
Pilot Study to Evaluate Serum Soluble Mesothelin-Related Peptide (SMRP) as Marker for Clinical Monitoring of Pleural Mesothelioma (PM): Correlation with Modified RECIST Score

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Measurement of Serum SMRP
2.3. CT Imaging and Modified RECIST Score
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
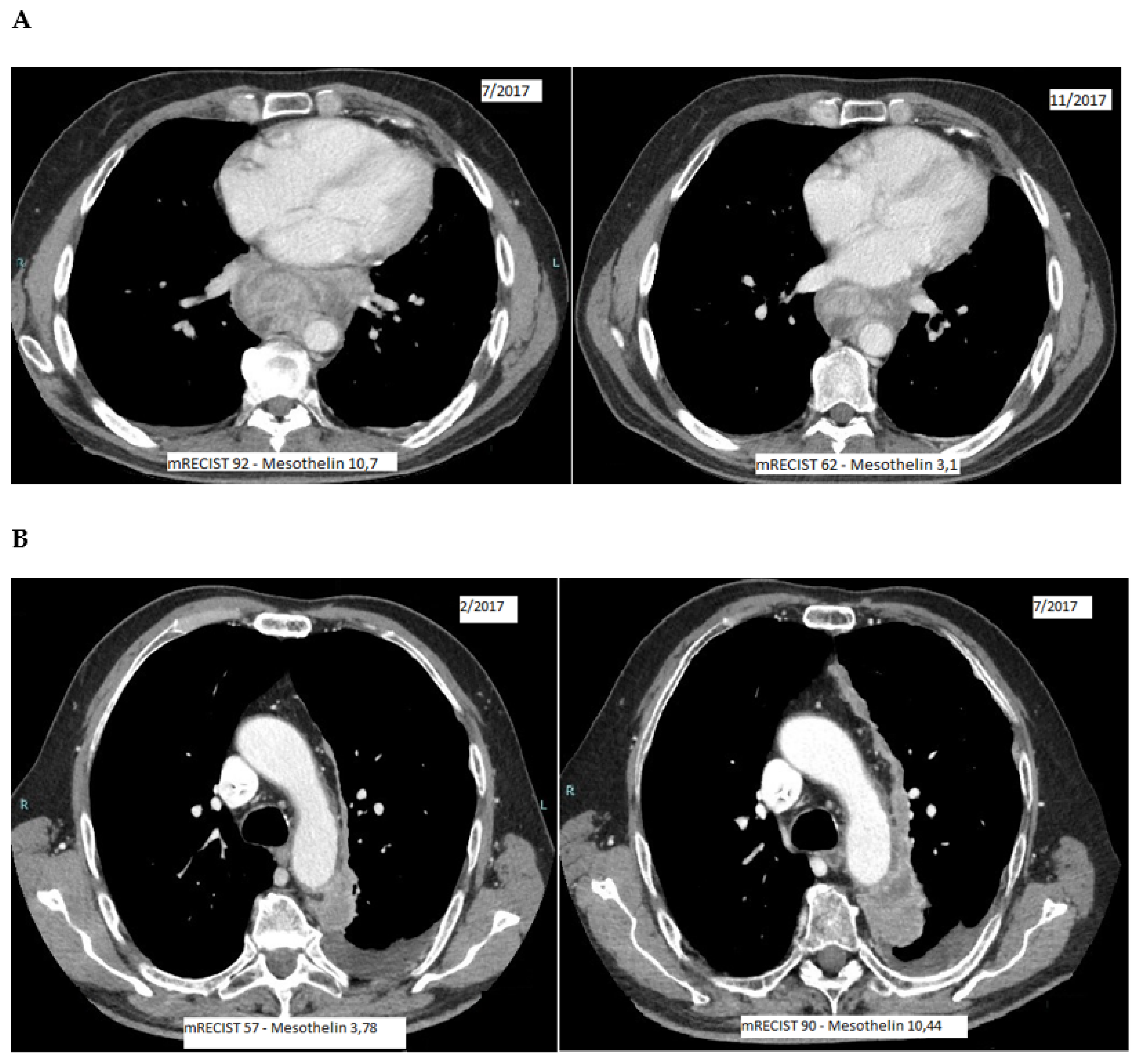
3.2. SMRP and mRECIST Measurements
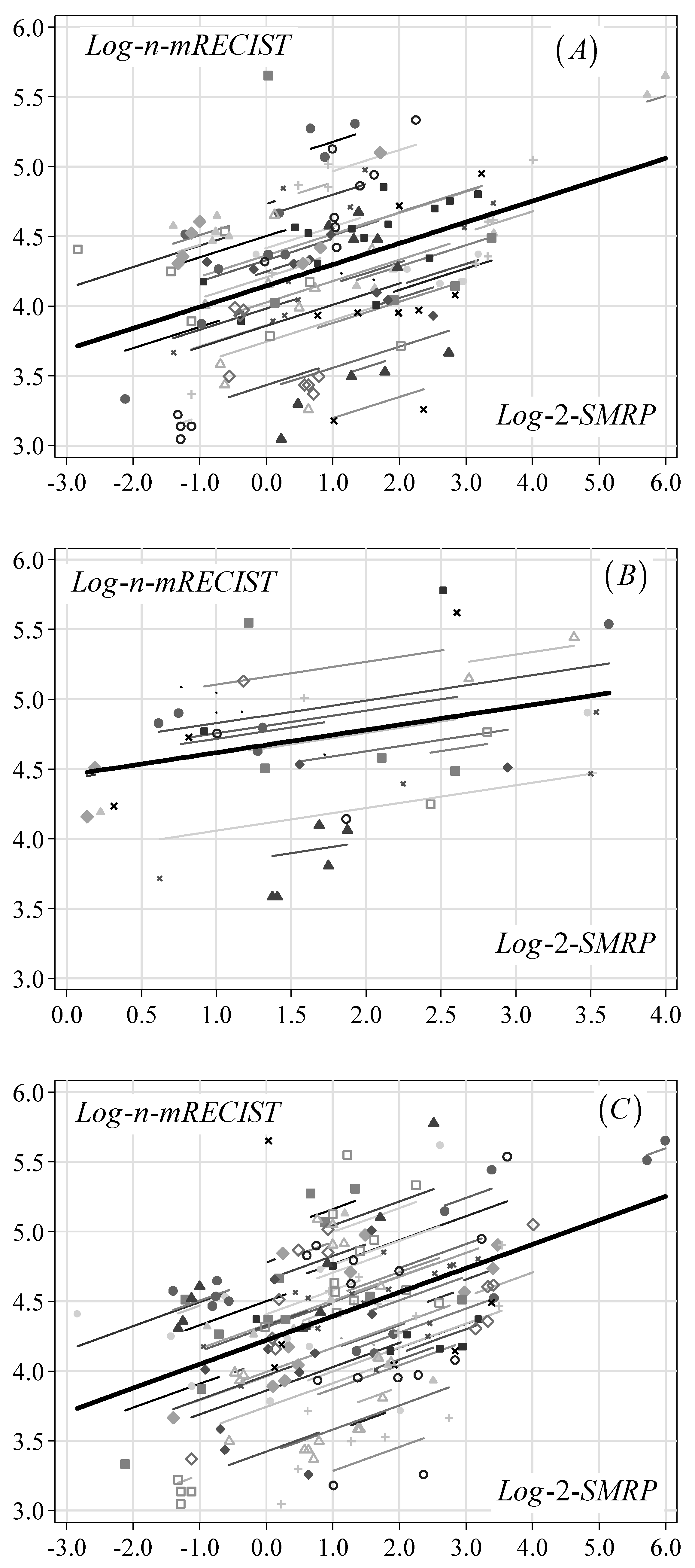
3.3. Relationship between SMPR and mRECIST
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Merritt, N.; Blewett, C.J.; Miller, J.D.; Bennett, W.F.; Young, J.E.; Urschel, J.D. Survival after conservative (palliative) management of pleural malignant mesothelioma. J. Surg. Oncol. 2001, 78, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Milano, M.T.; Zhang, H. Malignant pleural mesothelioma: A population-based study of survival. J. Thorac. Oncol. 2010, 5, 1841–1848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogelzang, N.J.; Rusthoven, J.J.; Symanowski, J.; Denham, C.; Kaukel, E.; Ruffie, P.; Gatzemeier, U.; Boyer, M.; Emri, S.; Manegold, C.; et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J. Clin. Oncol. 2003, 21, 2636–2644. [Google Scholar] [CrossRef]
- Baas, P.; Scherpereel, A.; Nowak, A.K.; Fujimoto, N.; Peters, S.; Tsao, A.S.; Mansfield, A.S.; Popat, S.; Jahan, T.; Antonia, S.; et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): A multicentre, randomised, open-label, phase 3 trial. Lancet 2021, 397, 375–386. [Google Scholar] [CrossRef]
- Zauderer, M.G.; Kass, S.L.; Woo, K.; Sima, C.S.; Ginsberg, M.S.; Krug, L.M. Vinorelbine and gemcitabine as second- or third-line therapy for malignant pleural mesothelioma. Lung Cancer 2014, 84, 271–274. [Google Scholar] [CrossRef] [Green Version]
- Pagano, M.; Ceresoli, G.; Zucali, P.A.; Giulia, P.; Chiara, G.M.; Federica, G.; Marcello, T.; Parra, H.J.S.; Francesca, Z.; Federico, C.; et al. Randomized phase II study on gemcitabine with or without ramucirumab as second-line treatment for advanced malignant pleural mesothelioma (MPM): Results of Italian Rames Study. J. Clin. Oncol. 2020, 38, 9004. [Google Scholar] [CrossRef]
