
A Multi-Center, Multi-Vendor Study to Evaluate the Generalizability of a Radiomics Model for Classifying Prostate cancer: High Grade vs. Low Grade

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ground Truth Construction: Pathology-MRI Correlation
2.2. Image Pre-Processing.
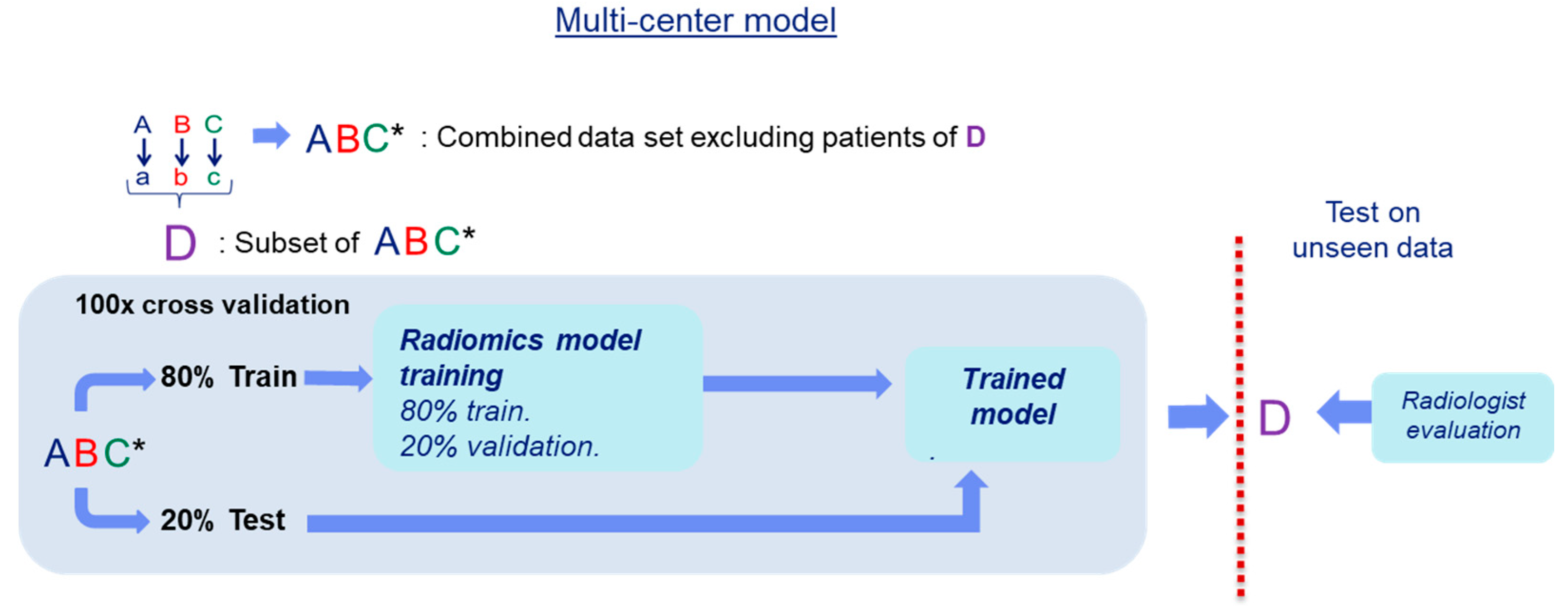
2.3. Radiomics Generalizability Evaluation
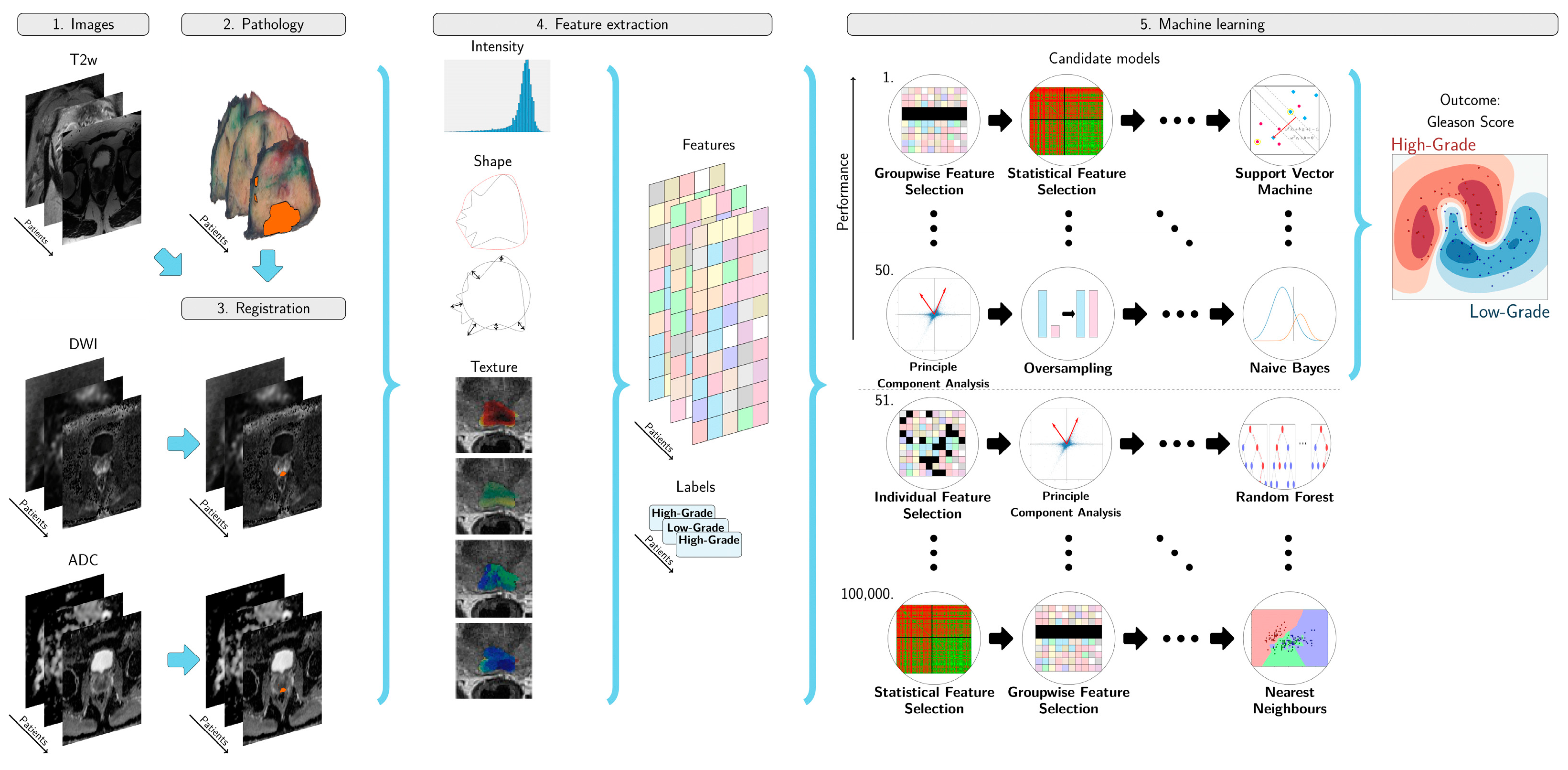
2.4. Radiomics Model Development
2.5. Radiomics Classifier Evaluation
2.6. Comparison of Our Radiomics Model with the Clinical Assessment using PIRADS v2
3. Results
Comparison of Our Radiomics Model with the Clinical Assessment using PIRADS v2
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Center. | Vendor | Model | Magnetic Field (Tesla). | #Patients | Sequence | Voxel Size (mm) | B-Values | Endorectal Coil |
|---|---|---|---|---|---|---|---|---|
| A. | GE Medical Systems. | MR750. | 3T. | 21. | T2. | 0.37 × 0.37 × 3.00… | No… | |
| DWI | 1.09 × 1.09 × 4.00 | 50/400/800 | ||||||
| GE Medical Systems | MR450 | 1.5T | 3 | T2 | 0.47 × 0.47 × 3.00 | No | ||
