
Electromyography-Guided Adjustment of an Occlusal Appliance: Effect on Pain Perceptions Related with Temporomandibular Disorders. A Controlled Clinical Study

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
Data Handling and Statistical Analyses
3. Results
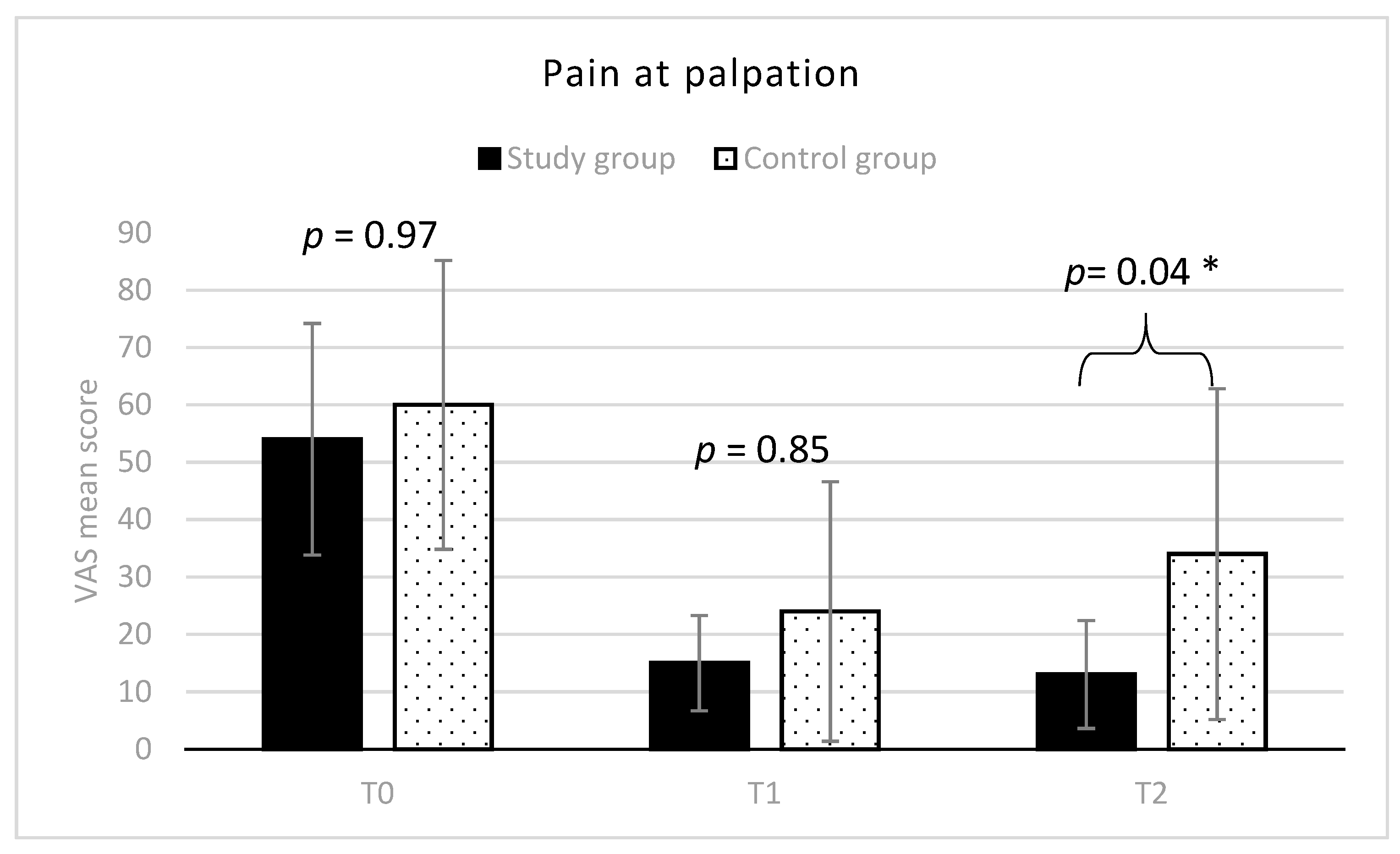
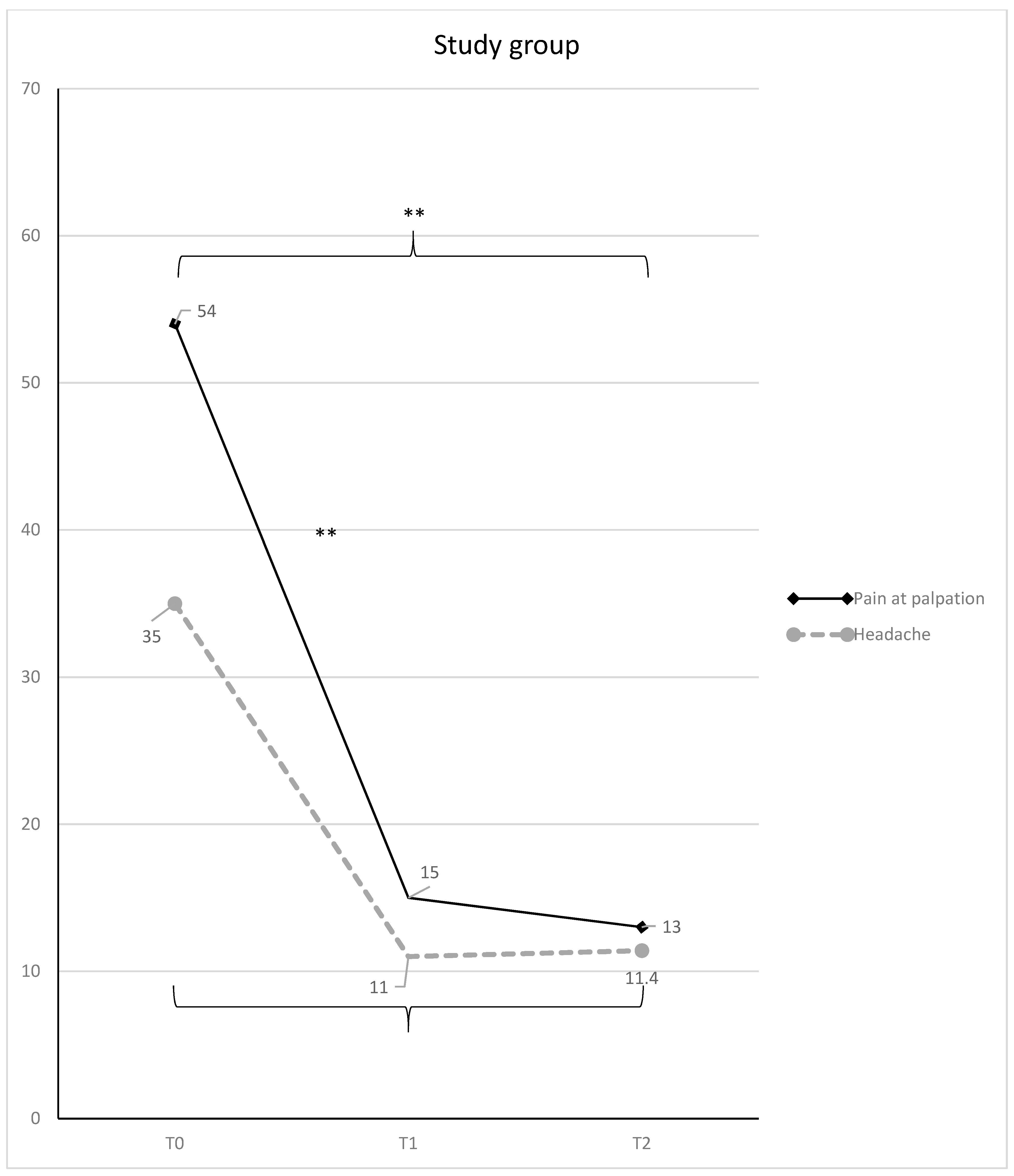
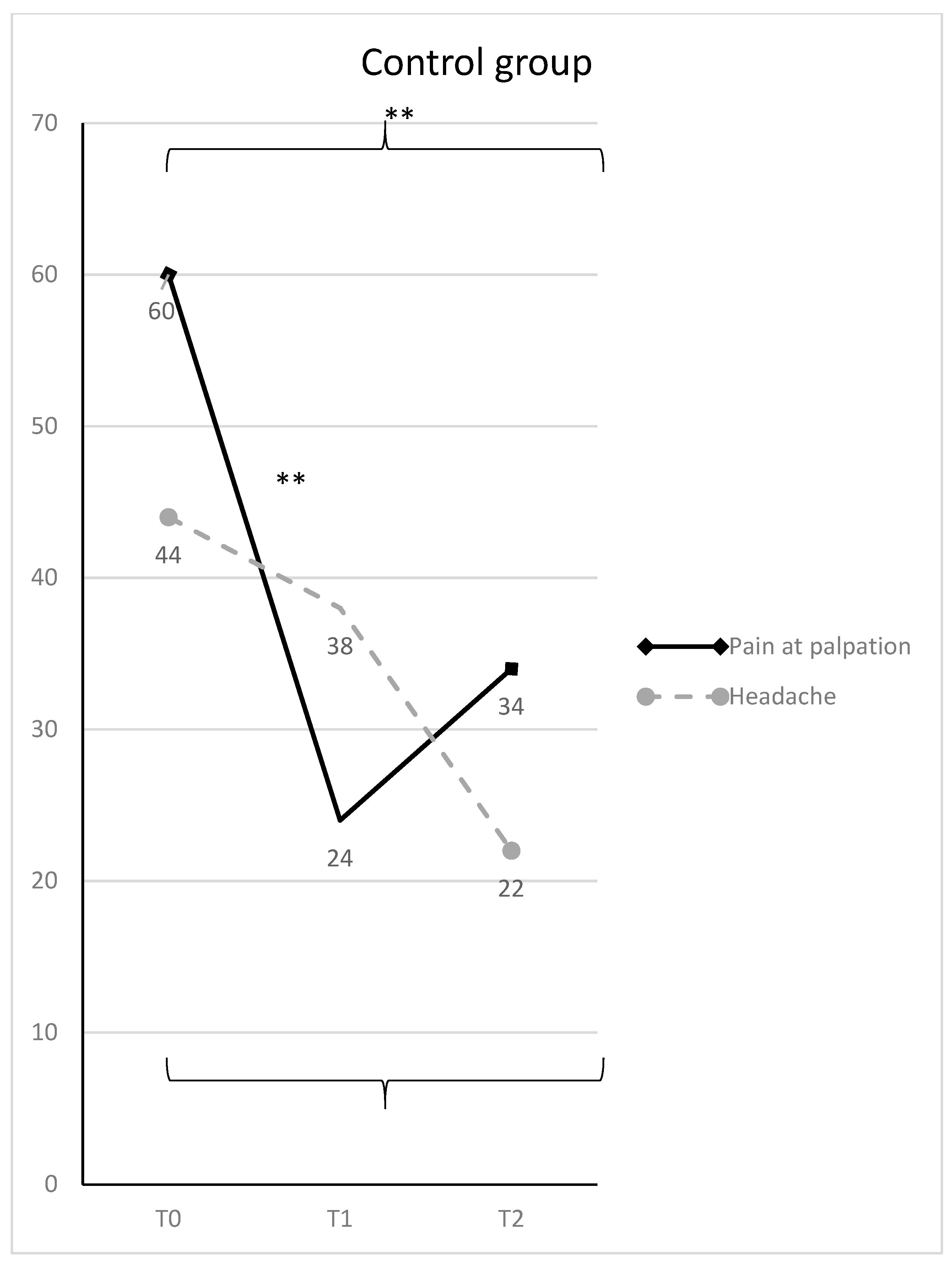
3.1. Muscular Pain at Palpation
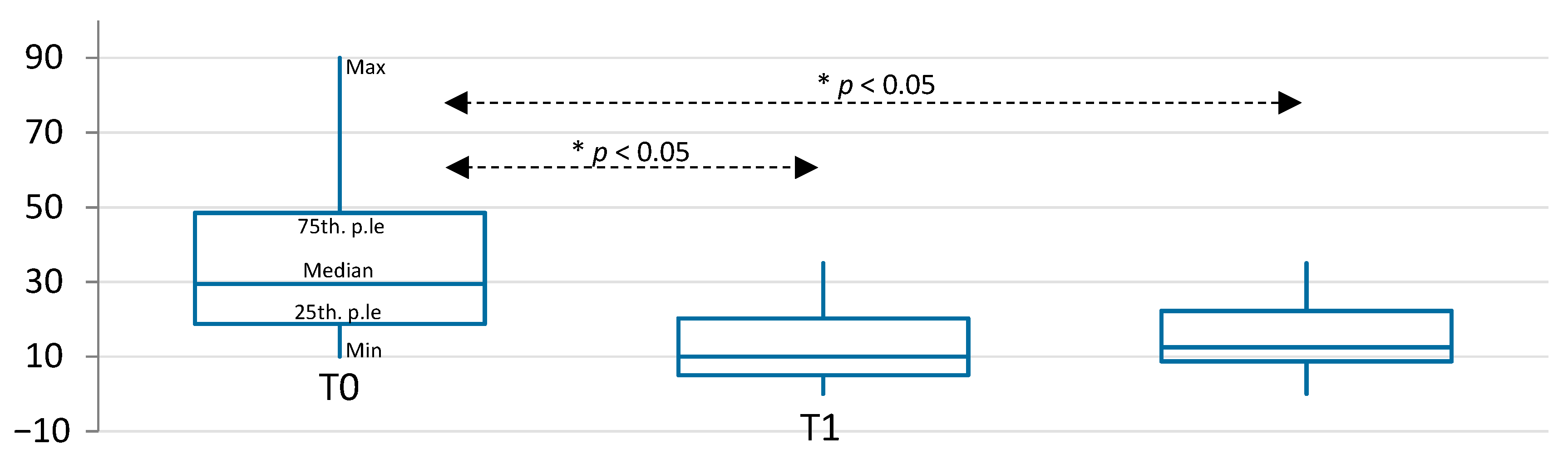
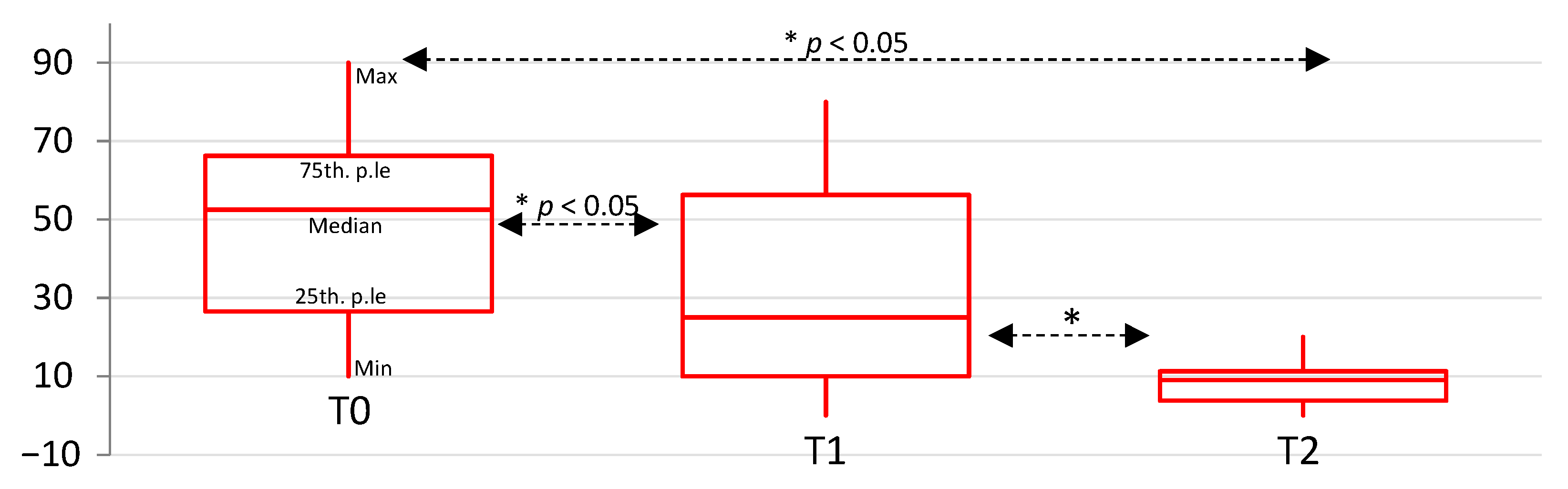
3.2. Functional Pain
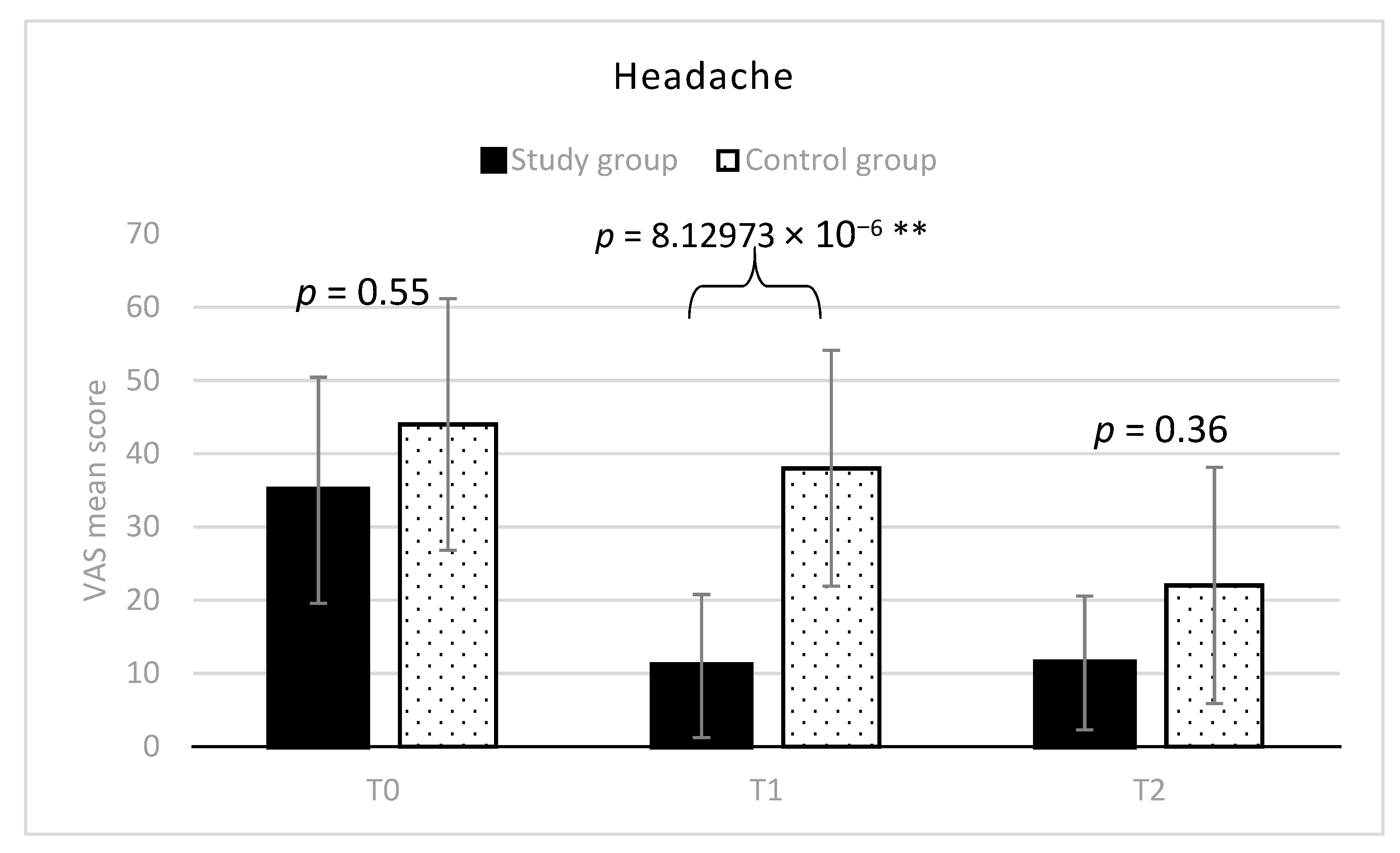
3.3. Muscular Tension Headache
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manfredini, D.; Perinetti, G.; Stellini, E.; Di Leonardo, B.; Guarda-Nardini, L. Prevalence of Static and Dynamic Dental Malocclusion features in Subgroups of Temporomandibular Disorder Patients: Implications for the Epidemiology of the TMD-Occlusion Association. Quintessence Int. 2015, 46, 341–349. [Google Scholar] [PubMed]
- Li, D.T.S.; Leung, Y.Y. Temporomandibular Disorders: Current Concepts and Controversies in Diagnosis and Management. Diagnostics 2021, 11, 459. