
Automated Motion Analysis of Bony Joint Structures from Dynamic Computer Tomography Images: A Multi-Atlas Approach

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
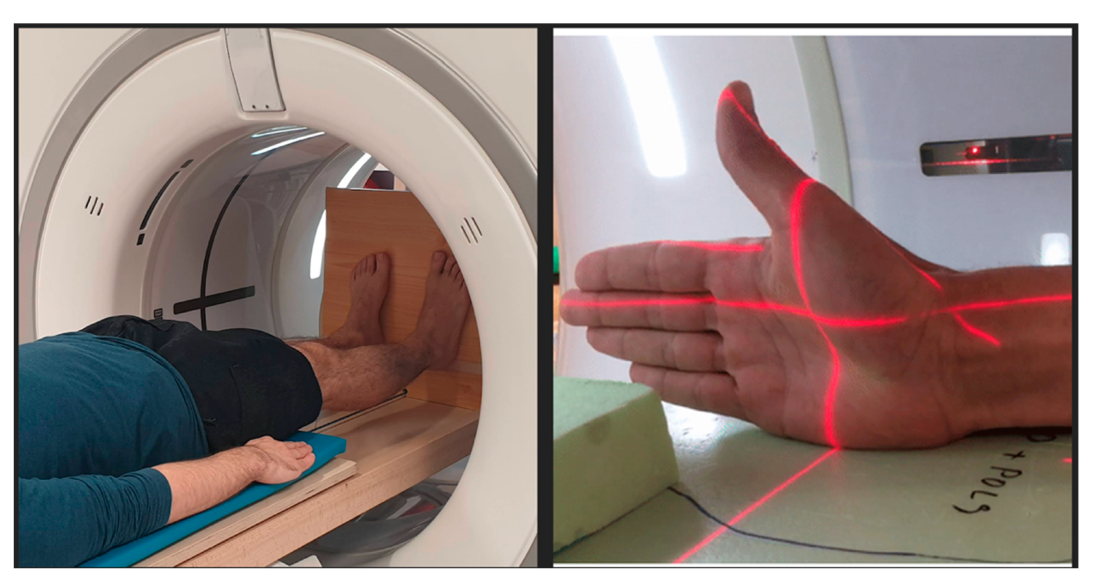
2.1. Subject Recruitment
