1. Introduction
To date, there are no doubts that the earlier a child’s problems in the cognitive and psychomotor development are detected, the higher the chances for timely intervention and changing the potential trajectory of his/her development. A temporary delay in the acquisition of cognitive, sensory and motor skills can be caused by various neurodevelopmental disorders [
1], and quite often is burdened by autistic-like symptoms [
2]. The problem of developmental delay (DD) at an early age needs precise consideration, since such children are at higher risk for mental disorders, compared with typically developing peers [
3]. Also, behavioral disorders affect about 50% of children with DD or at risk for DD at the age of 2–3 years [
4], and this tendency worsens over time if there is the absence of appropriate corrective interventions [
5]. Burdening DD with autistic-like symptoms is a prognostic adverse circumstance. Symptoms of autistic spectrum disorder (ASD) are diverse and most often include various patterns of sensory disintegration, propensities to stereotyped movements and a limited behavioral repertoire. The task of diagnosing and quantifying children with ASD is difficult to implement primarily due to heterogeneity of symptoms, the absence of biological diagnostic markers and changes in diagnostic criteria [
6]. A progress in early detection symptoms of ASD and following intervention can significantly improve the social adaptation of affected children. Therefore, more research has recently been devoted to the study of the predictors of ASD outcomes and the actual needs of adolescents and adults with autism [
7,
8].
Screening tools developed in the West for children with DD and ASD differ in their methodology. In the first case, such screenings of children’s mental development as Griffiths, Denver, Vineland are widely used [
9,
10]. To identify ASD, questionnaires and observation sheets for cognitive and adaptive behavior are mainly used, for example, ADOS (Autism Diagnostic Observation Schedule) [
11] and ADI-R (Autism Diagnostic Interview-Revised) [
12]. In Russia, however, there is no diagnostic screening developed for a sample of Russian children for early identification of problems or deviations in mental development. The complexity of translation and adaptation of Western methods is comparable to the elaboration of a new diagnostic tool, while the problem of taking into account the specifics of Russian children’s cognitive development is not solved, not to mention the cost of a license to use foreign screening. Therefore, we set out to create screening scales for early detection of possible problems in the cognitive and psychomotor development of children and differentiation of children into typically developing and ones who need the attention of specialists. Utilizing these early screening diagnostics, which take up to 20–30 min and can be carried out both at preschool educational institutions and at district clinics, we plan to optimize the process of early intervention and “unload” specialists, giving them the opportunity to work with children who really need special attention.
In one of the most well-known and widely used Western screenings, Denver [
9], child development is evaluated by the following domains, implying that these areas are development vectors and related to the factor structure of intelligence: (1) large and fine motor skills; (2) speech development; and (3) communication and social adaptation. Similar scales were identified earlier in the elaboration of screening tools for early diagnosis of DD, and included 3 scales for 4–5-year-olds: “Logical reasoning”, “Motor skills” and “General awareness”. These scales coincided in content for children of these age groups, but differed in the task sets: for 4-year-olds - simpler, for 5-year-olds - more complex) [
13].
In this study, we aimed to develop analogous scales for 3-year-olds. We paid attention to this age last because of the difficulties in data collection for samples of children with DD and ASD, since children in Russia only begin to attend preschool institutions at this age. Respectively, it is only from this age that children with developmental problems come to the attention of specialists and may be assessed as belonging to DD or ASD groups. In this regard, over the past 4 years of the study, the sample of 3-year-olds with established developmental problems consisted of only 26 children with DD and 23 children with ASD, which is almost 3 times less than the number of children in older groups. Due to the small sample sizes of children with DD and ASD in this study, in contrast to the previous ones, the development of scales was carried out on a sample of children without a diagnosis (belonging to Norm group), and data on children with DD and ASD was used to test the discriminative validity of the selected scales. However, we assumed that our research for 3-year-olds would reveal scales similar to those we obtained for older children, correlating with Denver screening, and including at least such factors as “General awareness”, “Motor skills”, and “Logical reasoning”.
