
Increased Red Blood Cell Distribution Width in the First Year after Diagnosis Predicts Worsening of Systemic Sclerosis-Associated Interstitial Lung Disease at 5 Years: A Pilot Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Data Collection
2.3. Definition of Progressive Fibrosing ILD
2.4. Statistical Analysis
3. Results
3.1. Patients’ Demographics
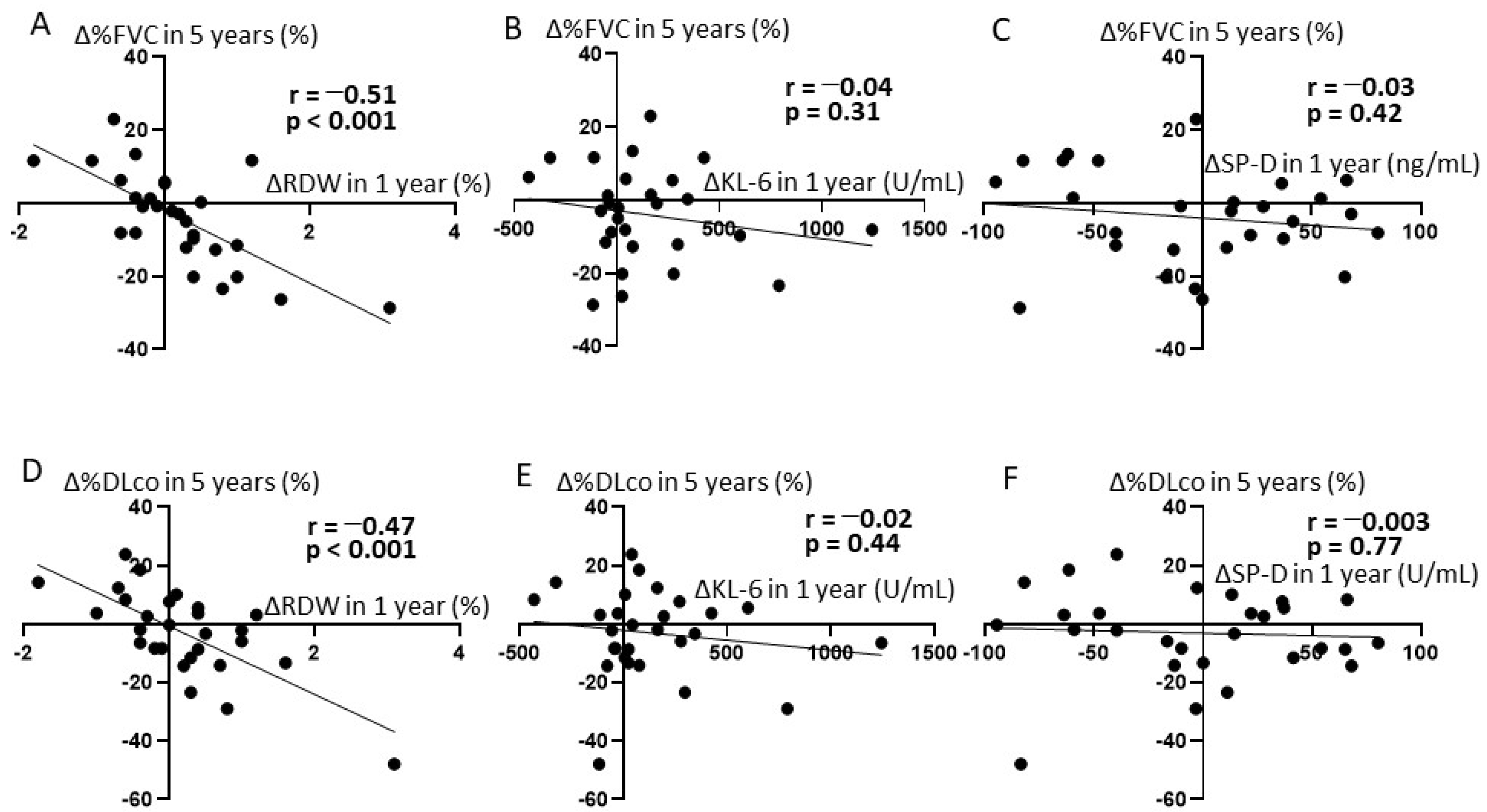
3.2. The Correlation between Short-Term ΔRDW and Long-Term Changes in Pulmonary Function
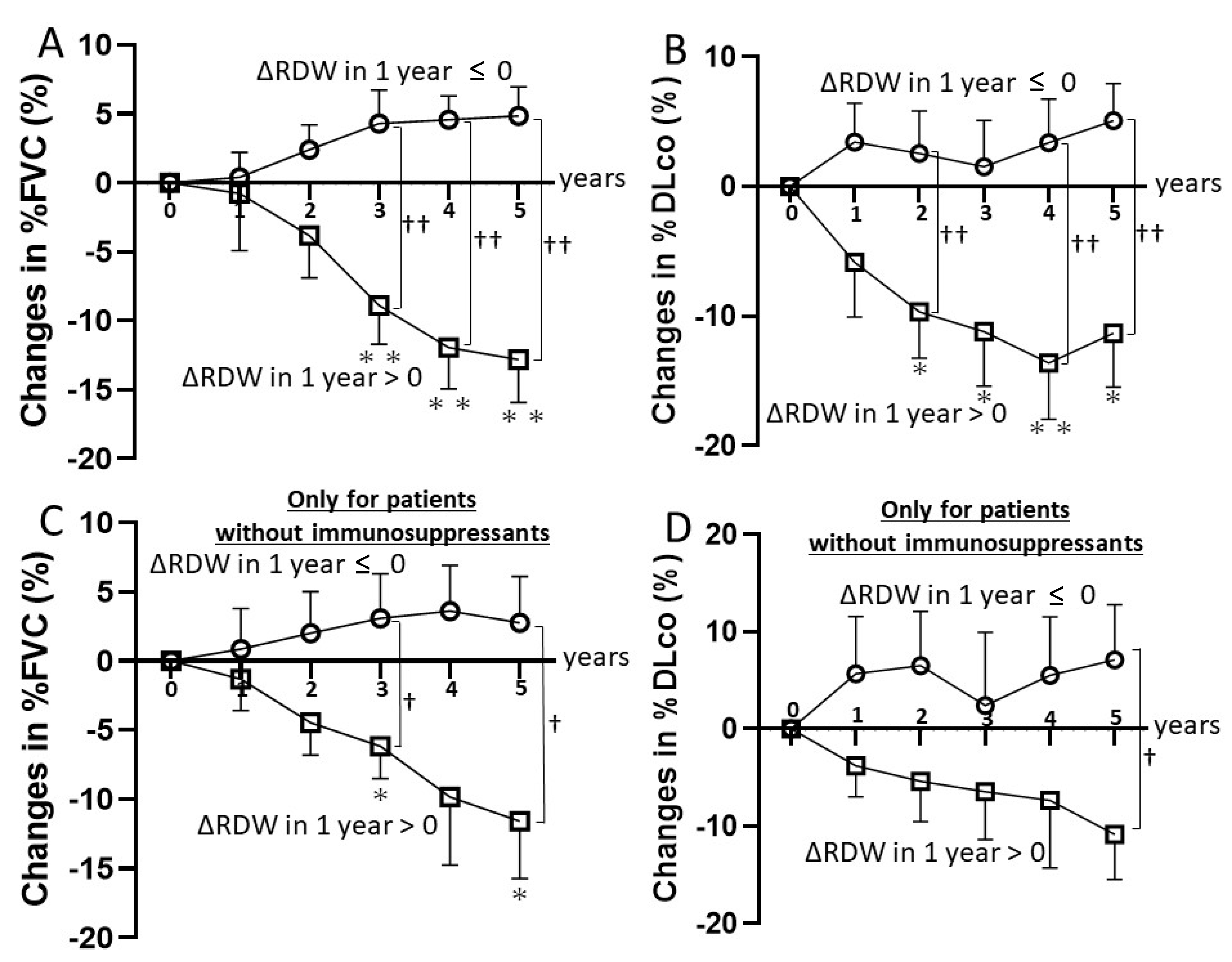
3.3. Clinical Course of SSc-ILD Stratified by ΔRDW
3.4. Sensitivity and Specificity of Identifying Progressive Fibrosing IPF by RDW Elevation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- LeRoy, E.C.; Black, C.; Fleischmajer, R.; Jablonska, S.; Krieg, T.; Medsger, T.A., Jr.; Rowell, N.; Wollheim, F. Scleroderma (systemic sclerosis): Classification, subsets and pathogenesis. J. Rheumatol. 1988, 15, 202–205. [Google Scholar] [PubMed]
- Denton, C.P.; Khanna, D. Systemic sclerosis. Lancet 2017, 390, 1685–1699. [Google Scholar] [CrossRef]
- Allanore, Y.; Simms, R.; Distler, O.; Trojanowska, M.; Pope, J.; Denton, C.P.; Varga, J. Systemic sclerosis. Nat. Rev. Dis. Primers 2015, 1, 15002. [Google Scholar] [CrossRef]
- Tyndall, A.J.; Bannert, B.; Vonk, M.; Airò, P.; Cozzi, F.; Carreira, P.E.; Bancel, D.F.; Allanore, Y.; Müller-Ladner, U.; Distler, O.; et al. Causes and risk factors for death in systemic sclerosis: A study from the EULAR Scleroderma Trials and Research (EUSTAR) database. Ann. Rheum. Dis. 2010, 69, 1809–1815. [Google Scholar] [CrossRef] [Green Version]
- Bouros, D.; Wells, A.U.; Nicholson, A.G.; Colby, T.V.; Polychronopoulos, V.; Pantelidis, P.; Haslam, P.L.; Vassilakis, D.A.; Black, C.M.; Du Bois, R.M. Histopathologic subsets of fibrosing alveolitis in patients with systemic sclerosis and their relationship to outcome. Am. J. Respir. Crit. Care Med. 2002, 165, 1581–1586. [Google Scholar] [CrossRef]
- Rubio-Rivas, M.; Royo, C.; Simeón, C.P.; Corbella, X.; Fonollosa, V. Mortality and survival in systemic sclerosis: Systematic review and meta-analysis. Semin. Arthritis Rheum. 2014, 44, 208–219. [Google Scholar] [CrossRef]
