
Atypical Granulomatosis with Polyangiitis Presenting with Meibomitis, Scleritis, Uveitis and Papillary Bladder Tumor: A Case Report and Literature Review

 ,
,  ,
,
Abstract
:1. Introduction
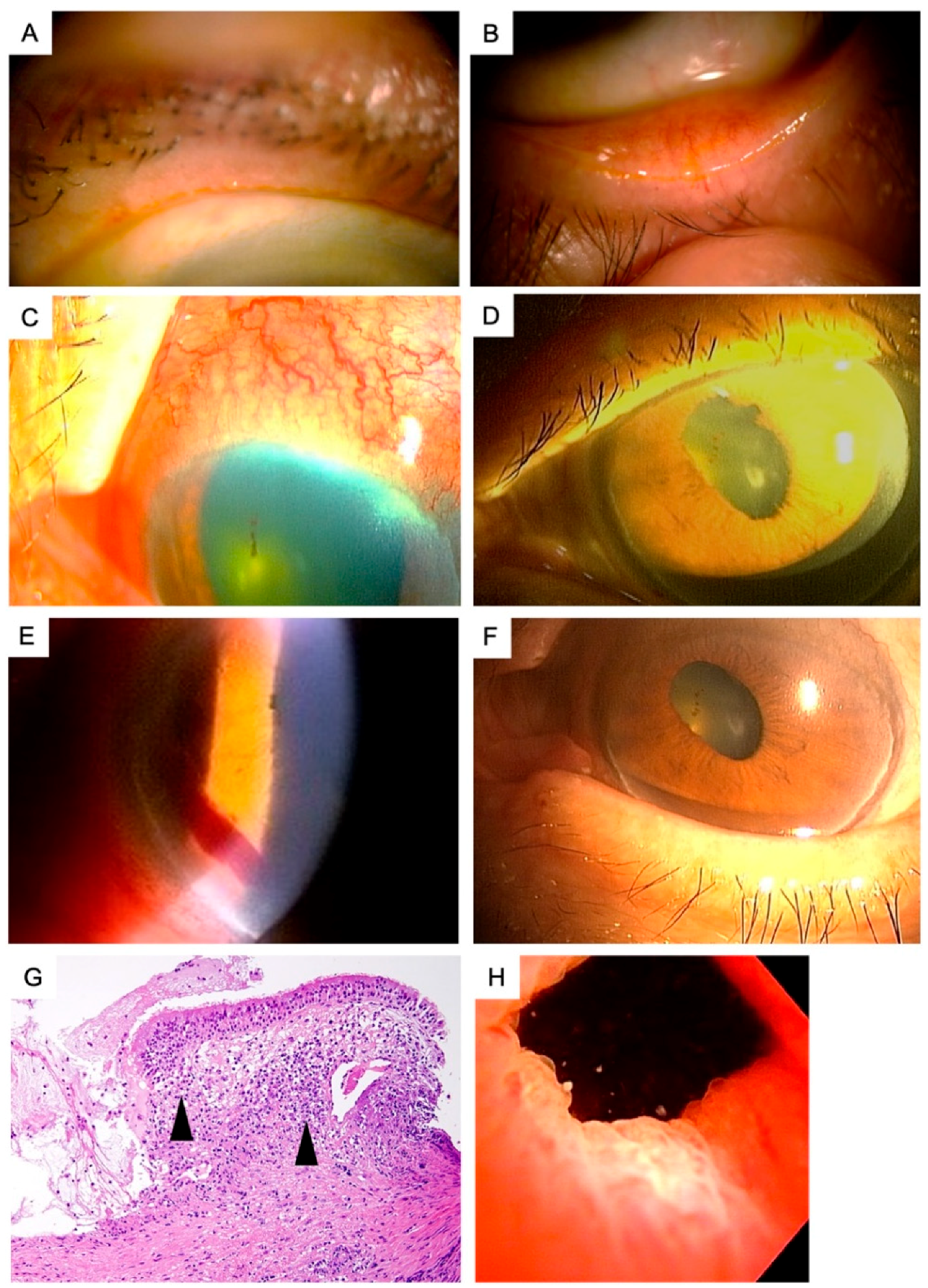
2. Report of a Case
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kojima, T.; Dogru, M.; Matsumoto, Y.; Goto, E.; Tsubota, K. Tear film and ocular surface abnormalities after eyelid tattooing. Ophthalmic Plast. Reconstr. Surg. 2005, 21, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Chhadva, P.; Goldhardt, R.; Galor, A. Meibomian gland disease: The role of gland dysfunction in dry eye disease. Ophthalmology 2017, 124, S20–S26. [Google Scholar] [CrossRef] [PubMed]
- Amano, S. Meibomian gland dysfunction: Recent progress worldwide and in Japan. Investig. Ophthalmol. Vis. Sci. 2018, 59, DES87–DES93. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.C.Y.; Chow, S.S.W.; Wan, K.H.N.; Yuen, H.K.L. Update on the association between dry eye disease and meibomian gland dysfunction. Hong Kong Med. J. 2019, 25, 38–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, J.D.; Shimazaki, J.; Benitez-del-Castillo, J.M.; Craig, J.P.; McCulley, J.P.; Den, S.; Foulks, G.N. The international workshop on meibomian gland dysfunction: Report of the definition and classification subcommittee. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1930–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blackie, C.A.; Korb, D.R.; Knop, E.; Bedi, R.; Knop, N.; Holland, E.J. Nonobvious obstructive meibomian gland dysfunction. Cornea 2010, 29, 1333–1345. [Google Scholar] [CrossRef] [Green Version]
- Nichols, K.K.; Foulks, G.N.; Bron, A.J.; Glasgow, B.J.; Dogru, M.; Tsubota, K.; Lemp, M.A.; Sullivan, D.A. The international workshop on meibomian gland dysfunction: Executive summary. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1922–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaumberg, D.A.; Nichols, J.J.; Papas, E.B.; Tong, L.; Uchino, M.; Nichols, K.K. The international workshop on meibomian gland dysfunction: Report of the subcommittee on the epidemiology of, and associated risk factors for, MGD. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1994–2005. [Google Scholar] [CrossRef] [Green Version]
- Kabatas, N.; Dogan, A.S.; Kabatas, E.U.; Acar, M.; Bicer, T.; Gurdal, C. The effect of demodex infestation on blepharitis and the ocular symptoms. Eye Contact Lens 2017, 43, 64–67. [Google Scholar] [CrossRef]
- Ucakhan, O.; Arslanturk-Eren, M. The role of soft contact lens wear on meibomian gland morphology and function. Eye Contact Lens 2019, 45, 292–300. [Google Scholar] [CrossRef]
