Diagnostic Task Specific Activations in Functional MRI and Aberrant Connectivity of Insula with Middle Frontal Gyrus Can Inform the Differential Diagnosis of Psychosis

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Image Acquisition
2.3. fMRI Task
2.4. MRI Data Analysis
2.4.1. Structural Data Analysis—Voxel-Based Morphometry (VBM)
2.4.2. Task-Related Functional Data Analysis
2.4.3. Resting State Data Analysis—Effective Connectivity
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Voxel-Based Morphometry Analysis
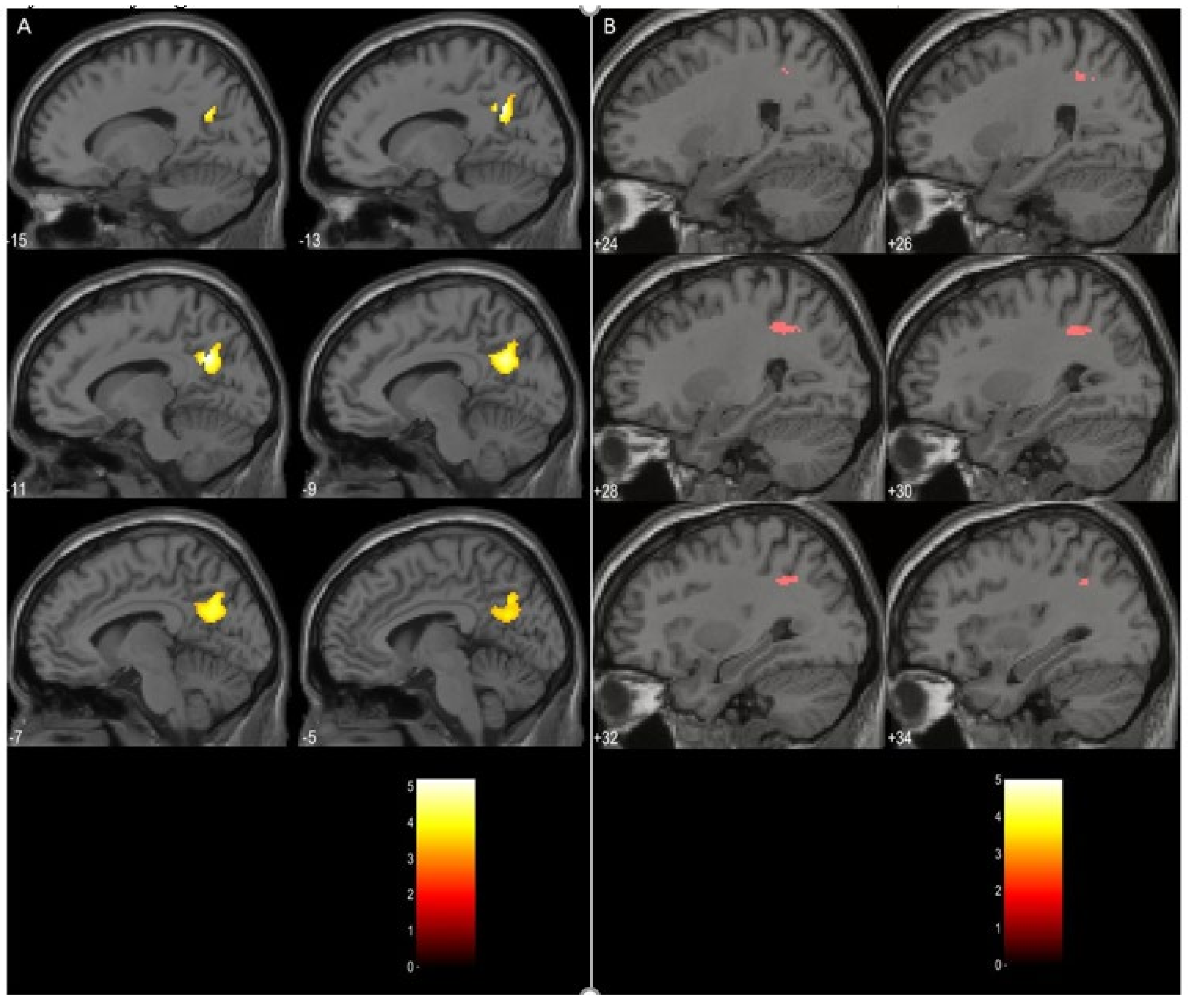
3.3. Task Related Data Analysis
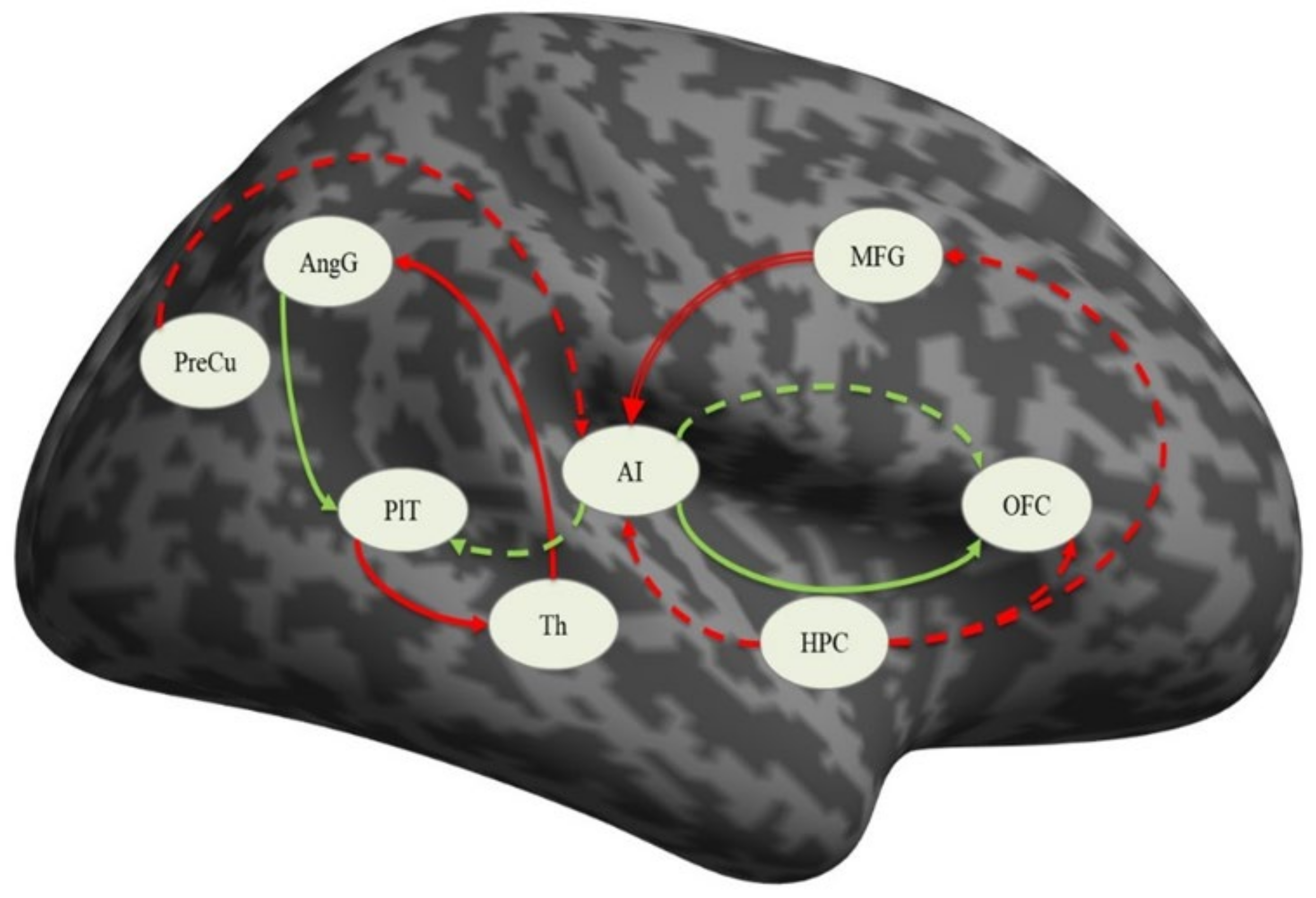
3.4. Effective Connectivity Analysis
3.4.1. Effective Connectivity in the Sample
3.4.2. Effective Connectivity in the Schizophrenia Group
3.4.3. Effective Connectivity in the Depressed Group
3.4.4. Differences between Schizophrenic and Depressed Patients
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Whiteford, H.A.; Degenhardt, L.; Rehm, J.; Baxter, A.J.; Ferrari, A.J.; Erskine, H.E.; Charlson, F.J.; Norman, R.E.; Flaxman, A.D.; Johns, N.; et al. Global burden of disease attributable to mental and substance use disorders: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1575–1586. [Google Scholar] [CrossRef]
- Zhdanava, M.; Kuvadia, H.; Joshi, K.; Daly, E.; Pilon, D.; Rossi, C.; Morrison, L.; Lefebvre, P.; Nelson, C. Economic burden of treatment-resistant depression in privately insured US patients with co-occurring anxiety disorder and/or substance use disorder. Curr. Med. Res. Opin. 