction of Carotid Artery Stenosis before and after Surgical Treatments. Front. Physiol. 2023, 13, 1094743. [Google Scholar] [CrossRef]
- De Bruyne, B.; Sarma, J. Fractional Flow Reserve: A Review: Invasive Imaging. Heart 2008, 94, 949–959. [Google Scholar] [CrossRef]
- Leng, X.; Scalzo, F.; Fong, A.K.; Johnson, M.; Ip, H.L.; Soo, Y.; Leung, T.; Liu, L.; Feldmann, E.; Wong, K.S.; et al. Computational Fluid Dynamics of Computed Tomography Angiography to Detect the Hemodynamic Impact of Intracranial Atherosclerotic Stenosis. Neurovasc. Imaging 2015, 1, 1. [Google Scholar] [CrossRef]
- Leng, X.; Scalzo, F.; Ip, H.L.; Johnson, M.; Fong, A.K.; Fan, F.S.Y.; Chen, X.; Soo, Y.O.Y.; Miao, Z.; Liu, L.; et al. Computational Fluid Dynamics Modeling of Symptomatic Intracranial Atherosclerosis May Predict Risk of Stroke Recurrence. PLoS ONE 2014, 9, e97531. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICA Stenosis (%NASCET) | ICA Stenosis (%ECST) |
|---|---|
| 30 | 60 |
| 50 | 70 |
| 60 | 75 |
| 70 | 80 |
| 80 | 90 |
| ICA Stenosis (NASCET) | ICA PSV (cm/s) | ICA EDV (cm/s) | PSV Ratio (ICA/ECA) |
|---|---|---|---|
| Normal | <125 | <40 | <2.0 |
| <50% | <125 | <40 | <2.0 |
| 50–60% | 125–130 | 40–100 | 2.0–4.0 |
| >70% | >230 | >100 | >4.0 |
| Near-occlusion | Variable | Variable | Variable |
| Total occlusion | Undetectable | Undetectable | Undetectable |
| DSA [48] | Delayed time of contrast arrival Evidence of collaterals ICA-to-ICA comparison of diameter reduction ICA-to-ECA comparison of diameter reduction |
| US [63] | Distal PSV < 50 cm/s in high-PSV stenoses |
| CTA [53] | Distal ICA < 2 mm ICA ratio < 0.42 |
| PC-MRA [51] | ICA-CBF * < 0.225 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saba, L.; Scicolone, R.; Johansson, E.; Nardi, V.; Lanzino, G.; Kakkos, S.K.; Pontone, G.; Annoni, A.D.; Paraskevas, K.I.; Fox, A.J. Quantifying Carotid Stenosis: History, Current Applications, Limitations, and Potential: How Imaging Is Changing the Scenario. Life 2024, 14, 73. https://0-doi-org.brum.beds.ac.uk/10.3390/life14010073
Saba L, Scicolone R, Johansson E, Nardi V, Lanzino G, Kakkos SK, Pontone G, Annoni AD, Paraskevas KI, Fox AJ. Quantifying Carotid Stenosis: History, Current Applications, Limitations, and Potential: How Imaging Is Changing the Scenario. Life. 2024; 14(1):73. https://0-doi-org.brum.beds.ac.uk/10.3390/life14010073
Chicago/Turabian StyleSaba, Luca, Roberta Scicolone, Elias Johansson, Valentina Nardi, Giuseppe Lanzino, Stavros K. Kakkos, Gianluca Pontone, Andrea D. Annoni, Kosmas I. Paraskevas, and Allan J. Fox. 2024. "Quantifying Carotid Stenosis: History, Current Applications, Limitations, and Potential: How Imaging Is Changing the Scenario" Life 14, no. 1: 73. https://0-doi-org.brum.beds.ac.uk/10.3390/life14010073