Expression Analysis of Muscle-Specific miRNAs in Plasma-Derived Extracellular Vesicles from Patients with Chronic Obstructive Pulmonary Disease

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort Characteristics
2.2. Isolation and Characterization of Extracellular Vesicles
2.3. Evaluation of EV-Derived miRNA Expression
2.4. miRNA Target Prediction and Pathway Analysis
2.5. Statistical Analysis
3. Results
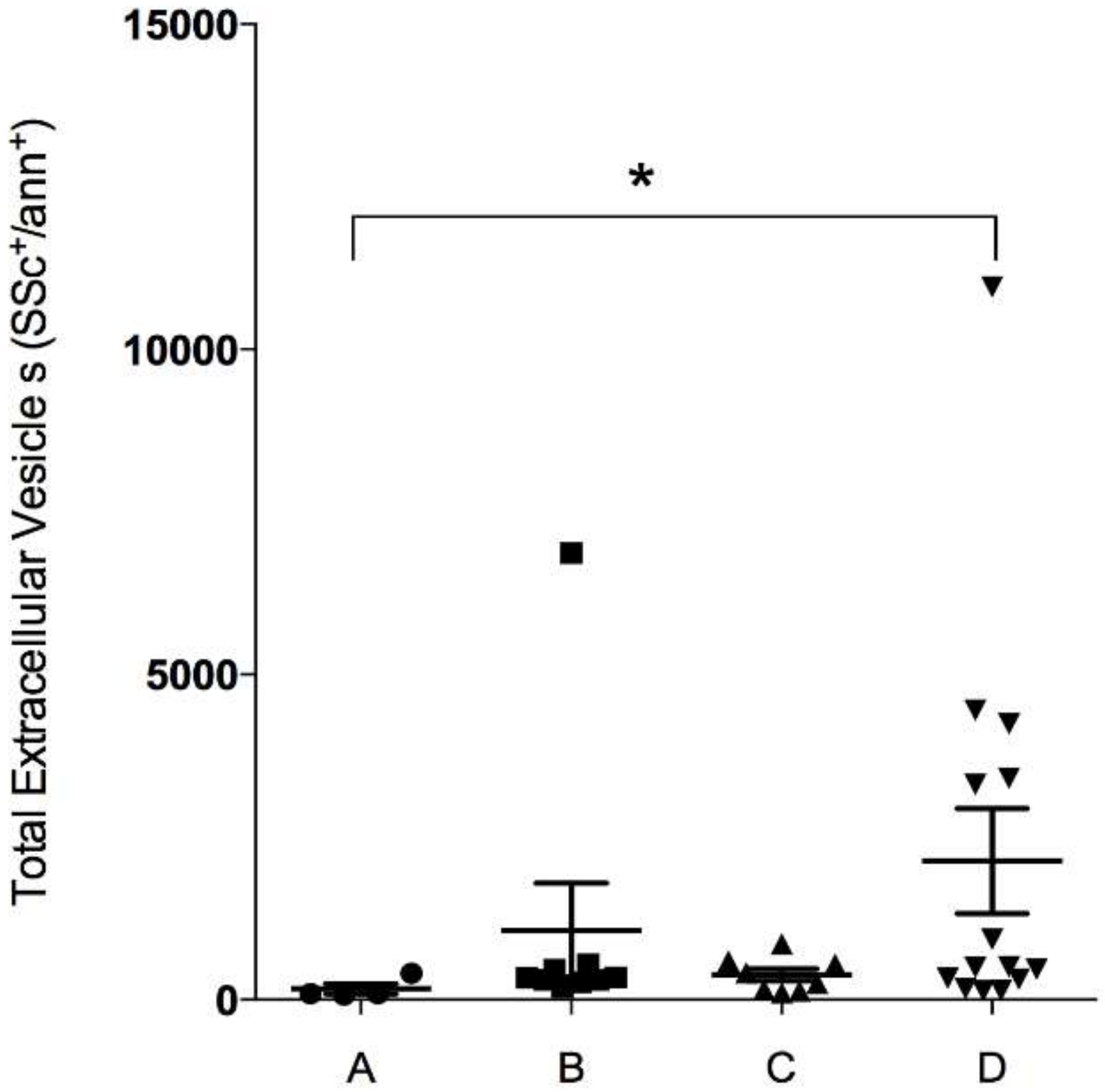
3.1. Patient Characteristics and Enumeration of EV According to GOLD Groups
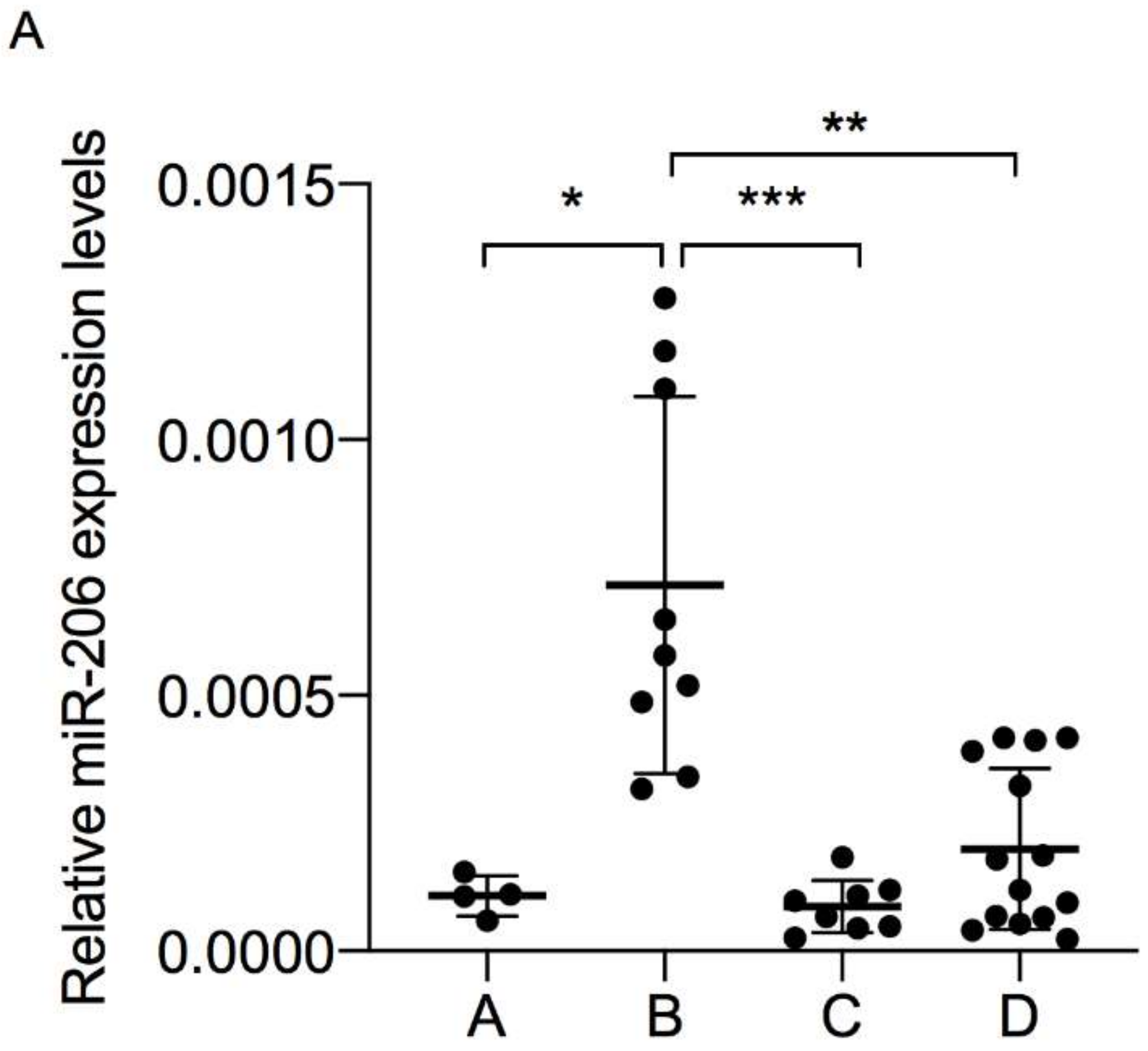
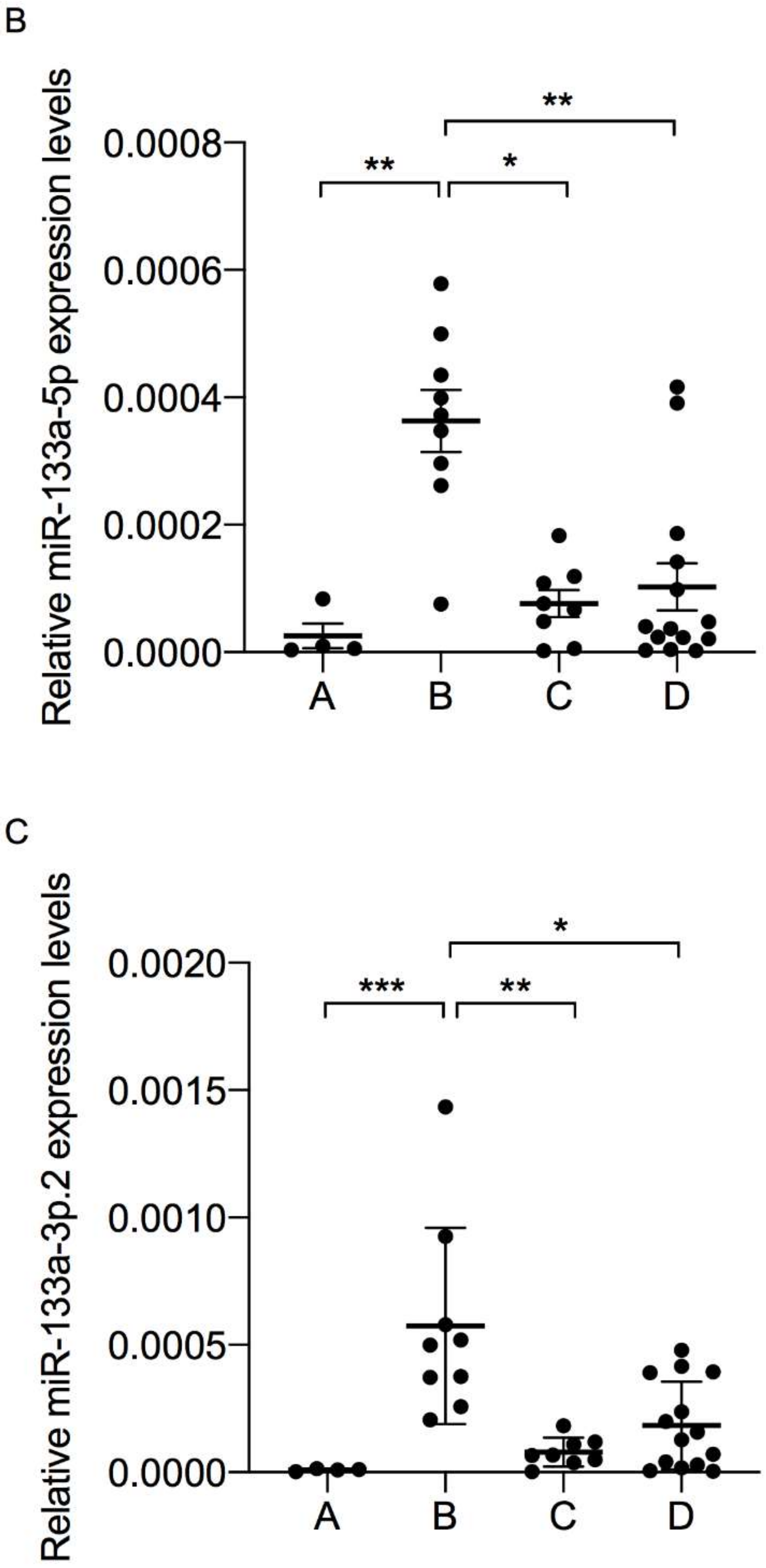
3.2. Muscle-Specific miRNAs Expression in Plasma-Derived EV
3.3. Classification Value of Triple Signature of EV-Derived myo-miRNAs
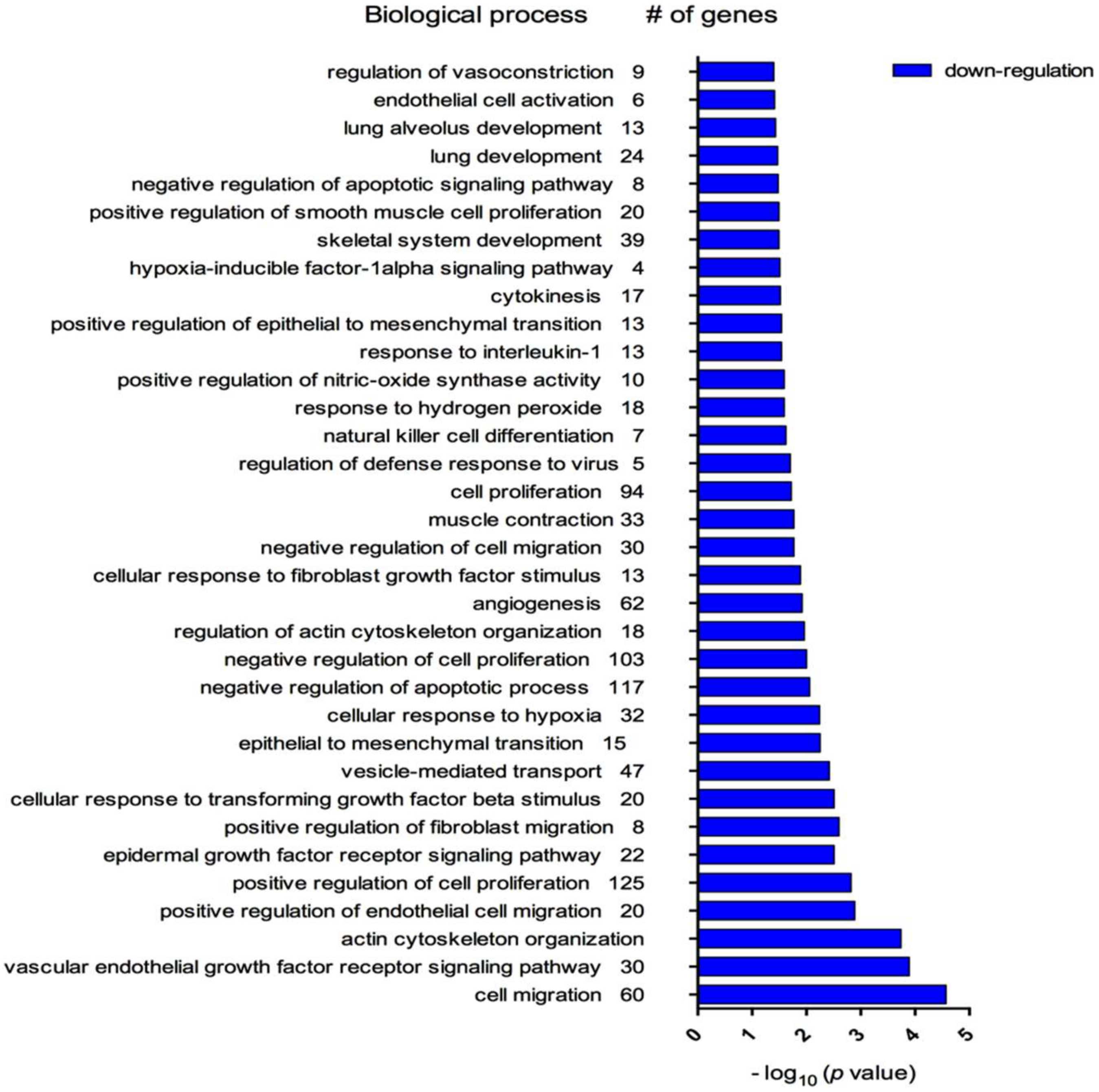
3.4. Biological Processes Associated with myo-miRNAs Modulation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Agusti, A.; Sobradillo, P.; Celli, B. Addressing the complexity of chronic obstructive pulmonary disease: From phenotypes and biomarkers to scale-free networks, systems biology, and P4 medicine. Am. J. Respir. Crit. Care Med. 2011, 183, 1129–1137. [Google Scholar] [CrossRef]
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef]
- Lange, P.; Marott, J.L.; Vestbo, J.; Olsen, K.R.; Ingebrigtsen, T.S.; Dahl, M.; Nordestgaard, B.G. Prediction of the clinical course of chronic obstructive pulmonary disease, using the new GOLD classification: A study of the general population. Am. J. Respir. Crit. Care Med. 2012, 186, 975–981. [Google Scholar] [CrossRef]