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, J.L.; Altar, C.A.; Taylor, D.L.; Degtiar, I.; Hornberger, J.C. The social and economic burden of treatment-resistant schizophrenia: A systematic literature review. Int. Clin. Psychopharmacol. 2014, 29, 63–76. [Google Scholar] [CrossRef] [PubMed]
- Mistry, S.; Harrison, J.R.; Smith, D.J.; Escott-Price, V.; Zammit, S. The use of polygenic risk scores to identify phenotypes associated with genetic risk of bipolar disorder and depression: A systematic review. J. Affect. Disord. 2018, 234, 148–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legge, S.E.; Jones, H.J.; Kendall, K.M.; Pardiñas, A.F.; Menzies, G.; Bracher-Smith, M.; Escott-Price, V.; Rees, E.; Davis, K.A.S.; Hotopf, M.; et al. Association of Genetic Liability to Psychotic Experiences With Neuropsychotic Disorders and Traits. JAMA Psychiatry 2019, 76, 1256–1265. [Google Scholar] [CrossRef] [Green Version]
- Fusar-Poli, P.; Smieskova, R.; Serafini, G.; Politi, P.; Borgwardt, S. Neuroanatomical markers of genetic liability to psychosis and first episode psychosis: A voxelwise meta-analytical comparison. World J. Biol. Psychiatry 2014, 15, 219–228. [Google Scholar] [CrossRef]
- Mullins, N.; Bigdeli, T.B.; Børglum, A.D.; Coleman, J.R.I.; Demontis, D.; Mehta, D.; Power, R.A.; Ripke, S.; Stahl, E.A.; Starnawska, A.; et al. GWAS of Suicide Attempt in Psychiatric Disorders and Association With Major Depression Polygenic Risk Scores. Am. J. Psychiatry 2019, 176, 651–660. [Google Scholar] [CrossRef]
