
Differential Diagnosis of Abdominal Tuberculosis in the Adult—Literature Review

 ,
,
Abstract
:1. Introduction
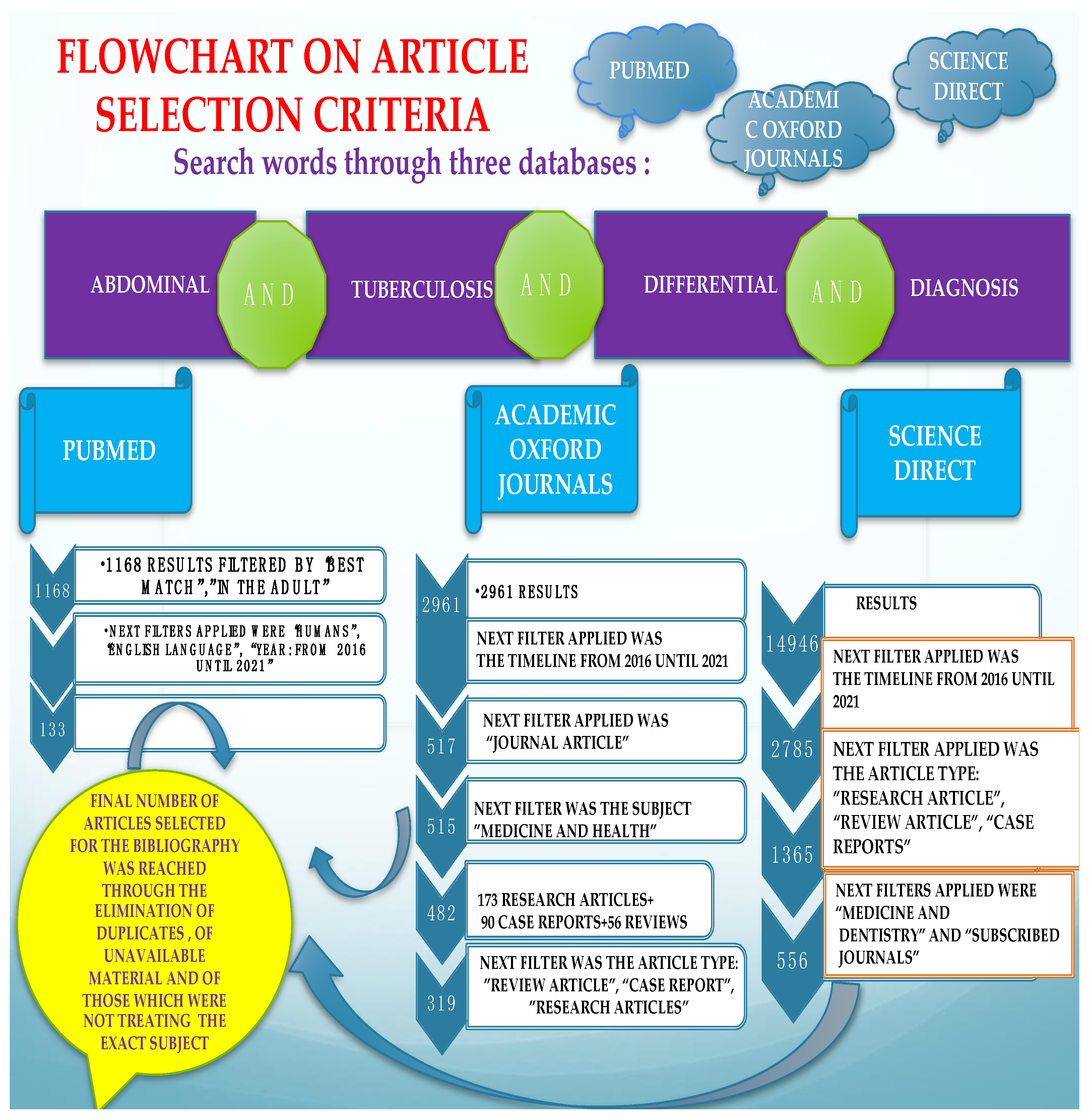
2. Materials and Methods
3. Results
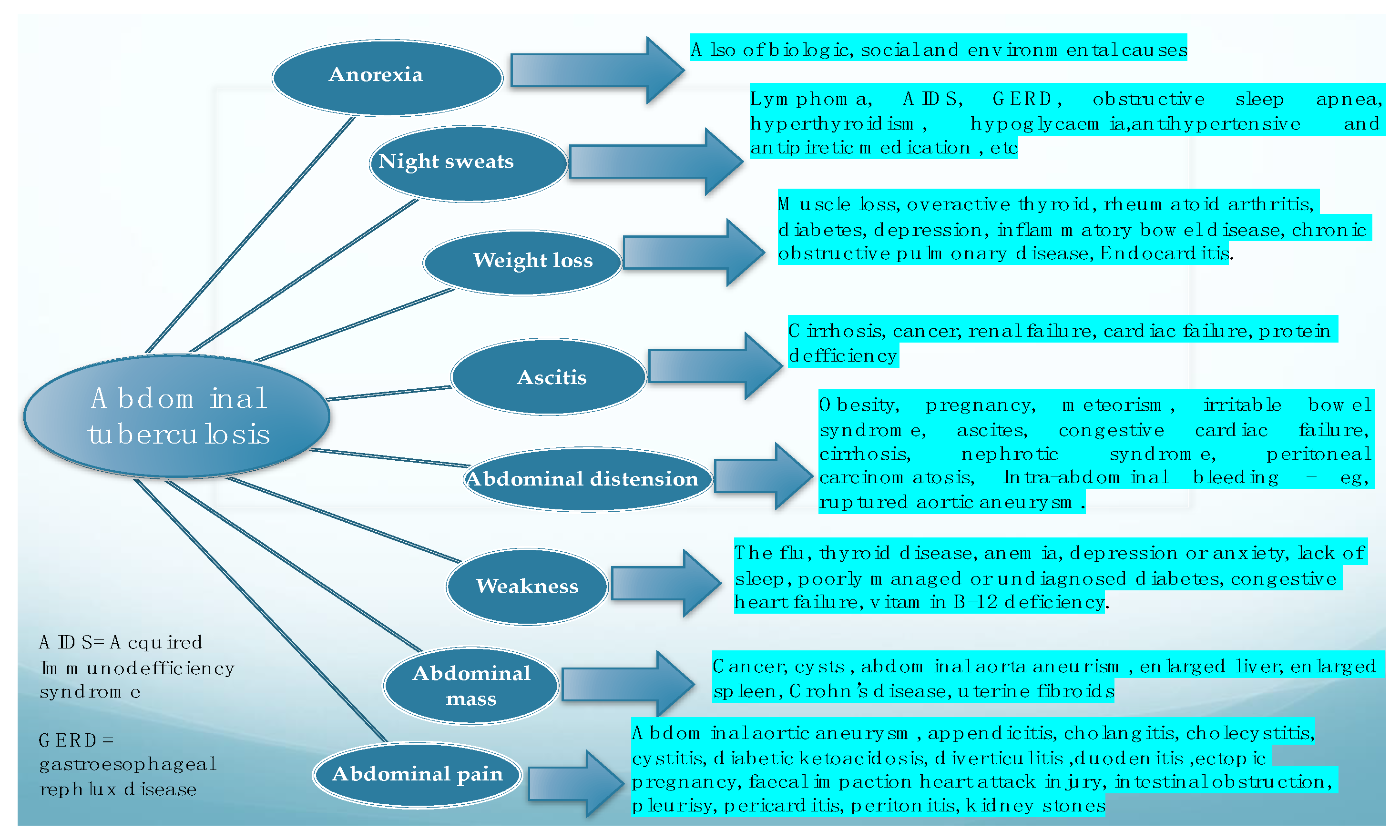
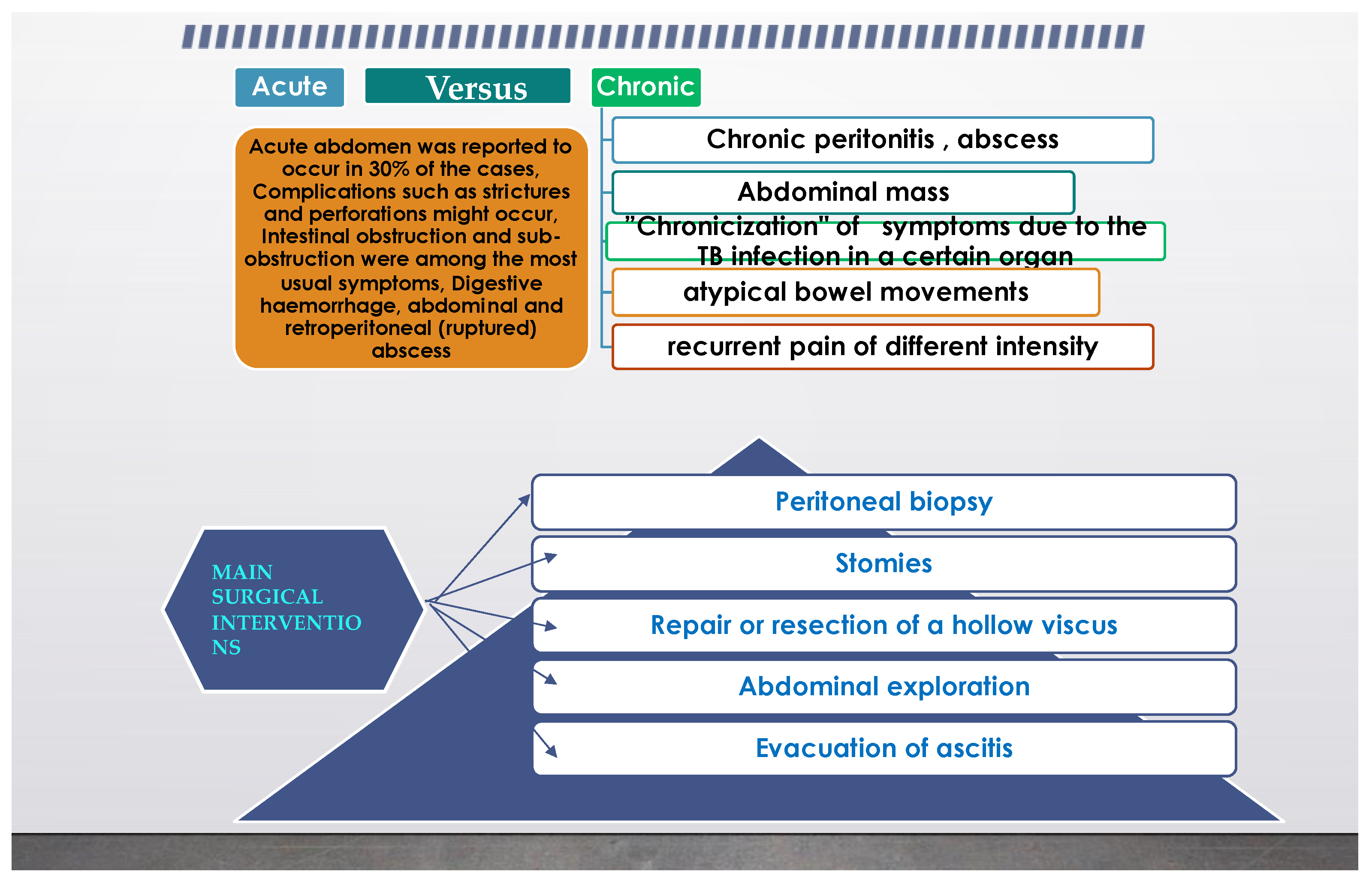
3.1. General Features Regarding the Diagnosis of Abdominal Tuberculosis
3.2. Different Intra-Abdominal Organs and Their Involvement
3.2.1. Oesophageal TB
3.2.2. Gastroduodenal TB
3.2.3. Jejunal, Ileal, and Colonic TB
3.2.4. Rectal TB
3.2.5. Liver and Splenic TB
3.2.6. Pancreatic TB. Approach to Cystic Lesions. Pancreatic Cysts
3.2.7. Calcified Lymphadenopathy and Tuberculous Lymphadenitis
3.2.8. Primary Gallbladder Tuberculosis
3.2.9. Pelvic TB, Retroperitoneal and Extraperitoneal Space Lesions
3.3. Special Challenges in the Differentiation of Abdominal TB
3.3.1. Diagnostic Overlap
3.3.2. TB in Transplant Candidates and Transplant Recipients
3.3.3. Zoonotic Tuberculosis zTB
3.3.4. Challenges Imposed by HIV–TB Coinfection
3.3.5. Pathogenicity and Complexity of the Immune Response in Case of TB Infection
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TB | Tuberculosis |
| MTB | Mycobacterium tuberculosis |
| HIV | Human Immunodeficiency Virus |
| MDR-TB | multi-drug resistant tuberculosis |
| ATM | Atypical mycobacteria |
| AIDS | Acquired Immune Deficiency Syndrome |
| i.v. | Intravenous |
| Pts | Patients |
| CT | computed tomography |
| MRI | Magnetic Resonance Imaging |
| FNAB | fine needle aspiration biopsy |
| FNA | fine needle aspiration |
| CA 19-9 | carbohydrate antigen Ca19-9 |
| CEA | carcinoembryonic antigen |
| ERCP | endoscopic retrograde cholangiopancreatography |
| PCR | polymerase chain reaction |
| IVP | intravenous pyelography |
| TB-IRIS | TB associated immune reconstitution inflammatory syndrome that complicates treatment |
| ART | antiretroviral medication |
References
- Abu-Zidan, F.M.; Sheek-Hussein, M. Diagnosis of abdominal tuberculosis: Lessons learned over 30 years: Pectoral assay. World J. Emerg. Surg. 2019, 14, 33. [Google Scholar] [CrossRef] [Green Version]
- Uzunkoy, A. Diagnosis of abdominal tuberculosis: Experience from 11 cases and review of the literature. World J. Gastroenterol. 2004, 10, 3647. [Google Scholar] [CrossRef] [PubMed]
- Debi, U. Abdominal tuberculosis of the gastrointestinal tract: Revisited. World J. Gastroenterol. 2014, 20, 14831. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.; Thomas, W.M. Diagnosis of abdominal tuberculosis: The importance of laparoscopy. JRSM 2003, 96, 586–588. [Google Scholar] [CrossRef]
- Pattanayak, S.; Behuria, S. Is abdominal tuberculosis a surgical problem? Ann. R. Coll. Surg. Engl. 2015, 97, 414–419. [Google Scholar] [CrossRef] [Green Version]