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.M.; Cézar Simamoto-Júnior, P.; Soares, C.J.; Ramos, A.M.d.A.M.; Fernandes-Neto, A.J. Effect of Occlusal Splints on the Stress Distribution on the Temporomandibular Joint Disc. Braz. Dent. J. 2017, 28, 324–329. [Google Scholar] [CrossRef] [Green Version]
- Bender, S.D. Orofacial Pain and Headache: A Review and Look at the Commonalities. Curr. Pain Headache Rep. 2014, 18, 400. [Google Scholar] [CrossRef] [PubMed]
- Tecco, S.; Festa, F.; Salini, V.; Epifania, E.; D’Attilio, M. Treatment of Joint Pain and Joint Noises Associated with a Recent TMJ Internal Derangement: A Comparison of an Anterior Repositioning Splint, a Full-Arch Maxillary Stabilization Splint, and an Untreated Control Group. Cranio 2004, 22, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, T.; Egermarki, I.; Carlsson, G.E. A Prospective Investigation Over Two Decades on Signs and Symptoms of Temporomandibular Disorders and Associated Variables. A Final Summary. Acta Odontol. Scand. 2005, 63, 99–109. [Google Scholar] [CrossRef]
- Wiens, J.P. A Progressive Approach for the Use of Occlusal Devices in the Management of Temporomandibular Disorders. Gen. Dent. 2016, 64, 29–36. [Google Scholar]