- Celli, B.R.; Decramer, M.; Wedzicha, J.A.; Wilson, K.C.; Agustí, A.A.; Criner, G.J.; MacNee, W.; Make, B.J.; Rennard, S.I.; Stockley, R.A.; et al. An official American Thoracic Society/European Respiratory Society statement: Research questions in COPD. Eur. Respir. Rev. 2015, 24, 159–172. [Google Scholar] [CrossRef] [Green Version]
- Sin, D.D.; Vestbo, J. Biomarkers in chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2009, 6, 543–545. [Google Scholar] [CrossRef] [Green Version]
- Mannino, D.M. Biomarkers in COPD: The search continues! Eur. Respir. J. 2015, 45, 872–874. [Google Scholar] [CrossRef] [Green Version]
- Agustí, A.; Celli, B.; Faner, R. What does endotyping mean for treatment in chronic obstructive pulmonary disease? Lancet 2017, 390, 980–987. [Google Scholar] [CrossRef]
- Gon, Y.; Shimizu, T.; Mizumura, K.; Maruoka, S.; Hikichi, M. Molecular techniques for respiratory diseases: MicroRNA and extracellular vesicles. Respirology 2020, 25, 149–160. [Google Scholar] [CrossRef] [Green Version]
- Théry, C.; Witwer, K.W.; Aikawa, E.; Alcaraz, M.J.; Anderson, J.D.; Andriantsitohaina, R.; Antoniou, A.; Arab, T.; Archer, F.; Atkin-Smith, G.K.; et al. Minimal information for studies of extracellular vesicles 2018 (MISEV2018): A position statement of the International Society for Extracellular Vesicles and update of the MISEV2014 guidelines. J. Extracell Vesicles 2018, 7, 1535750. [Google Scholar] [CrossRef] [Green Version]
- Nieri, D.; Neri, T.; Petrini, S.; Vagaggini, B.; Paggiaro, P.; Celi, A. Cell-derived microparticles and the lung. Eur. Respir. Rev. 2016, 25, 266–277. