Breakfast Skipping in Female College Students Is a Potential and Preventable Predictor of Gynecologic Disorders at Health Service Centers

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
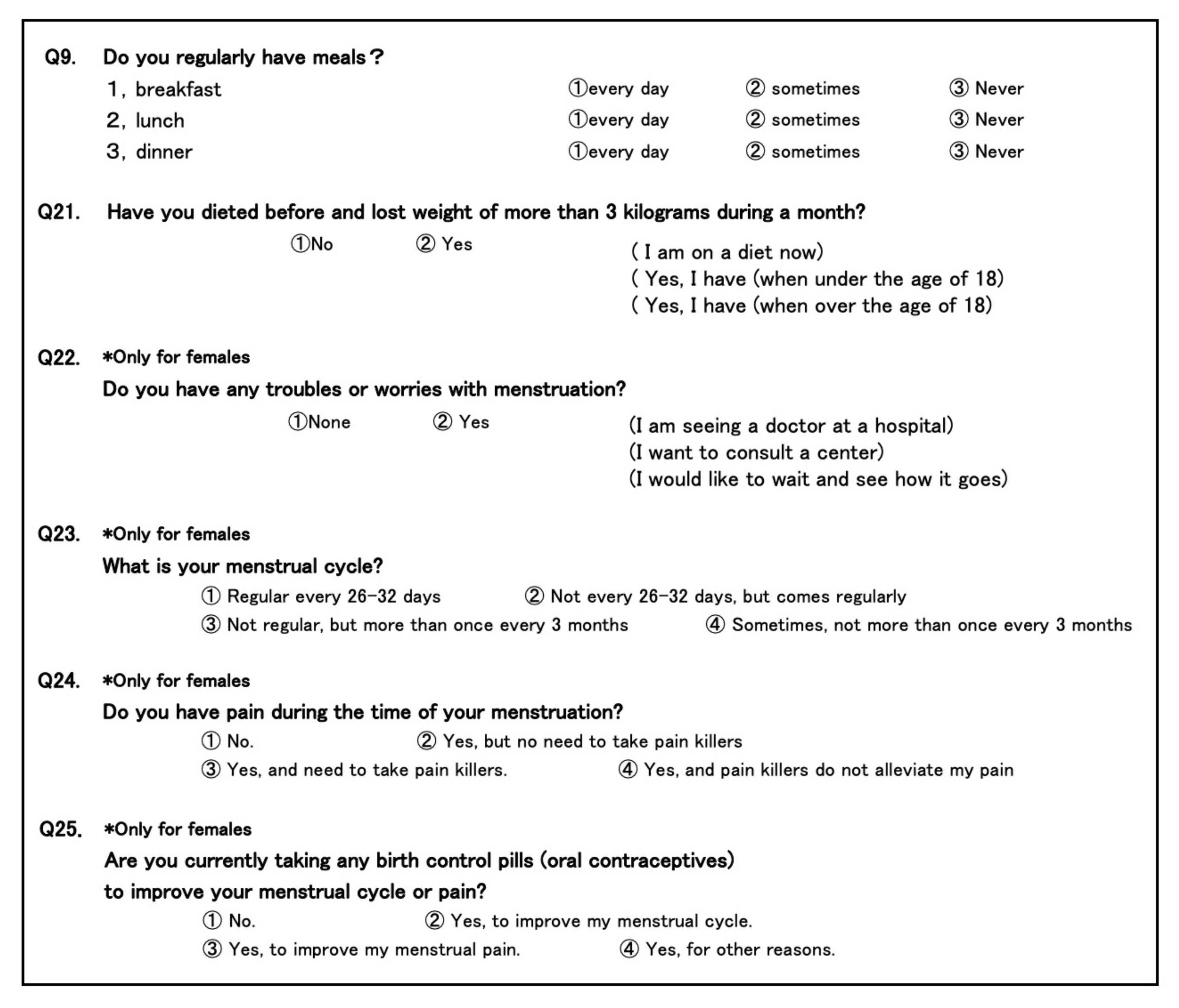
2.2. Dietary Habits
2.2.1. Meal Skipping
2.2.2. History of Dieting
2.3. Menstrual Disorders
2.3.1. Troubles or Worries with Menstruation
2.3.2. Menstrual Irregularity
2.3.3. Menstrual Pain
2.3.4. Use of Oral Contraceptives
2.4. Statistical Analysis
3. Results
3.1. Dietary Habits
3.1.1. Meal Skipping
3.1.2. History of Diet
3.2. Menstrual Disorders
3.2.1. Troubles or Worries with Menstruation
3.2.2. Menstrual Irregularity
3.2.3. Menstrual Pain
3.2.4. Use of Oral Contraceptives
3.2.5. Correction by Data of Oral Contraceptive Users
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Das, J.K.; Salam, R.A.; Thornburg, K.L.; Prentice, A.M.; Campisi, S.; Lassi, Z.S.; Koletzko, B.; Bhutta, Z.A. Nutrition in adolescents: Physiology, metabolism, and nutritional needs. Ann. N. Y. Acad. Sci. 2017, 1393, 21–33. [Google Scholar] [CrossRef]
- Pendergast, F.J.; Livingstone, K.M.; Worsley, A.; McNaughton, S.A. Correlates of meal skipping in young adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadolowska, L.; Hamulka, J.; Kowalkowska, J.; Wojtas, N.; Górnicka, M.; Jeruszka-Bielak, M.; Kostecka, M.; Wawrzyniak, A. Skipping Breakfast and a Meal at School: Its Correlates in Adiposity Context. Report from the ABC of Healthy Eating Study of Polish Teenagers. Nutrients 2019, 11, 1563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, K.; Nakamura, K.; Nishiwaki, T.; Saito, T.; Okuda, Y.; Yamamoto, M. Intakes of calcium and other nutrients related to bone health in Japanese female college students: A study using the duplicate portion sampling method. Tohoku J. Exp. Med. 2005, 206, 319–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assefa, N.; Demissie, A.; Hailemeskel, S. Primary dysmenorrhea magnitude, associated risk factors, and its effect on academic performance: Evidence from female university students in Ethiopia. Int. J. Women’s Health 2016, 8, 489–496. [Google Scholar] [CrossRef] [Green Version]
- Nazni, P. Association of western diet & lifestyle with decreased fertility. Indian J. Med. Res. 2014, 14, S78–S81. [Google Scholar]
- Bajalan, Z.; Alimoradi, Z.; Moafi, F. Nutrition as a Potential Factor of Primary Dysmenorrhea: A Systematic Review of Observational Studies. Gynecol. Obstet. Investig. 2019, 84, 209–224. [Google Scholar] [CrossRef]
- Kyriakidis, M.; Caetano, L.; Anastasiadou, N.; Karasu, T.; Lashen, H. Functional hypothalamic amenorrhoea: Leptin treatment, dietary intervention, and counselling as alternatives to traditional practice—Systematic review. Eur. J. Obstet. Gynecol. Reprod. Boil. 2016, 198, 131–137. [Google Scholar] [CrossRef]