- Serafini, G.; Pompili, M.; Haghighat, R.; Pucci, D.; Pastina, M.; Lester, D.; Angeletti, G.; Tatarelli, R.; Girardi, P. Stigmatization of schizophrenia as perceived by nurses, medical doctors, medical students and patients. J. Psychiatr. Ment. Health Nurs. 2011, 18, 576–585. [Google Scholar] [CrossRef]
- Americans, N.; Article, S.; Haghir, H.; Mokhber, N.; Azarpazhooh, M.R.; Haghighi, M.B.; Radmard, M.; It, B.; Bank, T.W.; Adjusted, D.; et al. The ICD-10 Classification of Mental and Behavioural Disorders. IACAPAP E-Textb. Child Adolesc. Ment. Health 2013, 55, 135–139. [Google Scholar]
- Wakefield, J.C. DSM-5: An Overview of Changes and Controversies. Clin. Soc. Work J. 2013, 41, 139–154. [Google Scholar] [CrossRef]
- Brunoni, A.R. Beyond the DSM: Trends in Psychiatry Diagnoses. Arch Clin Psychiatry. 2017, 44, 154–158. [Google Scholar] [CrossRef] [Green Version]
- Stoyanov, D.; Kandilarova, S.; Paunova, R.; Barranco Garcia, J.; Latypova, A.; Kherif, F. Cross-Validation of Functional MRI and Paranoid-Depressive Scale: Results From Multivariate Analysis. Front. Psychiatry 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Todeva-Radneva, A.; Paunova, R.; Kandilarova, S.; St. Stoyanov, D. The Value of Neuroimaging Techniques in the Translation and Transdiagnostic Validation of Psychiatric Diagnoses—Selective Review. Curr. Top. Med. Chem. 2020, 20, 540–553. [Google Scholar] [CrossRef] [PubMed]
- Specht, K. Current Challenges in Translational and Clinical fMRI and Future Directions. Front. Psychiatry 2020, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoyanov, D.; Kandilarova, S.; Borgwardt, S.; Stieglitz, R.