- Diop, A.D.; Fontarensky, M.; Montoriol, P.-F.; da Ines, D. CT imaging of peritoneal carcinomatosis and its mimics. Diagn. Interv. Imaging 2014, 95, 861–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, S.K.; Jain, S.; Jain, M.; Yaduvanshi, A. Esophageal tuberculosis: Is it so rare? Report of 12 cases and review of the literature. Am. J. Gastroenterol. 2002, 97, 287–291. [Google Scholar] [CrossRef]
- Kocaman, O.; Arabaci, E.; Turkdogan, K.; Danalioglu, A.; Senturk, H.; Ince, A.; Yildiz, K. Endosonography and elastography in the diagnosis of esophageal tuberculosis. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2013, 24, 290–291. [Google Scholar] [CrossRef]
- Plat, V.D.; Bootsma, B.T.; van der Wielen, N.; Straatman, J.; Schoonmade, L.J.; van der Peet, D.L.; Daams, F. The role of tissue adhesives in esophageal surgery, a systematic review of literature. Int. J. Surg. 2017, 40, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Borges, M.C.; Colares, J.K.B.; Lima, D.M.; Fonseca, B.A.L. Advantages and Pitfalls of the Polymerase Chain Reaction in the Diagnosis of Esophageal Ulcers in AIDS Patients. Dig. Dis. Sci. 2009, 54, 1933–1939. [Google Scholar] [CrossRef]
- Jain, S.; Kumar, N.; Das, D.K.; Jain, S.K. Esophageal Tuberculosis. Acta Cytol. 1999, 43, 1085–1090. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, P.; Khan, A.Q.; Lal, R.; Bhadana, U. Gastric tuberculosis. Indian J. Tuberc. 2019, 66, 411–417. [Google Scholar] [CrossRef]
- Barat, M.; Dohan, A.; Dautry, R.; Barral, M.; Boudiaf, M.; Hoeffel, C.; Soyer, P. Mass-forming lesions of the duodenum: A pictorial review. Diagn. Interv. Imaging 2017, 98, 663–675. [Google Scholar] [CrossRef]
- Srisajjakul, S.; Prapaisilp, P.; Bangchokdee, S. Imaging spectrum of nonneoplastic duodenal diseases. Clin. Imaging 2016, 40, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Kedia, S.; Das, P.; Madhusudhan, K.S.; Dattagupta, S.; Sharma, R.; Sahni, P.; Makharia, G.; Ahuja, V. Differentiating Crohn’s disease from intestinal tuberculosis. World J. Gastroenterol. 2019, 25, 418–432. [Google Scholar] [CrossRef]
- Aris, F.; Naim, C.; Bessissow, T.; Amre, R.; Artho, G.P. AIRP Best Cases in Radiologic-Pathologic Correlation: Mycobacterium avium-intracellulare Complex Enteritis. Radiographics 2011, 31, 825–830. [Google Scholar] [CrossRef]
- Chaudhary, P.; Nagpal, A.; Padala, S.B.; Mukund, M.; Bansal, L.K.; Lal, R. Rectal tuberculosis: A systematic review. Indian J. Tuberc. 2021. [Google Scholar] [CrossRef]
- Rakinic, J. Benign Anorectal Surgery. Adv. Surg. 2018, 52, 179–204. [Google Scholar] [CrossRef] [PubMed]
- Puri, A.S.; Vij, J.C.; Chaudhary, A.; Kumar, N.; Sachdev, A.; Malhotra, V.; Malik, V.K.; Broor, S.L. Diagnosis and outcome of isolated rectal tuberculosis. Dis. Colon Rectum 1996, 39, 1126–1129. [Google Scholar] [CrossRef]
- Chaudhary, A.; Gupta, N.M. Colorectal tuberculosis. Dis. Colon Rectum 1986, 29, 738–741. [Google Scholar] [CrossRef]