| DWI | 1.25 × 1.25 × 4.00 | 100/500/1000 | ||||||
| SIEMENS | Avanto | 1.5T | 5 | T2 | 0.70 × 0.70 × 3.00 | No | ||
| DWI | 1.85 × 1.85 × 6.00 | 50/400/600 | ||||||
| B | Philips Healthcare | Achieva | 3T | 38 | T2 | 0.27 × 0.27 × 3.00 | Yes | |
| DWI | 1.03 × 1.03 × 3.00 | 150/300/450/600/750 | ||||||
| C | SIEMENS | TrioTim | 3T | 17 | T2 | 0.63 × 0.63 × 3.00 | ||
| DWI | 2.00 × 2.00 × 4.00 | 50/500/800 | No | |||||
| Skyra | 3T | 23 | ||||||
| T2 | 0.60 × 0.60 × 3.00 | |||||||
| DWI | 2.00 × 2.00 × 4.00 | 50/500/800 | No |
Appendix B. Radiomics Features Extraction
Appendix C. Adaptive Workflow Optimization for Automatic Decision Model Creation
Appendix D. Appendix References
- Frangi, A.F.; Niessen, W.J.; Vincken, K.L.; Viergever, M.A. Multiscale Vessel Enhancement Filtering. In Medical Image Computing and Computer-Assisted Intervention—MICCAI’98; MICCAI 1998, Lecture Notes in Computer Science; Wells, W.M., Colchester, A., Delp, S., Eds.; Springer: Berlin/Heidelberg, Germany, 1998; Volume 1496, doi:10.1007/BFb0056195.