-D.; Hugdahl, K.; Kostianev, S. Psychopathology Assessment Methods Revisited: On Translational Cross-Validation of Clinical Self-Evaluation Scale and fMRI. Front. Psychiatry 2018, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoyanov, D.S. AS09-02—Translational cross-validation among neuroscience and psychiatry: Prospects for diagnostic assessment and psychopharmacology. Eur. Psychiatry 2012, 27, 17. [Google Scholar] [CrossRef]
- Aryutova, K.; Kandilarova, S.; Todeva-Radneva, A.; Stoyanov, D. Clinical Use of Neurophysiological Biomarkers and Self-Assessment Scales to Predict and Monitor Treatment Response for Psychotic and Affective disorders. Curr. Pharm. Des. 2021; in press. [Google Scholar]
- Stoyanov, D.; Kandilarova, S.; Arabadzhiev, Z.; Paunova, R.; Schmidt, A.; Borgwardt, S. Cross-Validation of Paranoid-Depressive Scale and Functional MRI: New Paradigm for Neuroscience Informed Clinical Psychopathology. Front. Psychiatry 2019, 10. [Google Scholar] [CrossRef] [Green Version]
- von Zerssen, D. Clinical Self-Rating Scales (CSRS) of the Munich Psychiatric Information System (PSYCHIS München). In Assessment of Depression; Springer: Berlin/Heidelberg, Germany, 1986. [Google Scholar]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; Text Revision; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Sullivan, H.S. The Psychiatric Interview; W. W. Norton & Co.: Oxford, UK, 1954. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. S20), 22–33. [Google Scholar]
- Clinical Global Impressions Scale (CGI). Simple Pract. Ment. Health. Available online: https://simpleandpractical.com/clinical-global-impressions-scale-cgi/ (accessed on 30 November 2020).