- Klasser, G.D.; Greene, C.S. Oral Appliances in the Management of Temporomandibular Disorders. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, V.F.; Sforza, C. Coordinated Electromyographic Activity of the Human Masseter and Temporalis Anterior Muscles During Mastication. Eur. J. Oral Sci. 1996, 104, 511–517. [Google Scholar] [CrossRef]
- Tecco, S.; Cattoni, F.; Darvizeh, A.; Bosco, F.; Sanci, V.; Nota, A.; Gastaldi, G.; Gherlone, E.F. Evaluation of Masticatory Muscle Function Using Digital versus Traditional Techniques for Mockup Fabrication: A Controlled Prospective Study. Appl. Sci. 2020, 10, 6013. [Google Scholar] [CrossRef]
- Tecco, S.; Mummolo, S.; Marchetti, E.; Tetè, S.; Campanella, V.; Gatto, R.; Gallusi, G.; Tagliabue, A.; Marzo, G. sEMG Activity of Masticatory, Neck, and Trunk Muscles During the Treatment of Scoliosis with Functional Braces. A Longitudinal Controlled Study. J. Electromyogr. Kinesiol. 2011, 21, 885–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Rafah, E.M.; Alammari, M.R.; Banasr, F.H. The efficacy of bilateral balanced and canine guidance occlusal splints in the treatment of temporomandibular joint disorder. Oral Health Dent. Manag. 2014, 13, 536–542. [Google Scholar]