2. Materials and Methods
In total, 840 3-year-olds were examined, evenly represented in the age range from 1095 to 1459 calendar days. Of these, the main sample consisted of 814 typically developing children (group “Norm”). A sample of 26 children with DD was used to test the discriminative validity of the developed scales. A sample of 23 children with ASD was used to analyze the applicability of the existing tasks bank (tasks, formalized observations) and determine the need to supplement to the tasks bank, as well as check the functionality of the software, taking into account the specialists’ feedbacks. Diagnosis of the children (including assignment to the Norm, DD or ASD groups) was carried out by experienced specialists from psychological counseling centers and pre-school institutions with the participation of neurologists, psychologists, psychiatrists before the survey. Data collection was carried out by tutors and psychologists engaged in psychological and pedagogical support of children in ordinary and special preschool institutions (Saint Petersburg and its region, Rostov-on-don and Murmansk). Diagnosis was carried out as a part of children’s routine examinations, after receiving written parental consent. The data was collected in 26 preschool institutions using the computer system “Longitude” (Software Longitude, Version 19, production of LLC “Longitude”, S-Petersburg, Russia) [
14], as previously for elder children [
13,
15,
16]. “Longitude” is regularly used in these institutions for annual surveys. The study used all the results of diagnostics of 3-year-old children, including children without a diagnosis (group Norm) and with an assessed diagnosis (groups DD/ASD), in the period from 2015 to 2019. The data was transmitted to us in an impersonal form.
“Longitude” software included a large bank of tasks, presented in accordance with the child’s calendar age, and aimed at estimating a wide range of abilities in primary domains such as motor skills, social adaptation, and cognitive abilities. A psychologist worked with the child, conducted the evaluations, and filled out the test’s electronic forms. To collect data in different conditions, offline and online versions of the program have been developed that allowed obtaining quickly representative data from different regions of Russia. Herewith, for all the participants the same standardized instructions and stimulus materials were used as a part of the software during the process of data collection. The software choice as the main form of implementation of the data collection was due to both the described data collection capabilities at the research stage, and the literature data on the higher efficiency of computer techniques in their application. The choice of data collection computerized form was due to the greater practicality and simplicity of implementation, but also, to the higher efficiency of application. For example, Carroll et al. showed that the use of computer-based cognitive development screenings for the purpose of detecting DD significantly increased the number of children diagnosed and those ones whose development was corrected timely at an early age [
17].
The content of the questions and tasks was typical for screenings and development tests, but at the same time very versatile, since the bank of tasks was created as the result of a survey of a large number of expert practitioner psychologists. In this study, the “Longitude” software was used only as a tool to collect raw data for subsequent analysis, without taking into account the grouping of tasks in the structure of the original method; thus we worked with completely “clean” data, not distorted by the a priori subtest or factor structure of the method used.
The initial tasks bank included 502 tasks for children aged from 2 months to 7 years of which tasks relevant for 3-year-olds were selected. As a result of reducing the responses to tasks to a uniform dichotomous form, the initial data for analysis included 847 dichotomous items: 1-cannot perform, 2-can perform. The full content of items, tasks and stimuli materials is presented on the project’s website
http://info11.testpsy.net/.
Statistical analysis was performed for the following purposes: (1) identification of scales which have factor validity and sufficiently high reliability for the “Norm” sample; (2) selection of scales that have the highest discriminative validity according to the “Norm–DD” criterion (diagnosis), validity in content; (3) interpretation of the relationships between scales-predictors, age and their relative contribution to the prediction of the diagnosis; and (4) standardization of the scales for 3-year-olds (the “Norm” sample). Statistical analysis was performed using IBM SPSS Statistics and AMOS 25 version (IBM Corp. Released 2017. IBM SPSS Statistics & AMOS for Windows, Version 25.0. Armonk, NY, USA).
4. Discussion
This work became the next stage of our long-term research based on psychometric approach in elaboration screening tools. When developing this screening, we strictly adhered to the current recommendations for the psychometric tools standards in the test construction concerning such properties as reliability and specificity [
22]. Looking forward, procedures of the screening standardization and accuracy computations will be our next steps. In order to avoid common biases in screening test elaboration [
23], we carried out our research on a huge sample, used initially wide range of test tasks to face possible non-equivalent test bias and the process of data collection was strictly identical for each participant to prevent a procedural bias. However, the weak point of our research is a relatively small number of children assessed with a diagnosis (DD/ASD), understood as a spectrum bias, which is reflected in the limitations section and which nonetheless can be partially overcome by the large sample size and high reliability and specificity of the forecast. Discussing the results, first of all, it should be emphasized that the elaborated screening scales can only be used for early diagnosis of children with DD without autistic-like symptoms presence after required standardization and validation procedures. Tasks in the scales assume the child’s ability to social interaction at the level of instruction understanding and its implementation. For children with autistic-like symptoms, first comes a lack of social interaction [
24], limitations in the instructions understanding [
25], repetitive behaviours with elements of self-stimulation [
26], and stimulus overselectivity in relation to relevant stimulus [
27]. In addition, these children often show a refusal to cooperate in a new environment with new people [
28]. For early detection of autistic-like developmental disorders, it is necessary to evaluate the child’s behavioral and cognitive skills using parental questionnaires and check-lists of spontaneous behavioural activity of the child.
