
Salivary Inflammatory Molecules as Biomarkers of Sleep Alterations: A Scoping Review

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
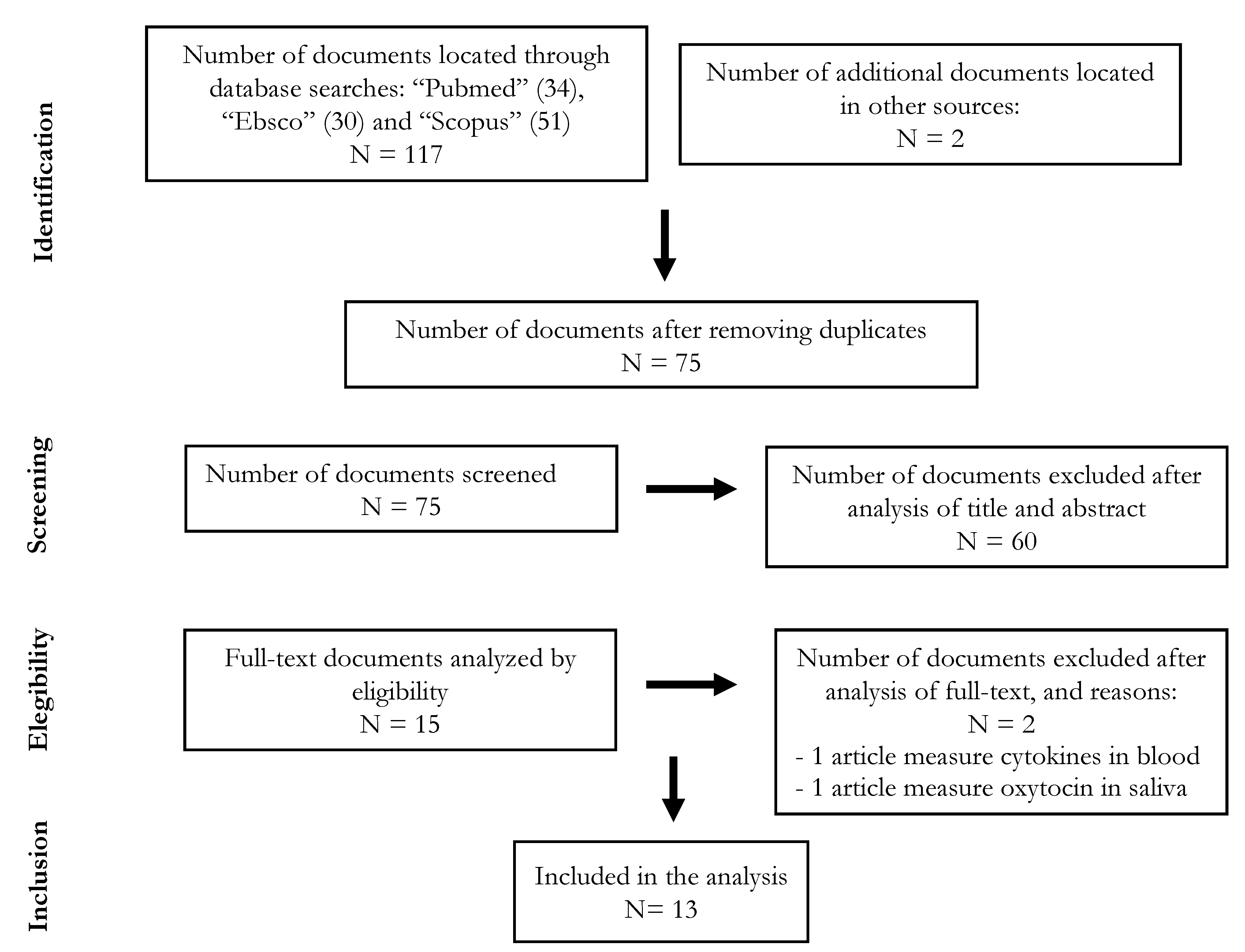
2.1. Search Process
2.2. Inclusion and Exclusion Criteria
2.3. Studies Selection and Analysis
2.4. Salivary Inflammatory Markers Measured in the Analyzed Studies
2.5. Sleep Detection Methods Used the Analyzed Studies
- -
- -
- -
- -
- -
- The 10-item sleep-wake problem subscale of the School Sleep Habits Survey (SSHS) assesses the frequency with which sleep is interrupted, ranging from 1 (never) to 5 (every day). Higher scores on this instrument indicate greater sleep disturbance. The SSHS has shown strong psychometric properties [67] and was used in one [46] of the articles analyzed in this review. Sleep diaries represent another subjective measurement that is completed over a longer period of time (typically several times during one to two weeks) and were used in two studies including in the review [47,52].
2.6. Evaluation of the Quality of the Methodology
- Define the source of information (survey, record review).
- List inclusion and exclusion criteria for exposed and unexposed subjects (cases and controls) or refer to previous publications.
- Indicate time period used for identifying patients.
- Indicate whether or not subjects were consecutive if not population-based.
- Indicate if evaluators of subjective components of study were masked to other aspects of the status of the participants.
- Describe any assessments undertaken for quality assurance purposes (e.g., test/retest of primary outcome measurements).
- Explain any patient exclusions from analysis.
- Describe how confounding was assessed and/or controlled.
- If applicable, explain how missing data were handled in the analysis.