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Bell, C.C. DSM-IV: Diagnostic and Statistical Manual of Mental Disorders. JAMA 1994, 272, 828–829. [Google Scholar] [CrossRef]
- Stoyanov, D.; Kandilarova, S.; Sirakov, N.; Stoeva, M.; Velkova, K. Psychiatry in crisis: Potentialities of translational functional neuroimaging. Bulg. J. Psychiatry 2017, 2, 134–141. [Google Scholar]
- Bora, E.; Fornito, A.; Pantelis, C.; Yücel, M. Gray matter abnormalities in Major Depressive Disorder: A meta-analysis of voxel based morphometry studies. J. Affect. Disord. 2012, 138, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Gur, R.E.; Turetsky, B.I.; Cowell, P.E.; Finkelman, C.; Maany, V.; Grossman, R.I.; Arnold, S.E.; Bilker, W.B.; Gur, R.C. Temporolimbic Volume Reductions in Schizophrenia. Arch. Gen. Psychiatry 2000, 57, 769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gur, R.E.; Cowell, P.E.; Latshaw, A.; Turetsky, B.I.; Grossman, R.I.; Arnold, S.E.; Bilker, W.B.; Gur, R.C. Reduced Dorsal and Orbital Prefrontal Gray Matter Volumes in Schizophrenia. Arch. Gen. Psychiatry 2000, 57, 761. [Google Scholar] [CrossRef]
- Maggioni, E.; Crespo-Facorro, B.; Nenadic, I.; Benedetti, F.; Gaser, C.; Sauer, H.; Roiz-Santiañez, R.; Poletti, S.; Marinelli, V.; Bellani, M.; et al. Common and distinct structural features of schizophrenia and bipolar disorder: The European Network on Psychosis, Affective disorders and Cognitive Trajectory (ENPACT) study. PLoS ONE 2017, 12, e0188000. [Google Scholar] [CrossRef] [Green Version]
- Shao, J.; Meng, C.; Tahmasian, M.; Brandl, F.; Yang, Q.; Luo, G.; Luo, C.; Yao, D.; Gao, L.; Riedl, V.; et al. Common and distinct changes of default mode and salience network in schizophrenia and major depression. Brain Imaging Behav. 2018, 12, 1708–1719. [Google Scholar] [CrossRef]
- Leech, R.; Braga, R.; Sharp, D.J. Echoes of the Brain within the Posterior Cingulate Cortex. J. Neurosci. 2012, 32, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Maddock, R.J.; Garrett, A.S.; Buonocore, M.H. Remembering familiar people: The posterior cingulate cortex and autobiographical memory retrieval. Neuroscience 2001, 104, 667–676. [Google Scholar] [CrossRef]
- Buckner, R.L.; Andrews-Hanna, J.R.; Schactera, L.D. The brain’s default network: Anatomy, function, and relevance to disease. Ann. N. Y. Acad. Sci. 2008, 1124, 1–38. [Google Scholar] [CrossRef] [Green Version]
- The Role of the Posterior Cingulate Cortex in Cognition and Disease. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC3891440/ (accessed on 25 November 2020).
- Nakao, T.; Radua, J.; Rubia, K.; Mataix-Cols, D. Gray matter volume abnormalities in ADHD: Voxel-based meta-analysis exploring the effects of age and stimulant medication. Am. J. Psychiatry 2011, 168, 1154–1163. [Google Scholar] [CrossRef]
- Newell, K.A.; Zavitsanou, K.; Huang, X.-F. Ionotropic glutamate receptor binding in the posterior cingulate cortex in schizophrenia patients. Neuroreport 2005, 16, 1363–1367. [Google Scholar] [CrossRef]
- Lundstrom, B. Isolating the retrieval of imagined pictures during episodic memory: Activation of the left precuneus and left prefrontal cortex. NeuroImage 2003, 20, 1934–1943. [Google Scholar] [CrossRef]