- Fennell, D.; Ottensmeier, C.; Califano, R.; Hanna, G.G.; Ewings, S.; Kayleigh, H.; Wilding, S.; Danson, S.; Nye, M.; Steele, N. Nivolumab versus placebo in relapsed malignant mesothelioma: Preliminary results from the CONFIRM phase 3 trial. In Proceedings of the 2020 World Conference on Lung Cancer Singapore, Virtual, 28–31 January 2021. [Google Scholar]
- Byrne, M.J.; Nowak, A.K. Modified RECIST criteria for assessment of response in malignant pleural mesothelioma. Ann. Oncol. 2004, 15, 257–260. [Google Scholar] [CrossRef]
- Armato, S.G.; Nowak, A.K. Revised Modified Response Evaluation Criteria in Solid Tumors for Assessment of Response in Malignant Pleural Mesothelioma (Version 1.1). J. Thorac. Oncol. 2018, 13, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.W.; Creaney, J.; Lake, R.; Nowak, A.; Musk, A.W.; de Klerk, N.; Winzell, P.; Hellstrom, K.E.; Hellstrom, I. Mesothelin-family proteins and diagnosis of mesothelioma. Lancet 2003, 362, 1612–1616. [Google Scholar] [CrossRef]
- Hassan, R.; Laszik, Z.G.; Lerner, M.; Raffeld, M.; Postier, R.; Brackett, D. Mesothelin is overexpressed in pancreaticobiliary adenocarcinomas but not in normal pancreas and chronic pancreatitis. Am. J. Clin. Pathol. 2005, 124, 838–845. [Google Scholar] [CrossRef]
- Ho, M.; Bera, T.K.; Willingham, M.C.; Onda, M.; Hassan, R.; FitzGerald, D.; Pastan, I. Mesothelin expression in human lung cancer. Clin. Cancer Res. 2007, 13, 1571–1575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beyer, H.L.; Geschwindt, R.D.; Glover, C.L.; Tran, L.; Hellstrom, I.; Hellstrom, K.E.; Miller, M.C.; Verch, T.; Allard, W.J.; Pass, H.I.; et al. MESOMARK: A potential test for malignant pleural mesothelioma. Clin. Chem. 2007, 53, 666–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burt, B.M.; Lee, H.S.; Lenge De Rosen, V.; Hamaji, M.; Groth, S.S.; Wheeler, T.M.; Sugarbaker, D.J. Soluble Mesothelin-Related