- Warren, M.P.; Voussoughian, F.; Geer, E.B.; Hyle, E.P.; Adberg, C.L.; Ramos, R.H. Functional Hypothalamic Amenorrhea: Hypoleptinemia and Disordered Eating. J. Clin. Endocrinol. Metab. 1999, 84, 873–877. [Google Scholar] [CrossRef]
- Harris, H.R.; Eke, A.C.; Chavarro, J.E.; Missmer, S.A. Fruit and vegetable consumption and risk of endometriosis. Hum. Reprod. 2018, 33, 715–727. [Google Scholar] [CrossRef]
- Fontana, R.; Della Torre, S. The Deep Correlation between Energy Metabolism and Reproduction: A View on the Effects of Nutrition for Women Fertility. Nutrients 2016, 8, 87. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T. Skipping breakfast is associated with dysmenorrhea in young women in Japan. Int. J. Food Sci. Nutr. 2003, 54, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T.; Nakata, R. Skipping breakfast is associated with reproductive dysfunction in post-adolescent female college students. Appetite 2010, 55, 714–717. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T. Diet during adolescence is a trigger for subsequent development of dysmenorrhea in young women. Int. J. Food Sci. Nutr. 2007, 58, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T.; Ono, M.; Mieda, M.; Yoshikawa, H.; Nakata, R.; Daikoku, T.; Sekizuka-Kagami, N.; Maida, Y.; Ando, H.; Fujiwara, H. Adolescent Dietary Habit-induced Obstetric and Gynecologic Disease (ADHOGD) as a New Hypothesis-Possible Involvement of Clock System. Nutrients 2020, 12, 1294. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, I.; Póvoa, A.M. Primary Dysmenorrhea: Assessment and Treatment, ACOG Committee Opinion, No. 760. Obstet. Gynecol. 2018, 132, e249–e258. [Google Scholar] [CrossRef]
- Ryan, T.H. Significance tests for multiple comparison of proportions, variances, and other statistics. Psychol. Bull. 1960, 57, 318–328. [Google Scholar] [CrossRef]
- Dandotiya, D.; Priya, A.; Toppo, M.; Melwani, V.; Dohare, P.; Khan, A.; Sethia, S. Effect of Skipping Breakfast on Young Girls’ Menstruation. Indian J. Youth Adolesc. Health 2017, 4, 17–20. [Google Scholar] [CrossRef] [Green Version]
- Abu-Helwa, H.A.; Mitaeb, A.A.; Al-Hamshri, S.; Sweileh, W.M. Prevalence of dysmenorrhea and predictors of its pain intensity among Palestinian female university students. BMC Women’s Health 2018, 18, 18. [Google Scholar] [CrossRef] [Green Version]