2.2. CT Acquisitions
2.3. Atlas Dataset
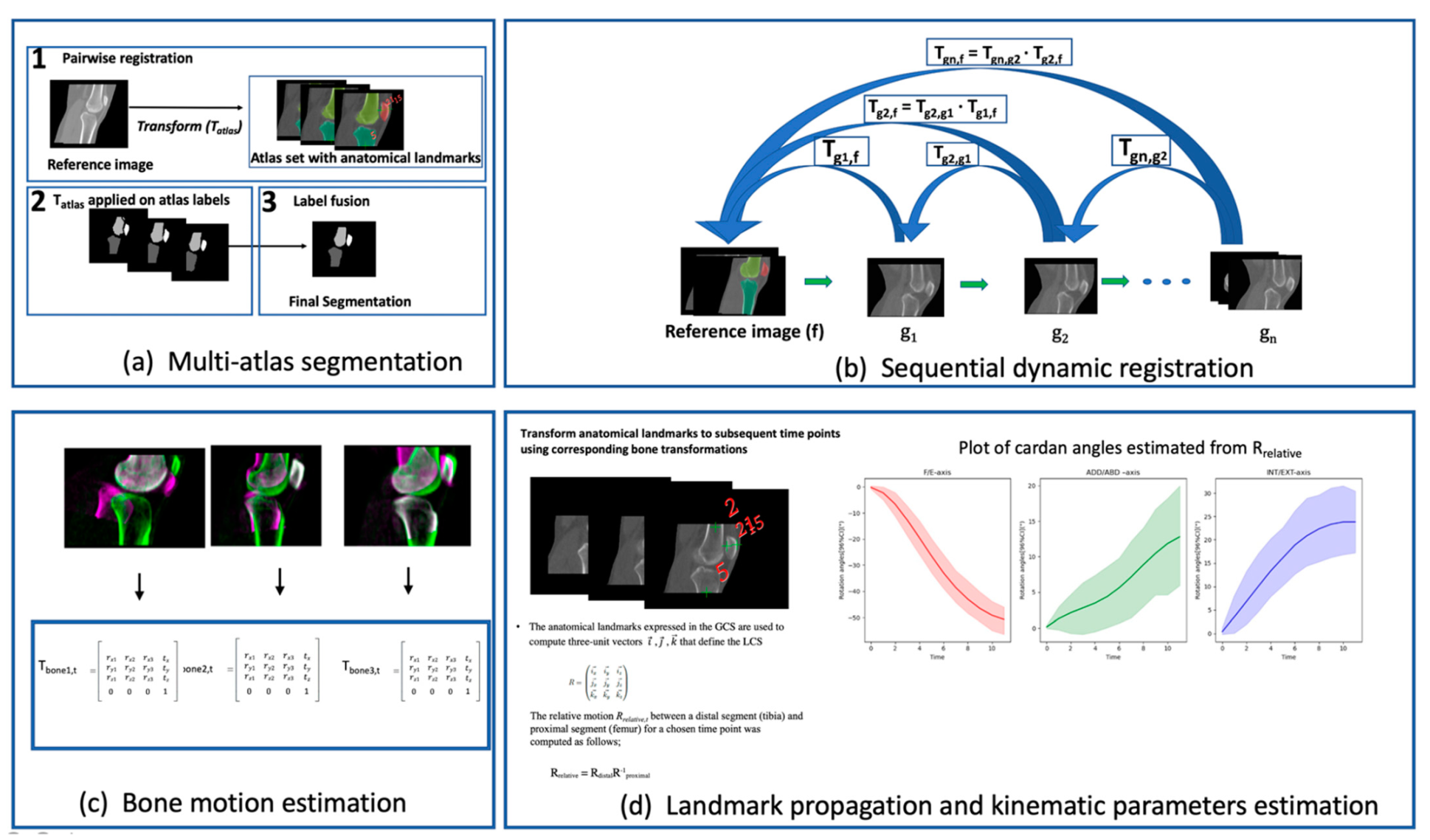
2.4. Multi-Atlas Segmentation
2.5. Dynamic Registration Framework
2.6. Landmark Propagation and Kinematic Parameters Estimation
2.7. Validation
2.8. Statistical Analysis