- Kovesi, P. Symmetry and Asymmetry from Local Phase. In Proceedings of the Roceedings of the 10th Australian Joint Conference on Artificial Intelligence: Advanced Topics in Artificial Intelligence, Perth, Australia, 1997, pp. 185–190.
- Kovesi, P. Phase Congruency Detects Corners and Edges. In Proceedings of the VIIth Digital Image Computing: Techniques and Applications, Sydney, Australia, 10−12 December 2003.
- Lemaitre, G.; Nogueira, F.; Aridas, C.K. Imbalanced-learn: A Python Toolbox to Tackle the Curse of Imbalanced Datasets in Machine Learning. J. Mach. Learn. Res. 2017, 18.
- Ojala, T.; Pietikainen, M.; Maenpaa, T. Multiresolution gray-scale and rotation invariant texture classification with local binary patterns. IEEE Trans. Pattern Anal. Mach. Intell. 2002, 24, 971–987, doi:10.1109/TPAMI.2002.1017623.
- Starmans, M.P.A. Workflow for Optimal Radiomics Classification (WORC) Documentation. Available online: https://worc.readthedocs.io (accessed on 16 February 2021); doi:10.5281/zenodo.3840534.
- Starmans, M.P.A. GISTRadiomics. Available online: https://github.com/MStarmans91/GISTRadiomics (accessed on 16 February 2021); doi:10.5281/zenodo.3839323.
- Starmans, M.P.A.; Van der Voort, S.R.; Phil, T.; Klein, S. Workflow for Optimal Radiomics Classification (WORC). Available online: https://github.com/MStarmans91/WORC (accessed on 16 February 2021); doi:10.5281/zenodo.3840534.
- Timbergen, M.J.M.; Starmans, M.P.A.; Padmos, G.A.; Grünhagen, D.J.; van Leenders, G.J.L.H.; Hanff, D.; Niessen, W.J.; Sleijfer, S.; Klein, S.; Visser, J.J. Differential diagnosis and mutation stratification of desmoid-type fibromatosis on MRI using radiomics. Eur. J. Radiol. 2020, 109266, doi:10.1016/j.ejrad.2020.109266.
- Van der Voort, S.R.; Starmans, M.P.A. Predict a Radiomics Extensive Differentiable Interchangable Classification Toolkit (P ICT). Available online: https://github.com/Svdvoort/PREDICTFastr (accessed on 16 February 2021); doi:10.5281/zenodo.3854839.
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin,, J.-C.; Pieper, S.; Aerts, H.J. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, e104–e107, doi:10.1158/0008-5472.CAN-17-0339.
- Vos, M.; Starmans, M.P.A.; Timbergen, M.J.M.; van der Voort, S.R.; Padmos, G.A.; Kessels, W.; Visser, J.J.; Niessen, W.J.; van Leenders, G.J.L.H.; Grünhagen, D.J.; Sleijfer, S.; et al.Radiomics approach to distinguish between well differentiated liposarcomas and lipomas on MRI. Br. J. Surg. 2019, 106, 1800–1809, doi:10.1002/bjs.11410.
- Zwanenburg, A.; Vallières, M.; Abdalah, M.; Aerts, H.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 191145, doi:10.1148/radiol.2020191145.