Peptides to Monitor Recurrence After Resection of Pleural Mesothelioma. Ann. Thorac. Surg. 2017, 104, 1679–1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollevoet, K.; Van Cleemput, J.; Thimpont, J.; De Vuyst, P.; Bosquée, L.; Nackaerts, K.; Germonpré, P.; Vansteelandt, S.; Kishi, Y.; Delanghe, J.R.; et al. Serial measurements of mesothelioma serum biomarkers in asbestos-exposed individuals: A prospective longitudinal cohort study. J. Thorac. Oncol. 2011, 6, 889–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheatley-Price, P.; Yang, B.; Patsios, D.; Patel, D.; Ma, C.; Xu, W.; Leighl, N.; Feld, R.; Cho, B.C.; O’Sullivan, B.; et al. Soluble mesothelin-related Peptide and osteopontin as markers of response in malignant mesothelioma. J. Clin. Oncol. 2010, 28, 3316–3322. [Google Scholar] [CrossRef] [PubMed]
- Creaney, J.; Francis, R.J.; Dick, I.M.; Musk, A.W.; Robinson, B.W.; Byrne, M.J.; Nowak, A.K. Serum soluble mesothelin concentrations in malignant pleural mesothelioma: Relationship to tumor volume, clinical stage and changes in tumor burden. Clin. Cancer Res. 2011, 17, 1181–1189. [Google Scholar] [CrossRef] [Green Version]
- Arnold, D.T.; De Fonseka, D.; Hamilton, F.W.; Rahman, N.M.; Maskell, N.A. Prognostication and monitoring of mesothelioma using biomarkers: A systematic review. Br. J. Cancer 2017, 116, 731–741. [Google Scholar] [CrossRef] [Green Version]
- Fontana, V.; Vigani, A.; Pistillo, M.P.; Giannoni, U.; Rosemberg, I.; Canessa, P.A.; Berisso, G.; Ferro, P.; Franceschini, M.C.; Tonarelli, M.; et al. The Correlation of Serum Mesothelin Level With Pleural Thickness in Malignant Pleural Mesothelioma Makes it a Valuable Tool for Monitoring Tumor Progression. J. Thorac. Oncol. 2019, 14, e92–e94. [Google Scholar] [CrossRef]
- Kindler, H.L.; Ismaila, N.; Armato, S.G.; Bueno, R.; Hesdorffer, M.; Jahan, T.; Jones, C.M.; Miettinen, M.; Pass, H.; Rimner, A.; et al. Treatment of Malignant Pleural Mesothelioma: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1343–1373. [Google Scholar] [CrossRef]