- Vieira de Silva, C.A.; da Silva, M.A.M.R.; Melchior, M.d.O.; de Felício, C.M.; Sforza, C.; Tartaglia, G.M. Treatment for TMD with Occlusal Splint and Electromyographic Control: Application of the FARC Protocol in a Brazilian Population. Cranio 2012, 30, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Ciuffolo, F.; Manzoli, L.; Ferritto, A.L.; Tecco, S.; D’Attilio, M.; Festa, F. Surface Electromyographic Response of the Neck Muscles to Maximal Voluntary Clenching of the Teeth. J. Oral Rehabil. 2005, 32, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Tecco, S.; Nota, A.; Caruso, S.; Primozic, J.; Marzo, G.; Baldini, A.; Gherlone, E.F. Temporomandibular Clinical Exploration in Italian Adolescents. Cranio 2019, 37, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Tecco, S.; Caputi, S.; Festa, F. Evaluation of Cervical Posture Following Palatal Expansion: A 12-Month Follow-Up Controlled Study. Eur. J. Orthod. 2007, 29, 45–51, Erratum in: Eur. J. Orthod. 2008, 30, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tecco, S.; Polimeni, A.; Saccucci, M.; Festa, F. Postural Loads During Walking After an Imbalance of Occlusion Created with Unilateral Cotton Roll. BMC Res Notes. 