- Summarize patient response rates and completeness of data collection.
- Clarify what follow-up, if any, was expected and the percentage of patients for which incomplete data or follow-up was obtained.
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Crowley, K. Sleep and Sleep Disorders in Older Adults. Neuropsychol. Rev. 2011, 21, 41–53. [Google Scholar] [CrossRef]
- Muñoz-Pareja, M.; Loch, M.R.; Santos, H.G.; Bortoletto, M.S.S.; González, A.D.; Andrade, S.M. Factores asociados a mala calidad de sueño en población brasilera a partir de los 40 años de edad: Estudio VIGICARDIO. Gac. Sanit. 2016, 30, 444–450. [Google Scholar] [CrossRef] [Green Version]
- Goel, N.; Rao, H.; Durmer, J.S.; Dinges, D.F. Neurocognitive Consequences of Sleep Deprivation. Semin. Neurol. 2009, 29, 320–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEwen, B.S.; Karatsoreos, I.N. Sleep Deprivation and Circadian Disruption: Stress, Allostasis, and Allostatic Load. Sleep Med. Clin. 2015, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Tobaldini, E.; Costantino, G.; Solbiati, M.; Cogliati, C.; Kara, T.; Nobili, L.; Montano, N. Sleep, sleep deprivation, autonomic nervous system and cardiovascular diseases. Neurosci. Biobehav. Rev. 2017, 74, 321–329. [Google Scholar] [CrossRef]
- Ting, L.; Malhotra, A. Disorders of Sleep: An Overview. Prim. Care 2005, 32, 305–318. [Google Scholar] [CrossRef] [Green Version]
- Bonnet, M.H.; Arand, D.L. Clinical effects of sleep fragmentation versus sleep deprivation. Sleep Med. Rev. 2003, 7, 297–310. [Google Scholar] [CrossRef] [Green Version]
- Martin, S.E.; Wraith, P.K.; Deary, I.J.; Douglas, N. The effect of nonvisible sleep fragmentation on daytime function. Am. J. Respir. Crit. Care Med. 1997, 155, 1596–1601. [Google Scholar] [CrossRef] [PubMed]
- Stepanski, E.J. The Effect of Sleep Fragmentation on Daytime Function. Sleep 2002, 25, 268–276. [Google Scholar] [CrossRef]
- Engleman, H.M.; Cheshire, K.E.; Deary, I.J.; Douglas, N.J. Daytime sleepiness, cognitive performance and mood after continuous positive airway pressure for the sleep apnoea/hypopnoea syndrome. Thorax 1993, 48, 911–914. [Google Scholar] [CrossRef] [Green Version]
- Durmer, J.S.; Dinges, D.F. Neurocognitive Consequences of Sleep Deprivation. Semin. Neurol. 2005, 25, 117–129. [Google Scholar] [CrossRef] [Green Version]
- Jackson, M.L.; Howard, M.E.; Barnes, M. Cognition and daytime functioning in sleep-related breathing disorders. Prog. Brain Res. 2011, 190, 53–68. [Google Scholar] [CrossRef]
- Depner, C.M.; Stothard, E.R.; Wright, K.P., Jr. Metabolic Consequences of Sleep and Circadian Disorders. Curr. Diabetes Rep. 2014, 14, 507. [Google Scholar] [CrossRef]
- Kripke, D.F.; Garfinkel, L.; Wingard, D.L.; Klauber, M.R.; Marler, M.R. Mortality Associated with Sleep Duration and Insomnia. Arch. Gen. Psychiatry 2002, 59, 131–136. [Google Scholar] [CrossRef] [Green Version]
- Besedovsky, L.; Lange, T.; Born, J. Sleep and immune function. Pflügers Archiv. Eur. J. Physiol. 2012, 463, 121–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, T.; Dimitrov, S.; Born, J. Effects of sleep and circadian rhythm on the human immune system. Ann. N. Y. Acad. Sci. 2010, 1193, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Haus, E.; Smolensky, M.H. Biologic Rhythms in the Immune System. Chronobiol. Int. 1999, 16, 581–622. [Google Scholar] [CrossRef] [PubMed]
- Chennaoui, M.; Sauvet, F.; Drogou, C.; Van Beers, P.; Langrume, C.; Guillard, M.; Gourby, B.; Bourrilhon, C.; Florence, G.; Gomez-Merino, D. Effect of one night of sleep loss on changes in tumor necrosis factor alpha (TNF-α) levels in healthy men. Cytokine 2011, 56, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Grandner, M.A.; Buxton, O.M.; Jackson, N.; Sands-Lincoln, M.; Pandey, A.; Jean-Louis, G. Extreme Sleep Durations and Increased C-Reactive Protein: Effects of Sex and Ethnoracial Group. Sleep 2013, 36, 769–779. [Google Scholar] [CrossRef] [Green Version]