- Fitzmaurice, G.M.; Laird, N.M.; Ware, J.H. Applied Longitudinal Analysis, 2nd ed.; Wiley: Hoboken, NJ, USA, 2011. [Google Scholar]
- Grigoriu, B.D.; Chahine, B.; Vachani, A.; Gey, T.; Conti, M.; Sterman, D.H.; Marchandise, G.; Porte, H.; Albelda, S.M.; Scherpereel, A. Kinetics of soluble mesothelin in patients with malignant pleural mesothelioma during treatment. Am. J. Respir. Crit. Care Med. 2009, 179, 950–954. [Google Scholar] [CrossRef]
- de Fonseka, D.; Arnold, D.T.; Stadon, L.; Morley, A.; Keenan, E.; Darby, M.; Armstrong, L.; Virgo, P.; Maskell, N.A. A prospective study to investigate the role of serial serum mesothelin in monitoring mesothelioma. BMC Cancer 2018, 18, 199. [Google Scholar] [CrossRef]
- Pass, H.I.; Temeck, B.K.; Kranda, K.; Steinberg, S.M.; Feuerstein, I.R. Preoperative tumor volume is associated with outcome in malignant pleural mesothelioma. J. Thorac. Cardiovasc. Surg. 1998, 115, 310–317. [Google Scholar] [CrossRef] [Green Version]
- Gill, R.R.; Richards, W.G.; Yeap, B.Y.; Matsuoka, S.; Wolf, A.S.; Gerbaudo, V.H.; Bueno, R.; Sugarbaker, D.J.; Hatabu, H. Epithelial malignant pleural mesothelioma after extrapleural pneumonectomy: Stratification of survival with CT-derived tumor volume. AJR Am. J. Roentgenol. 2012, 198, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Frauenfelder, T.; Tutic, M.; Weder, W.; Götti, R.P.; Stahel, R.A.; Seifert, B.; Opitz, I. Volumetry: An alternative to assess therapy response for malignant pleural mesothelioma? Eur. Respir. J. 2011, 38, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.J.; Gill, R.R. Volumetric assessment in malignant pleural mesothelioma. Ann. Transl. Med. 2017, 5, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | AL Cohort | SP Cohort | Both Cohorts | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | % | P50 | IQR | No. | % | P50 | IQR | No. | % | P50 | IQR | |
| Age at diagnosis | 67 | 61–72 | 68 | 63–72 | 67 | 62–72 | ||||||
| Days from diagnosis | 5 | 3–27 | 3 | 0–56 | 5 | 2–30 | ||||||