- Patil, S.; Shah, A.G.; Bhatt, H.; Nalawade, N.; Mangal, A. Tuberculosis of rectum simulating malignancy and presenting as rectal prolapse—A case report and review. Indian J. Tuberc. 2013, 60, 184–185. [Google Scholar] [PubMed]
- Berzigotti, A. Non-invasive evaluation of portal hypertension using ultrasound elastography. J. Hepatol. 2017, 67, 399–411. [Google Scholar] [CrossRef] [PubMed]
- Sangster, G.P.; Malikayil, K.; Donato, M.; Ballard, D.H. MDCT Findings of Splenic Pathology. Curr. Probl. Diagn. Radiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Khan, Z.; Chetty, R. A review of the cysts of the spleen. Diagn. Histopathol. 2016, 22, 479–484. [Google Scholar] [CrossRef]
- Ricci, Z.J.; Oh, S.K.; Chernyak, V.; Flusberg, M.; Rozenblit, A.M.; Kaul, B.; Stein, M.W.; Mazzariol, F.S. Improving diagnosis of atraumatic splenic lesions, part I: Nonneoplastic lesions. Clin. Imaging 2016, 40, 769–779. [Google Scholar] [CrossRef]
- Gupta, A. Splenic tuberculosis: A comprehensive review of literature. Pol. Prz. Chir. 2018, 90, 49–51. [Google Scholar] [CrossRef]
- Ais, G.; Ortega, M.; Esteban, F.; González, A.; Manzanares, J. Hypersplenism secondary to splenic tuberculosis. Rev. Esp. Enferm. Dig. Organo Of. Soc. Esp. Patol. Dig. 1993, 83, 397–399. [Google Scholar]
- Cho, S.B. Pancreatic tuberculosis presenting with pancreatic cystic tumor: A case report and review of the literature. Korean J. Gastroenterol. Taehan Sohwagi Hakhoe Chi 2009, 53, 324–328. [Google Scholar] [CrossRef] [Green Version]
- Ray, S.; Das, K.; Mridha, A.R. Pancreatic and peripancreatic nodal tuberculosis in immunocompetent patients: Report of three cases. JOP J. Pancreas 2012, 13, 667–670. [Google Scholar] [CrossRef]
- Irfan, M.; Thiavalappil, F.; Nagaraj, J.; Brown, T.H.; Roberts, D.; Mcknight, L.; Harrison, N.K. Tuberculous pancreatitis complicated by ruptured splenic artery pseudoaneurysm. Monaldi Arch. Chest Dis. 2013, 79, 134–135. [Google Scholar] [CrossRef] [Green Version]
- D’Cruz, S.; Sachdev, A.; Kaur, L.; Handa, U.; Bhalla, A.; Lehl, S.S. Fine needle aspiration diagnosis of isolated pancreatic tuberculosis. A case report and review of literature. JOP J. Pancreas 2003, 4, 158–162. [Google Scholar]
- Ladumor, H.; Al-Mohannadi, S.; Ameerudeen, F.S.; Ladumor, S.; Fadl, S. TB or not TB: A comprehensive review of imaging manifestations of abdominal tuberculosis and its mimics. Clin. Imaging 2021, 76, 130–143. [Google Scholar] [CrossRef] [PubMed]
- Fritscher-Ravens, A.; Ghanbari, A.; Topalidis, T.; Pelling, M.; Kon, O.M.; Patel, K.; Arlt, A.; Bhowmik, A. Granulomatous mediastinal adenopathy: Can endoscopic ultrasound-guided fine-needle aspiration differentiate between tuberculosis and sarcoidosis? Endoscopy 2011, 43, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Huang, X.; Yang, Q.; He, J. Calcified peripancreatic lymph nodes in pancreatic and hepatic tuberculosis mimicking pancreatic malignancy: A case report and review of literature. Medicine 2018, 97, e12255. [Google Scholar] [CrossRef]