3. Results
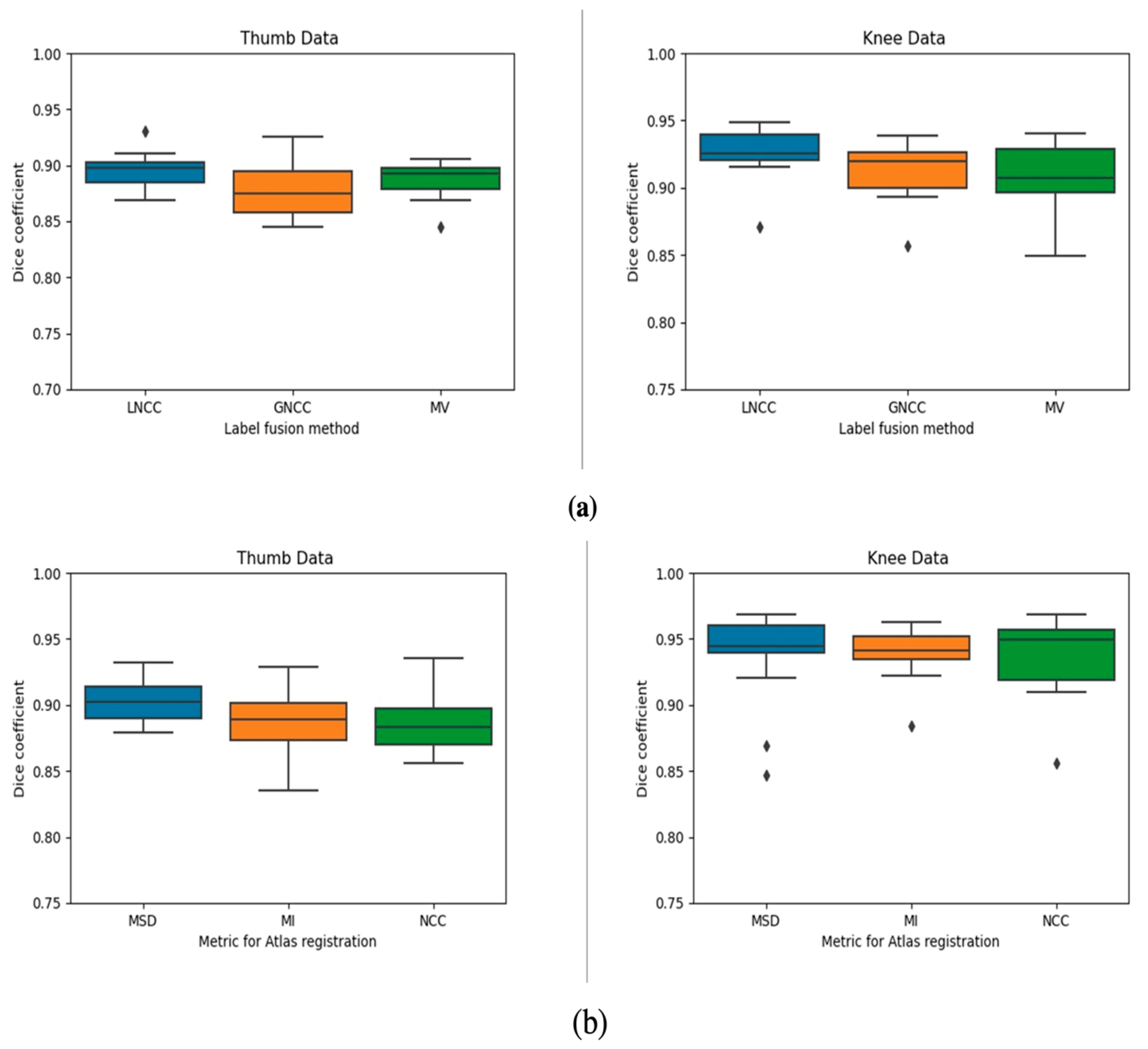
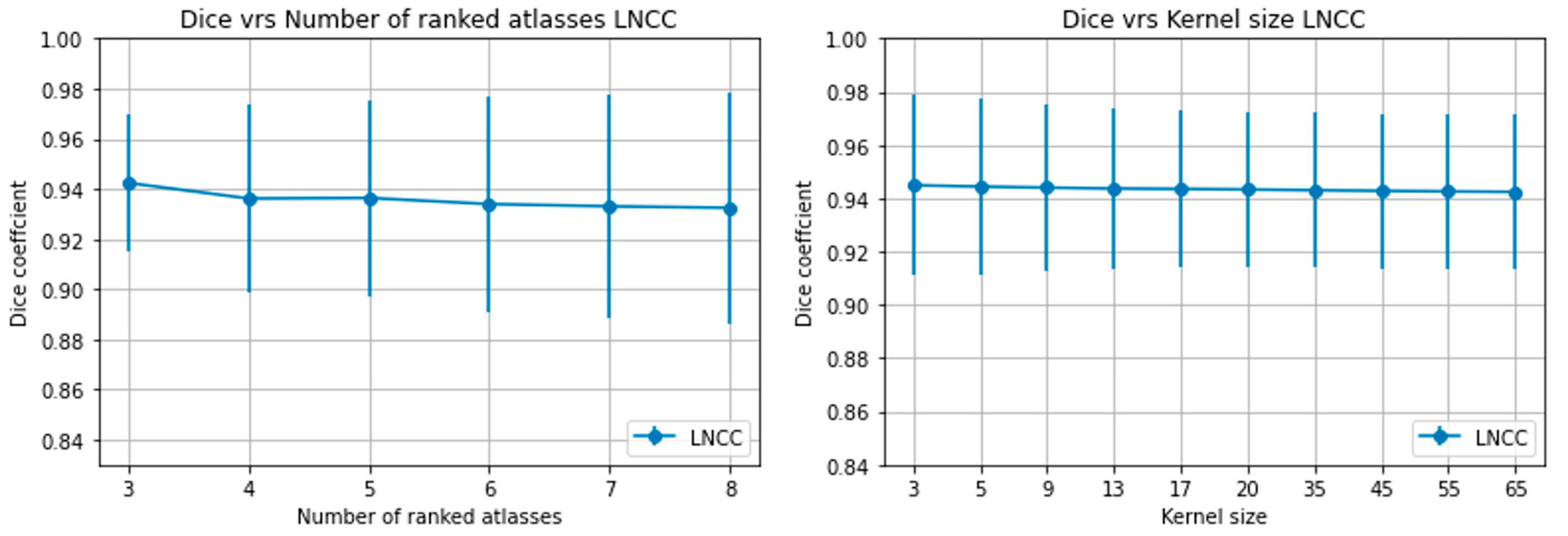
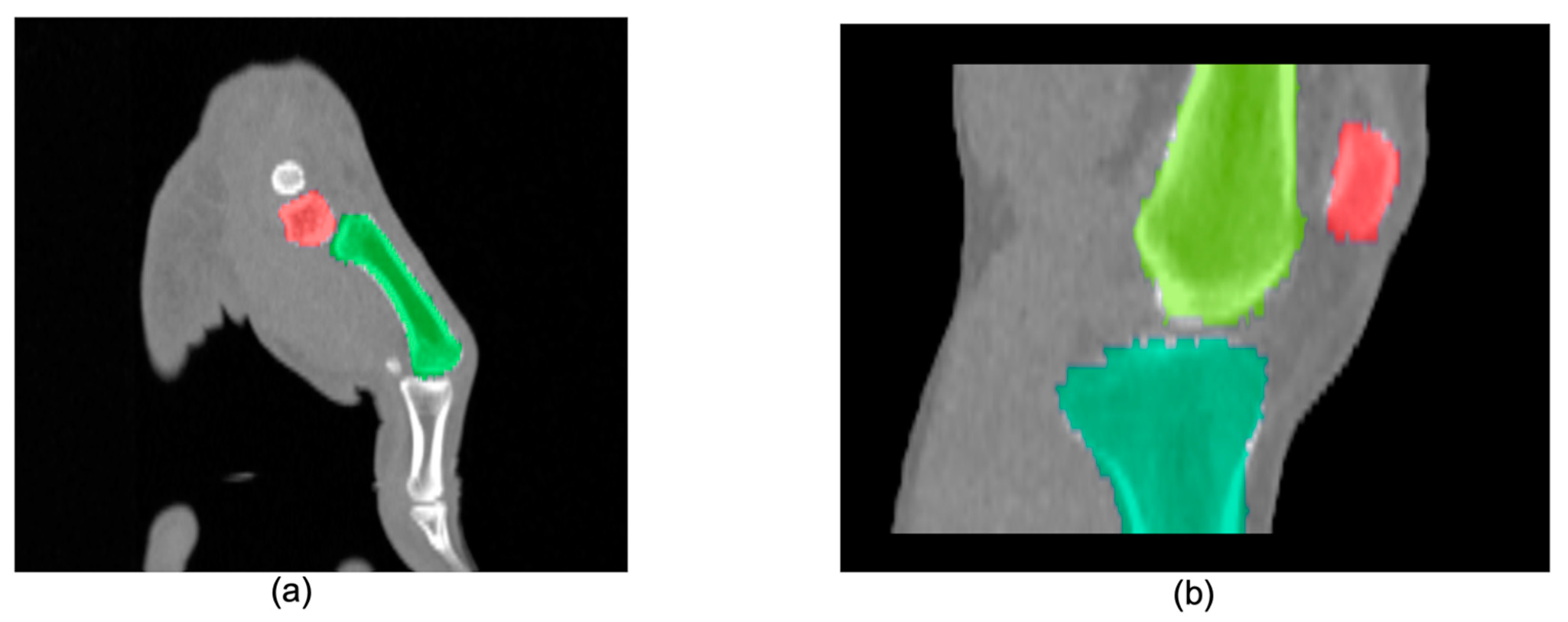
3.1. Multi-Atlas Segmentation
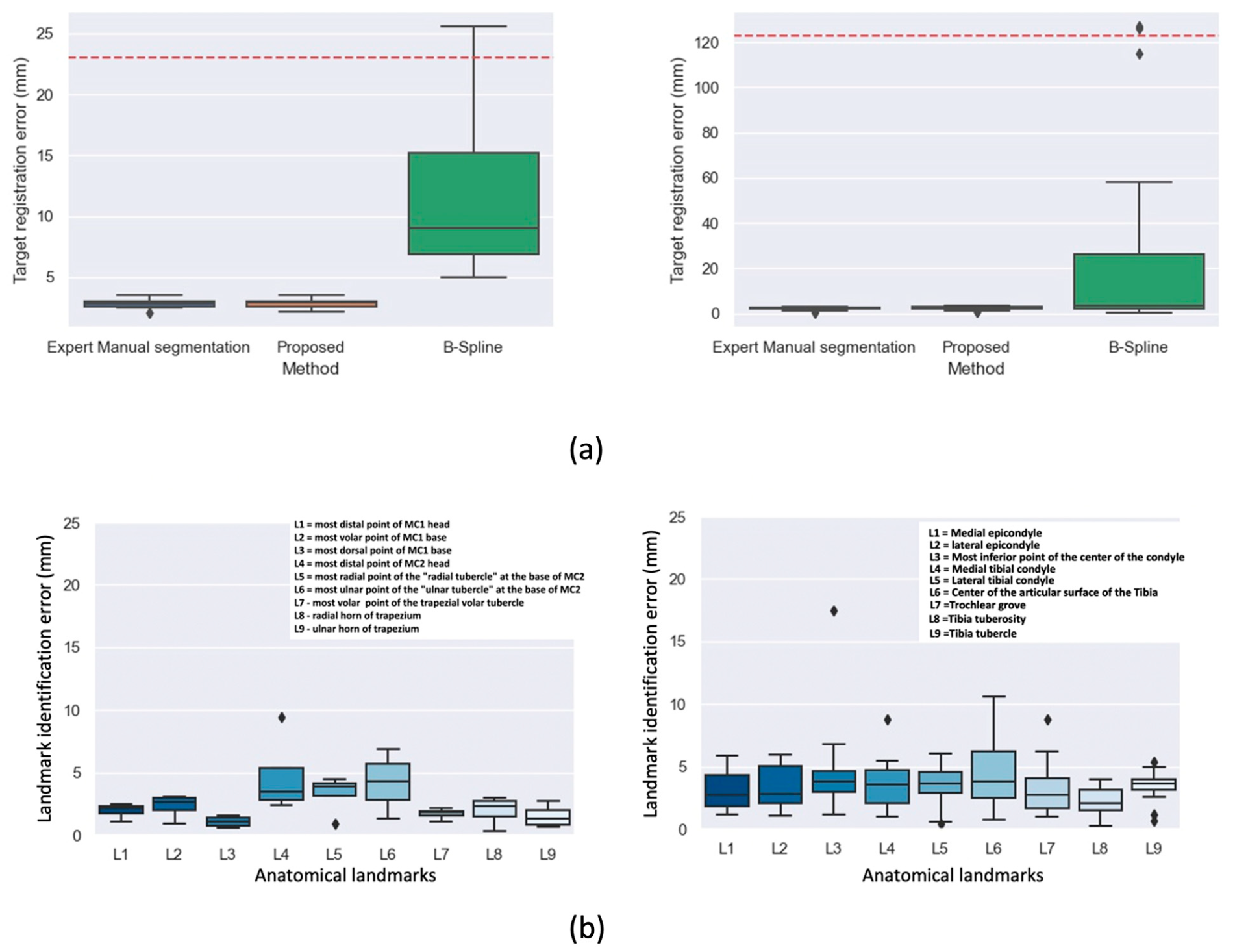
3.2. Dynamic Registration