- Rohleder, N.; Aringer, M.; Boentert, M. Role of interleukin-6 in stress, sleep, and fatigue. Ann. N. Y. Acad. Sci. 2012, 1261, 88–96. [Google Scholar] [CrossRef]
- Irwin, M.R.; Wang, M.; Ribeiro, D.; Cho, H.J.; Olmstead, R.; Breen, E.C.; Martinez-Maza, O.; Cole, S. Sleep Loss Activates Cellular Inflammatory Signaling. Biol. Psychiatry 2008, 64, 538–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donath, M.Y.; Shoelson, S.E. Type 2 diabetes as an inflammatory disease. Nat. Rev. Immunol. 2011, 11, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Ruparelia, N.; Chai, J.T.; Fisher, E.A.; Choudhury, R.P. Inflammatory processes in cardiovascular disease: A route to targeted therapies. Nat. Rev. Cardiol. 2017, 14, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.J.; Moalem-Taylor, G. The neuro-immune balance in neuropathic pain: Involvement of inflammatory immune cells, immune-like glial cells and cytokines. J. Neuroimmunol. 2010, 229, 26–50. [Google Scholar] [CrossRef] [PubMed]
- Elinav, E.; Nowarski, R.; Thaiss, C.A.; Hu, B.; Jin, C.; Flavell, R.A. Inflammation-induced cancer: Crosstalk between tumours, immune cells and microorganisms. Nat. Rev. Cancer 2013, 13, 759–771. [Google Scholar] [CrossRef] [PubMed]
- Amor, S.; Peferoen, L.A.N.; Vogel, D.Y.S.; Breur, M.; Van Der Valk, P.; Baker, D.; Van Noort, J.M. Inflammation in neurodegenerative diseases—An update. Immunology 2014, 142, 151–166. [Google Scholar] [CrossRef] [PubMed]
- Kamath, J.; Prpich, G.; Jillani, S. Sleep Disturbances in Patients with Medical Conditions. Psychiatr. Clin. N. Am. 2015, 38, 825–841. [Google Scholar] [CrossRef]
- Bauer, J.; Hohagen, F.; Ebert, T.; Timmer, J.; Ganter, U.; Krieger, S.; Lis, S.; Postler, E.; Voderholzer, U.; Berger, M. Interleukin-6 serum levels in healthy persons correspond to the sleep-wake cycle. Clin Investig. 1994, 72, 315. [Google Scholar] [CrossRef] [PubMed]
- Krueger, J.M.; Rector, D.M.; Roy, S.; Van Dongen, H.P.A.; Belenky, G.; Panksepp, J. Sleep as a fundamental property of neuronal assemblies. Nat. Rev. Neurosci. 2008, 9, 910–919. [Google Scholar] [CrossRef]
- De Almeida, C.M.O.; Malheiro, A. Sleep, immunity and shift workers: A review. Sleep Sci. 2016, 9, 164–168. [Google Scholar] [CrossRef] [Green Version]
- Lancel, M.; Mathias, S.; Faulhaber, J.; Schiffelholz, T. Effect of interleukin-1 beta on EEG power density during sleep depends on circadian phase. Am. J. Physiol. 1996, 270, R830–R837. [Google Scholar] [CrossRef] [PubMed]
- Manfridi, A.; Brambilla, D.; Bianchi, S.; Mariotti, M.; Opp, M.R.; Imeri, L. Interleukin-1beta enhances non-rapid eye movement sleep when microinjected into the dorsal raphe nucleus and inhibits serotonergic neurons in vitro. Eur. J. Neurosci. 2003, 18, 1041–1049. [Google Scholar] [CrossRef]
- Opp, M.R. Cytokines and sleep. Sleep Med. Rev. 2005, 9, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Byrne, M.L.; O’Brien-Simpson, N.M.; Reynolds, E.C.; Walsh, K.A.; Laughton, K.; Waloszek, J.M.; Woods, M.J.; Trinder, J.; Allen, N.B. Acute phase protein and cytokine levels in serum and saliva: A comparison of detectable levels and correlations in a depressed and healthy adolescent sample. Brain Behav. Immun. 2013, 34, 164–175. [Google Scholar] [CrossRef] [PubMed]
- La Fratta, I.; Tatangelo, R.; Campagna, G.; Rizzuto, A.; Franceschelli, S.; Ferrone, A.; Patruno, A.; Speranza, L.; De Lutiis, M.A.; Felaco, M.; et al. The plasmatic and salivary levels of IL-1β, IL-18 and IL-6 are associated to emotional difference during stress in young male. Sci. Rep. 2018, 8, 3031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vining, R.F.; McGinley, R.A.; Maksvytis, J.J.; Ho, K.Y. Salivary Cortisol: A Better Measure of Adrenal Cortical Function than Serum Cortisol. Ann. Clin. Biochem. Int. J. Lab. Med. 1983, 20, 329–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Wallace, L.; Theou, O.; Rockwood, K.; Andrew, M.K. Relationship between frailty and Alzheimer’s disease biomarkers: A scoping review. Alzheimer’s Dement. 2018, 10, 394–401. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Akpinar, M.E.; Yigit, O.; Altundag, A.; Demirel, G.Y.; Kocak, I. Salivary and serum myeloperoxidase in obstructive sleep apnea. J. Otolaryngol. Head Neck Surg. 2012, 41, 22762704. [Google Scholar]