- Gupta, A.; Gupta, A.; Anjum, R.; Agrawal, S.; Mallik, D. A comprehensive review on Primary gallbladder tuberculosis. Pol. J. Surg. 2018, 90, 10–12. [Google Scholar] [CrossRef]
- Yates, J.A.; Collis, O.A.; Sueblinvong, T.; Collis, T.K. Red Snappers and Red Herrings: Pelvic Tuberculosis Causing Elevated CA 125 and Mimicking Advanced Ovarian Cancer. A Case Report and Literature Review. Hawai’i J. Med. Public Health J. Asia Pac. Med. Public Health 2017, 76, 220–224. [Google Scholar]
- Wang, B.; Liu, W.; Shao, Z.; Zeng, X. Retroperitoneal metastatic poorly differentiated carcinoma with β-human chorionic gonadotropin secretion presenting as a psoas abscess: A case report and review of the literature. Medicine 2017, 96, e6837. [Google Scholar] [CrossRef] [PubMed]
- Moetamin, A.; Bhatia, K. Clinical aspects of endocrinology: Parathyroid and adrenal gland disorders. Anaesth. Intensive Care Med. 2017, 18, 465–471. [Google Scholar] [CrossRef]
- Epstein, D.; Watermeyer, G.; Kirsch, R. Review article: The diagnosis and management of Crohn’s disease in populations with high-risk rates for tuberculosis. Aliment. Pharmacol. Ther. 2007, 25, 1373–1388. [Google Scholar] [CrossRef]
- Mayito, J.; Andia, I.; Belay, M.; Jolliffe, D.A.; Kateete, D.P.; Reece, S.T.; Martineau, A.R. Anatomic and Cellular Niches for Mycobacterium tuberculosis in Latent Tuberculosis Infection. J. Infect. Dis. 2019, 219, 685–694. [Google Scholar] [CrossRef] [Green Version]
- Macedo Couto, R.; Ranzani, O.T.; Waldman, E.A. Zoonotic Tuberculosis in Humans: Control, Surveillance, and the One Health Approach. Epidemiol. Rev. 2019, 41, 130–144. [Google Scholar] [CrossRef]
- Moyo, M.; Lebina, L.; Milovanovic, M.; MacPherson, P.; Michel, A.; Martinson, N. Tuberculosis patients at the human-animal interface: Potential zooanthroponotic and zoonotic transmission. One Health 2021, 13, 100319. [Google Scholar] [CrossRef]
- Davis, W.C.; Abdellrazeq, G.S.; Mahmoud, A.H.; Park, K.T.; Elnaggar, M.M.; Donofrio, G.; Hulubei, V.; Fry, L.M. Advances in Understanding of the Immune Response to Mycobacterial Pathogens and Vaccines through Use of Cattle and Mycobacterium avium subsp. paratuberculosis as a Prototypic Mycobacterial Pathogen. Vaccines 2021, 9, 1085. [Google Scholar] [CrossRef] [PubMed]
- Quinn, C.M.; Poplin, V.; Kasibante, J.; Yuquimpo, K.; Gakuru, J.; Cresswell, F.V.; Bahr, N.C. Tuberculosis IRIS: Pathogenesis, Presentation, and Management across the Spectrum of Disease. Life 2020, 10, 262. [Google Scholar] [CrossRef]
- Zhai, W.; Wu, F.; Zhang, Y.; Fu, Y.; Liu, Z. The Immune Escape Mechanisms of Mycobacterium Tuberculosis. Int. J. Mol. Sci. 2019, 20, 340. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Consolidated Guidelines on Tuberculosis; World Health Organization (WHO): Geneva, Switzerland, 2021. [Google Scholar]