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.J.; Baek, M.; Gusev, Y.; Brackett, D.J.; Nuovo, G.J.; Schmittgen, T.D. Systematic evaluation of microRNA processing patterns in tissues, cell lines, and tumors. RNA 2007, 14, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Diniz, G.P.; Wang, D.-Z. Regulation of Skeletal Muscle by microRNAs. In Comprehensive Physiology; Terjung, R., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2016; ISBN 978-0-470-65071-4. [Google Scholar]
- Schwarzenbach, H.; Nishida, N.; Calin, G.A.; Pantel, K. Clinical relevance of circulating cell-free microRNAs in cancer. Nat. Rev. Clin. Oncol. 2014, 11, 145–156. [Google Scholar] [CrossRef]
- Pritchard, C.C.; Cheng, H.H.; Tewari, M. MicroRNA profiling: Approaches and considerations. Nat. Rev. Genet. 2012, 13, 358–369. [Google Scholar] [CrossRef]
- Crist, C.G.; Buckingham, M. microRNAs gain magnitude in muscle. Cell Cycle 2009, 8, 3627–3628. [Google Scholar] [CrossRef]
- Siracusa, J.; Koulmann, N.; Banzet, S. Circulating myomiRs: A new class of biomarkers to monitor skeletal muscle in physiology and medicine. J. Cachexia Sarcopenia Muscle 2018, 9, 20–27. [Google Scholar] [CrossRef]
- Barreiro, E. The role of MicroRNAs in COPD muscle dysfunction and mass loss: Implications on the clinic. Expert Rev. Respir. Med. 2016, 10, 1011–1022. [Google Scholar] [CrossRef]
- Shigeyasu, K.; Toden, S.; Zumwalt, T.J.; Okugawa, Y.; Goel, A. Emerging Role of MicroRNAs as Liquid Biopsy Biomarkers in Gastrointestinal Cancers. Clin. Cancer Res. 2017, 23, 2391–2399. [Google Scholar] [CrossRef] [Green Version]
- Maltais, F.; Decramer, M.; Casaburi, R.; Barreiro, E.; Burelle, Y.; Debigaré, R.; Dekhuijzen, P.N.R.; Franssen, F.; Gayan-Ramirez, G.; Gea, J.; et al. An official American Thoracic Society/European Respiratory Society statement: Update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2014, 189, e15–e62. [Google Scholar] [CrossRef] [Green Version]