2010, 25, 3–141. [Google Scholar] [CrossRef] [Green Version]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Orofacial Pain Special Interest Group, International Association for the Study of Pain. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Baldini, A.; Tecco, S.; Cioffi, D.; Rinaldi, A.; Longoni, S. Gnatho-Postural Treatment in an Air Force Pilot. Aviat. Space Environ. Med. 2012, 83, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, V.F.; Tartaglia, G.M.; Galletta, A.; Grassi, G.P.; Sforza, C. The Influence of Occlusion on Jaw and Neck Muscle Activity: A Surface EMG study in Healthy Young Adults. J. Oral Rehabil. 2006, 33, 341–348. [Google Scholar] [CrossRef]
- Sforza, C.; Rosati, R.; De Menezes, M.; Musto, F.; Toma, M. EMG Analysis of Trapezius and Masticatory Muscles: Experimental Protocol and Data Reproducibility. J. Oral Rehabil. 2011, 38, 648–654. [Google Scholar] [CrossRef] [PubMed]
- De Felício, C.M.; Ferreira, C.L.P.; Medeiros, A.P.M.; Rodrigues Da Silva, M.A.M.; Tartaglia, G.M.; Sforza, C. Electromyographic Indices, Orofacial Myofunctional Status and Temporomandibular Disorders Severity: A Correlation Study. J. Electromyogr. Kinesiol. 2012, 22, 266–272. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test Group | Control Group | |||||
|---|---|---|---|---|---|---|
| T0 Mean ± SD | T1 Mean ± SD | T2 Mean ± SD | T0 Mean ± SD | T1 Mean ± SD | T2 Mean ± SD | |
| VAS (Muscular Pain at Palpation) | 54 ± 20.2 | 15 ± 8.29 | 13 ± 9.36 | 60 ± 25.17 | 24 ± 22.61 | 34 ± 28.82 |
| VAS (Headache) | 35 ± 15.44 | 11 ± 9.76 | 11.4 ± 9.13 | 44 ± 17.18 | 38 ± 16.08 | 22 ± 16.13 |
| Test Group | Control Group | |||||
|---|---|---|---|---|---|---|
| T0 Median (25th and 75th p.le) | T1 Median (25th and 75th p.le) | T2 Median (25th and 75th p.le) | T0 Median (25th and 75th p.le) | T1 Median (25th and 75th p.le) | T2 Median (25th and 75th p.le) | |
| VAS (Functional Pain) | 29.5 (18.75–48.5) | 10 * (5–20.25) | 12.5 (8.75–22.25) | 52.5 (26.5–66.25) | 25 (10–56.25) | 9 (3.75–11.25) |
| Group 1 | Group 2 | |||||
|---|---|---|---|---|---|---|
| T0-T1 | T1-T2 | T0-T2 | T0-T1 | T1-T2 | T0-T2 | |
| Muscular Pain at Palpation | −72.22% | −13.32% | −75.92% | −60.00% | +41.66% | −43.33% |
| Headache | −68.57% | +3.63% | −67.42% | −13.63% | −42.10% | −50% |
| Functional Pain | −66.66% | +25% | −58.33% | −36.00% | −62.5% | −76% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tecco, S.; Quinzi, V.; Nota, A.; Giovannozzi, A.; Abed, M.R.; Marzo, G. Electromyography-Guided Adjustment of an Occlusal Appliance: Effect on Pain Perceptions Related with Temporomandibular Disorders. A Controlled Clinical Study. Diagnostics 2021, 11, 667. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040667
Tecco S, Quinzi V, Nota A, Giovannozzi A, Abed MR, Marzo G. Electromyography-Guided Adjustment of an Occlusal Appliance: Effect on Pain Perceptions Related with Temporomandibular Disorders. A Controlled Clinical Study. Diagnostics. 2021; 11(4):667. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040667
Chicago/Turabian StyleTecco, Simona, Vincenzo Quinzi, Alessandro Nota, Alessandro Giovannozzi, Maria Rosaria Abed, and Giuseppe Marzo. 2021. "Electromyography-Guided Adjustment of an Occlusal Appliance: Effect on Pain Perceptions Related with Temporomandibular Disorders. A Controlled Clinical Study" Diagnostics 11, no. 4: 667. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040667