- Hu, Z.; Tang, L.; Chen, L.; Kaminga, A.C.; Xu, H. Prevalence and Risk Factors Associated with Primary Dysmenorrhea among Chinese Female University Students: A Cross-sectional Study. J. Pediatr. Adolesc. Gynecol. 2020, 33, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Faramarzi, M.; Salmalian, H. Association of Psychologic and Nonpsychologic Factors with Primary Dysmenorrhea. Iran. Red Crescent Med. J. 2014, 16, e16307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagua, T.; Tkeshelashvili, B.; Gagua, D. Primary dysmenorrhea: Prevalence in adolescent population of Tbilisi, Georgia, and risk factors. J. Turk. Gynecol. Assoc. 2012, 13, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Mieda, M.; Ono, D.; Hasegawa, E.; Okamoto, H.; Honma, K.-I.; Honma, S.; Sakurai, T. Cellular Clocks in AVP Neurons of the SCN Are Critical for Interneuronal Coupling Regulating Circadian Behavior Rhythm. Neuron 2015, 85, 1103–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mieda, M.; Sakurai, T. Bmal1 in the Nervous System Is Essential for Normal Adaptation of Circadian Locomotor Activity and Food Intake to Periodic Feeding. J. Neurosci. 2011, 31, 15391–15396. [Google Scholar] [CrossRef] [Green Version]
- Mieda, M. The central circadian clock of the suprachiasmatic nucleus as an ensemble of multiple oscillatory neurons. Neurosci. Res. 2019. [Google Scholar] [CrossRef]
- Deligeoroglou, E. Dysmenorrhea. Ann. N. Y. Acad. Sci. 2006, 900, 237–244. [Google Scholar] [CrossRef]
- Dawood, M.; Dawood, M.Y. Dysmenorrhoea and Prostaglandins: Pharmacological and Therapeutic Considerations. Drugs 1981, 22, 42–56. [Google Scholar] [CrossRef]
- Bernardi, M.; Lazzeri, L.; Perelli, F.; Reis, F.M.; Petraglia, F. Dysmenorrhea and related disorders. F1000Research 2017, 6, 1645. [Google Scholar] [CrossRef] [Green Version]
- Lundström, V.; Green, K. Endogenous levels of prostaglandin F2α and its main metabolites in plasma and endometrium of normal and dysmenorrheic women. Am. J. Obstet. Gynecol. 1978, 130, 640–646. [Google Scholar] [CrossRef]
- Fujiwara, T.; Nakata, R.; Ono, M.; Mieda, M.; Ando, H.; Daikoku, T.; Fujiwara, H. Time Restriction of Food Intake During the Circadian Cycle Is a Possible Regulator of Reproductive Function in Postadolescent Female Rats. Curr. Dev. Nutr. 2018, 3, nzy093. [Google Scholar] [CrossRef]
- Morotti, M.; Vincent, K.; Becker, C.M. Mechanisms of pain in endometriosis. Eur. J. Obstet. Gynecol. Reprod. Boil. 2017, 209, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Kim, J.H. Endometriosis and Female Pelvic Pain. Semin. Reprod. Med. 2018, 36, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Dawood, M.Y. Dysmenorrhea. Clin. Obstet. Gynecol. 1990, 33, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Montero, P.; Bernis, C.; Fernandez, V.; Castro, S. Influence of body mass index and slimming habits on menstrual pain and cycle irregularity. J. Biosoc. Sci. 1996, 28, 315–323. [Google Scholar] [CrossRef]


{kind=link}
| Having Meals | Without Troubles or Worries | With Troubles or Worries | ||