- Volkmann, E.R.; Varga, J. Emerging targets of disease-modifying therapy for systemic sclerosis. Nat. Rev. Rheumatol. 2019, 15, 208–224. [Google Scholar] [CrossRef]
- Merkel, P.A.; Silliman, N.P.; Clements, P.J.; Denton, C.P.; Furst, D.E.; Mayes, M.D.; Pope, J.E.; Polisson, R.P.; Streisand, J.B.; Seibold, J.R. Patterns and predictors of change in outcome measures in clinical trials in scleroderma: An individual patient meta-analysis of 629 subjects with diffuse cutaneous systemic sclerosis. Arthritis Rheum. 2012, 64, 3420–3429. [Google Scholar] [CrossRef] [PubMed]
- Giacomelli, R.; Liakouli, V.; Berardicurti, O.; Ruscitti, P.; Di Benedetto, P.; Carubbi, F.; Guggino, G.; Di Bartolomeo, S.; Ciccia, F.; Triolo, G.; et al. Interstitial lung disease in systemic sclerosis: Current and future treatment. Rheumatol. Int. 2017, 37, 853–863. [Google Scholar] [CrossRef]
- Bonhomme, O.; André, B.; Gester, F.; de Seny, D.; Moermans, C.; Struman, I.; Louis, R.; Malaise, M.; Guiot, J. Biomarkers in systemic sclerosis-associated interstitial lung disease: Review of the literature. Rheumatology 2019, 58, 1534–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lippi, G.; Targher, G.; Montagnana, M.; Salvagno, G.L.; Zoppini, G.; Guidi, G.C. Relation between red blood cell distribution width and inflammatory biomarkers in a large cohort of unselected outpatients. Arch. Pathol. Lab. Med. 2009, 133, 628–632. [Google Scholar] [CrossRef]
- He, Y.; Liu, C.; Zeng, Z.; Ye, W.; Lin, J.; Ou, Q. Red blood cell distribution width: A potential laboratory parameter for monitoring inflammation in rheumatoid arthritis. Clin. Rheumatol. 2018, 37, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Carrio, J.; Alperi-López, M.; López, P.; Alonso-Castro, S.; Ballina-García, F.J.; Suárez, A. Red cell distribution width is associated with cardiovascular risk and disease parameters in rheumatoid arthritis. Rheumatology 2015, 54, 641–646. [Google Scholar] [CrossRef] [Green Version]
- Hassan, S.; Antonelli, M.; Ballou, S. Red cell distribution width: A measure of cardiovascular risk in rheumatoid arthritis patients? Clin. Rheumatol. 2015, 34, 1053–1057. [Google Scholar] [CrossRef] [PubMed]