3.3. Landmark Propagation
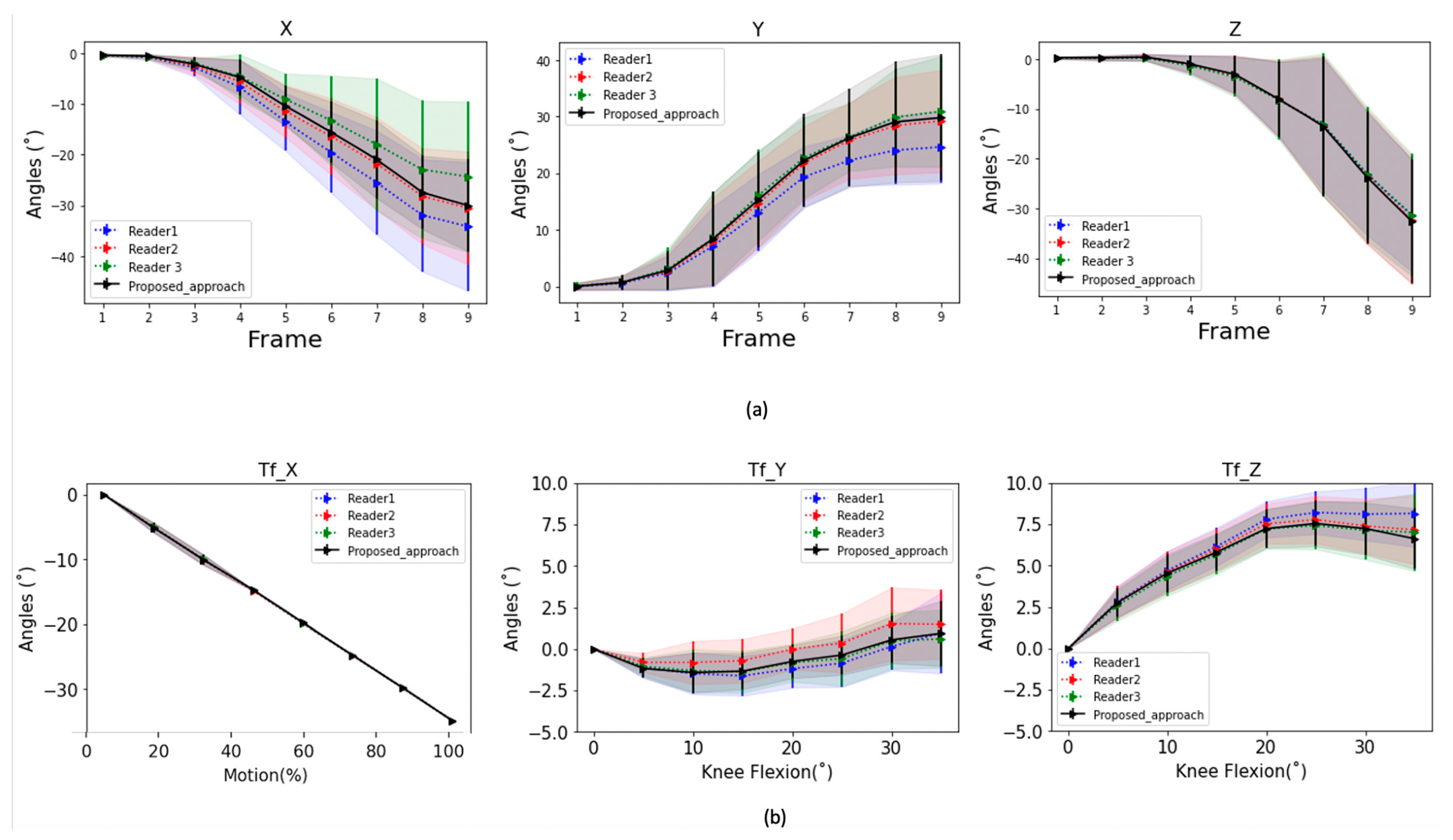
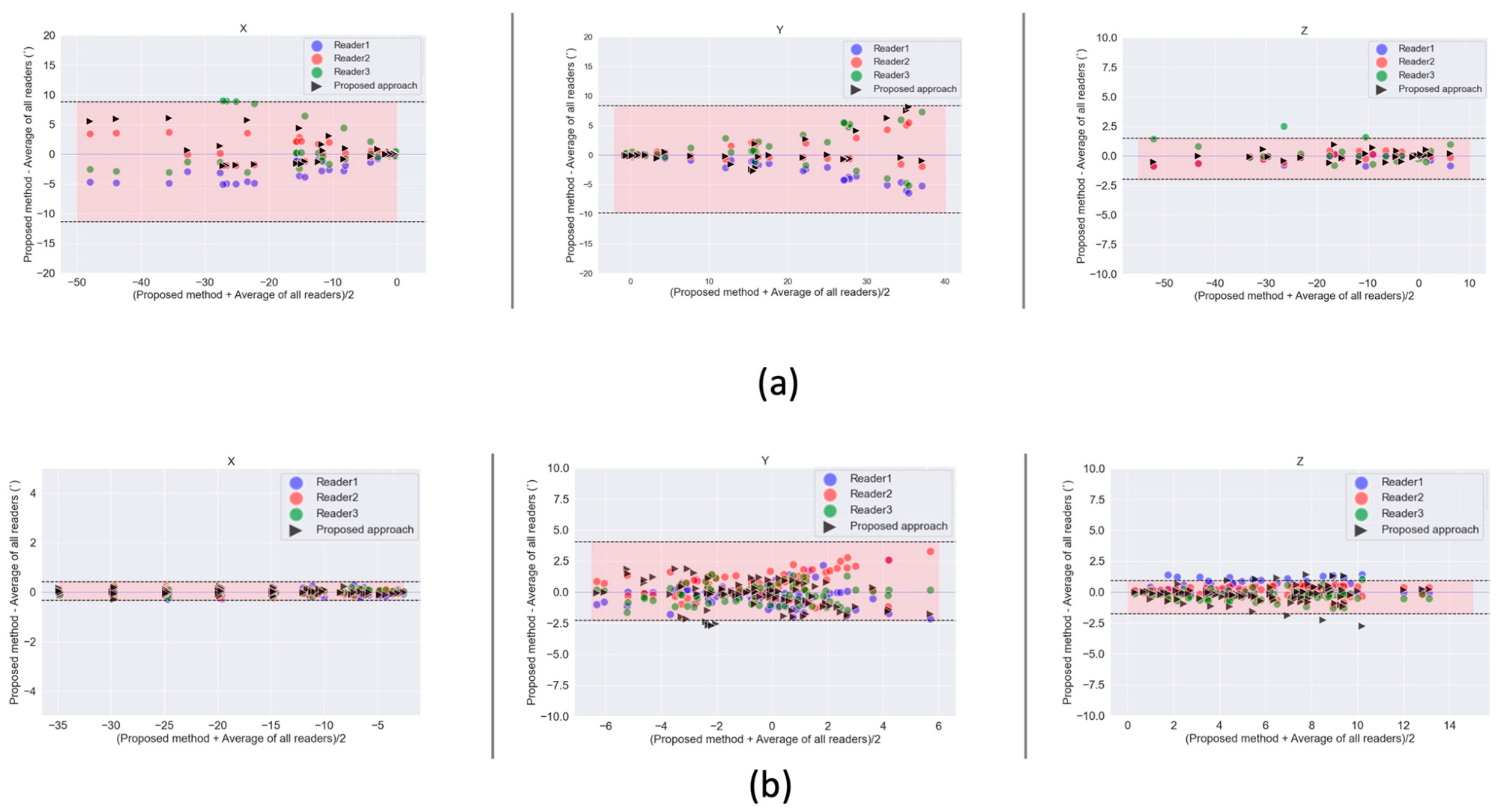
3.4. Kinematic Parameters
3.5. Discussion
3.6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; A Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Musculoskeletal Conditions|BMUS: The Burden of Musculoskeletal Diseases in the United States, (n.d.). Available online: https://www.boneandjointburden.org/fourth-edition/ib2/musculoskeletal-conditions (accessed on 21 October 2021).