|---|---|---|---|---|
| Breakfast (n/%) | ||||
| Every day | 1756/83.6 | 345/16.4 |  | ** |
| Sometimes | 707/80.2 | 174/19.8 | ||
| None | 98/76.6 | 30/23.4 | ||
| Lunch (n/%) | ||||
| Every day | 2429/82.7 | 507/17.3 |  | * |
| Sometimes | 132/76.3 | 41/23.7 | ||
| None | 0/0.0 | 1/100.0 | ||
| Dinner (n/%) | ||||
| Every day | 2410/72.6 | 507/17.4 |  | n.s. |
| Sometimes | 150/78.5 | 41/21.5 | ||
| None | 1/50.0 | 1/50.0 | ||
| History of dieting (n/%) | ||||
| Not done | 2423/83.0 | 496/17.0 |  | *** |
| Done | 138/72.3 | 53/27.7 | ||
| At present | 9/75.0 | 3/25.0 | ||
| Past at 18< | 59/72.0 | 23/28.0 | ||
| Past at 18≥ | 56/76.7 | 17/23.3 | ||
| Trouble or Worries with Menstruation | Menstrual Pain | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
| Having breakfast Everyday vs. Sometimes or none | 1.22 (1.00–1.49) | 0.048 | 1.23 (1.05–1.43) | 0.012 |
| Having lunch Everyday vs. Sometimes or none | 1.36 (0.91–2.01) | 0.124 | 1.29 (0.92–1.79) | 0.137 |
| Having dinner Everyday vs. Sometimes or none | 1.00 (0.68–1.45) | 0.966 | 0.94 (0.68–1.30) | 0.697 |
| History of dieting | ||||
| Done vs. Not done | 1.88 (1.35–2.61) | <0.001 | 1.05 (0.78–1.42) | 0.740 |
| Meal Skipping | Regular | Constant Out of 26–32-Days | Irregular, within 3 M | Sometimes, More than 3 M | ||
|---|---|---|---|---|---|---|
| Breakfast (n/%) | ||||||
| Every day | 1420/67.6 | 381/18.1 | 255/12.1 | 45/2.1 |  | n.s. |
| Sometimes | 594/67.4 | 162/18.4 | 112/12.7 | 13/1.5 | ||
| None | 77/60.2 | 35/27.3 | 12/9.4 | 4/3.1 | ||
| Lunch (n/%) | ||||||
| Every day | 1971/67.1 | 551/18.8 | 353/12.0 | 61/2.1 |  | n.s. |
| Sometimes | 119/68.8 | 27/15.6 | 26/15.0 | 1/0.6 | ||
| None | 1/100.0 | 0/0.0 | 0/0.0 | 0/0.0 | ||
| Dinner (n/%) | ||||||
| Every day | 1974/67.7 | 535/18.3 | 349/12.0 | 59/2.0 |  | n.s. |
| Sometimes | 116/60.7 | 43/22.5 | 29/15.2 | 3/1.6 | ||
| None | 1/50.0 | 0/0.0 | 1/50.0 | 0/0.0 | ||
| History of dieting (n/%) | ||||||
| Not done | 1973/67.6 | 539/18.5 | 352/12.1 | 55/1.9 |  | n.s. |
| Done | 118/61.8 | 39/20.4 | 27/14.1 | 7/3.7 | ||
| At present | 10/83.3 | 1/8.3 | 0/0.0 | 1/8.3 | ||
| Past at 18< | 51/62.2 | 18/22.0 | 12/14.6 | 1/1.2 | ||
| Past at 18≥ | 49/67.1 | 11/15.1 | 9/12.3 | 4/5.5 | ||
| Meal Skipping | Free of Pain | Not Requiring Analgesic | Requiring Analgesic | Not Relieved by Analgesic | ||||
|---|---|---|---|---|---|---|---|---|
| Breakfast (n/%) | ||||||||
| Every day | 496/23.6 | 822/39.1 | 746/35.5 | 37/1.8 |  | n.s. | *** | |
| Sometimes | 169/19.2 | 354/40.2 | 343/38.9 | 15/1.7 | *** | |||
| None | 18/14.1 | 38/29.7 | 68/53.1 | 4/3.1 | ||||
| Lunch (n/%) | ||||||||
| Every day | 650/22.1 | 1153/39.3 | 1083/36.9 | 50/1.7 |  | n.s. | ||