- Tecer, D.; Sezgin, M.; Kanık, A.; İncel, N.A.; Çimen, Ö.B.; Biçer, A.; Şahin, G. Can mean platelet volume and red blood cell distribution width show disease activity in rheumatoid arthritis? Biomark. Med. 2016, 10, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.D.; Chen, Y.; Zhang, L.; Sun, Y.; Huang, Y.L.; Wang, Q.Q.; Xu, Y.L.; Chen, S.X.; Qin, Q.; Deng, A.M. Red blood cell distribution width is a potential index to assess the disease activity of systemic lupus erythematosus. Clin. Chim. Acta 2013, 425, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.L.; Lin, X.J.; Ni, X.; Wang, J.; Liu, W.; Wei, J. Baseline red blood cell distribution width correlates with disease activity and therapeutic outcomes in patients with systemic lupus erythematosus, irrespective of anemia status. Clin. Lab. 2016, 62, 1841–1850. [Google Scholar] [CrossRef]
- Hu, Z.D.; Sun, Y.; Guo, J.; Huang, Y.L.; Qin, B.D.; Gao, Q.; Qin, Q.; Deng, A.M.; Zhong, R.Q. Red blood cell distribution width and neutrophil/lymphocyte ratio are positively correlated with disease activity in primary Sjögren’s syndrome. Clin. Biochem. 2014, 47, 287–290. [Google Scholar] [CrossRef]
- Farkas, N.; Szabó, A.; Lóránd, V.; Sarlós, D.P.; Minier, T.; Prohászka, Z.; Czirják, L.; Varjú, C. Clinical usefulness of measuring red blood cell distribution width in patients with systemic sclerosis. Rheumatology 2014, 53, 1439–1445. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Mo, H.; Guo, X.; Wang, Q.; Xu, D.; Hou, Y.; Tian, Z.; Liu, Y.; Wang, H.; Lai, J.; et al. Red blood cell distribution width as a related factor of pulmonary arterial hypertension in patients with systemic sclerosis. Clin. Rheumatol. 2018, 37, 979–985. [Google Scholar] [CrossRef]
- Nathan, S.D.; Reffett, T.; Brown, A.W.; Fischer, C.P.; Shlobin, O.A.; Ahmad, S.; Weir, N.; Sheridan, M.J. The red cell distribution width as a prognostic indicator in idiopathic pulmonary fibrosis. Chest 2013, 143, 1692–1698. [Google Scholar] [CrossRef] [PubMed]