- Flores-Ibarra, A.A.; Ochoa-Vázquez, M.D.; Sánchez-Tec, G.A. Diagnostic strategies in the Tuberculosis Clinic of the Hospital General La Raza National Medical Center. Rev. Med. Inst. Mex. Seguro Soc. 2016, 54, 122–127. [Google Scholar] [PubMed]
- Kanaan, R.; Farkas, N.; Hegyi, P.; Soós, A.; Hegyi, D.; Németh, K.; Horváth, O.; Tenk, J.; Mikó, A.; Szentesi, A.; et al. Rats sniff out pulmonary tuberculosis from sputum: A diagnostic accuracy meta-analysis. Sci. Rep. 2021, 11, 1877. [Google Scholar] [CrossRef] [PubMed]
- Santos, N.C.D.S.; Scodro, R.B.D.L.; Sampiron, E.G.; Ieque, A.L.; Carvalho, H.C.D.; Santos, T.D.S.; Ghiraldi Lopes, L.D.; Campanerut-Sá, P.A.Z.; Siqueira, V.L.D.; Caleffi-Ferracioli, K.R.; et al. Minimum Bactericidal Concentration Techniques in Mycobacterium tuberculosis: A Systematic Review. Microb. Drug Resist. 2020, 26, 752–765. [Google Scholar] [CrossRef]
- Kwak, M.; Lee, W.K.; Lim, Y.J.; Lee, S.H.; Ryoo, S. Systematic review and meta-analysis of the nitrate reductase assay for drug susceptibility testing of Mycobacterium tuberculosis and the detection limits in liquid medium. J. Microbiol. Methods 2017, 141, 1–9. [Google Scholar] [CrossRef]
- Ledesma, J.R.; Ma, J.; Zheng, P.; Ross, J.M.; Vos, T.; Kyu, H.H. Interferon-gamma release assay levels and risk of progression to active tuberculosis: A systematic review and dose-response meta-regression analysis. BMC Infect. Dis. 2021, 21, 467. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Xu, Y.; Cao, X.; Chen, X.; Zhong, Y. Diagnostic value of interferon- γ release assay in HIV-infected individuals complicated with active tuberculosis: A systematic review and meta-analysis. Epidemiol. Infect. 2021, 149, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Salimiyan Rizi, K.; Aryan, E.; Meshkat, Z.; Ranjbar, G.; Sankian, M.; Ghazvini, K.; Farsiani, H.; Pourianfar, H.R.; Rezayi, M. The overview and perspectives of biosensors and Mycobacterium tuberculosis: A systematic review. J. Cell. Physiol. 2021, 236, 1730–1750. [Google Scholar] [CrossRef] [PubMed]
- Arora, G.; Misra, R.; Sajid, A. Model Systems for Pulmonary Infectious Diseases: Paradigms of Anthrax and Tuberculosis. Curr. Top. Med. Chem. 2017, 17, 2077–2099. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
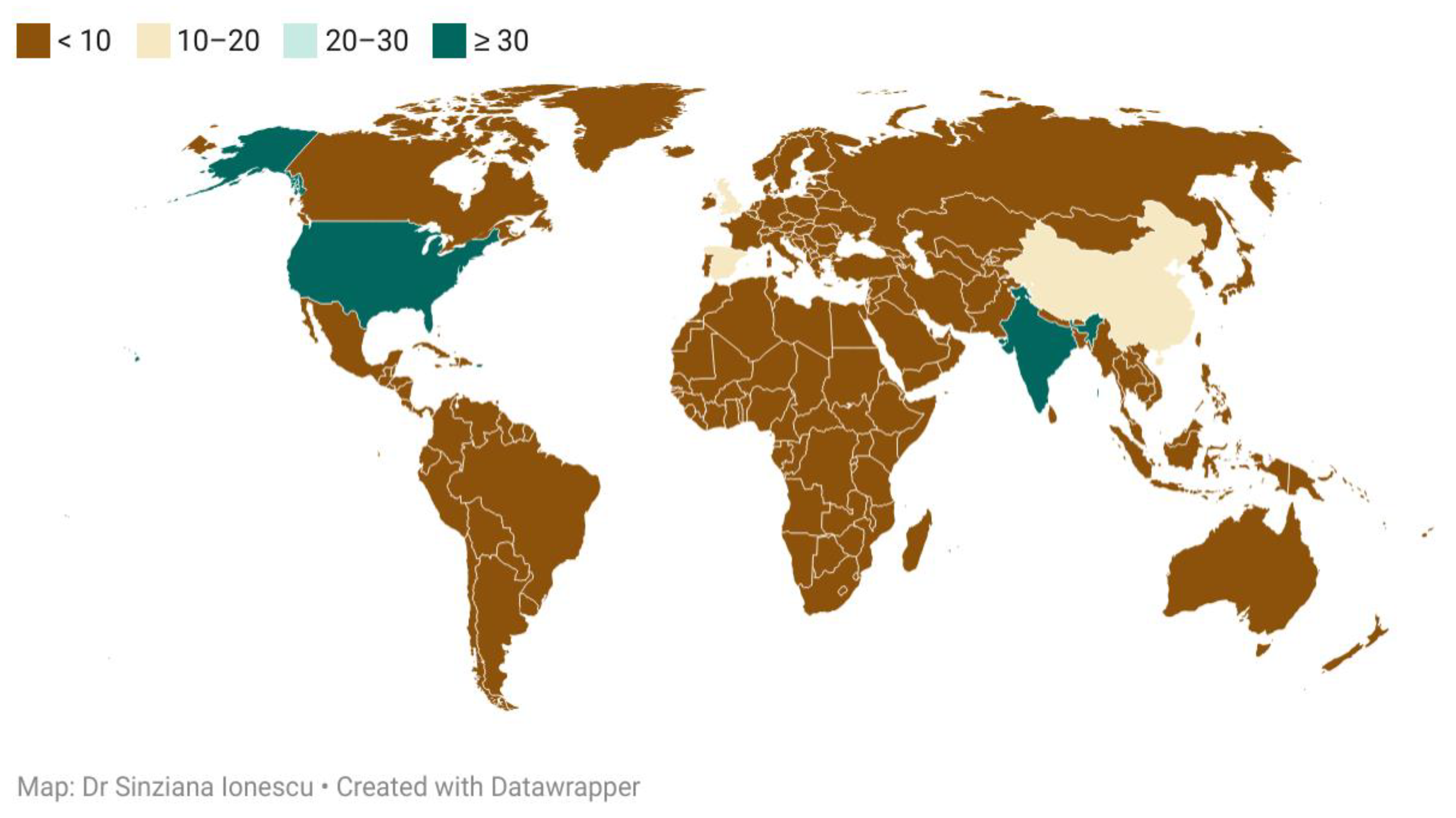
| Country Name | Number of Articles | Country Name | Number of Articles |
|---|---|---|---|
| Belgium | 1 | United States of America | 36 |
| Cameroon | 1 | India | 32 |
| Colombia | 1 | China | 17 |
| Democratic Republic of Congo | 1 | United Kingdom | 14 |
| Ecuador | 1 | Spain | 11 |
| Indonesia | 1 | Netherlands | 9 |
| Ireland | 1 | D. P. R. of Korea | 8 |
| Kosovo | 1 | Japan | 7 |
| New Zealand | 1 | France | 6 |
| Nigeria | 1 | Germany | 6 |
| Peru | 1 | Pakistan | 5 |
| Portugal | 1 | Brazil | 4 |