- Lundstrom, B.N.; Ingvar, M.; Petersson, K.M. The role of precuneus and left inferior frontal cortex during source memory episodic retrieval. NeuroImage 2005, 27, 824–834. [Google Scholar] [CrossRef]
- Vogeley, K.; May, M.; Ritzl, A.; Falkai, P.; Zilles, K.; Fink, G.R. Neural correlates of first-person perspective as one constituent of human self-consciousness. J. Cogn. Neurosci. 2004, 16, 817–827. [Google Scholar] [CrossRef]
- Farrow, T.F.; Zheng, Y.; Wilkinson, I.D.; Spence, S.A.; Deakin, J.F.; Tarrier, N.; Griffiths, P.D.; Woodruff, P.W. Investigating the functional anatomy of empathy and forgiveness. Neuroreport 2001, 12, 2433–2438. [Google Scholar] [CrossRef]
- Vatansever, D.; Manktelow, A.E.; Sahakian, B.J.; Menon, D.K.; Stamatakis, E.A. Angular default mode network connectivity across working memory load. Hum. Brain Mapp. 2016, 38, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Seghier, M.L. The Angular Gyrus: Multiple Functions and Multiple Subdivisions. Neuroscientist 2013. [Google Scholar] [CrossRef] [Green Version]
- Farrer, C.; Franck, N.; Frith, C.D.; Decety, J.; Georgieff, N.; d’Amato, T.; Jeannerod, M. Neural correlates of action attribution in schizophrenia. Psychiatry Res. Neuroimaging 2004, 131, 31–44. [Google Scholar] [CrossRef]
- Niznikiewicz, M.; Donnino, R.; McCarley, R.W.; Nestor, P.G.; Iosifescu, D.V.; O’Donnell, B.; Levitt, J.; Shenton, M.E. Abnormal Angular Gyrus Asymmetry in Schizophrenia. AJP 2000, 157, 428–437. [Google Scholar] [CrossRef]
- Sanches, M.; Caetano, S.; Nicoletti, M.; Monkul, E.S.; Chen, H.H.; Hatch, J.P.; Yeh, P.-H.; Mullis, R.L.; Keshavan, M.S.; Rajowska, G.; et al. An MRI-based approach for the measurement of the dorsolateral prefrontal cortex in humans. Psychiatry Res. 2009, 173, 150–154. [Google Scholar] [CrossRef] [Green Version]
- Goldman-Rakic, P.S. Architecture of the prefrontal cortex and the central executive. Ann. N. Y. Acad. Sci. 1995, 769, 71–83. [Google Scholar] [CrossRef]
- Greene, J.; Sommerville, R.; Nystrom, L.; Darley, J.; Cohen, J.D. An fMRI Investigation of Emotional Engagement in Moral Judgment. Science 2001, 293, 2105–2108. [Google Scholar] [CrossRef] [Green Version]
- Monsell, S. Task switching. Trends Cogn. Sci. 2003, 7, 134–140. [Google Scholar] [CrossRef]
- Chan, R.C.K.; Shum, D.; Toulopoulou, T.; Chen, E.Y.H. Assessment of executive functions: Review of instruments and identification of critical issues. Arch. Clin. Neuropsychol. 2008, 23, 201–216. [Google Scholar] [CrossRef] [Green Version]
- Ito, A.; Abe, N.; Fujii, T.; Hayashi, A.; Mori, E. The contribution of the dorsolateral prefrontal cortex to the preparation for deception and truth-telling. Brain Res. 2012, 1464, 43–52. [Google Scholar] [CrossRef]
- Yoon, J.H.; Minzenberg, M.J.; Ursu, S.; Walters, R.; Wendelken, C.; Ragland, J.D.; Carter, C.S. Association of Dorsolateral Prefrontal Cortex Dysfunction with Disrupted Coordinated Brain Activity in Schizophrenia: Relationship with Impaired Cognition, Behavioral Disorganization, and Global Function. AJP 2008, 165, 1006–1014. [Google Scholar] [CrossRef]