- van den Hoogen, F.; Khanna, D.; Fransen, J.; Fischer, C.P.; Shlobin, O.A.; Ahmad, S.; Weir, N.; Sheridan, M.J. 2013 Classification criteria for systemic sclerosis: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2013, 72, 1747–1755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khanna, D.; Furst, D.E.; Clements, P.J.; Allanore, Y.; Baron, M.; Czirjak, L.; Distler, O.; Foeldvari, I.; Kuwana, M.; Matucci-Cerinic, M.; et al. Standardization of the modified Rodnan skin score for use in clinical trials of systemic sclerosis. J. Scleroderma Relat. Disord. 2017, 2, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Khanna, D.; Nagaraja, V.; Tseng, C.-H.; Abtin, F.; Suh, R.; Kim, G.; Wells, A.; Furst, D.E.; Clements, P.J.; Roth, M.D.; et al. Predictors of lung function decline in scleroderma-related interstitial lung disease based on high-resolution computed tomography: Implications for cohort enrichment in systemic sclerosis-associated interstitial lung disease trials. Arthritis Res. Ther. 2015, 17, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goh, N.S.; Hoyles, R.K.; Denton, C.P.; Hansell, D.M.; Renzoni, E.A.; Maher, T.M.; Nicholson, A.G.; Wells, A.U. Short-Term pulmonary function trends are predictive of mortality in interstitial lung disease associated with systemic sclerosis. Arthritis Rheumatol. 2017, 69, 1670–1678. [Google Scholar] [CrossRef]
- Distler, O.; Highland, K.B.; Gahlemann, M.; Azuma, A.; Fischer, A.; Mayes, M.D.; Raghu, G.; Sauter, W.; Girard, M.; Alves, M.; et al. Nintedanib for Systemic Sclerosis-Associated Interstitial Lung Disease. N. Engl. J. Med. 2019, 380, 2518–2528. [Google Scholar] [CrossRef]
- Khanna, D.; Lin, C.J.F.; Furst, D.E.; Goldin, J.; Kim, G.; Kuwana, M.; Allanore, Y.; Matucci-Cerinic, M.; Distler, O.; Shima, Y.; et al. Tocilizumab in systemic sclerosis: A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir. Med. 2020, 8, 963–974. [Google Scholar] [CrossRef]
- Ebata, S.; Yoshizaki, A.; Oba, K.; Kashiwabara, K.; Ueda, K.; Uemura, Y.; Watadani, T.; Fukasawa, T.; Miura, S.; Yoshizaki-Ogawa, A.; et al. Safety and efficacy of rituximab in systemic sclerosis (DESIRES): A double-blind, investigator-initiated, randomised, placebo-controlled trial. Lancet Rheumatol. 2021, 3, e489–e497. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | All (n = 28) | ΔRDW ≤ 0 (n = 13) | ΔRDW > 0 (n = 15) |