- Wang, M.T.M.; Muntz, A.; Lim, J.; Kim, J.S.; Lacerda, L.; Arora, A.; Craig, J.P. Ageing and the natural history of dry eye disease: A prospective registry-based cross-sectional study. Ocul. Surf. 2020, 18, 736–741. [Google Scholar] [CrossRef]
- Lin, X.; Xu, B.; Zheng, Y.; Coursey, T.G.; Zhao, Y.; Li, J.; Fu, Y.; Chen, X.; Zhao, Y.E. Meibomian gland dysfunction in type 2 diabetic patients. J. Ophthalmol. 2017, 2017, 3047867. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, J.; Goto, E.; Ono, M.; Shimmura, S.; Tsubota, K. Meibomian gland dysfunction in patients with Sjogren syndrome. Ophthalmology 1998, 105, 1485–1488. [Google Scholar] [CrossRef]
- Kubaisi, B.; Abu Samra, K.; Foster, C.S. Granulomatosis with polyangiitis (Wegener’s disease): An updated review of ocular disease manifestations. Intractable Rare Dis. Res. 2016, 5, 61–69. [Google Scholar] [CrossRef] [Green Version]
- Sfiniadaki, E.; Tsiara, I.; Theodossiadis, P.; Chatziralli, I. Ocular manifestations of granulomatosis with polyangiitis: A review of the literature. Ophthalmol. Ther. 2019, 8, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Catanoso, M.; Macchioni, P.; Boiardi, L.; Manenti, L.; Tumiati, B.; Cavazza, A.; Luberto, F.; Pipitone, N.; Salvarani, C. Epidemiology of granulomatosis with polyangiitis (Wegener’s granulomatosis) in Northern Italy: A 15-year population-based study. Semin. Arthritis Rheum. 2014, 44, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Villa-Forte, A.; Clark, T.M.; Gomes, M.; Carey, J.; Mascha, E.; Karafa, M.T.; Roberson, G.; Langford, C.A.; Hoffman, G.S. Substitution of methotrexate for cyclophosphamide in Wegener granulomatosis: A 12-year single-practice experience. Medicine 2007, 86, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Tarabishy, A.B.; Schulte, M.; Papaliodis, G.N.; Hoffman, G.S. Wegener’s granulomatosis: Clinical manifestations, differential diagnosis, and management of ocular and systemic disease. Surv. Ophthalmol. 2010, 55, 429–444. [Google Scholar] [CrossRef] [PubMed]
- Chipczynska, B.; Gralek, M.; Hautz, W.; Zegadlo-Mylik, M.; Kocyla-Karczmarewicz, B.; Kanigowska, K.; Seroczynska, M.; Kepa, B.; Klimczak-Slaczka, D. Orbital tumor as an initial manifestation of Wegener’s granulomatosis in children: A series of four cases. Med. Sci. Monit. 2009, 15, CS135–CS138. [Google Scholar] [PubMed]
- Muller, K.; Lin, J.H. Orbital granulomatosis with polyangiitis (Wegener granulomatosis): Clinical and pathologic findings. Arch. Pathol. Lab. Med. 2014, 138, 1110–1114. [Google Scholar] [CrossRef] [Green Version]
- Hibino, M.; Kondo, T. Dacryoadenitis with ptosis and diplopia as the initial presentation of granulomatosis with polyangiitis. Intern. Med. 2017, 56, 2649–2653. [Google Scholar] [CrossRef] [Green Version]