| Sometimes | 33/19.1 | 61/35.3 | 73/42.2 | 6/3.5 | ||||
| None | 0/0.0 | 0/0.0 | 1/100.0 | 0/0.0 | ||||
| Dinner (n/%) | ||||||||
| Every day | 635/21.8 | 1148/39.4 | 1083/37.1 | 51/1.7 |  | n.s. | ||
| Sometimes | 48/25.1 | 65/34.0 | 74/38.7 | 4/2.1 | ||||
| None | 0/0.0 | 1/50.0 | 0/0.0 | 1/50.0 | ||||
| History of dieting (n/%) | ||||||||
| Not done | 641/22.0 | 1143/39.2 | 1086/37.2 | 49/1.7 |  | n.s. | ||
| Done | 42/22.0 | 71/37.2 | 71/37.2 | 7/3.7 | ||||
| At present | 4/33.3 | 4/33.3 | 3/25.0 | 1/8.3 | ||||
| Past at 18< | 18/22.0 | 37/45.1 | 25/30.5 | 2/2.4 | n.s. | |||
| Past at 18≥ | 17/23.3 | 22/30.1 | 31/42.5 | 3/4.1 | ||||
| Meal Skipping | Not Using | Using for Menstrual Cycle | Using for Menstrual Pain | Other Reasons | ||
|---|---|---|---|---|---|---|
| Breakfast (n/%) | ||||||
| Every day | 2012/95.8 | 41/2.0 | 33/1.6 | 15/0.7 |  | n.s. |
| Sometimes | 837/95.0 | 15/1.7 | 21/2.4 | 8/0.9 | ||
| None | 121/94.5 | 3/2.3 | 2/1.6 | 2/1.6 | ||
| Lunch (n/%) | ||||||
| Every day | 2805/95.5 | 55/1.9 | 53/1.8 | 23/0.8 |  | n.s. |
| Sometimes | 164/94.8 | 4/2.3 | 3/1.7 | 2/1.2 | ||
| None | 1/100.0 | 0/0.0 | 0/0.0 | 0/0.0 | ||
| Dinner (n/%) | ||||||
| Every day | 2785/95.5 | 56/1.9 | 52/1.8 | 24/0.8 |  | n.s. |
| Sometimes | 184/96.3 | 3/1.6 | 3/1.6 | 1/0.5 | ||
| None | 1/50.0 | 0/0.0 | 1/50.0 | 0/0.0 | ||
| History of dieting (n/%) | ||||||
| Not done | 2798/95.9 | 55/1.9 | 47/1.6 | 19/0.7 |  | *** |
| Done | 172/90.1 | 4/2.1 | 9/4.7 | 6/3.1 | ||
| At present | 9/75.0 | 0/0.0 | 2/16.7 | 1/8.3 | ||
| Past at 18< | 74/90.2 | 2/2.4 | 4/4.9 | 2/2.4 | ||
| Past at 18≥ | 66/90.4 | 2/2.7 | 2/2.7 | 3/4.1 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujiwara, T.; Ono, M.; Iizuka, T.; Sekizuka-Kagami, N.; Maida, Y.; Adachi, Y.; Fujiwara, H.; Yoshikawa, H. Breakfast Skipping in Female College Students Is a Potential and Preventable Predictor of Gynecologic Disorders at Health Service Centers. Diagnostics 2020, 10, 476. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070476
Fujiwara T, Ono M, Iizuka T, Sekizuka-Kagami N, Maida Y, Adachi Y, Fujiwara H, Yoshikawa H. Breakfast Skipping in Female College Students Is a Potential and Preventable Predictor of Gynecologic Disorders at Health Service Centers. Diagnostics. 2020; 10(7):476. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070476
Chicago/Turabian StyleFujiwara, Tomoko, Masanori Ono, Takashi Iizuka, Naomi Sekizuka-Kagami, Yoshiko Maida, Yumi Adachi, Hiroshi Fujiwara, and Hiroaki Yoshikawa. 2020. "Breakfast Skipping in Female College Students Is a Potential and Preventable Predictor of Gynecologic Disorders at Health Service Centers" Diagnostics 10, no. 7: 476. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070476