It is important to note that the identified structure of scales for 3-year-olds is similar to the previously identified scales sets for 4- and 5-year-olds [
13], according to the factors of logical reasoning, motor development and general awareness, but differs from the previously identified scales sets for 6-year-olds, where the most important factors in predicting the diagnosis were sustained attention and counting [
29]. For 3-year-olds, the executive functions factor is additionally allocated. At the same time, the obtained models correspond to the Denver screening [
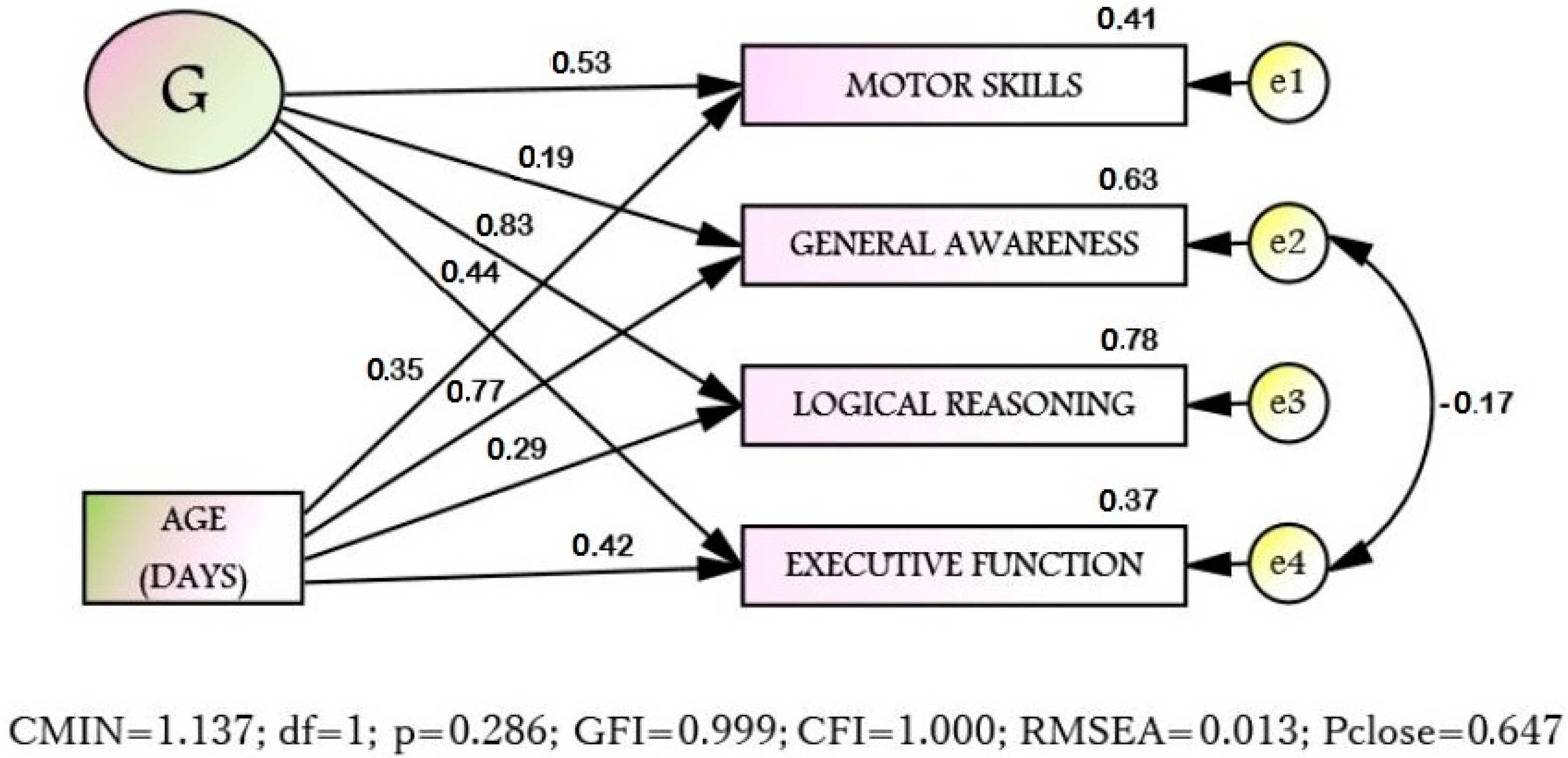
9] for motor development factor; speech development and communication presented in the Western screening in our model correspond to the General awareness factor, which assumes speech development of the child sufficient enough to expand his/her world comprehension and form communication at a level that allows to accumulate verbal knowledge; social adaptation in our models is not represented. However, for each age, the factor of Logical reasoning was additionally identified, and for 3-year-olds, the factor of Executive functions, which in fact reflects the structural and functional maturation of the brain and can be considered as the necessary neurophysiological basis for adaptive behavior. The weak negative link between errors (residuals) in the model (see
Figure 1) connecting “General Awareness” and “Executive functions” can be explained as follows: when a child has a delay in a maturation of the frontal cortex, which is reflected in an underdevelopment of executive functions [
30,
31], the main compensatory mechanism for children with DD is the mastering of verbal abilities and first of all an expansion of general awareness [
32].