References
- Rawla, P. Epidemiology of Prostate Cancer. Rev. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Cornford, P.; De Santis, M.; Fanti, S.; Gillessen, S.; Grummet, J.; Henry, A.M.; Lam, T.B.; et al. European Association of Urology: Prostate Cancer Guidelines. Available online: https://uroweb.org/wp-content/uploads/Prostate-Cancer-2018-pocket.pdf (accessed on 15 June 2019).
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging—Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef] [PubMed]
- Min, X.; Li, M.; Dong, D.; Feng, Z.; Zhang, P.; Ke, Z.; You, H.; Han, F.; Ma, H.; Tian, J.; et al. Multi-parametric MRI-based radiomics signature for discriminating between clinically significant and insignificant prostate cancer: Cross-validation of a machine learning method. Eur. J. Radiol. 2019, 115, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Hoang Dinh, A.; Souchon, R.; Melodelima, C.; Bratan, F.; Mège-Lechevallier, F.; Colombel, M.; Rouvière, O. Characterization of prostate cancer using T2 mapping at 3 T: A multi-scanner study. Diagn. Interv. Imaging 2015, 96, 365–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaddad, A.; Kucharczyk, M.J.; Niazi, T. Multimodal radiomic features for the predicting gleason score of prostate cancer. Cancers 2018, 10, 249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo, T.J.M.; Starmans, M.P.A.; Niessen, W.J.; Schoots, I.; Klein, S.; Veenland, J.F. Classification Of Prostate Cancer: High Grade Versus Low Grade Using A Radiomics Approach. In Proceedings of the 2019 IEEE(New York, USA) 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019; pp. 1319–1322. [Google Scholar]
- Castillo, T.J.M.; Arif, M.; Niessen, W.J.; Schoots, I.G.; Veenland, J.F. Automated Classification of Significant Prostate Cancer on MRI: A Systematic Review on the Performance of Machine Learning Applications. Cancers 2020, 12, 1606. [Google Scholar] [CrossRef] [PubMed]
- Stanzione, A.; Gambardella, M.; Cuocolo, R.; Ponsiglione, A.; Romeo, V.; Imbriaco, M. Prostate MRI radiomics: A systematic review and radiomic quality score assessment. Eur. J. Radiol. 2020, 129, 109095. [Google Scholar] [CrossRef] [PubMed]
- Transin, S.; Souchon, R.; Gonindard-Melodelima, C.; de Rozario, R.; Walker, P.; Funes de la Vega, M.; Loffroy, R.; Cormier, L.; Rouvière, O. Computer-aided diagnosis system for characterizing ISUP grade ≥2 prostate cancers at multiparametric MRI: A cross-vendor evaluation. Diagn. Interv. Imaging 2019, 100, 801–811. [Google Scholar] [CrossRef]
- Penzias, G.; Singanamalli, A.; Elliott, R.; Gollamudi, J.; Shih, N.; Feldman, M.; Stricker, P.D.; Delprado, W.; Tiwari, S.; Böhm, M.; et al. Identifying the morphologic basis for radiomic features in distinguishing different Gleason grades of prostate cancer on MRI: Preliminary findings. PLoS ONE 2018, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinh, A.H.; Melodelima, C.; Souchon, R.; Moldovan, P.C.; Bratan, F.; Pagnoux, G.; Mège-Lechevallier, F.; Ruffion, A.; Crouzet, S.; Colombel, M.; et al. Characterization of Prostate Cancer with Gleason Score of at Least 7 by Using Quantitative Multiparametric MR Imaging: Validation of a Computer-aided Diagnosis System in Patients Referred for Prostate Biopsy. Radiology 2018, 287, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Orlhac, F.; Boughdad, S.; Philippe, C.; Stalla-Bourdillon, H.; Nioche, C.; Champion, L.; Soussan, M.; Frouin, F.; Frouin, V.; Buvat, I. A postreconstruction harmonization method for multicenter radiomic studies in PET. J. Nucl. Med. 2018, 59, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, T.A.; Eruyar, A.T.; Cebeci, O.O.; Memik, O.; Ozcan, L.; Kuskonmaz, I. Interobserver variability in Gleason histological grading of prostate cancer. Scand. J. Urol. 2016, 50, 420–424. [Google Scholar] [CrossRef]
- Nilsson, B.; Egevad, L.; Sundelin, B.; Glaessgen, A.; Hamberg, H.; Pihl, C.-G. Interobserver reproducibility of modified Gleason score in radical prostatectomy specimens. Virchows Arch. 2004, 1, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, S.E.; Chirra, P.V.; Yim, M.C.; Rofsky, N.M.; Purysko, A.S.; Rosen, M.A.; Bloch, B.N.; Madabhushi, A. Comparing radiomic classifiers and classifier ensembles for detection of peripheral zone prostate tumors on T2-weighted MRI: A multi-site study. BMC Med. Imaging 2019, 19, 22. [Google Scholar] [CrossRef]
- Artan, Y.; Oto, A.; Yetik, I.S. Cross-Device Automated Prostate Cancer Localization With Multiparametric MRI. IEEE Trans. Image Process. 2013, 22, 5385–5394. [Google Scholar] [CrossRef]
- Peng, Y.; Jiang, Y.; Antic, T.; Giger, M.L.; Eggener, S.E.; Oto, A. Validation of Quantitative Analysis of Multiparametric Prostate MR Images for Prostate Cancer Detection and Aggressiveness Assessment: A Cross-Imager Study. Radiology 2014, 271, 461–471. [Google Scholar] [CrossRef] [PubMed]
- MeVisLab: MeVisLab. Available online: https://www.mevislab.de/ (accessed on 13 August 2020).