| Qatar | 1 | Australia | 3 |
| R. B. de Venezuela | 1 | South Africa | 3 |
| Romania | 1 | Turkey | 3 |
| Rwanda | 1 | United Arab Emirates | 3 |
| Saudi Arabia | 1 | Canada | 2 |
| Sudan | 1 | Denmark | 2 |
| Tanzania | 1 | Israel | 2 |
| Thailand | 1 | Italy | 2 |
| Uganda | 1 | Mexico | 2 |
| Zambia | 1 | Singapore | 2 |
| Name of the Study, Journal Where It Was Published, and Year | Investigations Used, Purpose of the Study | Findings | Number of Cases |
|---|---|---|---|
| Kocaman, Turk. J. Gastroenterol., 2013 [8] | Endosonography and elastography in the diagnosis of esophageal tuberculosis | Esophageal tuberculosis | Case report |
| V. D. Plat, Journal Of Surgery, 2017 [9] | Comparing endoscopic repair with surgical repair in brochoesophageal fistulas | Fistulas were caused by postoperative complications or pulmonary TB | 16 cases |
| S.K. Jain, The American Journal of Gastroenterology, 2002 [7] | Upper endoscopy Pathology exam Cytology | Pts with esophageal TB constituted 0.5% of pts with dysphagia and 1.3% of all pts with abnormal esophagoscopic findings | 12 cases |
| M.C. Borges, Dig. Dis. Sci., 2009 [10] | Evaluate the role of PCR in the etiology of ulcers in HIV-1 infected pts | 96 biopsies from HIV infected pts were processed by specific PCR | 79 cases |
| S.Jain, Acta Cytol., 1999 [11] | To study the utility of endoscopic cytology in the diagnosis of esophageal TB in clinically unsuspected cases | 228 cases of esophageal lesions | 8 cases |
| Review | Key-Features |
|---|---|
| P. Chaudhary, Indian Journal of Tuberculosis, 2019 [12] | Gastric TB is rare It mimics gastric carcinoma Responds well to conservative management Requires surgery for complications |
| M. Barat, Diagnostic and Interventional Imaging, 2017 [13] | Duodenal Tb is rare, the disease more commonly affects the ileocecum, colon, and jejunum, while more than 90% of duodenal TB was also found to have co-infections with other parts of the intestine On CT, duodenal Tb presents as strictures, extrinsic compression, polypoidal intraluminal mass, and duodenal ulcerations, associated with multiple hypoattenuating lymph nodes |
| S. Srisajjakul, Clinical Imaging, 2016 [14] | Duodenitis Aortoduodenal fistula |
| Study | Key-Features |
|---|---|
| Poras Chaudhary, Indian Journal of Tuberculosis, 2021 [17] | Rare, commonly misdiagnosed, curable with chemotherapy, surgery for complications |
| Jan Rakinic, Advances in Surgery, Volume 52, Issue 1, 2018 [18] | Anorectal fistulas |
| Puri, A.S., Dis. Colon Rectum, 1996, [19] | Rectal Tb can cause strictures |
| Chaudhary, A., Dis. Colon Rectum, 1986 [20] | Two cases of rectal strictures |
| Patil, S., Indian J. Tuberc., 2013 [21] | Rectal prolapse |
| Study | Form of TB Encountered in the Study |
|---|---|
| MDCT Findings of splenic pathology, Sangster, 2021 [23] | Microabscess, splenomegaly |