- Neri, T.; Tavanti, L.; De Magistris, S.; Lombardi, S.; Romei, C.; Falaschi, F.; Paggiaro, P.; Celi, A. Endothelial Cell-Derived Extracellular Vesicles as Potential Biomarkers in Chronic Interstitial Lung Diseases. Ann. Clin. Lab. Sci. 2019, 49, 608–610. [Google Scholar]
- Petrini, S.; Neri, T.; Lombardi, S.; Cordazzo, C.; Balìa, C.; Scalise, V.; Paggiaro, P.; Pedrinelli, R.; Celi, A. Leptin induces the generation of procoagulant, tissue factor bearing microparticles by human peripheral blood mononuclear cells. Biochim. Biophys. Acta 2016, 1860, 1354–1361. [Google Scholar] [CrossRef] [Green Version]
- Carpi, S.; Scoditti, E.; Massaro, M.; Polini, B.; Manera, C.; Digiacomo, M.; Esposito Salsano, J.; Poli, G.; Tuccinardi, T.; Doccini, S.; et al. The Extra-Virgin Olive Oil Polyphenols Oleocanthal and Oleacein Counteract Inflammation-Related Gene and miRNA Expression in Adipocytes by Attenuating NF-κB Activation. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, D.W.; Sherman, B.T.; Lempicki, R.A. Systematic and integrative analysis of large gene lists using DAVID bioinformatics resources. Nat. Protoc. 2009, 4, 44–57. [Google Scholar] [CrossRef]
- Vogelmeier, C.; Vestbo, J. COPD assessment: I, II, III, IV and/or A, B, C, D. Eur. Respir. J. 2014, 43, 949–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polini, B.; Carpi, S.; Romanini, A.; Breschi, M.C.; Nieri, P.; Podestà, A. Circulating cell-free microRNAs in cutaneous melanoma staging and recurrence or survival prognosis. Pigment. Cell Melanoma Res. 2019, 32, 486–499. [Google Scholar] [CrossRef] [PubMed]