- Starmans MPA GitHub—MStarmans91/WORC: Workflow for Optimal Radiomics Classification. Available online: https://github.com/MStarmans91/WORC (accessed on 17 October 2019).
- Fortin, J.P.; Parker, D.; Tunç, B.; Watanabe, T.; Elliott, M.A.; Ruparel, K.; Roalf, D.R.; Satterthwaite, T.D.; Gur, R.C.; Gur, R.E.; et al. Harmonization of multi-site diffusion tensor imaging data. Neuroimage 2017, 161, 149–170. [Google Scholar] [CrossRef] [PubMed]
- Josemanuel097/PCa_classification_generalizability. Available online: https://github.com/josemanuel097/PCa_classification_generalizability (accessed on 11 February 2021).
- Nadeau, C.; Bengio, Y. Inference for the Generalization Error. Mach Learn 2003, 52, 239–281. [Google Scholar] [CrossRef] [Green Version]
- Macskassy, S.A.; Provost, F.; Rosset, S. ROC Confidence Bands: An Empirical Evaluation. In Proceedings of the 22nd International Conference on Machine Learning, Bonn, Germany, 7–11 August 2005; Association for Computing Machinery: New York, NY, USA, 2005; pp. 537–544. [Google Scholar]
- Buch, K.; Kuno, H.; Qureshi, M.M.; Li, B.; Sakai, O. Quantitative variations in texture analysis features dependent on MRI scanning parameters: A phantom model. J. Appl. Clin. Med. Phys. 2018, 19, 253–264. [Google Scholar] [CrossRef] [Green Version]
- Schwier, M.; van Griethuysen, J.; Vangel, M.G.; Pieper, S.; Peled, S.; Tempany, C.; Aerts, H.J.W.L.; Kikinis, R.; Fennessy, F.M.; Fedorov, A. Repeatability of Multiparametric Prostate MRI Radiomics Features. Sci. Rep. 2019, 9, 9441. [Google Scholar] [CrossRef] [PubMed]
- Starmans, M.P.A.; van der Voort, S.R.; Castillo Tovar, J.M.; Veenland, J.F.; Klein, S.; Niessen, W.J. Radiomics: Data mining using quantitative medical image features. In Fichtinger GBT-H of MIC and CAI; Zhou, S.K., Rueckert, D., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 429–456. [Google Scholar]
- Rundo, L.; Militello, C.; Russo, G.; Garufi, A.; Vitabile, S.; Gilardi, M.C.; Mauri, G. Automated Prostate Gland Segmentation Based on an Unsupervised Fuzzy C-Means Clustering Technique Using Multispectral T1w and T2w MR Imaging. Information 2017, 8, 49. [Google Scholar] [CrossRef] [Green Version]
- Arif, M.; Schoots, I.G.; Castillo, T.J.M.; Bangma, C.H.; Krestin, G.P.; Roobol, M.J.; Niessen, W.; Veenland, J.F. Clinically significant prostate cancer detection and segmentation in low-risk patients using a convolutional neural network on multi-parametric MRI. Eur. Radiol. 2020, 1–11. [Google Scholar] [CrossRef]
- Hoang Dinh, A.; Melodelima, C.; Souchon, R.; Lehaire, J.; Bratan, F.; Mège-Lechevallier, F.; Ruffion, A.; Crouzet, S.; Colombel, M.; Rouvière, O. Quantitative Analysis of Prostate Multiparametric MR Images for Detection of Aggressive Prostate Cancer in the Peripheral Zone: A Multiple Imager Study. Radiology 2016, 280, 117–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Prostate Cancer Molecular Medicine Data set Clinical Variables | |||