- Nizam, N.; Basoglu, O.K.; Tasbakan, M.S.; Nalbantsoy, A.; Buduneli, N. Salivary Cytokines and the Association between Obstructive Sleep Apnea Syndrome and Periodontal Disease. J. Periodontol. 2014, 85, e251–e258. [Google Scholar] [CrossRef] [PubMed]
- Thimgan, M.S.; Toedebusch, C.; McLeland, J.; Duntley, S.P.; Shaw, P.J. Excessive Daytime Sleepiness Is Associated with Changes in Salivary Inflammatory Genes Transcripts. Mediat. Inflamm. 2015, 2015, 539627. [Google Scholar] [CrossRef] [Green Version]
- Yennurajalingam, S.; Kang, D.-H.; Hwu, W.-J.; Padhye, N.S.; Masino, C.; Dibaj, S.S.; Liu, D.D.; Williams, J.L.; Lu, Z.; Bruera, E. Cranial Electrotherapy Stimulation for the Management of Depression, Anxiety, Sleep Disturbance, and Pain in Patients with Advanced Cancer: A Preliminary Study. J. Pain Symptom Manag. 2018, 55, 198–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boström, A.; Scheele, D.; Stoffel-Wagner, B.; Hönig, F.; Chaudhry, S.R.; Muhammad, S.; Hurlemann, R.; Krauss, J.K.; Lendvai, I.S.; Chakravarthy, K.; et al. Saliva molecular inflammatory profiling in female migraine patients responsive to adjunctive cervical non-invasive vagus nerve stimulation: The MOXY study. J. Transl. Med. 2019, 17, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, A.R.; Da Silva, N.C.; Pinato, L. Analyses of melatonin, cytokines, and sleep in chronic renal failure. Sleep Breath. 2016, 20, 339–344. [Google Scholar] [CrossRef] [PubMed]
- El-Sheikh, M.; Buckhalt, J.A.; Granger, D.A.; Erath, S.A.; Acebo, C. The association between children’s sleep disruption and salivary interleukin-6. J. Sleep Res. 2007, 16, 188–197. [Google Scholar] [CrossRef]
- LaVoy, E.C.; Palmer, C.A.; So, C.; Alfano, C.A. Bidirectional relationships between sleep and biomarkers of stress and immunity in youth. Int. J. Psychophysiol. 2020, 158, 331–339. [Google Scholar] [CrossRef]
- Reinhardt, É.L.; Fernandes, P.A.C.M.; Markus, R.P.; Fischer, F.M. Night work effects on salivary cytokines TNF, IL-1β and IL-6. Chronobiol. Int. 2019, 36, 11–26. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, R.; Shen, Y.; Qiao, S.; Hui, Z.; Chen, J. Shimian granules improve sleep, mood and performance of shift nurses in association changes in melatonin and cytokine biomarkers: A randomized, double-blind, placebo-controlled pilot study. Chronobiol. Int. 2020, 37, 592–605. [Google Scholar] [CrossRef] [PubMed]
- Faraut, B.; Nakib, S.; Drogou, C.; Elbaz, M.; Sauvet, F.; De Bandt, J.-P.; Léger, D. Napping Reverses the Salivary Interleukin-6 and Urinary Norepinephrine Changes Induced by Sleep Restriction. J. Clin. Endocrinol. Metab. 2015, 100, E416–E426. [Google Scholar] [CrossRef] [Green Version]
- Reinhardt, É.L.; Fernandes, P.A.C.M.; Markus, R.P.; Fischer, F.M. Daily rhythm of salivary IL-1ß, cortisol and melatonin in day and night workers. Work 2012, 41, 5788–5790. [Google Scholar] [CrossRef] [Green Version]
- Reinhardt, É.L.; Fernandes, P.A.C.M.; Markus, R.P.; Fischer, F.M. Short sleep duration increases salivary IL-6 production. Chronobiol. Int. 2016, 33, 780–782. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez, V.; Silva, J.; Cauli, O. A survey on sleep assessment methods. PeerJ 2018, 6, e4849. [Google Scholar] [CrossRef] [Green Version]
- Robertson, B.; Marshall, B.; Carno, M.A. Polysomnography for the Sleep Technologist; Elsevier: Amsterdam, The Netherlands, 2014; ISBN 9780323100199. [Google Scholar]
- Pandi-Perumal, S.R.; Spence, D.W.; BaHammam, A.S. Polysomnography: An Overview. In Primary Care Sleep Medicine; Springer: New York, NY, USA, 2014; pp. 29–42. [Google Scholar]
- Armon, C.; Johnson, K.G.; Roy, A.; Nowack, W.J. Polysomnography. Medscape. 23 February 2016. Available online: http://www.medscape.com/ (accessed on 2 December 2020).