- Horak, M.; Novak, J.; Bienertova-Vasku, J. Muscle-specific microRNAs in skeletal muscle development. Dev. Biol. 2016, 410, 1–13. [Google Scholar] [CrossRef]
- Sun, Y.; An, N.; Li, J.; Xia, J.; Tian, Y.; Zhao, P.; Liu, X.; Huang, H.; Gao, J.; Zhang, X. miRNA-206 regulates human pulmonary microvascular endothelial cell apoptosis via targeting in chronic obstructive pulmonary disease. J. Cell. Biochem. 2019, 120, 6223–6236. [Google Scholar] [CrossRef]
- Puig-Vilanova, E.; Aguiló, R.; Rodríguez-Fuster, A.; Martínez-Llorens, J.; Gea, J.; Barreiro, E. Epigenetic mechanisms in respiratory muscle dysfunction of patients with chronic obstructive pulmonary disease. PLoS ONE 2014, 9, e111514. [Google Scholar] [CrossRef]
- Barreiro, E.; Sancho-Muñoz, A.; Puig-Vilanova, E.; Salazar-Degracia, A.; Pascual-Guardia, S.; Casadevall, C.; Gea, J. Differences in micro-RNA expression profile between vastus lateralis samples and myotubes in COPD cachexia. J. Appl. Physiol. 2019, 126, 403–412. [Google Scholar] [CrossRef]
- Donaldson, A.; Natanek, S.A.; Lewis, A.; Man, W.D.-C.; Hopkinson, N.S.; Polkey, M.I.; Kemp, P.R. Increased skeletal muscle-specific microRNA in the blood of patients with COPD. Thorax 2013, 68, 1140–1149. [Google Scholar] [CrossRef] [Green Version]
- Lewis, A.; Riddoch-Contreras, J.; Natanek, S.A.; Donaldson, A.; Man, W.D.