- Ghanem, R.C.; Chang, N.; Aoki, L.; Santo, R.M.; Matayoshi, S. Vasculitis of the lacrimal sac wall in Wegener granulomatosis. Ophthalmic Plast. Reconstr. Surg. 2004, 20, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Tullo, A.B.; Durrington, P.; Graham, E.; Holt, L.P.; Easty, D.L.; Bonshek, R.; Noble, J.L. Florid xanthelasmata (yellow lids) in orbital Wegener’s granulomatosis. Br. J. Ophthalmol. 1995, 79, 453–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, D.R.; Zafar, A.; Brownstein, S.; Faraji, H. Cicatricial conjunctival inflammation with trichiasis as the presenting feature of Wegener granulomatosis. Ophthalmic Plast. Reconstr. Surg. 2006, 22, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Miserocchi, E.; Waheed, N.K.; Baltatzis, S.; Foster, C.S. Chronic cicatrizing conjunctivitis in a patient with ocular cicatricial pemphigoid and fatal Wegener granulomatosis. Am. J. Ophthalmol. 2001, 132, 923–924. [Google Scholar] [CrossRef]
- Robinson, M.R.; Lee, S.S.; Sneller, M.C.; Lerner, R.; Langford, C.A.; Talar-Williams, C.; Cox, T.A.; Chan, C.C.; Smith, J.A. Tarsal-conjunctival disease associated with Wegener’s granulomatosis. Ophthalmology 2003, 110, 1770–1780. [Google Scholar] [CrossRef]
- Sadiq, S.A.; Jennings, C.R.; Jones, N.S.; Downes, R.N. Wegener’s granulomatosis: The ocular manifestations revisited. Orbit 2000, 19, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Cocho, L.; Gonzalez-Gonzalez, L.A.; Molina-Prat, N.; Doctor, P.; Sainz-de-la-Maza, M.; Foster, C.S. Scleritis in patients with granulomatosis with polyangiitis (Wegener). Br. J. Ophthalmol. 2016, 100, 1062–1065. [Google Scholar] [CrossRef]
- Fortney, A.C.; Chodosh, J. Conjunctival ulceration in recurrent Wegener granulomatosis. Cornea 2002, 21, 623–624. [Google Scholar] [CrossRef]
- Cao, Y.; Zhang, W.; Wu, J.; Zhang, H.; Zhou, H. Peripheral ulcerative keratitis associated with autoimmune disease: Pathogenesis and treatment. J. Ophthalmol. 2017, 2017, 7298026. [Google Scholar] [CrossRef] [Green Version]
- Reddy, S.C.; Tajunisah, I.; Rohana, T. Bilateral scleromalacia perforans and peripheral corneal thinning in Wegener’s granulomatosis. Int. J. Ophthalmol. 2011, 4, 439–442. [Google Scholar] [CrossRef]
- Wang, M.; Khurana, R.N.; Sadda, S.R. Central retinal vein occlusion in Wegener’s granulomatosis without retinal vasculitis. Br. J. Ophthalmol. 2006, 90, 1435–1436. [Google Scholar] [CrossRef] [Green Version]
- Lozano-Lopez, V.; Rodriguez-Lozano, B.; Losada-Castillo, M.J.; Delgado-Frias, E.; Dopazo-Luque, D.; Serrano-Garcia, M. Central retinal artery occlusion in Wegener’s granulomatosis: A diagnostic dilemma. J. Ophthalmic Inflamm. Infect. 2011, 1, 71–75. [Google Scholar] [CrossRef] [Green Version]