- Silva, G.E.; Vana, K.D.; Goodwin, J.L.; Sherrill, D.L.; Quan, S.F. Identification of Patients with Sleep Disordered Breathing: Comparing the Four-Variable Screening Tool, STOP, STOP-Bang, and Epworth Sleepiness Scales. J. Clin. Sleep Med. 2011, 7, 467–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Sayed, I.H. Comparison of four sleep questionnaires for screening obstructive sleep apnea. Egypt. J. Chest Dis. Tuberc. 2012, 61, 433–441. [Google Scholar] [CrossRef] [Green Version]
- Firat, H.; Yuceege, M.; Demir, A.; Ardic, S. Comparison of four established questionnaires to identify highway bus drivers at risk for obstructive sleep apnea in Turkey. Sleep Biol. Rhythm. 2012, 10, 231–236. [Google Scholar] [CrossRef]
- Luo, J.; Huang, R.; Zhong, X.; Xiao, Y.; Zhou, J. STOP-Bang questionnaire is superior to Epworth sleepiness scales, Berlin questionnaire, and STOP questionnaire in screening obstructive sleep apnea hypopnea syndrome patients. Chin. Med. J. 2014, 127, 25189946. [Google Scholar]
- Pataka, A.; Daskalopoulou, E.; Kalamaras, G.; Passa, K.F.; Argyropoulou, P. Evaluation of five different questionnaires for assessing sleep apnea syndrome in a sleep clinic. Sleep Med. 2014, 15, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Chai-Coetzer, C.L.; Antic, N.A.; Rowland, L.S.; Catcheside, P.G.; Esterman, A.; Reed, R.L.; Williams, H.; Dunn, S.V.; McEvoy, R.D. A simplified model of screening questionnaire and home monitoring for obstructive sleep apnoea in primary care. Thorax 2011, 66, 213–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Morin, C.M. Insomnia: Psychological Assessment and Management; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Owens, J.A.; Spirito, A.; McGuinn, M. The Children’s Sleep Habits Questionnaire (CSHQ): Psychometric properties of a survey instrument for school-aged children. Sleep 2000, 23, 1043–1051. [Google Scholar] [CrossRef]
- Wolfson, A.R.; Carskadon, M.A.; Acebo, C.; Seifer, R.; Fallone, G.; Labyak, S.E.; Martin, J.L. Evidence for the Validity of a Sleep Habits Survey for Adolescents. Sleep 2003, 26, 213–216. [Google Scholar] [CrossRef]
- Cole, R.J.; Kripke, D.F.; Gruen, W.; Mullaney, D.J.; Gillin, J.C. Technical note: Automatic sleep/wake identification from wrist actigraphy. Sleep 1992, 15, 461–469. [Google Scholar] [CrossRef]
- Sadeh, A.; Sharkey, K.M.; Carskadon, M.A. Activity-Based Sleep-Wake Identification: An Empirical Test of Methodological Issues. Sleep 1994, 17, 201–207. [Google Scholar] [CrossRef] [Green Version]
- Rico-Rosillo, M.G.; Vega-Robledo, G.B. Sueño y sistema immune [Sleep and immune system]. Rev. Alerg. Mex. 2018, 65, 160–170, In Spanish. [Google Scholar] [CrossRef] [Green Version]
- Papanicolaou, D.A.; Vgontzas, A.N. Interleukin-6: The Endocrine Cytokine. J. Clin. Endocrinol. Metab. 2000, 85, 1331–1333. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Papanicolaou, D.A.; Bixler, E.O.; Kales, A.; Tyson, K.; Chrousos, G.P. Elevation of plasma cytokines in disorders of excessive daytime sleepiness: Role of sleep disturbance and obesity. J. Clin. Endocrinol. Metab. 1997, 82, 1313–1316. [Google Scholar] [CrossRef] [PubMed]
- Rose-John, S. Interleukin-6 Family Cytokines. Cold Spring Harb. Perspect. Biol. 2018, 10, a028415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, T.G.; Trejo, M.E.P.; McClelland, R.; Bradley, R.; Blaha, M.J.; Zeb, I.; Corey, K.E.; Budoff, M.J.; Chung, R.T. Circulating Interleukin-6 is a biomarker for coronary atherosclerosis in nonalcoholic fatty liver disease: Results from the multi-ethnic study of atherosclerosis. Int. J. Cardiol. 2018, 259, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Huang, J.; Zhong, H.; Shen, N.; Faggioni, R.; Fung, M.; Yao, Y. Targeting interleukin-6 in inflammatory autoimmune diseases and cancers. Pharmacol. Ther. 2014, 141, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Jewett, K.A.; Krueger, J.M. Humoral Sleep Regulation; Interleukin-1 and Tumor Necrosis Factor. Vitam. Horm. 2012, 89, 241–257. [Google Scholar] [CrossRef] [Green Version]
- Van Leeuwen, W.M.A.; Lehto, M.; Karisola, P.; Lindholm, H.; Luukkonen, R.; Sallinen, M.; Härmä, M.; Porkka-Heiskanen, T.; Alenius, H. Sleep Restriction Increases the Risk of Developing Cardiovascular Diseases by Augmenting Proinflammatory Responses through IL-17 and CRP. PLoS ONE 2009, 4, e4589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frey, D.J.; Fleshner, M.; Wright, K.P., Jr. The effects of 40 hours of total sleep deprivation on inflammatory markers in healthy young adults. Brain Behav. Immun. 2007, 21, 1050–1057. [Google Scholar] [CrossRef]
- Prather, A.A.; Marsland, A.L.; Hall, M.; Neumann, S.A.; Muldoon, M.F.; Manuck, S.B. Normative variation in self-reported sleep quality and sleep debt is associated with stimulated pro-inflammatory cytokine production. Biol. Psychol. 2009, 82, 12–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markus, R.P.; Fernandes, P.A.; Kinker, G.S.; da Silveira Cruz-Machado, S.; Marçola, M. Immune-pineal axis-acute inflammatory responses coordinate melatonin synthesis by pinealocytes and phagocytes. Br. J. Pharmacol. 2018, 175, 3239–3250. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.-C.; Chiou, C.-H.; Liu, S.-C.; Hu, S.-L.; Su, C.-M.; Tsai, C.-H.; Tang, C.-H. Melatonin attenuates TNF-α and IL-1β expression in synovial fibroblasts and diminishes cartilage degradation: Implications for the treatment of rheumatoid arthritis. J. Pineal Res. 2019, 66, e12560. [Google Scholar] [CrossRef]