-C.; Moxham, J.; Hopkinson, N.S.; Polkey, M.I.; Kemp, P.R. Downregulation of the serum response factor/miR-1 axis in the quadriceps of patients with COPD. Thorax 2012, 67, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Yuasa, K.; Hagiwara, Y.; Ando, M.; Nakamura, A.; Takeda, S.; Hijikata, T. MicroRNA-206 is highly expressed in newly formed muscle fibers: Implications regarding potential for muscle regeneration and maturation in muscular dystrophy. Cell Struct. Funct. 2008, 33, 163–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cacchiarelli, D.; Legnini, I.; Martone, J.; Cazzella, V.; D’Amico, A.; Bertini, E.; Bozzoni, I. miRNAs as serum biomarkers for Duchenne muscular dystrophy. EMBO Mol. Med. 2011, 3, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-F.; Tao, Y.; Li, J.; Deng, Z.; Yan, Z.; Xiao, X.; Wang, D.-Z. microRNA-1 and microRNA-206 regulate skeletal muscle satellite cell proliferation and differentiation by repressing Pax7. J. Cell Biol. 2010, 190, 867–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, N.; Williams, A.H.; Maxeiner, J.M.; Bezprozvannaya, S.; Shelton, J.M.; Richardson, J.A.; Bassel-Duby, R.; Olson, E.N. microRNA-206 promotes skeletal muscle regeneration and delays progression of Duchenne muscular dystrophy in mice. J. Clin. Investig. 2012, 122, 2054–2065. [Google Scholar] [CrossRef] [Green Version]
- Pinkerton, M.; Chinchilli, V.; Banta, E.; Craig, T.; August, A.; Bascom, R.; Cantorna, M.; Harvill, E.; Ishmael, F.T. Differential expression of microRNAs in exhaled breath condensates of patients with asthma, patients with chronic obstructive pulmonary disease, and healthy adults. J. Allergy Clin. Immunol. 2013, 132, 217–219. [Google Scholar] [CrossRef]
- Agusti, A.; Edwards, L.D.; Celli, B.; Macnee, W.; Calverley, P.M.A.; Müllerova, H.; Lomas, D.A.; Wouters, E.; Bakke, P.; Rennard, S.; et al. Characteristics, stability and outcomes of the 2011 GOLD COPD groups in the ECLIPSE cohort. Eur. Respir. J. 2013, 42, 636–646. [Google Scholar] [CrossRef] [Green Version]