| A review of the cysts of the spleen, Khan, 2016 [24] | Peliosis |
| Improving diagnosis of atraumatic splenic lesions, Ricci, 2016 [25] | Calcified granuloma and peliosis |
| Splenic tuberculosis: a comprehensive review of literature, Gupta, 2018 [26] | Small splenomegaly, abscess+/- ascitis |
| Hypersplenism secondary to splenic tuberculosis, Ais, 1993 [27] | Hypersplenism |
| Main Author | Main features of the research | Main aspects followed |
| Ray et al., JOP, 2012 [29] | Pancreatic and peripancreatic nodal tuberculosis in immunocompetent patients: report of 3 cases | Description of pancreatic TB with contrast-enhanced ultrasound |
| Irfan M. Monaldi Arch. Chest Dis. 2013 [30] | Tb pancreatitis complicating with a ruptured splenic artery pseudoaneurysm | Emergency laparotomy for haemorrhage |
| D. Cruz S. JOP, 2003 [31] | Pancreatic TB | FNA biopsy |
| Method, Category | Main Features | |
|---|---|---|
| First line is auramine phenol staining, relying on the autofluorescence of the bacterial wall, followed in some labs by Ziehl-Neelsen staining [47,48] | |
| Gold standard for diagnosis, a positive culture is achieved in 2/3 of cases of extrapulmonary TB (automated liquid culture or solid culture Lowenstein Jensen) [49,50] | |
| Tuberculin skin testing or interferon gamma release assay [51,52] | |
| Nucleic acid amplification tests or whole genome sequencing tests, used for the detection of mycobacteria, identification of the most common mutations, strain typing | |
| D.1. Initial tests for diagnosis of TB with drug-resistance detection |
| The Xpert MTB/RIF assay is a cartridge-based automated test that uses real-time polymerase chain reaction (PCR) on the GeneXpert platform to identify MTBC and mutations associated with RIF resistance directly from sputum specimens in less than 2 h. |
| The Xpert MTB/RIF Ultra assay (hereafter called Xpert Ultra) uses the same GeneXpert platform as the Xpert MTB/RIF test and was developed to improve the sensitivity and reliability of detection of MTBC and RIF resistance | |
| The Truenat MTB and MTB Plus assays use chip-based real-time micro PCR for the semiquantitative detection of MTBC directly from sputum specimens and can report results in under an hour. The assays use automated, battery- operated devices that extract, amplify, and detect specific genomic DNA loci. | |
| The moderate complexity of the automated NAATs class of tests includes rapid and accurate tests for the detection of pulmonary TB from respiratory samples. | |
| D.2. Initial tests for diagnosis of TB without drug-resistance detection |
| The TB-LAMP assay is designed to detect MTBC directly from sputum specimens. This is a manual assay that provides results in less than 1 hour, does not require sophisticated instrumentation, and can be used at the peripheral health centre level, given biosafety requirements similar to those for sputum-smear microscopy. TB-LAMP does not detect resistance to anti-TB drugs. |