- da Silveira Cruz-Machado, S.; Campos, L.M.G.; Fadini, C.C.; Anderson, G.; Markus, R.P.; Pinato, L. Disrupted nocturnal melatonin in autism: Association with tumor necrosis factor and sleep disturbances. J. Pineal Res. 2021, e12715. [Google Scholar] [CrossRef]
- Castanon-Cervantes, O.; Wu, M.; Ehlen, J.C.; Paul, K.; Gamble, K.L.; Johnson, R.L.; Besing, R.C.; Menaker, M.; Gewirtz, A.T.; Davidson, A.J. Dysregulation of Inflammatory Responses by Chronic Circadian Disruption. J. Immunol. 2010, 185, 5796–5805. [Google Scholar] [CrossRef] [Green Version]
- Slavish, D.C.; Graham-Engeland, J.E.; Smyth, J.M.; Engeland, C.G. Salivary markers of inflammation in response to acute stress. Brain Behav. Immun. 2015, 44, 253–269. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Reference | N/Sex | Mean Age | Sample Characteristics | Instrument(s) Used to Assess Sleep Quality | Measurement | Relationship Between Salivary Inflammatory Markers and Sleep | Study Design |
|---|---|---|---|---|---|---|---|
| Reinhardt et al. 2019 [48] | 38 males | Day workers 32.1 years and night workers 32.5 years | Healthy controls (workers with no shifts but one group has a permanent day shift, from 7:00 to 17:00, and the other group has a permanent night shift, from 21:00 to 6:00). | Actigraphy | Sleep disturbance. Circadian disturbance | The levels of TNFα and IL-1β were similar for day and night shift workers, with higher daily production upon awakening, for day workers, for evening workers and for night workers. Day and night workers produced similar amounts of IL-6. | Observational Prospective |
| Zhang et al., 2020 [49] | 38 females | 29.0 years | Healthy controls (nurses with shifts) | Insomnia Severity Index (ISI) Pittsburgh Sleep Quality Index (PSQI) | Subjective insomnia severity Subjective quality of sleep | The levels of TNFα, IL-1β and IL-6 in saliva were lower with the Shimian granules (traditional Chinese herbal treatment for sleep disorders) treatment. TNFα and IL-6 levels were directly correlated with insomnia severity. | Experimental Clinical trial (placebo-controlled) |
| Faraut et al., 2015 [50] | 11 males | 27.0 years | Healthy controls (non-smokers) | Polysomnography | Monitor sleep-wake cycle after sleep restriction | IL-6 levels were lower at 10:00 a.m. and 7:00 p.m. on days with restricted nighttime sleep. The decrease in IL-6 normalized after a daytime nap (<30 min) | Experimental |
| Reinhardt et. al. 2012 [51] | 5 males | Not specified | Healthy controls (workers with shifts: 3 night (21:00–6:00) and 2 day (7:00–17:00)) | Actigraphy | Sleep deprivation caused by shift work | IL-1ß levels were higher upon awakening than at bedtime for all workers regardless of work shift, bedtime, sleep efficiency, or total sleep duration. | Observational Prospective |
| Reinhardt et al., 2016 [52] | 21 males | 32.1 years | Healthy controls (workers with no shifts) | Actigraphy | Sleep duration | Workers with a duration of sleep <6 h had higher levels of salivary IL-6 at bedtime IL-6 and at 14:00 h compared to workers with a longer duration of sleep (≥6 h). Workers with longer sleep duration presented a lower production of salivary IL-6 around 14:00 h, during work shift, and a higher production at awakening and at bedtime | Observational |
| Nizam et al., 2014 [41] | 52 (32 males;20 females) | 46.6 years | Healthy controls Individuals with sleep apnea (OSA) | Polysomnography Apnea-hypopnea index | Presence and severity of OSA | Salivary concentrations of IL-6 and IL-33 were statistically higher in OSA group compared to the control group. The concentrations of IL-1β and IL-21 were similar in all groups. | Observational Prospective |
| Yennurajalingam et al., 2017 [43] | 52 (20 males; 32 females) | 59 years (median) | Patients with advanced cancer | Pittsburgh Sleep Quality Index (PSQI) | Subjective quality of sleep | Improvement in the total PSQI sleep score by 2 points, and a significant improvement in the daytime PSQI dysfunction after cranial electrotherapy stimulation (CES). A trend towards improvement in IL-6 (but not in IL-1beta) after CES. | Experimental One group open label pre- and post-intervention |
| Boström et al., 2019 [44] | 24 females | 47.6 years | Healthy controls and Individuals with migraine | Pittsburgh Sleep Quality Index (PSQI) | Subjective quality of sleep | Migraine-related abnormalities in sleep architecture improved after ten weeks of vagus nerve stimulation (nVNS) treatment. IL-1β levels in saliva increased after nVNS therapy, producing values 2.5 times higher than those measured in healthy controls. | Observational Prospective Case-control study |