|---|---|---|---|
| Female sex, no. (%) | 25 (89.3) | 11 (84.6) | 14 (93.3) |
| Age, years | 53.1 ± 2.5 | 50.7 ± 2.8 | 55.2 ± 4.0 |
| Diffuse cutaneous systemic sclerosis, no. (%) | 22 (78.6) | 10 (76.9) | 12 (80.0) |
| Disease duration, months | 24.6 ± 3.9 | 24.5 ± 6.0 | 24.8 ± 5.1 |
| Range | 3–71 | 3–71 | 5–69 |
| Modified Rodnan skin score | 16.6 ± 1.7 | 17.2 ± 2.6 | 16.1 ± 2.2 |
| Smoking history, % yes | 17.9% | 15.4% | 20.0% |
| RDW, % | 13.6 ± 0.1 | 13.7 ± 0.2 | 13.5 ± 0.2 |
| FVC, % of predicted value | 81.2 ± 2.3 | 80.1 ± 3.6 | 82.1 ± 3.3 |
| DLCO, % of predicted value | 82.0 ± 2.9 | 80.0 ± 4.9 | 84.0 ± 4.0 |
| KL-6, U/mL | 765.4 ± 98.0 | 793.1 ± 144.0 | 673.3 ± 135.2 |
| SP-D, ng/mL | 111.9 ± 12.8 | 117.0 ± 22.9 | 101.3 ± 15.1 |
| Hemoglobin, g/dL | 12.7 ± 0.2 | 12.7 ± 0.3 | 12.9 ± 0.3 |
| Anti-topoisomerase I antibody positive, no. (%) | 20 (71.4) | 9 (69.2) | 11 (73.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ebata, S.; Yoshizaki, A.; Fukasawa, T.; Yoshizaki-Ogawa, A.; Asano, Y.; Kashiwabara, K.; Oba, K.; Sato, S. Increased Red Blood Cell Distribution Width in the First Year after Diagnosis Predicts Worsening of Systemic Sclerosis-Associated Interstitial Lung Disease at 5 Years: A Pilot Study. Diagnostics 2021, 11, 2274. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11122274
Ebata S, Yoshizaki A, Fukasawa T, Yoshizaki-Ogawa A, Asano Y, Kashiwabara K, Oba K, Sato S. Increased Red Blood Cell Distribution Width in the First Year after Diagnosis Predicts Worsening of Systemic Sclerosis-Associated Interstitial Lung Disease at 5 Years: A Pilot Study. Diagnostics. 2021; 11(12):2274. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11122274
Chicago/Turabian StyleEbata, Satoshi, Ayumi Yoshizaki, Takemichi Fukasawa, Asako Yoshizaki-Ogawa, Yoshihide Asano, Kosuke Kashiwabara, Koji Oba, and Shinichi Sato. 2021. "Increased Red Blood Cell Distribution Width in the First Year after Diagnosis Predicts Worsening of Systemic Sclerosis-Associated Interstitial Lung Disease at 5 Years: A Pilot Study" Diagnostics 11, no. 12: 2274. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11122274