|---|---|---|---|
| Center | A | B | C |
| Number of Patients | 29 | 38 | 40 |
| Age at Diagnosis (mean ± std years) | 64 ± 7 | NA | NA |
| PSA before treatment (mean ± std ng/mL) | 12 ± 10 | 9 ± 5 | 10 ± 8 |
| Lesions Characteristics | |||
| Number of lesions | 204 | ||
| Lesion location | |||
| PZ | 33 | 59 | 45 |
| TZ | 15 | 23 | 26 |
| AFS | NA | 2 | 1 |
| Lesion volume (median and IQR mL) | 1.6 (0.2–1.8) | 1.4 (0.1–1.5) | 0.8 (0.2–1.1) |
| Radiologist PIRADS grading | R1 | R2 | |
| I | 0 | 4 | |
| II | 16 | 9 | |
| III | 21 | 36 | |
| IV | 33 | 34 | |
| V | 43 | 61 | |
| Total | 113 | 144 | |
| Model | Internal | External LC | External CH | External PC | R1 and R2 |
|---|---|---|---|---|---|
| Trained on A | A | B and C | |||
| AUC | 0.75 (0.58–0.92) | 0.43 | 0.49 | 0.55 | 0.44 |
| Sensitivity | 0.91 (0.82–1.00) | 0.80 | 0.78 | 0.81 | 0.80 |
| Specificity | 0.30 (0.03–0.55) | 0.22 | 0.27 | 0.21 | 0.06 |
| Trained on B | B | A and C | |||
| AUC | 0.69 (0.57–0.81) | 0.60 | 0.57 | 0.55 | 0.50 |
| Sensitivity | 0.64 (0.47–0.80) | 0.43 | 0.74 | 0.86 | 0.88 |
| Specificity | 0.67 (0.50–0.83) | 0.62 | 0.38 | 0.25 | 0.13 |
| Trained on C | C | A and B | |||
| AUC | 0.80 (0.68–0.92) | 0.60 | 0.62 | 0.65 | 0.44 |
| Sensitivity | 0.74 (0.66–0.86) | 0.52 | 0.51 | 0.48 | 0.69 |
| Specificity | 0.66 (0.50–0.82) | 0.63 | 0.69 | 0.63 | 0.19 |
| Metrics | Internal | Model | R1 | R2 |
|---|---|---|---|---|
| AUC | 0.72 (0.64–0.79) | 0.75 | 0.50 | 0.44 |
| Sensitivity | 0.76 (0.66–0.89) | 0.88 | 0.76 | 0.88 |
| Specificity | 0.55 (0.44–0.66) | 0.63 | 0.25 | 0.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castillo T., J.M.; Starmans, M.P.A.; Arif, M.; Niessen, W.J.; Klein, S.; Bangma, C.H.; Schoots, I.G.; Veenland, J.F. A Multi-Center, Multi-Vendor Study to Evaluate the Generalizability of a Radiomics Model for Classifying Prostate cancer: High Grade vs. Low Grade. Diagnostics 2021, 11, 369. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020369
Castillo T. JM, Starmans MPA, Arif M, Niessen WJ, Klein S, Bangma CH, Schoots IG, Veenland JF. A Multi-Center, Multi-Vendor Study to Evaluate the Generalizability of a Radiomics Model for Classifying Prostate cancer: High Grade vs. Low Grade. Diagnostics. 2021; 11(2):369. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020369
Chicago/Turabian StyleCastillo T., Jose M., Martijn P. A. Starmans, Muhammad Arif, Wiro J. Niessen, Stefan Klein, Chris H. Bangma, Ivo G. Schoots, and Jifke F. Veenland. 2021. "A Multi-Center, Multi-Vendor Study to Evaluate the Generalizability of a Radiomics Model for Classifying Prostate cancer: High Grade vs. Low Grade" Diagnostics 11, no. 2: 369. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020369