| The urine LF-LAM is an immunocapture assay based on the detection of the mycobacterial LAM antigen in urine; it is a potential point-of-care test for certain populations being evaluated for TB. Although the assay lacks sensitivity, it can be used as a fast, bedside, rule-in test for HIV-positive individuals, especially in urgent cases, where a rapid TB diagnosis is critical for the patient’s survival. | |
| D.3. Follow-on diagnostic tests for detection of additional drug resistance |
| The “first in class” product for low complexity automated NAATs for detection of resistance to INH and second-line anti-TB drugs is the Xpert MTB/XDR Assay (Cepheid, Sunnyvale, USA). This test uses a cartridge designed for the GeneXpert instrument to detect resistance to INH, FQs, ETO, and second-line injectable drugs (AMK, kanamycin and capreomycin) |
| LPAs are a family of DNA strip-based tests that detect mutations associated with drug resistance. They do this either directly, through binding DNA amplification products (amplicons) to probes targeting the most commonly occurring mutations (MUT probes), or indirectly, inferred by the lack of binding of the amplicons to the corresponding wild-type probes. | |
| The “first in class” product for this class is the GenoScholar PZA-TB (Nipro, Osaka, Japan) for the detection of resistance to PZA. The GenoScholar PZA-TB test is based on the same principle as the FL-LPA and SL-LPA but requires the use of a large number of hybridization probes to cover the full pncA gene (>700 base pairs [bp]) | |
| The greatest potential and widespread use of biosensors for diagnosing Mycobacterium tuberculosis and drug resistance belong to DNA electrochemical biosensors (isoniazid and rifampin strains).Biosensors are increasingly being used to detect resistant strains of anti-TB antibiotics with high sensitivity and accuracy, and the speed of these sensory methods is also critical [53]. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ionescu, S.; Nicolescu, A.C.; Madge, O.L.; Marincas, M.; Radu, M.; Simion, L. Differential Diagnosis of Abdominal Tuberculosis in the Adult—Literature Review. Diagnostics 2021, 11, 2362. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11122362
Ionescu S, Nicolescu AC, Madge OL, Marincas M, Radu M, Simion L. Differential Diagnosis of Abdominal Tuberculosis in the Adult—Literature Review. Diagnostics. 2021; 11(12):2362. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11122362
Chicago/Turabian StyleIonescu, Sinziana, Alin Codrut Nicolescu, Octavia Luciana Madge, Marian Marincas, Madalina Radu, and Laurentiu Simion. 2021. "Differential Diagnosis of Abdominal Tuberculosis in the Adult—Literature Review" Diagnostics 11, no. 12: 2362. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11122362