- Kandilarova, S.; Stoyanov, D.; Kostianev, S.; Specht, K. Altered resting state effective connectivity of anterior insula in depression. Front. Psychiatry 2018, 9, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Uddin, L.Q. Salience processing and insular cortical function and dysfunction. Nat. Rev. Neurosci. 2015, 16, 55–61. [Google Scholar] [CrossRef]
- Power, J.D.; Cohen, A.L.; Nelson, S.M.; Wig, G.S.; Barnes, K.A.; Church, J.A.; Vogel, A.C.; Laumann, T.O.; Miezin, F.M.; Schlaggar, B.L.; et al. Functional network organization of the human brain. Neuron 2011, 72, 665–678. [Google Scholar] [CrossRef] [Green Version]
- Palaniyappan, L.; Al-Radaideh, A.; Mougin, O.; Gowland, P.; Liddle, P.F. Combined white matter imaging suggests myelination defects in visual processing regions in schizophrenia. Neuropsychopharmacology 2013, 38, 1808–1815. [Google Scholar] [CrossRef]
- Callicott, J.H.; Bertolino, A.; Mattay, V.S.; Langheim, F.J.; Duyn, J.; Coppola, R.; Goldberg, T.E.; Weinberger, D.R. Physiological dysfunction of the dorsolateral prefrontal cortex in schizophrenia revisited. Cereb. Cortex 2000, 10, 1078–1092. [Google Scholar] [CrossRef]
- Weinberger, D.R.; Berman, K.F.; Suddath, R.; Torrey, E.F. Evidence of dysfunction of a prefrontal-limbic network in schizophrenia: A magnetic resonance imaging and regional cerebral blood flow study of discordant monozygotic twins. Am. J. Psychiatry 1992, 149, 890–897. [Google Scholar]
- Stoyanov, D.; Maes, M.H. How to construct neuroscience-informed psychiatric classification? Towards nomothetic networks psychiatry. World J. Psychiatry, 2021; in press. [Google Scholar]
- Stoyanov, D.; Aryutova, K.; Kandilarova, S.; Paunova, R.; Arabadzhiev, Z.; Todeva, A.; Kostianev, S.; Borgwardt, S. Diagnostic Task Specific Activations in Functionoal Mri and Aberrant Connectivity of Insula with Middle Frontal Gyrus Can Inform the Differential Diagnosis of Psychosis. 2020. Available online: https://www.preprints.org/manuscript/202012.0031/v1 (accessed on 30 December 2020).
- George, M.S.; Padberg, F.; Schlaepfer, T.E.; O’Reardon, J.P.; Fitzgerald, P.B.; Nahas, Z.H.; Marcolin, M.A. Controversy: Repetitive transcranial magnetic stimulation or transcranial direct current stimulation shows efficacy in treating psychiatric diseases (depression, mania, schizophrenia, obsessive-complusive disorder, panic, posttraumatic stress disorder). Brain Stimulat. 2009, 2, 14–21. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Schizophrenia Patients (n = 25) | Depressed Patients (n = 26) | Statistical Significance | |
|---|---|---|---|
| Age (mean ± SD) | 38.8 ± 13.5 | 41 ± 11.4 | 0.434 a |
| Sex (M/F) | 13/12 | 9/17 | 0.210 b |
| Education (years) | 13.4 ± 3 | 13.6 ± 3.3 | 0.567 a |
| Age at onset (years) | 26 ± 9.2 | 29.6 ± 10.3 | 0.173 a |
| Illness duration (months) | 150 ± 115 | 139 ± 92 | 0.885 a |
| Episode duration (weeks) | 20.3 ± 28.4 | 12.6 ± 16 | 0.141 a |
| MDD Patients (n = 10) | BD Patients (n = 16) | Statistical Significance | |
|---|---|---|---|
| Age (mean ± SD) | 37.5 ± 9.9 | 43.1 ± 12.1 | 0.286 a |
| Sex (M/F) | 4/6 | 5/11 | 0.648 b |
| Education (years ± SD) | 16 ± 3.7 | 12.6 ± 2.6 | 0.113 a |