| Years of follow-up | 1.4 | 0.9–2.4 | 2.5 | 1.7–3.1 | 1.8 | 1.0–2.7 | ||||||
| Mortality rate/1000/month 1 | 41.8 | 29.8–58.4 | 33.8 | 21.3–53.6 | 38.6 | 29.4–50.7 | ||||||
| Gender | ||||||||||||
| Male | 29 | 72.5 | 17 | 94.4 | 46 | 79.3 | ||||||
| Female | 11 | 27.8 | 1 | 5.6 | 12 | 20.7 | ||||||
| Histology | ||||||||||||
| Epithelioid | 30 | 66.7 | 14 | 77.8 | 44 | 75.9 | ||||||
| Non-epithelioid | 10 | 33.3 | 4 | 22.2 | 14 | 24.1 | ||||||
| ECOG-PS | ||||||||||||
| ≤1 | 28 | 70.0 | 7 | 38.9 | 35 | 60.3 | ||||||
| >1 | 12 | 30.0 | 11 | 61.1 | 23 | 39.7 | ||||||
| Vital status | ||||||||||||
| Alive | 6 | 15.0 | 0 | 0.0 | 6 | 10.3 | ||||||
| Dead | 34 | 85.0 | 18 | 100.0 | 52 | 89.7 | ||||||
| Therapy | ||||||||||||
| Chemotherapy | 6 | 15.0 | 15 | 83.3 | 21 | 36.2 | ||||||
| Chemo and immunotherapy | 13 | 32.5 | 0 | 0.0 | 13 | 22.4 | ||||||
| Chemo and antiangiogenic | 21 | 52.5 | 0 | 0.0 | 21 | 36.2 | ||||||
| Supportive care | 0 | 0.0 | 3 | 16.6 | 3 | 5.2 | ||||||
| Whole sample | 40 | 100.0 | - | - | 18 | 100.0 | - | - | 58 | 100.0 | - | - |
| Clinical Marker | Histology | AL Cohort | SP Cohort | Both Cohorts | |||
|---|---|---|---|---|---|---|---|
| GM | 95% CL | GM | 95% CL | GM | 95% CL | ||
| SMRP levels (nM) | Epithelioid | 2.88 | 1.99–4.16 | 2.57 | 1.78–3.71 | 2.77 | 2.11–3.66 |
| Non-epithelioid | 1.43 | 0.76–7.70 | 3.81 | 1.92–7.56 | 1.89 | 1.16–3.09 | |
| Whole sample | 2.42 | 1.74–3.36 | 2.81 | 2.03–3.88 | 2.53 | 1.98–3.23 | |
| mRECIST score | Epithelioid | 81.8 | 67.0–99.8 | 97.1 | 76.6–123.0 | 86.3 | 74.2–100.5 |
| Non-epithelioid | 84.7 | 59.9–119.7 | 85.5 | 55.0–133.1 | 84.9 | 64.9–111.2 | |
| Whole sample | 82.5 | 69.5–97.8 | 94.4 | 77.0–115.6 | 86.0 | 75.4–98.0 | |
| AL Cohort | SP Cohort | Both Cohorts | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SMRP (nM) | GM | GMR | 95%-CL | p-Value | SMRP (nM) | GM | GMR | 95%-CL | p-Value | SMRP (nM) | GM | GMR | 95%-CL | p-Value |
| Categories (median) | 0.010 | Categories (median) | 0.043 | Categories (median) | 0.006 | |||||||||