The differences between typically developing children and children with a DD for 3-year-olds on each of the obtained scales are very significant (Cohen’s d >> 0.80). Thus, there is strong evidence in favor of the scales discriminative validity based on the criterion of differentiation of Norm/DD groups. The largest differences were found on the scales “Logical reasoning” and “Motor skills”, the smallest–on the scale “General awareness”. It is important to note that similar results were obtained for 4- and 5-year-olds: the greatest contribution to the differentiation of the groups Norm/DD for each age was implemented by the Logical reasoning factor, the smallest although significant, by General awareness factor [
13]. This result was quite expected, as it is known that the ability to reason logically belongs to the structure of nonverbal intelligence, reflects general intellectual abilities, and is largely due to biological inclinations and heredity, and, accordingly, is subject to training to a much lesser extent than verbal abilities. On the other hand, the smallest differences between groups for each age were obtained on the “General awareness” scale, which is also quite natural. The process of forming and expanding the child’s awareness about the world primarily reflects the time spent on classes with the child and is in fact the process of an information accumulation. This process can occur without additional comprehension or logical processing if they are beyond the child’s present capabilities, but if there are sufficient resources for memorization, often mechanical ones.
Structural equation modeling (
Figure 1) of the structure of the scales relationship with the age shows that the 4 selected scales are indicators of the General intelligence factor (G). Likewise for 4–5-year-olds, the age does not inflict a direct effect on General intelligence, but affects its indicators (scales) in different ways. It was found that the age has the greatest influence on “General awareness” (S2), while G factor has the least influence on “General awareness” (S2). “General awareness” traditionally refers to verbal abilities, while it is obvious that the older the child becomes, the wider his/her knowledge of the world, so the age naturally affects the development of General awareness. However, G factor, responsible for the success of intellectual tasks in general, affected General awareness to the least extent. This is probably due to the fact that General awareness is subject to training to the greatest extent and cannot serve as a reflection of a child’s general intellectual abilities. At the same time, the greatest contribution of factor G is observed in “Logical reasoning” (S3), an ability primarily related to non-verbal intelligence, reflecting the child’s highly inherited abilities, which are subject to training to a much lesser extent than verbal abilities. Interestingly, the influence of the age on “Logical reasoning” (S3) for 3-year-olds is minimal, which supports nativist theories that assume that a child has a certain set of innate abilities, the development of which is due to the deployment of genetic programs [
33] and by this age this ability is already represented in the structure of intelligence.
The fact that the scale values significantly correlate with the age in days was taken into account when developing test norms by introducing an adjustment for the child’s age in days using the linear regression model. As a result, for the same number of correctly completed tasks, the scale values for younger 3-year-old children are higher than those for older ones. The developed test norms demonstrate a high accuracy of more than 90% for distinguishing the Norm and DD groups.
5. Conclusions
The main result of our current research is the elaboration of a high-precise (at least 90%) rapid DD diagnosis in 3-year-olds, which allows identifying quickly the “risk group” for further clarification of the diagnosis and an educational route calculation. The expected accuracy of the prediction when using the elaborated screening is significantly higher than that in known sources (more than 90%). For example, Dawson [
9], in the article on testing Denver screening in clinical practice, found a prediction accuracy of less than 70% sufficient. It was found out that the scales for 3-year-olds, as the areas in which the Norm and DD samples differ most strongly, are broadly similar to the scales obtained for older preschoolers, and the most significant differences are shown in the scales “Logical reasoning” and “Motor skills”.
The study also showed that the initially wide range of used tasks is not adequate for diagnosing children with ASD. As was shown by the preliminary analysis of the data, the tasks suitable for children with DD gave an uncertain result for the children with ASD. Thus, for the diagnosis of ASD, more specific features should be considered such as the characteristics of behavior, social interaction and perception, information about which can be obtained from a survey of the child’s immediate environment. Thereby, the development of methods for rapid diagnostics of children with ASD is our next immediate task. The applied result of solving this problem should be creation of an online screening system for the diagnosis and differentiation of these developmental problems, developed on the basis of the current version of the research software and available to specialists of educational and medical institutions.






{kind=link}
{kind=link}