| Pinto et al. 2015 [45] | 39 (sex not specified) | 54.9 years | Healthy controls and patients with chronic renal failure (CRF). | Pittsburgh Sleep Quality Index (PSQI) | Subjective quality of sleep | The CRF group obtained a higher score than the control group on the global PSQI, i.e., lower sleep quality and a higher prevalence of sleep disorders. The CRF group also presented higher TNFα and IL-6 contents than the control group. | Experimental Clinical cross-sectional |
| El-Sheikh et al. 2007 [46] | 64 children (28 males; 36 females) | 8.8 years | Healthy controls | Actigraphy School Sleep habits Survey using Sleepiness and Morning/Eveningness (to children) Children’s Sleep Habits Questionnaire (CSHQ) (to Parents) | Quality and quantity of sleep, sleep onset time, daytime sleepiness | Children with higher salivary IL-6 levels reported increased Eveningness predispositions and their parents reported higher levels of sleep disordered breathing. | Observational Cross-sectional and Prospective |
| Thimgan et al., 2015 [42] | 40 (22 males; 18 females) | Control group: 40.8 years Sleep apnea (OSA) group:49.0 years | Healthy controls and individuals with sleep apnea | Polysomnography Apnea-hypopnea index Epworth Sleepiness Scale | Severity of OSA | The transcripts of the enzyme prostaglandin-endoperoxide synthase 2 (PTGS2) in saliva was increased in patients with sleep apnea. | Observational Prospective |
| Akpinar et al., 2012 [40] | 56 (40 males; 16 females) | Control group: 44.7 years; OSA group: 43.8 years | Healthy controls and individuals with obstructive sleep apnea (OSA) | PolysomnographyApnea-hypopnea index (AHI) | Severity of OSA | Salivary myeloperoxidase (MPO) levels were significantly higher in the OSA group compared to controls and the increase in MPO in saliva correlated with the severity of OSA according to the AHI and oxygen desaturation index. | Observational Prospective |
| LaVoy et al. 2020 [47] | 55 children (26 males; 29 females) | 12.2 years | Healthy controls and children with different type of psychiatric disorders | Actigraphy 10-item sleep-wake problems subscale of the School Sleep Habits Survey (SSHS). | Total sleep time, sleep efficiency, number of waking episodes, number of minutes spent awake during the night, sleep onset latency | Salivary Il-1β was positively associated with prior night total sleep time and negatively associated with sleep onset latency, and IL-6 was associated with greater sleep efficiency. Higher IL-1β predicted a longer sleep onset latency the following night. | Observational Prospective |
| Article\Items | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| El-Sheikh et al., 2007 [46] | Y | Y | Y | Y | U | Y | N | Y | NA | U | U |
| Reinhardt et al., 2012 [51] | Y | U | Y | Y | U | Y | Y | U | U | U | U |
| Akpinar et al., 2012 [40] | Y | Y | Y | Y | U | N | N | Y | NA | U | U |
| Nizam et al., 2014 [41] | Y | Y | Y | Y | U | N | N | N | U | U | U |
| Pinto et al., 2015 [45] | Y | Y | U | Y | U | Y | Y | Y | U | U | U |
| Faraut et al., 2015 [50] | Y | Y | Y | Y | Y | N | N | Y | U | U | U |
| Thimgan et al., 2015 [42] | Y | N | U | Y | N | Y | N | Y | NA | U | U |
| Reinhardt et al., 2016 [52] | Y | N | U | U | N | Y | N | N | U | U | U |
| Yennurajalingam et al., 2017 [43] | Y | Y | Y | Y | N | Y | Y | U | U | U | Y |
| Reinhardt et al., 2019 [48] | Y | Y | Y | Y | Y | Y | Y | U | U | U | U |
| Boström et al., 2019 [44] | Y | Y | Y | Y | N | N | Y | U | U | U | U |
| Zhang et al., 2020 [49] | Y | Y | Y | Y | Y | N | Y | U | U | U | U |
| LaVoy et al., 2020 [47] | Y | Y | Y | Y | Y | Y | Y | U | U | U | U |
| Reference | Strengths | Limitations |
|---|---|---|
| El-Sheik et al., 2007 [46] | Homogeneous sample: healthy children (age = 8–9, similar gender proportion) Sample size: N = 64 Sample collected at two different times (3 p.m. and 5 p.m.) Combines objective and subjective sleep assessment methods: one-week actigraphy + School Sleep habits Survey (children) and Children’s Sleep Habits Questionnaire (CSHQ) (parents) | Only IL-6 was studied |
| Reinhardt et. al., 2012 [51] | Homogeneous sample: healthy men Daytime workers and overnight workers were compared. Sample collected at two different times: wake time and midnight. Objective and subjective methods combined: Diaries + actigraphy Includes the study of melatonin in saliva | Small sample: N = 5 No analysis with the secondary variables assessed (depression, anxiety) |
| Akpinar et al., 2012 [40] | Narrow age range (control: 44.7 ± 13.75; experimental: 43.79 ± 12.72) Sample size N = 56 Healthy people and people with OSA are studied Objective and subjective methods combined: Polysomnography and Epworth Sleepiness Scale (ESS) Mieloperoxidase (MPO) was measured on blood and salivaIMC was measured as a secondary variable | Only MPO and PCR levels were assessed (other inflammatory markers such cytokines were not assessed). |
| Nizam et al., 2014 [41] | Polysomnography is applied to all participants (N = 52) Healthy people and people with OSA are studied Several cytokines were measured: IL-6, IL-33, IL-1β, IL-21, and pentraxin-3 (PTX3) | Unbalanced sample: 32 men and 20 women Wide age range: 21–64 years Only one sample collected |
| Faraut et al., 2015 [50] | Homogeneous sample: healthy men (age = 25–32) Polysomnography Sample collected at several time points (every two hours) | Small sample: N = 11 Only IL-6 was assessed |