| 0.14–0.99 (0.53) | 61.1 | 1.00 | (Ref.) | 1.10–1.99 (1.61) | 95.3 | 1.00 | (Ref.) | 0.14–1.14 (0.61) | 73.3 | 1.00 | (Ref.) | |||
| 1.00–1.71 (1.39) | 68.8 | 1.13 | 0.97–1.31 | 2.00–2.78 (2.42) | 104.4 | 1.09 | 0.83–1.44 | 1.15–2.01 (1.57) | 77.2 | 1.05 | 0.90–1.24 | |||
| 1.72–3.57 (2.55) | 77.2 | 1.26 | 1.06–1.51 | 2.79–5.72 (3.65) | 123.6 | 1.29 | 1.00–1.69 | 2.02–3.94 (2.79) | 90.2 | 1.23 | 1.02–1.49 | |||
| 3.58–63.9 (7.15) | 84.4 | 1.38 | 1.14–1.67 | 5.73–12.3 (9.10) | 134.5 | 1.41 | 1.06–1.88 | 3.95–63.9 (7.15) | 99.7 | 1.36 | 1.13–1.64 | |||
| Log-2-levels | <0.001 | Log-2-levels | 0.003 | Log-2-levels | <0.001 | |||||||||
| Linear trend | 1.16 | 1.11–1.22 | Linear trend | 1.18 | 1.06–1.31 | Linear trend | 1.19 | 1.13–1.25 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grosso, F.; Mannucci, M.; Ugo, F.; Ferro, P.; Cassinari, M.; Vigani, A.; De Angelis, A.M.; Delfanti, S.; Lia, M.; Guaschino, R.; et al. Pilot Study to Evaluate Serum Soluble Mesothelin-Related Peptide (SMRP) as Marker for Clinical Monitoring of Pleural Mesothelioma (PM): Correlation with Modified RECIST Score. Diagnostics 2021, 11, 2015. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112015
Grosso F, Mannucci M, Ugo F, Ferro P, Cassinari M, Vigani A, De Angelis AM, Delfanti S, Lia M, Guaschino R, et al. Pilot Study to Evaluate Serum Soluble Mesothelin-Related Peptide (SMRP) as Marker for Clinical Monitoring of Pleural Mesothelioma (PM): Correlation with Modified RECIST Score. Diagnostics. 2021; 11(11):2015. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112015
Chicago/Turabian StyleGrosso, Federica, Matilde Mannucci, Francesca Ugo, Paola Ferro, Maurizio Cassinari, Antonella Vigani, Antonina Maria De Angelis, Sara Delfanti, Michela Lia, Roberto Guaschino, and et al. 2021. "Pilot Study to Evaluate Serum Soluble Mesothelin-Related Peptide (SMRP) as Marker for Clinical Monitoring of Pleural Mesothelioma (PM): Correlation with Modified RECIST Score" Diagnostics 11, no. 11: 2015. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112015