- Fithian, D.C.; Paxton, E.W.; Stone, M.L.; Silva, P.; Davis, D.K.; Elias, D.A.; White, L. Epidemiology and Natural History of Acute Patellar Dislocation. Am. J. Sports Med. 2004, 32, 1114–1121. [Google Scholar] [CrossRef]
- Buckler, A.J.; Bresolin, L.; Dunnick, N.R.; Sullivan, D.C. For the Group A Collaborative Enterprise for Multi-Stakeholder Participation in the Advancement of Quantitative Imaging. Radiology 2011, 258, 906–914. [Google Scholar] [CrossRef] [Green Version]
- Buzzatti, L.; Keelson, B.; Apperloo, J.; Scheerlinck, T.; Baeyens, J.-P.; Van Gompel, G.; Vandemeulebroucke, J.; De Maeseneer, M.; De Mey, J.; Buls, N.; et al. Four-dimensional CT as a valid approach to detect and quantify kinematic changes after selective ankle ligament sectioning. Sci. Rep. 2019, 9, 1291. [Google Scholar] [CrossRef] [PubMed]
- Gervaise, A.; Louis, M.; Raymond, A.; Formery, A.-S.; Lecocq, S.; Blum, A.; Teixeira, P.A.G. Musculoskeletal Wide-Detector CT Kinematic Evaluation: From Motion to Image. Semin. Musculoskelet. Radiol. 2015, 19, 456–462. [Google Scholar] [CrossRef]
- Kerkhof, F.; Brugman, E.; D’Agostino, P.; Dourthe, B.; van Lenthe, H.G.; Stockmans, F.; Jonkers, I.; Vereecke, E. Quantifying thumb opposition kinematics using dynamic computed tomography. J. Biomech. 2016, 49, 1994–1999. [Google Scholar] [CrossRef] [PubMed]
- Tay, S.-C.; Primak, A.N.; Fletcher, J.G.; Schmidt, B.; Amrami, K.K.; Berger, R.A.; McCollough, C.H. Four-dimensional computed tomographic imaging in the wrist: Proof of feasibility in a cadaveric model. Skelet. Radiol. 2007, 36, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Demehri, S.; Thawait, G.K.; Williams, A.A.; Kompel, A.; Elias, J.J.; Carrino, J.A.; Cosgarea, A.J. Imaging Characteristics of Contralateral Asymptomatic Patellofemoral Joints in Patients with Unilateral Instability. Radiology 2014, 273, 821–830. [Google Scholar] [CrossRef]
- Forsberg, D.; Lindblom, M.; Quick, P.; Gauffin, H. Quantitative analysis of the patellofemoral motion pattern using semi-automatic processing of 4D CT data. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 1731–1741. [Google Scholar] [CrossRef]
- Rauch, A.; Arab, W.A.; Dap, F.; Dautel, G.; Blum, A.; Teixeira, P.A.G. Four-dimensional CT Analysis of Wrist Kinematics during Radioulnar Deviation. Radiology 2018, 289, 750–758. [Google Scholar] [CrossRef]
- Risser, L.; Vialard, F.-X.; Baluwala, H.Y.; Schnabel, J.A. Piecewise-diffeomorphic image registration: Application to the motion estimation between 3D CT lung images with sliding conditions. Med. Image Anal. 2013, 17, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Jain, J.; Jain, A. Displacement Measurement and Its Application in Interframe Image Coding. IEEE Trans. Commun. 1981, 29, 1799–1808. [Google Scholar] [CrossRef]
- Ourselin, S.; Roche, A.; Prima, S.; Ayache, N. Block Matching: A General Framework to Improve Robustness of Rigid Registration of Medical Images. In Logic-Based Program Synthesis and Transformation; Springer: Berlin/Heidelberg, Germany, 2000; pp. 557–566. [Google Scholar]
- Commowick, O.; Arsigny, V.; Isambert, A.; Costa, J.; Dhermain, F.; Bidault, F.; Bondiau, P.; Ayache, N.; Malandain, G. An efficient locally affine framework for the smooth registration of anatomical structures. Med. Image Anal. 2008, 12, 478–481. [Google Scholar] [CrossRef]
- Makki, K.; Borotikar, B.; Garetier, M.; Brochard, S.; BEN Salem, D.; Rousseau, F. In vivo ankle joint kinematics from dynamic magnetic resonance imaging using a registration-based framework. J. Biomech. 2019, 86, 193–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Agostino, P.; Dourthe, B.; Kerkhof, F.; Stockmans, F.; Vereecke, E.E. In vivo kinematics of the thumb during flexion and adduction motion: Evidence for a screw-home mechanism. J. Orthop. Res. 2016, 35, 1556–1564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donati, M.; Camomilla, V.; Vannozzi, G.; Cappozzo, A. Anatomical frame identification and reconstruction for repeatable lower limb joint kinematics estimates. J. Biomech. 2008, 41, 2219–2226. [Google Scholar] [CrossRef]
- Subburaj, K.; Ravi, B.; Agarwal, M. Automated identification of anatomical landmarks on 3D bone models reconstructed from CT scan images. Comput. Med. Imaging Graph. 2009, 33, 359–368. [Google Scholar] [CrossRef]
- Bier, B.; Aschoff, K.; Syben, C.; Unberath, M.; Levenston, M.; Gold, G.; Fahrig, R.; Maier, A. Detecting Anatomical Landmarks for Motion Estimation in Weight-Bearing Imaging of Knees. Tools Algorithms Constr. Anal. Syst. 2018, 11074 LNCS, 83–90. [Google Scholar] [CrossRef]
- Ebner, T.; Stern, D.; Donner, R.; Bischof, H.; Urschler, M. Towards Automatic Bone Age Estimation from MRI: Localization of 3D Anatomical Landmarks. In Implementation of Functional Languages; Springer: Berlin/Heidelberg, Germany, 2014; Volume 17, pp. 421–428. [Google Scholar]