- Agustí, A.; Edwards, L.D.; Rennard, S.I.; MacNee, W.; Tal-Singer, R.; Miller, B.E.; Vestbo, J.; Lomas, D.A.; Calverley, P.M.A.; Wouters, E.; et al. Persistent systemic inflammation is associated with poor clinical outcomes in COPD: A novel phenotype. PLoS ONE 2012, 7, e37483. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A (n = 4) | Group B (n = 9) | Group C (n = 8) | Group D (n = 14) | p-Value | |
|---|---|---|---|---|---|
| Male/Female | 4/0 | 6/3 | 8/0 | 8/6 | n.s. |
| Age (yrs) | 74.5 (10.0) | 70.0 (12.0) | 68 (12.0) | 71.5 (3.0) | n.s. |
| Smoking status (current/former) | 1/3 | 5/4 | 0/8 | 3/11 | n.s. |
| Pack-years | 39.0 (60.0) | 52.0 (18.5) | 50.0 (60.5) | 48.5 (33.0) | n.s. |
| Dyspnea, mMRC | 1.0 (1.0) | 1.0 (1.0) | 1.0 (1.0) | 2.0 (1.0) | 0.002 * |
| CAT | 7.5 (2.5) | 11.0 (6.0) | 8.0 (9.3) | 14.0 (9.5) | 0.003 * |
| BMI, Kg/m2 | 26.7 (10.3) | 31.7 (11.4) | 29.2 (7.5) | 27.4 (7.3) | n.s. |
| FEV1, L % pred. | 1.52 (0.59) 62.5 (30.0) | 1.65 (0.53) 62.0 (9.5) | 1.37 (0.46) 47.0 (17.3) | 0.99 (0.45) 50.0 (16.5) | 0.001 ° 0.004 ° |
| FEV1/FVC % | 52.0 (17.5) | 53.0 (15.5) | 42.5 (18.0) | 45.1 (16.0) | n.s. |
| DLCO, mL/min * mmHg % pred. | 16.9 (9.7) 84.0 (59.5) | 14.0 (8.7) 55.0 (29.5) | 24.5 (7.3) 96.5 (33.3) | 14.6 (8.6) 59.5 (17.0) | n.s. n.s. |
| Therapy | n.a. | ||||
| LAMA | 1 | ||||
| LABA-LAMA | 2 | 4 | 3 | 6 | |
| LABA-ICS | 1 | 1 | 1 | ||
| TRIPLE TH. | 2 | 4 | 2 | 7 | |
| LABA | 1 |
| EV-Derived Myo-miRna | AUC | 95% CI | p Value |
|---|---|---|---|