| MADRS score (mean ± SD) | 27.4 ± 4.7 | 30.4 ± 6.7 | 0.357 a |
| Age at onset (years) | 27.2 ± 6.4 | 31 ± 12 | 0.522 a |
| Illness duration (months) | 129.2 ± 98.5 | 144.3 ± 91.3 | 0.803 a |
| Episode duration (weeks) | 10.4 ± 11.2 | 13.7 ± 18.5 | 0.490 a |
| Connections | Mean | SD | a Significance |
|---|---|---|---|
| PreCu ⸧ | −0.133 | 0.290 | 0.002 |
| OFC→ PreCu | 0.094 | 0.334 | 0.027 |
| HPC ⸧ | −0.091 | 0.240 | 0.009 |
| PreCu→ AI | −0.151 | 0.328 | 0.002 |
| HPC→ AI | −0.128 | 0.354 | 0.013 |
| AI ⸧ | −0.159 | 0.226 | 0.000 ** |
| PreCu→ AngG | 0.154 | 0.420 | 0.013 |
| AngG⸧ | −0.160 | 0.301 | 0.000 ** |
| Th→ AngG | −0.117 | 0.348 | 0.021 |
| HPC→ OFC | −0.120 | 0.316 | 0.010 |
| AI→ OFC | 0.186 | 0.335 | 0.000 ** |
| OFC⸧ | −0.086 | 0.293 | 0.041 |
| AI→ PlT | 0.152 | 0.292 | 0.001 |
| AngG→ PlT | 0.088 | 0.293 | 0.015 |
| PlT⸧ | −0.182 | 0.216 | 0.000 ** |
| HPC→ Th | 0.080 | 0.276 | 0.045 |
| HPC→ MFG | −0.180 | 0.333 | 0.000 ** |
| Th→ MFG | −0.118 | 0.345 | 0.019 |
| MFG ⸧ | −0.220 | 0.271 | 0.000 ** |
| Connections | Mean | SD | a Significance |
|---|---|---|---|
| PreCu ⸧ | −0.156 | 0.263 | 0.008 |
| AI ⸧ | −0.108 | 0.207 | 0.017 |
| MFG→ AI | −0.112 | 0.257 | 0.043 |
| AngG⸧ | −0.161 | 0.300 | 0.015 |
| Th→ AngG | −0.199 | 0.337 | 0.011 |
| AI→ OFC | 0.169 | 0.256 | 0.004 |
| AngG→ PlT | 0.120 | 0.265 | 0.037 |
| PlT⸧ | −0.214 | 0.230 | 0.000 ** |
| PlT→ Th | −0.156 | 0.324 | 0.035 |
| Th ⸧ | −0.258 | 0.328 | 0.000 ** |
| Connections | Mean | SD | a Significance |
|---|---|---|---|
| HPC ⸧ | −0.145 | 0.270 | 0.011 |
| PreCu→ AI | −0.200 | 0.300 | 0.002 |
| HPC→ AI | −0.198 | 0.292 | 0.002 |
| AI ⸧ | −0.207 | 0.236 | 0.000 ** |
| AngG⸧ | −0.161 | 0.310 | 0.014 |
| HPC→ OFC | −0.173 | 0.289 | 0.005 |
| AI→ OFC | 0.202 | 0.400 | 0.016 |
| OFC⸧ | −0.140 | 0.241 | 0.007 |
| AI→ PlT | 0.208 | 0.311 | 0.002 |
| PlT⸧ | −0.154 | 0.204 | 0.001 |
| HPC→ MFG | −0.255 | 0.357 | 0.001 |
| MFG ⸧ | −0.186 | 0.209 | 0.000 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoyanov, D.; Aryutova, K.; Kandilarova, S.; Paunova, R.; Arabadzhiev, Z.; Todeva-Radneva, A.; Kostianev, S.; Borgwardt, S. Diagnostic Task Specific Activations in Functional MRI and Aberrant Connectivity of Insula with Middle Frontal Gyrus Can Inform the Differential Diagnosis of Psychosis. Diagnostics 2021, 11, 95. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010095
Stoyanov D, Aryutova K, Kandilarova S, Paunova R, Arabadzhiev Z, Todeva-Radneva A, Kostianev S, Borgwardt S. Diagnostic Task Specific Activations in Functional MRI and Aberrant Connectivity of Insula with Middle Frontal Gyrus Can Inform the Differential Diagnosis of Psychosis. Diagnostics. 2021; 11(1):95. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010095
Chicago/Turabian StyleStoyanov, Drozdstoy, Katrin Aryutova, Sevdalina Kandilarova, Rositsa Paunova, Zlatoslav Arabadzhiev, Anna Todeva-Radneva, Stefan Kostianev, and Stefan Borgwardt. 2021. "Diagnostic Task Specific Activations in Functional MRI and Aberrant Connectivity of Insula with Middle Frontal Gyrus Can Inform the Differential Diagnosis of Psychosis" Diagnostics 11, no. 1: 95. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010095