- Amerinatanzi, A.; Summers, R.K.; Ahmadi, K.; Goel, V.K.; Hewett, T.E.; Nyman, J.E. Automated Measurement of Patient-Specific Tibial Slopes from MRI. Bioengineering 2017, 4, 69. [Google Scholar] [CrossRef]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. NeuroImage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rueckert, D.; Sonoda, L.; Hayes, C.; Hill, D.; Leach, M.; Hawkes, D. Nonrigid registration using free-form deformations: Application to breast MR images. IEEE Trans. Med. Imaging 1999, 18, 712–721. [Google Scholar] [CrossRef] [PubMed]
- Ceranka, J.; Verga, S.; Kvasnytsia, M.; Lecouvet, F.; Michoux, N.; De Mey, J.; Raeymaekers, H.; Metens, T.; Absil, J.; Vandemeulebroucke, J. Multi-atlas segmentation of the skeleton from whole-body MRI—Impact of iterative background masking. Magn. Reson. Med. 2020, 83, 1851–1862. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.; Staring, M.; Murphy, K.; Viergever, M.A.; Pluim, J.P.W. elastix: A Toolbox for Intensity-Based Medical Image Registration. IEEE Trans. Med. Imaging 2009, 29, 196–205. [Google Scholar] [CrossRef]
- Xu, L.; Krzyzak, A.; Suen, C. Methods of combining multiple classifiers and their applications to handwriting recognition. IEEE Trans. Syst. Man Cybern. 1992, 22, 418–435. [Google Scholar] [CrossRef] [Green Version]
- Aljabar, P.; Heckemann, R.; Hammers, A.; Hajnal, J.; Rueckert, D. Multi-atlas based segmentation of brain images: Atlas selection and its effect on accuracy. NeuroImage 2009, 46, 726–738. [Google Scholar] [CrossRef]
- Artaechevarria, X.; Munoz-Barrutia, A.; de Solórzano, C.O. Combination Strategies in Multi-Atlas Image Segmentation: Application to Brain MR Data. IEEE Trans. Med. Imaging 2009, 28, 1266–1277. [Google Scholar] [CrossRef]
- GitHub—KCL-BMEIS/NiftySeg, (n.d.). Available online: https://github.com/KCL-BMEIS/NiftySeg (accessed on 25 May 2021).
- Wu, G.; Van Der Helm, F.C.; Veeger, H.E.J.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Insight Journal (ISSN 2327-770X)—Introducing Dice, Jaccard, and Other Label Overlap Measures To ITK, (n.d.). Available online: https://www.insight-journal.org/browse/publication/707 (accessed on 25 May 2021).
- Cheung, W.; Hamarneh, G. N-SIFT: N-Dimensional Scale Invariant Feature Transform for Matching Medical Images. In Proceedings of the 2007 4th IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Arlington, VA, USA, 12–15 May 2007; Institute of Electrical and Electronics Engineers (IEEE): Manhattan, NY, USA, 2007; pp. 720–723. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samples). Biometrika 1965, 52, 591. [Google Scholar] [CrossRef]
- Williams, W.A. Statistical Methods (8th ed.). J. Am. Stat. Assoc. 1991, 86, 834–835. Available online: https://go.gale.com/ps/i.do?p=AONE&sw=w&issn=01621459&v=2.1&it=r&id=GALE%7CA257786252&sid=googleScholar&linkaccess=fulltext (accessed on 25 May 2021). [CrossRef]
- Arabi, H.; Zaidi, H. Comparison of atlas-based techniques for whole-body bone segmentation. Med. Image Anal. 2017, 36, 98–112. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.A.; Elias, J.J.; Tanaka, M.J.; Thawait, G.K.; Demehri, S.; Carrino, J.A.; Cosgarea, A.J. The relationship between tibial tuberosity-trochlear groove distance and abnormal patellar tracking in patients with unilateral patellar instability. Imaging Characteristics of Contralateral Asymptomatic Patellofemoral Joints in Patients with Unilateral Instability. Arthroscopy 2016, 32, 55–61. [Google Scholar] [PubMed]
- Yang, Z.; Fripp, J.; Chandra, S.S.; Neubert, A.; Xia, Y.; Strudwick, M.; Paproki, A.; Engstrom, C.; Crozier, S. Automatic bone segmentation and bone-cartilage interface extraction for the shoulder joint from magnetic resonance images. Phys. Med. Biol. 2015, 60, 1441–1459. [Google Scholar] [CrossRef]
- Wang, K.K.; Zhang, X.; McCombe, D.; Ackland, D.C.; Ek, E.T.; Tham, S.K. Quantitative analysis of in-vivo thumb carpometacarpal joint kinematics using four-dimensional computed tomography. J. Hand Surg. Eur. Vol. 2018, 43, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Jacinto, H.; Valette, S.; Prost, R. Multi-atlas automatic positioning of anatomical landmarks. J. Vis. Commun. Image Represent. 2018, 50, 167–177. [Google Scholar] [CrossRef]
- Brehler, M.; Thawait, G.; Kaplan, J.; Ramsay, J.; Tanaka, M.J.; Demehri, S.; Siewerdsen, J.H.; Zbijewski, W. Atlas-based algorithm for automatic anatomical measurements in the knee. J. Med. Imaging 2019, 6, 026002. [Google Scholar] [CrossRef]
- Baek, S.; Wang, J.-H.; Song, I.; Lee, K.; Lee, J.; Koo, S. Automated bone landmarks prediction on the femur using anatomical deformation technique. Comput. Des. 2012, 45, 505–510. [Google Scholar] [CrossRef]
- Phan, C.-B.; Koo, S. Predicting anatomical landmarks and bone morphology of the femur using local region matching. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 1711–1719. [Google Scholar] [CrossRef]