- Takazawa, T.; Ikeda, K.; Nagaoka, T.; Hirayama, T.; Yamamoto, T.; Yanagihashi, M.; Tochikubo, T.; Iwasaki, Y. Wegener granulomatosis-associated optic perineuritis. Orbit 2014, 33, 13–16. [Google Scholar] [CrossRef]
- Purvin, V.; Kawasaki, A. Optic perineuritis secondary to Wegener’s granulomatosis. Clin. Exp. Ophthalmol. 2009, 37, 712–717. [Google Scholar] [CrossRef]
- Moubayed, S.P.; Black, D.O. Optic neuritis as an initial presentation of Wegener’s granulomatosis. Can. J. Ophthalmol. 2009, 44, e59. [Google Scholar] [CrossRef]
- Niskopoulou, M.; Du Toit, N. Optic neuritis as a feature of Wegener’s granulomatosis. Eye 2002, 16, 320–321. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, M.L.; Borges, W.I.; do Val Ferreira Ramos, C.; Lucato, L.T.; Leite, C.C. Bilateral optic neuritis in wegener granulomatosis. J. Neuroophthalmol. 2005, 25, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Nowack, R.; Wachtler, P.; Kunz, J.; Rasmussen, N. Cranial nerve palsy in Wegener’s granulomatosis—Lessons from clinical cases. J. Neurol. 2009, 256, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.R.; Theaker, J.M.; Manners, R.M. Wegener’s granulomatosis masquerading as upper lid chalazion. Eye 2007, 21, 883–884. [Google Scholar] [CrossRef] [PubMed]
- Rafiei, R.; Alizadeh, N.; Nejad, K.G.; Rafiee, B.; Najirad, S. Unilateral eyelid edema and mucosal involvement as the first presentations of Wegener granulomatosis. Casp. J. Intern. Med. 2019, 10, 343–346. [Google Scholar] [CrossRef]
- Knop, E.; Knop, N.; Millar, T.; Obata, H.; Sullivan, D.A. The international workshop on meibomian gland dysfunction: Report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1938–1978. [Google Scholar] [CrossRef] [Green Version]
- McCulley, J.P.; Shine, W.E. Meibomian gland function and the tear lipid layer. Ocul. Surf. 2003, 1, 97–106. [Google Scholar] [CrossRef]
- Frangou, E.; Vassilopoulos, D.; Boletis, J.; Boumpas, D.T. An emerging role of neutrophils and NETosis in chronic inflammation and fibrosis in systemic lupus erythematosus (SLE) and ANCA-associated vasculitides (AAV): Implications for the pathogenesis and treatment. Autoimmun. Rev. 2019, 18, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Negreros, M.; Flores-Suarez, L.F. A proposed role of neutrophil extracellular traps and their interplay with fibroblasts in ANCA-associated vasculitis lung fibrosis. Autoimmun. Rev. 2021, 20, 102781. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Yasuoka, H.; Yoshimoto, K.; Suzuki, K.; Takeuchi, T. Platelet CXCL4 mediates neutrophil extracellular traps formation in ANCA-associated vasculitis. Sci. Rep. 2021, 11, 222. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, D.; Masuda, S.; Tomaru, U.; Ishizu, A. Pathogenesis and therapeutic interventions for ANCA-associated vasculitis. Nat. Rev. Rheumatol. 2019, 15, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, A.; Hasikova, L.; Hampel, U.; Gruneboom, A.; Shan, X.; Herrmann, I.; Garreis, F.; Bock, F.; Knopf, J.; Singh, J.; et al. Aggregated neutrophil extracellular traps occlude Meibomian glands during ocular surface inflammation. Ocul. Surf. 2021, 20, 1–12. [Google Scholar] [CrossRef]


{kind=link}
| Tissue | Diseases |
|---|---|
| Orbital Involvement (45–50%) | Dacryoadenitis, Orbital Myositis, Orbital Pseudotumor |
| Eyelids, Lacrimal system and the conjunctiva (16%) | Dacryoadenitis, Dacryocystitis, Nasolacrimal duct obstruction, Ptosis, Lid granuloma, Chalazion, Entropion, Trichiasis, Xanthelasma, Cicatrizing conjunctivitis, Conjunctival ulceration/necrosis |
| Sclera (16–38%) | Diffuse, nodular or necrotizing anterior scleritis, Posterior scleritis |
| Cornea (0–40%) | Peripheral ulcerative keratitis, Exposure keratopathy, Infectious keratitis, Corneal perforation |
| Uvea (0–10%) | Unilateral or bilateral anterior, intermediate or posterior uveitis |
| Retina and choroid | Unilateral or bilateral, central or multifocal vasculitis, Retinitis, Chorioretinitis, Macular edema, Exudative retinal detachment, Retinal necrosis, Retinal vein occlusion |
| Neuroophthalmic manifestations | Optic neuritis/perineuritis, Compressive optic neuropathy, Oculomotor, trochlear and abducens nerve palsies, Horner’s syndrome |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kojima, T.; Dogru, M.; Shimizu, E.; Yazu, H.; Takahashi, A.; Shimazaki, J. Atypical Granulomatosis with Polyangiitis Presenting with Meibomitis, Scleritis, Uveitis and Papillary Bladder Tumor: A Case Report and Literature Review. Diagnostics 2021, 11, 680. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040680
Kojima T, Dogru M, Shimizu E, Yazu H, Takahashi A, Shimazaki J. Atypical Granulomatosis with Polyangiitis Presenting with Meibomitis, Scleritis, Uveitis and Papillary Bladder Tumor: A Case Report and Literature Review. Diagnostics. 2021; 11(4):680. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040680
Chicago/Turabian StyleKojima, Takashi, Murat Dogru, Eisuke Shimizu, Hiroyuki Yazu, Aya Takahashi, and Jun Shimazaki. 2021. "Atypical Granulomatosis with Polyangiitis Presenting with Meibomitis, Scleritis, Uveitis and Papillary Bladder Tumor: A Case Report and Literature Review" Diagnostics 11, no. 4: 680. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040680