| Pinto et al., 2016 [45] | Sample collected at several times (every four hours) Includes the study of melatonin in saliva | Heterogeneous sample: healthy people and people with chronic renal failure. Wide age range: 29–79 years (N = 39) Only TNFα and IL-6 were assessed Samples were collected along a period of only 24 h. Cytokines were assessed only in blood (not in saliva) Sleep assessed with only one questionary: Sleep Quality e Index Pittsburgh (PSQI) |
| Thimgam et al., 2015 [42] | Objective and subjective methods combined: Polysomnography and Epworth Sleepiness Scale (ESS) A polysomnogram was produced for all patients (N = 40) IMC was measured as a secondary variable | Heterogeneous sample: healthy people (5 men/3 women), OSA patients (11 men/3 women), and patients with suspected OSA (6 men/12 women) Inflammatory transcriptions were assessed, but not cytokines |
| Reinhardt et al., 2016 [38] | Homogeneous sample: healthy men workers with day work shift. Narrow age range (32.14 ± 7.61) Objective and subjective methods combined: Actigraphy and diaries Sample collected at three different times (wake, 2pm and bedtime) | Small sample: N = 21 Only IL-6 was studied |
| Yennurajalingam et al., 2017 [43] | Sample (N = 52) collected at two different times (wake and bedtime) IL-1β and IL-6 were assessed Secondary variables were measured: anxiety, depression with HADS (Edmonton Symptom Assessment Scale), pain with BPI (Brief Pain Inventory) and drugs used. | Heterogeneous sample: advanced cancer patients with at least one symptom of depression, anxiety, sleep disorders, and pain. Unbalanced sample: 32 men and 20 women Sleep assessed with only one questionary: Pittsburgh Sleep Quality Index (PSQI) Sample collected only once a week |
| Reinhardt et al. 2019 [48] | Homogeneous sample: healthy men workers. Narrow age range: day workers 32.14 ± 7.61 years old and night workers 32.59 ± 5.62 years old Different work shifts were analyzed Actigraphy used for 10 days (24 h/day) Sample collected at two different times TNFα, interleukin-1β (IL-1β), and IL-6 were studied Melatonin levels in saliva were assessed. | Sample size: N = 38 Different number of workers in each group (day: 21; night: 17) No secondary variable was studied |
| Boström et al., 2019 [44] | All participants were women. All samples collected at the same time Secondary variables were studied: functional capacity with MIDAS (Migraine Disability Assessment), depressive symptoms with BDI (Beck Depression Inventory) and quality of life (EuroQuol EQ-5D-5L) | Heterogeneous simple (N = 24): healthy women and women with migraine Wide age range: 34–65 years Sleep assessed with only one questionary: Pittsburgh Sleep Quality Index (PSQI) Samples were collected only twice along the whole research (at the beginning and at the end, after 10 weeks with nVNS). Only IL-1β was studied |
| Zhang et al., 2020 [49] | Homogeneous sample: nurse women that work in rotative work shifts. Daily samples collected Different cytokines, e.g., IL-6, IL-1β, and TNFα were studied. Melatonin levels in saliva were assessed. Secondary variables related to sleep were studied: insomnia, anxiety, depression (with HADS) and alert level (with PVT, psychomotor vigilance task) | Sample size: N = 32 Different sample size for the control (13) and experimental groups (19) Sleep assessed with only subjective methods: Pittsburgh Sleep Quality Index (PSQI) and Insomnia Severity Index (ISI) Samples were collected only once a week |
| LaVoy et al., 2020 [47] | Similar gender proportion (53% women) Narrow age range: 8–16 years Objective and subjective methods combined: Actigraphy, sleep diaries and the School Sleep Habits Survey (SSHS) Daily simple collection (at wake time) All samples were analyzed twice IL-6 and IL-1β were studied Secondary variables were studied: the z-score of body mass index (zBMI), collection time, and season of data collection. | Heterogeneous sample: healthy people and people with at least a diagnostic of attention deficit hyperactivity disorder (n = 1), generalized anxiety disorder (n = 5), major depressive disorder (n = 2), social anxiety disorder (n = 4), specific phobia (n = 3), pervasive developmental disorder (n = 1), depressive disorder not otherwise specified (n = 1), and disruptive mood dysregulation disorder (n = 1). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibáñez-del Valle, V.; Navarro-Martínez, R.; Ballestar-Tarín, M.L.; Cauli, O. Salivary Inflammatory Molecules as Biomarkers of Sleep Alterations: A Scoping Review. Diagnostics 2021, 11, 278. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020278
Ibáñez-del Valle V, Navarro-Martínez R, Ballestar-Tarín ML, Cauli O. Salivary Inflammatory Molecules as Biomarkers of Sleep Alterations: A Scoping Review. Diagnostics. 2021; 11(2):278. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020278
Chicago/Turabian StyleIbáñez-del Valle, Vanessa, Rut Navarro-Martínez, Maria Luisa Ballestar-Tarín, and Omar Cauli. 2021. "Salivary Inflammatory Molecules as Biomarkers of Sleep Alterations: A Scoping Review" Diagnostics 11, no. 2: 278. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020278