- Langerak, T.R.; Berendsen, F.F.; Van Der Heide, U.A.; Kotte, A.N.T.J.; Pluim, J.P.W. Multiatlas-based segmentation with preregistration atlas selection. Med. Phys. 2013, 40, 091701. [Google Scholar] [CrossRef] [PubMed]
- Van Rikxoort, E.M.; Isgum, I.; Arzhaeva, Y.; Staring, M.; Klein, S.; Viergever, M.A.; Pluim, J.P.; Van Ginneken, B.B. Adaptive local multi-atlas segmentation: Application to the heart and the caudate nucleus. Med. Image Anal. 2010, 14, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Duc, A.K.H.; Modat, M.; Leung, K.K.; Cardoso, M.J.; Barnes, J.; Kadir, T.; Ourselin, S. Using Manifold Learning for Atlas Selection in Multi-Atlas Segmentation. PLoS ONE 2013, 8, e70059. [Google Scholar] [CrossRef] [Green Version]
- Han, X.; Hibbard, L.S.; Willcut, V. GPU-accelerated, gradient-free MI deformable registration for atlas-based MR brain image segmentation. In Proceedings of the 2009 IEEE Computer Society Conference on Computer Vision and Pattern Recognition Workshops, Miami, FL, USA, 20–25 June 2009; Institute of Electrical and Electronics Engineers (IEEE): Manhattan, NY, USA, 2009; pp. 141–148. [Google Scholar]
- Warfield, S.K.; Zou, K.H.; Wells, W.M. Simultaneous Truth and Performance Level Estimation (STAPLE): An Algorithm for the Validation of Image Segmentation. IEEE Trans. Med. Imaging 2004, 23, 903–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuadra, M.B.; Favre, J.; Omoumi, P. Quantification in Musculoskeletal Imaging Using Computational Analysis and Machine Learning: Segmentation and Radiomics. Semin. Musculoskelet. Radiol. 2020, 24, 50–64. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dynamic Acquisition | Static Acquisitions | |
|---|---|---|
| Knee | ||
| Tube Voltage | 80 kV | 120 kV |
| Tube current | 50 mA | 80 mA |
| Tube rotation time | 0.28 s | 0.28 s |
| Reconstructed slice thickness | 2.5 mm | 2.5 mm |
| Field of View | 500 mm | 500 mm |
| Collimation | 256 × 0.625 mm | 256 × 0.625 mm |
| Dose length product | 107.91 mGycm | 23.06 mGycm |
| * CTDI | 6.74 mGy | 1.44 mGy |
| Thumb | ||
| Tube Voltage | 80 kV | 120 kV |
| Tube current | 50 mA | 80 mA |
| Tube rotation time | 0.28 s | 0.28 s |
| Reconstructed slice thickness | 1.25 mm | 1.25 mm |
| Field of View | 300 mm | 300 mm |
| Collimation | 192 × 0.625 mm | 192 × 0.625 mm |
| Dose length product | 156.45 mGycm | 19.58 mGycm |
| CTDI | 13 mGy | 1.63 mGy |
| Parameter | First Stage | Second Stage | Final Stage |
|---|---|---|---|
| Similarity Metric | (MSD/MI/NCC) * | (MSD/MI/NCC) * | (MSD/MI/NCC) * |
| Regulariser | / | / | Bending energy |
| Transform | Rigid | Affine | B-Spline |
| Multi Resolution levels | 4 | 4 | 4 |
| Number of histogram bins used for MI | 32 | 32 | 32 |
| Sampler | Random | Random | Random |
| Max iterations | 2000 | 1000 | 1000 |
| Number of samples | 2000 | 2000 | 2000 |
| Optimizer | Stochastic Gradient Descent | Stochastic Gradient Descent | Stochastic Gradient Descent |
| Joint | Dice Score | FP | FN | Mean Surface Distance (mm) | Max Surface Distance (mm) | SD Surface Distance (mm) |
|---|---|---|---|---|---|---|
| Thumb | 0.90 ± 0.01 | 0.08 ± 0.02 | 0.14 ± 0.03 | 0.53 ± 0.05 | 4.89 ± 1.25 | 0.68 ± 0.05 |
| Knee | 0.94 ± 0.02 | 0.05 ± 0.02 | 0.06 ± 0.02 | 0.42 ± 0.16 | 4.91 ± 1.13 | 0.66 ± 0.18 |
| Thumb | * AUTO | ||
|---|---|---|---|
| X | Y | Z | |
| Reader 1 | 0.99 | 0.99 | 0.99 |
| Reader 2 | 0.95 | 0.94 | 0.99 |
| Reader 3 | 0.92 | 0.94 | 0.99 |
| Reader AVG | 0.95 | 0.97 | 0.99 |
| Knee | X | Y | Z |
| Reader 1 | 0.99 | 0.72 | 0.96 |
| Reader 2 | 0.99 | 0.76 | 0.95 |
| Reader 3 | 0.99 | 0.83 | 0.94 |
| * Reader AVG | 0.99 | 0.82 | 0.96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keelson, B.; Buzzatti, L.; Ceranka, J.; Gutiérrez, A.; Battista, S.; Scheerlinck, T.; Van Gompel, G.; De Mey, J.; Cattrysse, E.; Buls, N.; et al. Automated Motion Analysis of Bony Joint Structures from Dynamic Computer Tomography Images: A Multi-Atlas Approach. Diagnostics 2021, 11, 2062. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112062
Keelson B, Buzzatti L, Ceranka J, Gutiérrez A, Battista S, Scheerlinck T, Van Gompel G, De Mey J, Cattrysse E, Buls N, et al. Automated Motion Analysis of Bony Joint Structures from Dynamic Computer Tomography Images: A Multi-Atlas Approach. Diagnostics. 2021; 11(11):2062. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112062
Chicago/Turabian StyleKeelson, Benyameen, Luca Buzzatti, Jakub Ceranka, Adrián Gutiérrez, Simone Battista, Thierry Scheerlinck, Gert Van Gompel, Johan De Mey, Erik Cattrysse, Nico Buls, and et al. 2021. "Automated Motion Analysis of Bony Joint Structures from Dynamic Computer Tomography Images: A Multi-Atlas Approach" Diagnostics 11, no. 11: 2062. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112062