| GOLD Group B vs C | |||
| miR-206 | 78.89% | 63.4–93.7% | <0.0813 |
| miR-133a-5p | 75.33% | 55.2–88.4% | 0.0063 |
| miR-133a-3p.2 | 73.96% | 54.1–89.5% | 0.3533 |
| Triple signature | 89.74% | 70.8–92% | <0.0008 |
| GOLD Group B vs A | |||
| miR-206 | 78.74% | 51.5–90.6% | 0.0044 |
| miR-133a-5p | 83.82% | 52–92.5% | 0.0001 |
| miR-133a-3p.2 | 87.5% | 62.5–87.5% | 0.1709 |
| Triple signature | 83.9% | 58.5–91.6% | <0.0001 |
| GOLD Group B vs D | |||
| miR-206 | 67.09% | 49.5–80.2% | 0.0134 |
| miR-133a-5p | 73.41% | 55.7–86.9% | 0.0005 |
| miR-133a-3p.2 | 61.46% | 45.2–77% | 0.6595 |
| Triple signature | 69.4% | 53.8–83.4% | <0.0042 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carpi, S.; Polini, B.; Nieri, D.; Dubbini, N.; Celi, A.; Nieri, P.; Neri, T. Expression Analysis of Muscle-Specific miRNAs in Plasma-Derived Extracellular Vesicles from Patients with Chronic Obstructive Pulmonary Disease. Diagnostics 2020, 10, 502. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070502
Carpi S, Polini B, Nieri D, Dubbini N, Celi A, Nieri P, Neri T. Expression Analysis of Muscle-Specific miRNAs in Plasma-Derived Extracellular Vesicles from Patients with Chronic Obstructive Pulmonary Disease. Diagnostics. 2020; 10(7):502. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070502
Chicago/Turabian StyleCarpi, Sara, Beatrice Polini, Dario Nieri, Nevio Dubbini, Alessandro Celi, Paola Nieri, and Tommaso Neri. 2020. "Expression Analysis of Muscle-Specific miRNAs in Plasma-Derived Extracellular Vesicles from Patients with Chronic Obstructive Pulmonary Disease" Diagnostics 10, no. 7: 502. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070502